Embed Size (px)
Citation preview
Familial Mediterranean Fever(FMF)
Definition
An autosomal recessive disease, characterized by recurrent febrile episodes
with serositis involving the peritoneum, pleura and synovium.
Ethnic distribution
• Turks• Armenian• Arabs and Druzes• Non-Ashkenazi Jews.• Sporadic cases - all over the world.
Age of Onset
0-10 years 53% 11-20 years 29% 21-30 years 14% 31-40 years 3% Over 40 years 1%
Attack Duration and Frequency
• Lasts 24-96 hours• Peak intensity –12 hours• Vary• Once –twice a week to once a year
Fever
• In most of the cases (99%).
• Temp. 37.5 to 40 C.• Rarely can be the
only feature.
Peritonitis
- In 96 % of the cases. - Presenting feature in 80%. - Resembles “surgical Abdomen”. - About 30% undergo Appendectomy.
Pleuritis
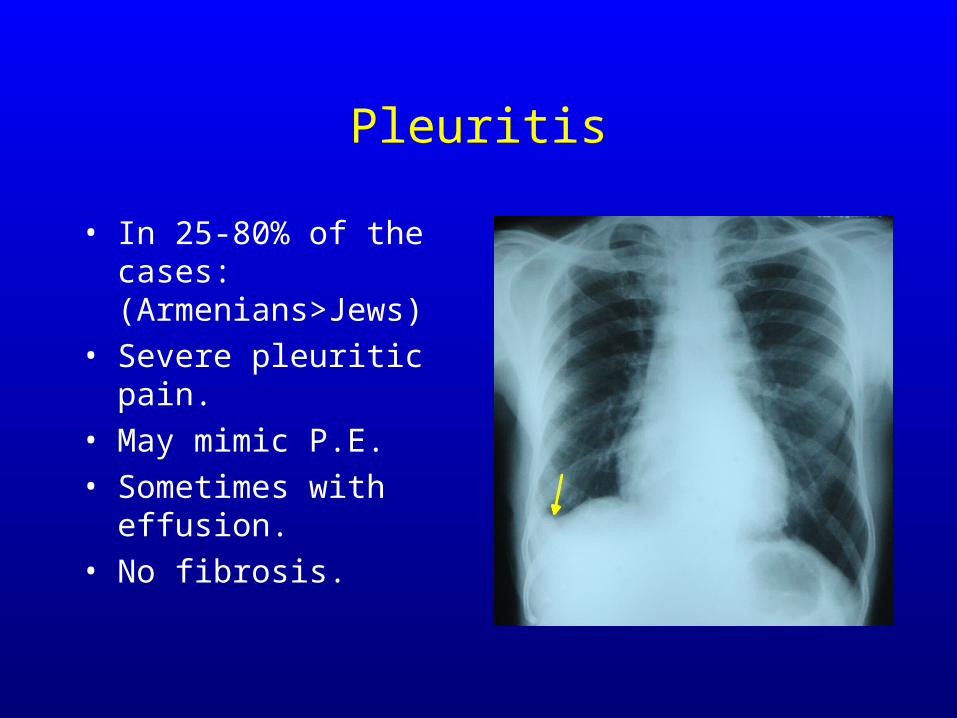
• In 25-80% of the cases: (Armenians>Jews)
• Severe pleuritic pain.• May mimic P.E.• Sometimes with
effusion.• No fibrosis.
Pericarditis
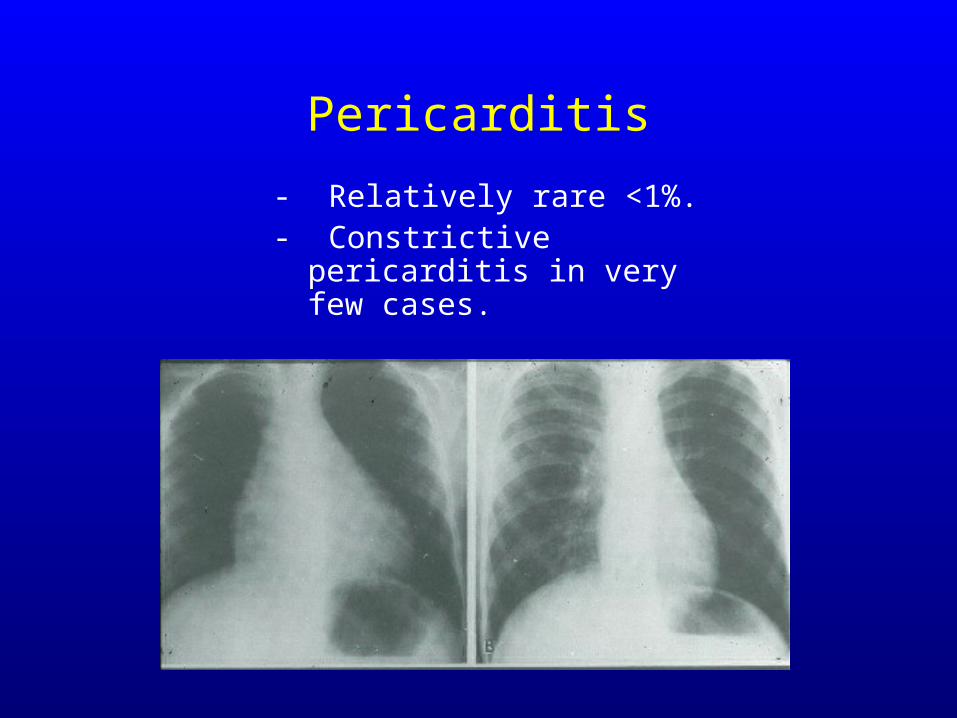
- Relatively rare <1%.- Constrictive pericarditis in
very few cases.
