Embed Size (px)
Citation preview
Familial oligoasthenoteratozoospermia:evidence of autosomal dominantinheritance with sex-limited expression
Joep H. A. M. Tuerlings, M.D., Ph.D.,a Ron J. T. van Golde, M.D.,b
Astrid R. Oudakker, M.Sc.,a Helger G. Yntema, Ph.D.,a andJan A. M. Kremer, M.D., Ph.D.b
University Medical Centre Nijmegen, Nijmegen, The Netherlands
Objective: To report the familial occurrence of severe oligoasthenoteratozoospermia in a man and five malerelatives related through their mothers.
Design: Case report.
Setting: University medical center.
Patient(s): Six affected family members.
Main Outcome Measure(s): Blood and semen samples were collected from all affected males and some oftheir healthy male relatives. Pedigree analysis and exclusion of X-linked disorder were done.
Result(s): Analysis suggested that familial nonsyndromic male factor infertility was present.
Conclusion(s): The family described in this report suggests the existence of an autosomal dominant trait ofmale infertility with sex-limited expression. (Fertil Steril� 2002;77:415–8. ©2002 by American Society forReproductive Medicine.)
Key Words: Oligoasthenoteratozoospermia, familial, inheritance, autosomal dominant
Severe oligoasthenoteratozoospermia (OAT),defined as �1 � 106 spermatozoa/mL plus pro-gressive motility per ejaculate and azoosper-mia, are rare disorders in otherwise healthymen. The estimated prevalence is approxi-mately 0.3% in all men (1). In most men withseverely abnormal semen variables, the etiol-ogy remains obscure, but genetic factors arethought to play an important role (2).
The current lack of knowledge about thegenetic factors involved in spermatogenesis isa source of concern, these unknown factorsmay be transmitted to offspring during ICSI.Large-scale family studies in defined groupsthat might reveal these genetic factors arescarce (3, 4). Results of these studies and casereports of infertile brothers all suggest thatautosomal recessive mutations might accountfor many cases of undiagnosed male infertility(3–5). Little is currently known about autoso-mal dominant or X-linked factors involved innonsyndromic male infertility.
We describe a family in which several third-
degree male relatives have idiopathic severeOAT. The mothers of these men are sisters(Fig. 1).
MATERIALS AND METHODS
The proband of the family presented to thefertility clinic of the University Medical CentreNijmegen with primary infertility. A familyhistory was obtained by interview, and familymembers were invited for evaluation of theirfertility status, including andrologic examina-tion, karyotyping, and screening for microde-letions of the Y chromosome (6). After in-formed consent was obtained, blood sampleswere taken for molecular research purposes.
The DNA from peripheral lymphocytes wasisolated according to the procedure of Miller etal. (7). The family was screened for linkagewith the X-chromosomal markers of the ABIPRISM Linkage Mapping Set, version 2 (Ap-plied Biosystems, Nieuwekerk a/ol Yssel, TheNetherlands). These markers were selectedfrom the Genethon human linkage map (8) and
Received May 21, 2001;revised and acceptedOctober 10, 2001.Reprint requests: JoepH. A. M. Tuerlings, M.D.,Ph.D., Department ofHuman Genetics,University Medical CentreNijmegen, P.O. Box 9101,6500 HB Nijmegen, TheNetherlands (FAX: 31-24-356-5026; E-mail: [email protected]).a Department of HumanGenetics.b Department of Obstetricsand Gynaecology.
FERTILITY AND STERILITY�VOL. 77, NO. 2, FEBRUARY 2002Copyright ©2002 American Society for Reproductive MedicinePublished by Elsevier Science Inc.Printed on acid-free paper in U.S.A.
0015-0282/02/$22.00PII S0015-0282(01)02996-X
415
are spaced every 10 cM, on average. Approval of the insti-tutional human investigation review board was obtained.
RESULTS
Case 1The proband (III-5; Fig. 1), now 33 years of age, is the
third child of nonconsanguineous healthy Dutch parents. Hehas two healthy brothers. At 5 years of age, he underwentsurgery for torsion of a testicle. The proband has epilepsy,for which he uses antiepileptic medicine.
