Embed Size (px)
Citation preview

Br HIeart J 1988;60:247-51
Familial neurofibromatosis and hypertrophiccardiomyopathy
A P FITZPATRICK, R W EMANUEL
From the Cardiac Department, Westminster Hospital; and National Heart Hospital, London
SUMMARY Two siblings from a family in which neurofibromatosis was inherited as an autosomaldominant had hypertrophic cardiomyopathy and neurofibromatosis. Idiopathic hypertrophiccardiomyopathy may have occurred by chance in two first degree relatives with neurofibromatosis.An alternative explanation is that these diseases are both manifestations of a common hereditarydefect ofneural crest tissue. Another possibility is that abnormalities of catecholamine metabolismand nerve growth factor in neurofibromatosis can cause secondary ventricular hypertrophy withseptal involvement.
The aetiology of hypertrophic cardiomyopathy isunknown, although genetic factors are almost cer-tainly involved. In addition, there is increasingevidence, both clinical and experimental, of anabnormality of catecholamine metabolism. Reportsof abnormal catecholamine metabolism inneurofibromatosis have led to the suggestion thatthere is an aetiological link between the two diseases.
Case reports
CASE 1The index case (II.2, age 42) presented with exer-tional chest pain and a systolic murmur (figs 1 and2a). There was a past history of peptic ulceration.The resting electrocardiogram showed considerableleft ventricular hypertrophy. Cross sectional and Mmode echocardiography (fig 2b and c) showed hyper-trophic cardiomyopathy with asymmetric septalhypertrophy. The interventricular septum was 2-8cm thick, and the posterior left ventricular wall was1-2 cm thick. In systole there was pronouncedanterior motion ofthe mitral valve and obliteration ofthe left ventricular cavity. Cardiac catheterisationand angiography showed normal coronary arteries,and a left ventricular outflow gradient of 70mm Hg.Radionuclide ventriculography showed an ejection
Requests for reprints to Dr A P Fitzpatrick, Cardiac Department,Westminster Hospital, Dean Ryle Street, Horseferry Road, LondonSWlP 2AP.
Accepted for publication 26 April 1988
I(1 2)
II (1-3)
III (1-8)
IV (1-3)
Examined. * NF and HCM
e E NF, no HCMOL !Cafe au lait/NF,0 1 no HCM® Wo No NF, no HCM
/1 Propositus
Not examined - reported
JENFO [11 Cafe au lait/NF
0 D No NF
~0'JZf' Dead
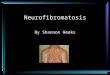
Fig 1 Thefamily pedigree.1.1 Father of propositus, known to have NF, died aged 64 ofcarcinoma of stomach; 1.2 mother of propositus, alive and well, aged74, no clinical evidence of NF or HCM; 11.1 sister of propositus,aged 49, classic NF and HCM; 11.2 propositus, classic NF andHCM, aged 47; I1.3 brother of propositus, known to have NF, aged46, refused examination; III.1 woman aged 26, known to have NF,refused examination; 111.2 woman aged 25, examined-normal;I11.3 man aged 19, classic NF, heart normal; III.4 woman aged 24,reported normal, refused examination; II1.5 girl aged 5, NF oftypical cafe au lait type, heart normal; III.6 boy aged 4, classic NF,heart normal; III.7 boy aged 9, reported NF, parents refusedpermission forexamination; III.8 girl aged 6, reportedNF (as III.7);IV.1 girl aged 7, reported NF of typical cafe au lait type (as III.7);IV.2 girl aged 4, normal at examination; IV.3 boy aged 3, reportednormal, refused examination. NF, neurofibromatosis; HCM, hyper-trophic cardiomyopathy.
247
on May 5, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.60.3.247 on 1 Septem
ber 1988. Dow
nloaded from

Fitzpatrick, Emanuel
RV
-- I RE-2- - -- "---- ,copy he- OPcR.. ItrX DCTCI 11-4-65 ID4 "09
~~~~ ~~~~~~~I II
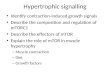
Fig 2 (a) Anterior view of chest in propositus showing multiple cutaneous neurofibromas. (b) Long axis, parasternal, crosssectional echocardiogram ofpropositus showing gross septal hypertrophy with typical echogenic appearance of the septalmyocardium. IVS, interventricular septum; LA, left atrium; LV, left ventricle; SAM, systolic anterior motion of the mitralvalve. (c) M mode echocardiographic recording showing gross thickening of the interventricular septum (IVS) and SAM.amvl, anterior mitral valve leaflet; PW, posterior wall of left ventricle.
fraction of 100 00 and typical features ofhypertrophiccardiomyopathy. Biopsy of the skin nodulesconfirmed neurofibromatosis. Concentrations ofplasma catecholamines and urinary catecholaminemetabolites were normal. Serum concentrations ofcalcium and fasting gastrin were also normal.