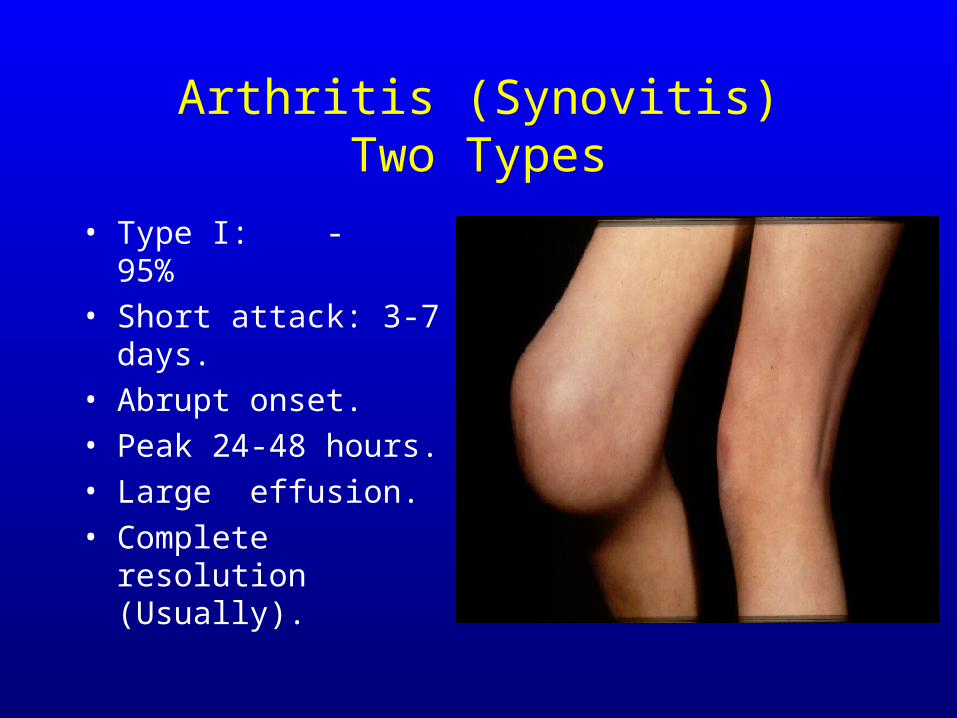
Arthritis (Synovitis)Two Types
• Type I: - 95%• Short attack: 3-7
days.• Abrupt onset.• Peak 24-48 hours.• Large effusion.• Complete resolution
(Usually).
Arthritis (Cont.)
• Type II:• Chronic destructive arthritis.• Commonly affects the hips and knees.• Sometimes – sacroiliitis-HLA B27
negative.
Skin Involvement
• In 7-40% of the cases.• Erysipelas-like erythema.• Medial or lateral aspect of the ankles or
dorsum of the foot.• D.D with cellulitis or arthritis.• May be an only feature in children.

Myalgia
• Three types (mainly in children) - 25%.• Spontaneous pattern (8%):appearing
during attacks, affecting legs and arms.• Exercised induced (81%) - may occur
between attacks.• Protracted febrile myalgia (11%) -
vasculitis? Steroid responsive.
Involvement of Other Organs
• Acute orchitis.• Splenomegaly with no amyloidosis.• Meningitis?? (Mollaret’s).
Precipitating Factors
• Physical activity.• Emotional stress.• Inter-current infections.• Cold exposure.• Menstruation.• Fatty meal ??
Amyloidosis
• Type I: Following many years of typical FMF attacks. ( with no treatment).
• Type II (?): Appearance of nephrotic syndrome without previous classic FMF attacks.
Etiology and Pathogenesis-(hypotheses)
• Autoimmune disease (vasculitis) ?.• Etiocholanolone fever ?.• Disturbed metabolism of
cathecholamines ?.• Deficiency of complement
components ?.• HLA-related ?.
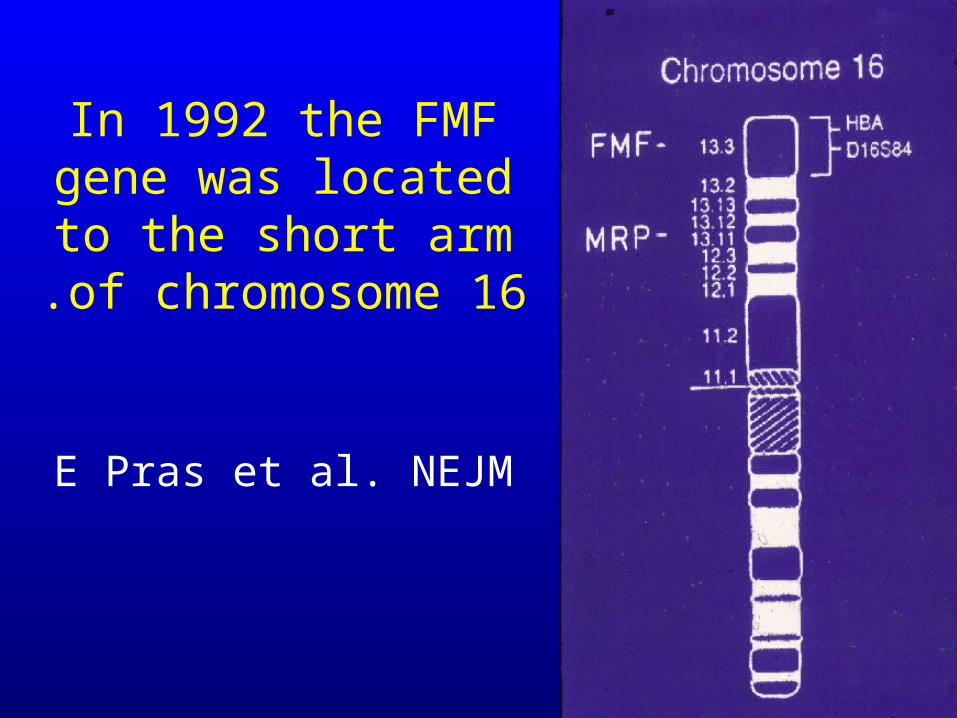
In 1992 the FMF gene was located to
the short arm of chromosome 16.
E Pras et al. NEJM

In 1997 the MEFV gene was isolated independently by two
consortia:The International FMF consortium The French
consortium.
Marenostrin/Pyrin (1997-2000)
• A new cytosolic protein with unknown function.
• 781 amino acids.• Expressed mainly in mature neutrophils.• Is not expressed by synovial or
peritoneal cells.
C-CPYD B B30.2
PYD
PYD CARD
PYD
HIN-200
PYD HIN-200
PYD HIN-200HIN-200
CARDNBS LRRPYD
PYD NBS LRR
PYD NBS LRR
PYD NBS LRR