CASE 2The 46 year old sister of case 1 has severe kyphos-coliosis, large numbers of neurofibromas, and giantcafe au lait patches (fig 3a and b). Cardiovascularexamination and resting electrocardiography werenormal but the chest x ray showed a right paraver-tebral neurofibroma. Her thoracic deformity ham-pered echocardiography but an apical four chambercross sectional view showed evidence ofhypertrophic
cardiomyopathy (fig 3d and e) with subaortic septalhypertrophy. Cardiac catheterisation and angiogra-phy showed normal coronary arteries with a grosslyabnormal left ventriculogram. There was a"ballerina foot" deformity with mid-cavity oblitera-tion and an ejection fraction of 70" ,. No intracavitygradient was found. Left and right heart pressureswere normal. Concentrations of plasma cate-cholamines and urinary metabolites were normal.
THE FAMILYThe family consisted of the index case (II.2), six firstdegree, and nine second degree relatives. With theexception of the index case and his sister all thoseexamined had normal hearts. Four first degree and
248
on May 5, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.60.3.247 on 1 Septem
ber 1988. Dow
nloaded from

Familial neurofibromatosis and hypertrophic cardiomyopathy'F-
iI
zzt.-sia;M i 3 >~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
.>st, bt 1ts t-Ez ,, 1. . .wii -i I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I':§-c3r_ ~~~~~~A~~~~~~~~~~~~~~~~~~~~~~~~~~~~a-
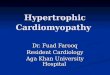
Fig 3 (a) Anterior view of case II showing typical cutaneous neurofibromas. (b) Lateral view of case II showing the severedegree of kyphoscoliosis. (c) Posterior anterior chest radiograph of case II showing the severity of her skeletal deformity and alarge neurofibroma in the right upper zone (arrows). (d) Apicalfive chamber cross sectional echocardiogram from case IIshowing pronounced subaortic hypertrophy of the septal myocardium (arrows). (e) Apicalfour chamber view in case IIshowing a pronounced septal bulge above the mitral valve. av, aortic valve; IVS, interventricular septum; LA, left atrium;LV, left ventricle; mv, mitral valve; RA, right atrium; R V, right ventricle; tv, tricuspid valve.
five second degree relatives had neurofibromatosis(see fig 1).
Discussion
Cross sectional echocardiography showed hypertro-phic cardiomyopathy in the index case (II.2, fig 2b)and his sister (II.1, fig 3d and e). Both had consider-able asymmetric hypertrophy of the interventricularseptum. There was evidence ofobstruction ofthe leftventricular outflow tract in case II.2 which wasconfirmed at catheterisation, but this feature was notpresent in his sister (II.1). Neurofibromatosis hasbeen misdiagnosed as lentiginosis.' Our diagnoseswere confirmed by biopsy of the skin nodules in case
I1.2 and by associated skeletal and dermatologicalfindings in his sister (II.1).Where neurofibromatosis is suspected in the
absence of skin nodules, the diagnosis may be madeby the finding of six or more cafe au lait skin patchesof > 1-5 cm2.2 Neurofibromatosis was diagnosed inthis way in cases III.5 and IV.1.The association between hypertrophic cardio-
myopathy and neurofibromatosis has already beenreported.'4 The cells responsible for the neuro-fibromas are of neural crest origin and it may berelevant that other neuro-ectodermal conditionshave been reported in association with hypertrophiccardiomyopathy. The best known ofthese is lentigin-osis,' where the melanocytes responsible for the
ll.t:N
249
on May 5, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.60.3.247 on 1 Septem
ber 1988. Dow
nloaded from

250
skin lesions arise from the neural crest. Two studieshave indicated that the association of hypertrophiccardiomyopathy and lentiginosis might be familialand autosomal dominant,67 but other family studieshave failed to confirm this.8 Hypertrophic car-diomyopathy has been described with phaeo-chromocytoma9 and parathyroid tumours.'° Symonset al have studied this association. They showed thatpatients with hypercalcaemia caused by hyper-parathyroidism may have asymmetric septal hyper-trophy, and also that normocalcaemic patients withhypertrophic cardiomyopathy have raised concen-trations of parathyroid hormone.'0 They also showedthat unexplained hypertrophy may also be found inthyrotoxicosis where sympathetic activity isincreased."' Tumours of the parathyroid, adrenalmedulla, and medullary cells of the thyroid (allof neuro-ectodermal origin), occur together in themultiple endocrine adenoma syndrome type II, orSipple's syndrome. This is often autosomal domin-ant" and has been reported in association withhypertrophic cardiomyopathy and with neuro-fibromatosis. Riccardi reported raised concentra-tions of catecholamines in neurofibromatosis. In atleast two cases no phaeochromocytoma could befound and neurofibromas were thought to be thesource.13There is increasing debate about the role of