Pyrin
NALP1(DEFCAP, CARD7)
NALP2
NALP3(Cryopyrin)
NALP4
ASC
POP1
AIM2
MNDA
IFI16
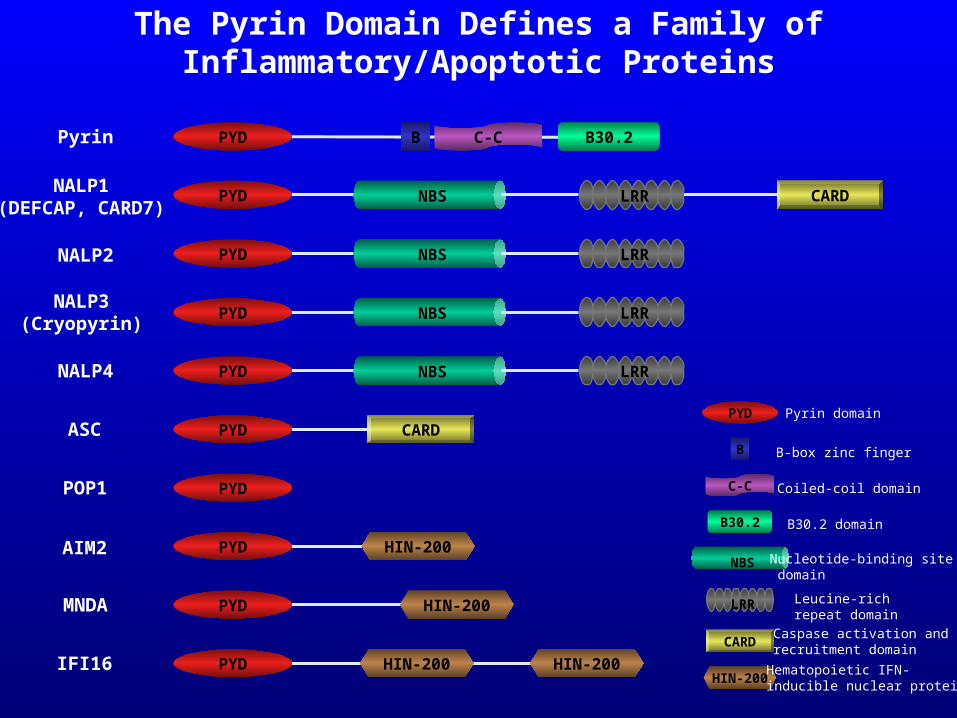
The Pyrin Domain Defines a Family of Inflammatory/Apoptotic Proteins
PYD
B
C-C
B30.2
NBS
LRR
CARD
HIN-200
Pyrin domain
B-box zinc finger
Coiled-coil domain
B30.2 domain
Nucleotide-binding site domain
Leucine-rich repeat domain
Caspase activation and recruitment domain
Hematopoietic IFN-inducible nuclear protein
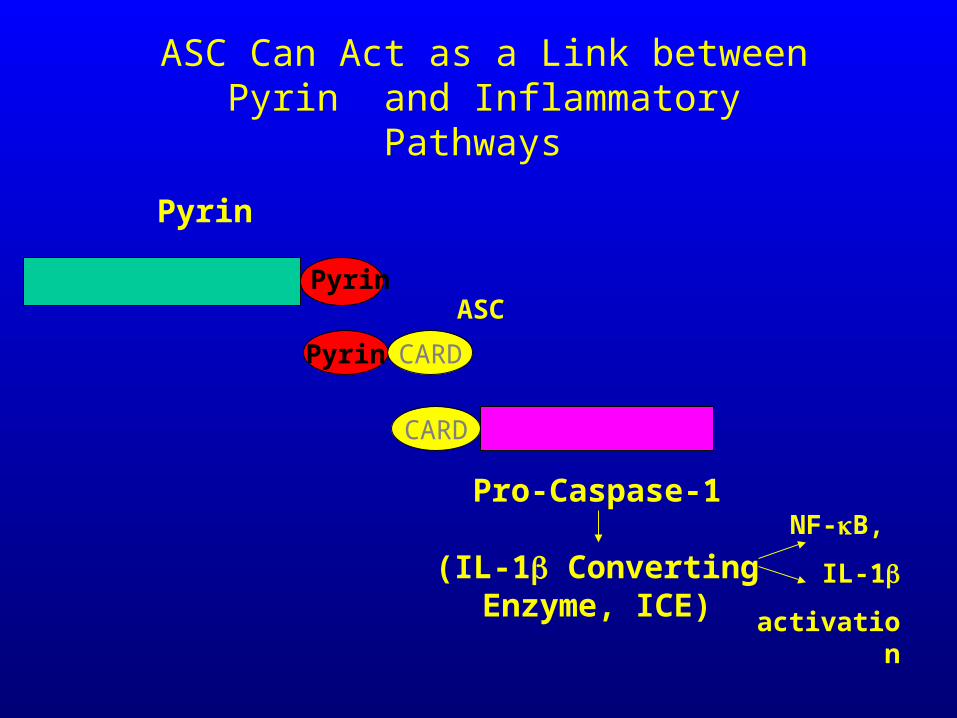
Pyrin
Pyrin
Pyrin CARD
ASC
ASC Can Act as a Link between Pyrin and Inflammatory Pathways
NF-B,
IL-1
activation
CARD
Pro-Caspase-1
(IL-1 Converting Enzyme, ICE)
FMF - Diagnosis
• Typical clinical manifestations.• Family history.• Routine laboratory tests are not specific
or contributory.
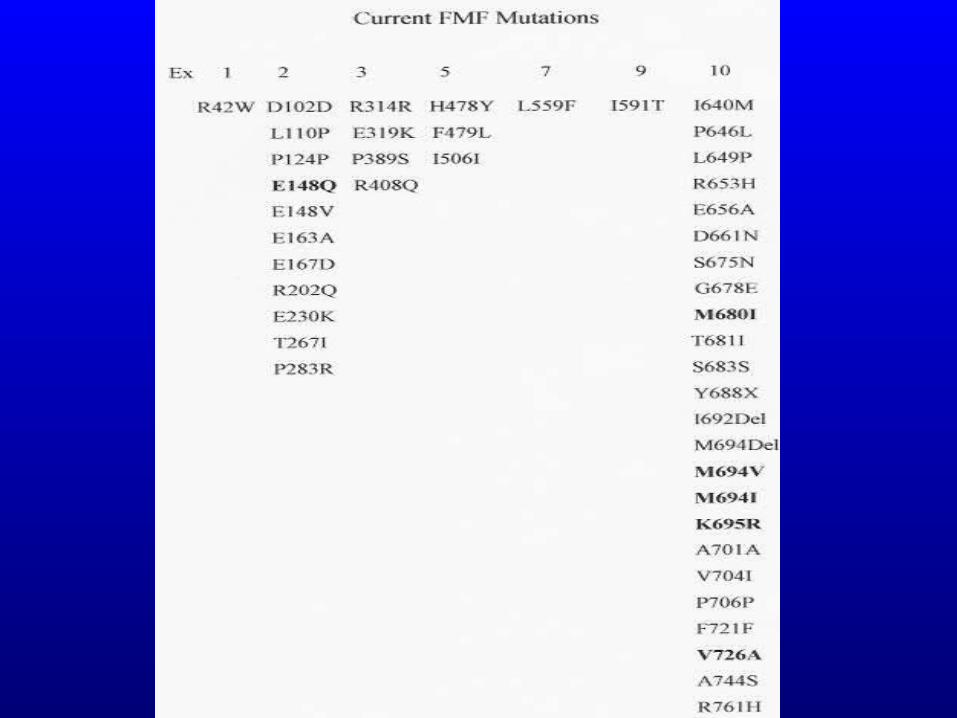
FMF Diagnosis (Cont.)
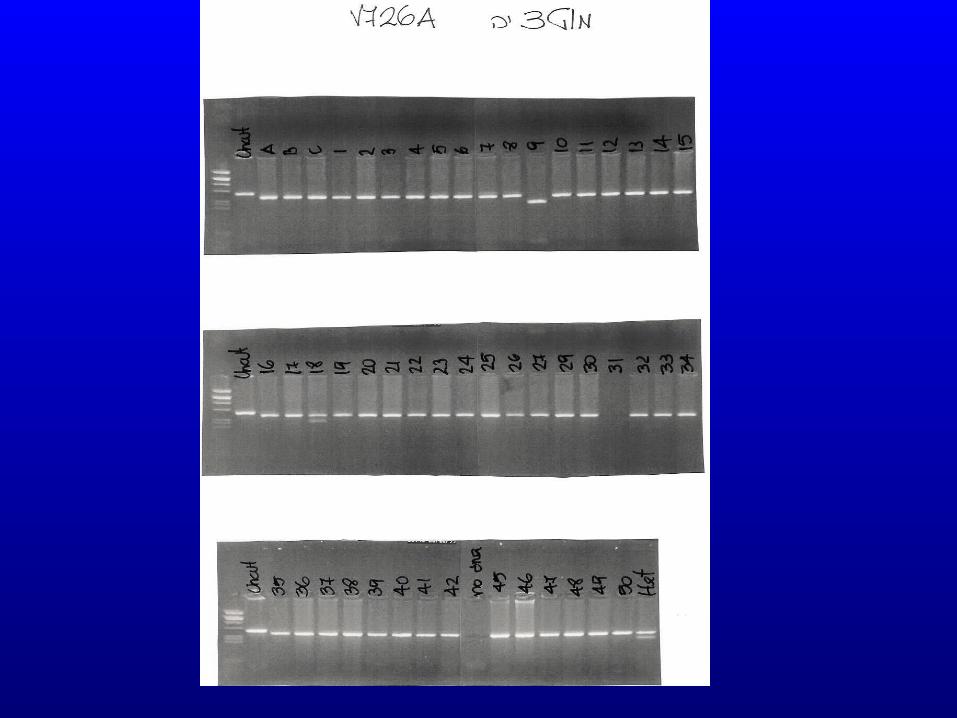
In atypical cases:• Mutations detected by PCR is an
additional tool for FMF diagnosis, especially in atypical cases.
Genetics of FMF
• FMF occurs in members of one generation – suggesting autosomal recessive heredity.
• High consanguinity rate may lead to its occurrence in successive generations – pseudo-dominant trait.
• Several studies described autosomal dominant transmission in patients with mutations of deletion (M694del).
Genetics (Cont.)