catecholamines in hypertrophic cardiomyopathy.Dense sympathetic innervation and high tissue cate-cholamine concentrations in the septal myocardiumhave been reported.'4 Others have refuted this.'516The developing myocardium is known to be verysensitive to catecholamines, and in normal neonatescirculating concentrations are already high.Experimental work by Olsen et al has shed some lighton possible interactions in the developing myocar-dium. The administration of TRIAC (dieth-amolamine salt oftriiodothyronine), a triiodothyron-ine analogue, to pregnant rats produced widespreadcellular disarray resembling that seen in hypertro-phic cardiomyopathy. This reaction could beblocked by propranolol." Perloff suggested that apossible mechanism for the development of hyper-trophic cardiomyopathy is that catecholamine abnor-malities lead to cellular disarray. He postulated thatthe inherent isometric contraction ofmalaligned cellsis less effective and leads to secondary myocardialhypertrophy.'8 If Perloffs theory is correct myocar-dial disarray with subsequent hypertrophy could be asecondary phenomenon in neurofibromatosis if cate-cholamine concentrations are abnormal during earlydevelopment when the septum is known to behypersensitive.
Other hormonal mechanisms may be involved.Nerve growth factor is a naturally occurring
Fitzpatrick, Emanuelglycoprotein required for growth and maintenance ofsympathetic and sensory neurones.'9 Abnormalmetabolism of this substance is thought to be a factorin the pathogenesis of neurofibromatosis anddifferent forms of the disease are distinguishable bythe circulating concentrations of nerve growth fac-tor.20 Whereas sensory ganglia respond only duringembryogenesis, when the influence of nerve growthfactor is greatest, mature sympathetic neuronesremain responsive to this factor.'9 Imbalance of thedelicate interaction between developing myocar-dium, sympathetic innervation, catecholamines, andnerve growth factor has been proposed as a model forthe pathogenesis of hypertrophic cardiomyopathy.'8We found hypertrophic cardiomyopathy and
neurofibromatosis in two siblings. There are threepossible explanations for this. Firstly, the two dis-eases could have appeared together by chance,although this seems unlikely. Both are relativelycommon conditions with a similar incidence, about1:3000,'3 2 although this figure is less certain in thecase of hypertrophic cardiomyopathy.2" Secondly,left ventricular hypertrophy may be secondary toneurofibromatosis, perhaps as a result of abnormalmetabolism of catecholamines or nerve growthfactor. Thirdly, both diseases could be commonmanifestations of a defect of neural crest tissue withautosomal dominant inheritance.The known coincidence of hypertrophic car-
diomyopathy with conditions such as lentiginosisand hyperparathyroidism argues in favour of a com-mon defect of the neural crest. This seems moreplausible than secondary left ventricular hypertro-phy in the presence of an abnormality of cate-cholamines or nerve growth factor, which mayoccur in neurofibromatosis. Furthermore, neuro-fibromatosis is independently associated with hyper-parathyroidism and with Sipple's syndrome,'3 andthe pattern ofasymmetric septal hypertrophy seen inthese two cases is indistinguishable from that seen inidiopathic hypertrophic cardiomyopathy.There is circumstantial evidence suggesting a link
between neurofibromatosis and hypertrophic car-diomyopathy. Abnormalities of catecholaminemetabolism, sympathetic innervation, and nervegrowth factor may account for the development ofidiopathic left ventricular hypertrophy in certainsubjects with neurofibromatosis. An alternativeexplanation, supported by the known association ofboth conditions with other diseases of neural crestorigin, is that they are genetically linked. Thesequence containing the gene for neurofibromatosishas recently been located by linkage analysis topolymorphic markers on chromosome 17.23 Wespeculate that this could lead to the identification of agenetic marker for hypertrophic cardiomyopathy.
on May 5, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.60.3.247 on 1 Septem
ber 1988. Dow
nloaded from

Familial neurofibromatosis and hypertrophic cardiomyopathy 251
We thank Caroline Westgate for the echocardiogra-phy.