• Carrier rate varies among ethnic groups:
• Iraqi Jews - 1:3• North-African Jews - 1:5• Ashkenazi Jews - 1:10• Israeli Arabs - 1:10• Armenians - 1:7• Turkish - 1:5
Mutations Distribution
• In Israel• North-African Jews - M694V, E148Q• Iraqui Jews-V726A, M694V,
E148Q,M680I• Ashkenazi Jews – E148Q,V726A, • Arabs -
V726A,M680I,M694V,M694I,E148Q• Turks – M694V, M680I, V726A, E148Q

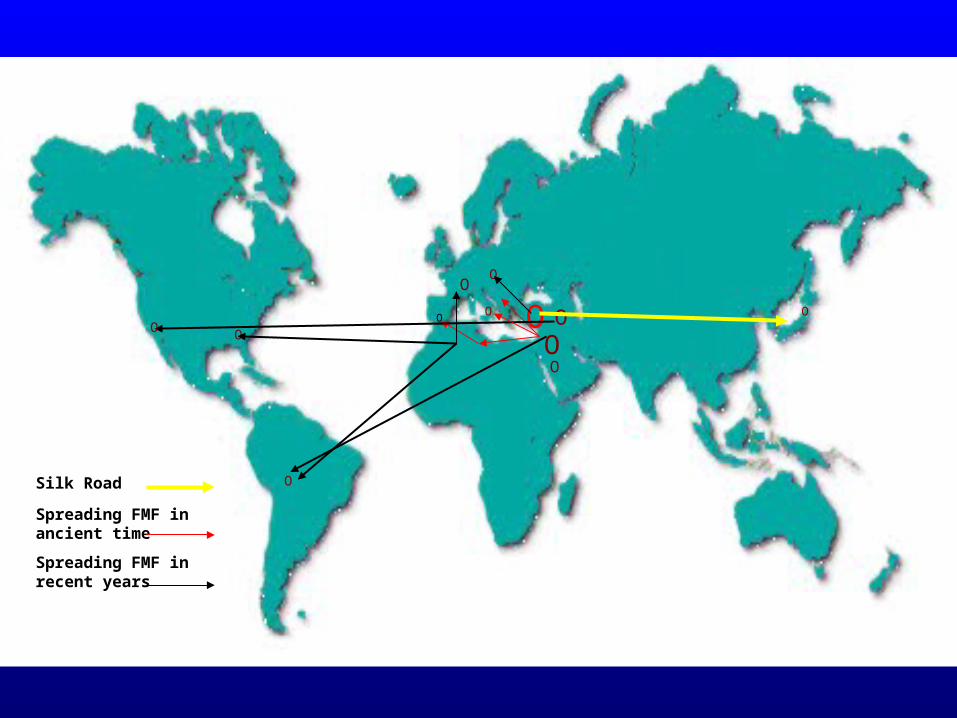
O
OO
O O
O
OO
O
O
OSilk Road Spreading FMF in ancient time
Spreading FMF in recent years
O
Phenotype-Genotype Correlation
• M694V is associated with more severe disease:
• Earlier onset• More arthritis• Higher dose of colchicine• Amyloidosis
TreatmentColchicine - is the drug of choice
since 1972.
Goldfinger, NEJMOzkan, Medical Bulletin of Istanbul
Mechanism of Action Colchicine Inhibits leukocytes
chemotaxis
• It may interfere microtubules function.
• It may affect the function of adhesion molecules on the surface of leukocytes and endothelial cells.
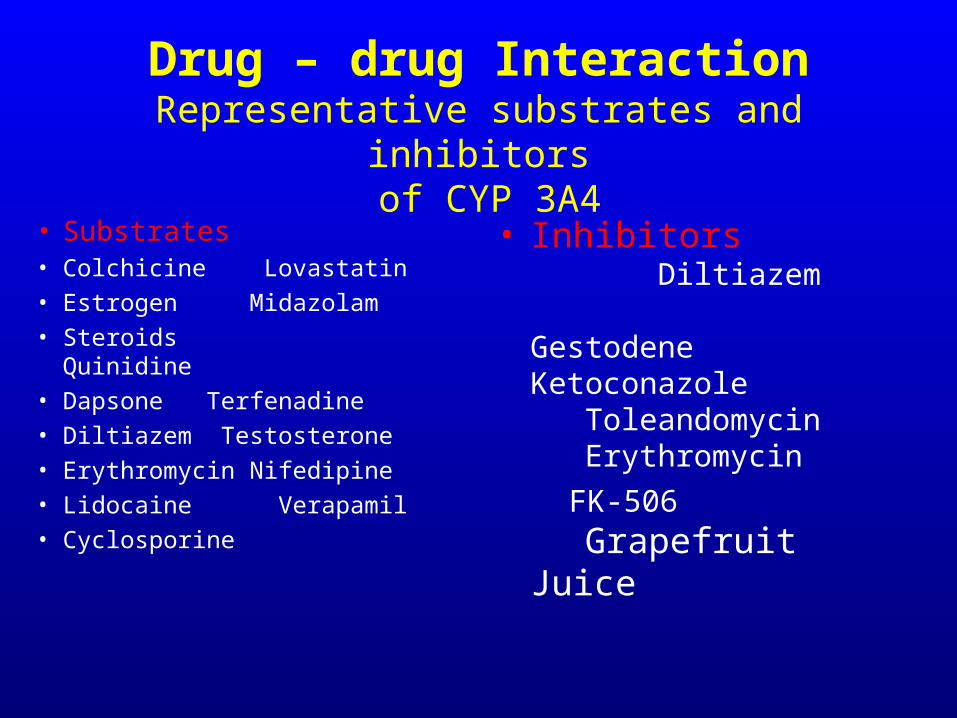
Drug – drug InteractionRepresentative substrates and inhibitors
of CYP 3A4
• Substrates • Colchicine Lovastatin• Estrogen Midazolam• Steroids Quinidine• Dapsone Terfenadine• Diltiazem Testosterone• Erythromycin
Nifedipine• Lidocaine Verapamil• Cyclosporine
• Inhibitors Diltiazem Gestodene Ketoconazole Toleandomycin Erythromycin
FK-506 Grapefruit Juice
Long-term colchicine treatment in childbearing
age
• Colchicine and male fertility• Colchicine and pregnancy• Colchicine and breast feeding• Colchicine and child growth
Colchicine and male fertility
Colchicine may cause oligo or azoospermia (very rarely in FMF and Gout, but relatively more frequently in Behcet’s syndrome).
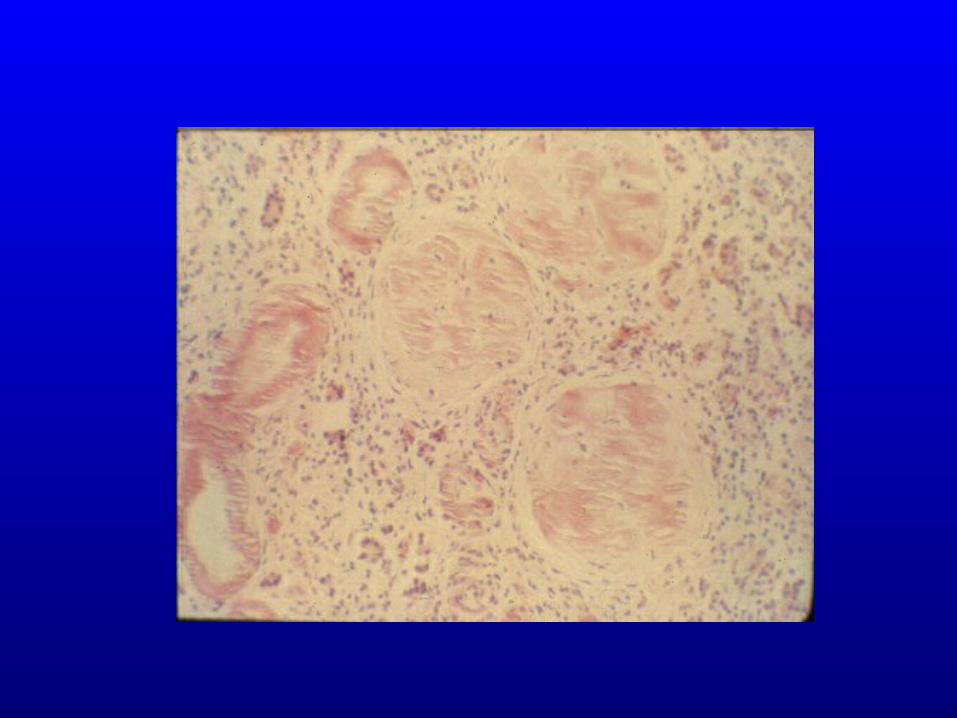
In some cases of azoospermia biopsies from
the testes disclosed amyloidosis
Can amyloidosis affect male fertility ?