References
1 Somerville J, Bonham-Carter RE. The heart in len-tiginosis. Br Heart J 1972;34:58-66.
2 Crowe FW, Schull WJ, Neel JV. A clinical, pathologicaland genetic study of multiple neurofibromatosis.Springfield, Illinois: Charles C Thomas, 1956.
3 Elliott CM, Tajik AJ, Giuliani ER, Gordon H.Idiopathic hypertrophic subaortic stenosis associatedwith cutaneous neurofibromatosis: report of a case.Am Heart J 1976;92:368-72.
4 Sachs RN, Buschauer-Bonnet Ch, Kemeny JL,Amouroux J, Lanfranchi J. Myocardiopathie hyper-trophique et maladie de von Recklinghausen. RevMed Interne 1984;5:154-6.
5 Polani PE, Moynahan EJ. Progressive cardiomyopathiclentiginosis. Q J Med 1972;41:205-25.
6 Hopkins BE, Taylor RR, Robinson JS. Familial hyper-trophic cardiomyopathy and lentiginosis. Aust NZ JMed 1975;5:359-64
7 Cronje RE, Feinberg A. Lentiginosis, deafness andcardiac abnormalities. S Afr Med J 1973;47:15-7.
8 Sutton MG St-J, Talik AJ, Giuliani ER, Gordon H, SuWPD. Hypertrophic obstructive cardiomyopathyand lentiginosis: a little known neural ectodermalsyndrome. Am J Cardiol 1981;47:214-7.
9 Goodwin JF. Prospects and predictions for thecardiomyopathies. Circulation 1974;50:210-9.
10 Symons C, Fortune F, Greenbaum RA, Dandona P.Cardiac hypertrophy, hypertrophic cardiomyopathy,and hyperparathyroidism-an association. Br Heart J1985;54:539-42.
11 Symons C, Richardson PJ, Feizi 0. Hypertrophiccardiomyopathy and hyperparathyroidism: a report
of threetases. Thorax 1974;29:713-9.12 Keiser HR, Beavens MA, Doppman J, Wells S, Bunja
LM. Sipple's syndrome: medullary thyroid carcin-oma, phaeochromocytoma and parathyroid disease.Ann Intern Med 1973;78:561-5.
13 Riccardi VM. Von Recklinghausen neurofibromatosis.NEngl J Med 1981;305:1617-22.
14 Pearse AGE. The histochemistry and electron micro-scopy of obstructive cardiomyopathy. In: Wolsten-holme GEW, O'Connor M, eds. Ciba Foundationsymposium on cardiomyopathies. Boston: Little Brown,1964:132-64.
15 McCallister BD, Brown AL. Fine structure study ofidiopathic hypertrophic subaortic stenosis. Am JCardiol 1967;19:142-6.
16 Van Noorden S, Olsen EG, Pearse AGE. Hypertrophicobstructive cardiomyopathy. A histological, histo-chemical and ultrastructural study of biopsy material.Cardiovasc Res 1971;5:118-31.
17 Olsen EGJ, Symons C, Hawkey C. Effect ofTRIAC onthe developing heart. Lancet 1977;ii:221-3.
18 Perloff JK. Pathogenesis of hypertrophic car-diomyopathy: hypotheses and speculations. AmHeart J 1981;101:219-26.
19 Mobley WC, Server AC, Ishii DN, Riopelle RJ,Shooter EM. Nerve growth factor. N Engi J Med1977;297:1096-104.
20 Rubenstein AE, Revoltella RP, Eldridge R. Humannerve growth factor in neurofibromatosis [Abstract].Child Neurolog Soc 1979:137.
21 Bjarnason I, Jonsson S, Hardarson T. Mode ofinheritance of hypertrophic cardiomyopathy inIceland. Echocardiographic study. Br Heart J1982;47:122-9.
22 Burn J. The genetics of hypertrophic cardiomyopathy.Int J Cardiol 1985;7:135-8.
23 Barker D, Wright E, Nyugen K, et al. Gene for vonRecklinghausen is in the pericentromeric region ofchromosome 17. Science 1987;236:1100-2.
on May 5, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.60.3.247 on 1 Septem
ber 1988. Dow
nloaded from



![Cranial MR Imaging in Neurofibromatosis · bromatosis), neurofibromatosis II (bilateral acoustic neurofibromatosis), and other forms [5, 6]. Neuroradiology has traditionally played](https://img.pdfslide.net/doc/110x75/5ed593375be95c6187174771/cranial-mr-imaging-in-bromatosis-neurofibromatosis-ii-bilateral-acoustic-neurofibromatosis.jpg)