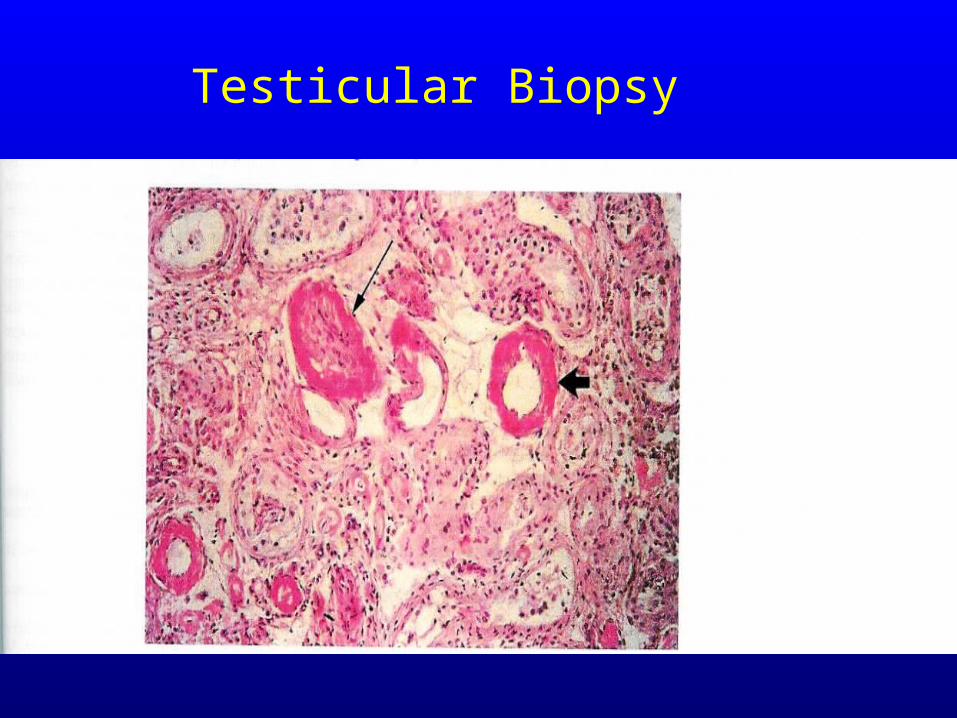
Testicular Biopsy
Long-term colchicine treatment in childbearing
age
• Colchicine and male fertility• Colchicine and pregnancy• Colchicine and breast feeding• Colchicine and child growth
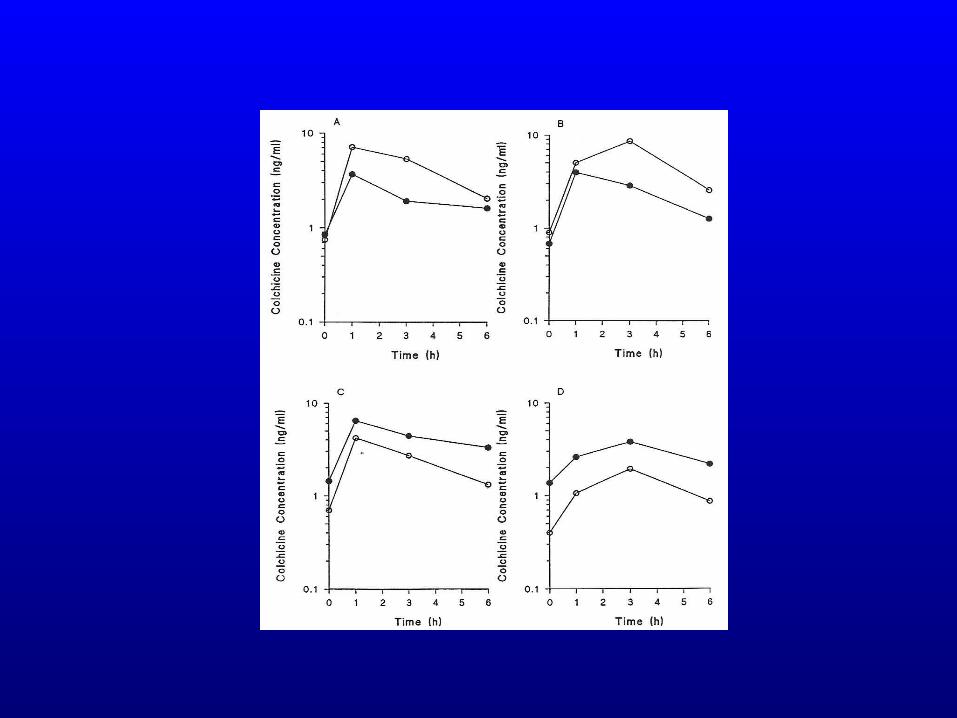
Conclusion:
Breast feeding is safe under colchicine treatment
Long-term colchicine treatment in childbearing
age
• Colchicine and male fertility• Colchicine and pregnancy• Colchicine and breast feeding• Colchicine and child growth
Long-term colchicine treatment in childbearing
age
• Colchicine and male fertility• Colchicine and pregnancy• Colchicine and breast feeding• Colchicine and child growth
Colchicine and pregnancy(Studied in FMF)
• Does not increase abortion rate• Normal pregnancy length• Normal birth weight• Normal outcome
• Amniocentesis ? No need E Ben-Chetrit et al.
AC&R 2011