The proband and his wife presented at our clinic with ahistory of primary infertility for 3 years. His infertility wasevaluated at 30 years of age. Semen analysis revealed severeOAT (3.0 � 106 spermatozoa/mL); andrologic examinationshowed no additional abnormalities. His hormonal valueswere within the range of normal. His karyotype was normal,
and Y-chromosomal microdeletion screening did not revealabnormalities. The family history was positive for maleinfertility.
Case 2Family member III-7 is a third-degree relative of the
proband (III-5). He is 45 years of age. His parents arenonconsanguineous and he has one sister, three healthybrothers, and a fourth brother who also experienced infertil-ity. Family member III-9 and his 45-year-old wife remainedchildless against their wishes. They first attended our clinicin 1980.
All semen variables in III-7 have been consistently im-paired (0.6 � 106 spermatozoa/mL) since his initial presen-tation. Andrologic history included surgical correction of avaricocele. Results of andrologic examination, includinghormonal profile, karyotyping, and screening for microdele-
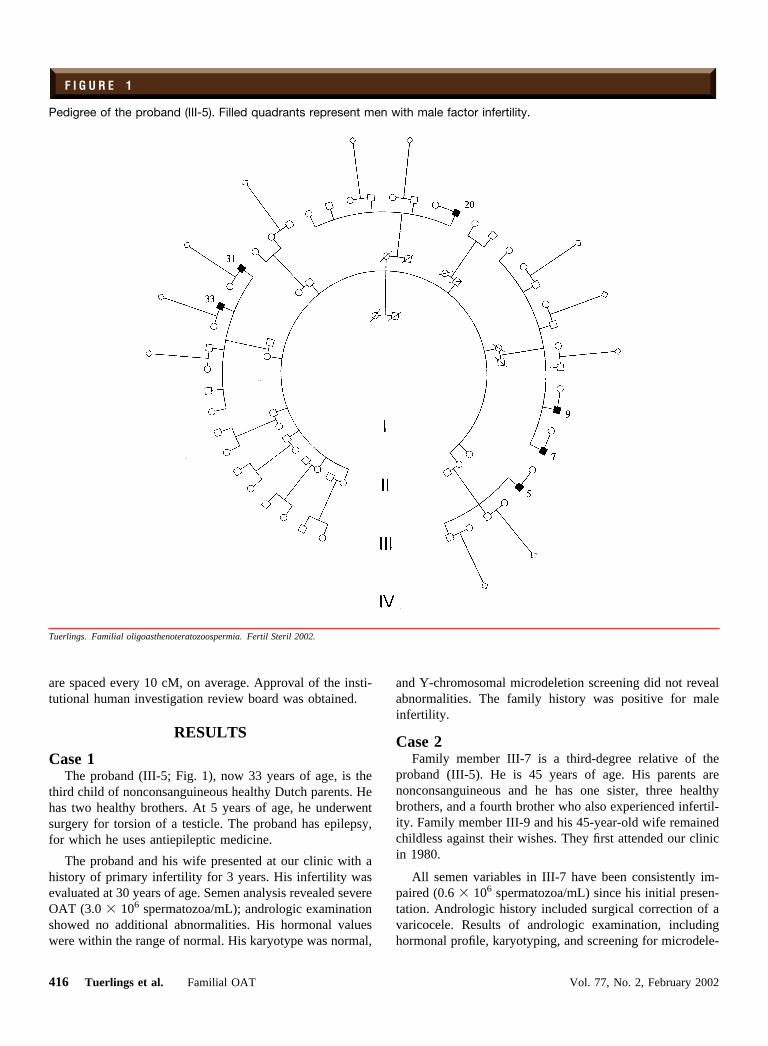
F I G U R E 1
Pedigree of the proband (III-5). Filled quadrants represent men with male factor infertility.
Tuerlings. Familial oligoasthenoteratozoospermia. Fertil Steril 2002.
416 Tuerlings et al. Familial OAT Vol. 77, No. 2, February 2002

tions of the Y chromosome, revealed no additional abnor-malities.
Case 3This 43-year-old man (III-9) is the brother of case 2
(III-7). He and his 43-year-old female partner had experi-enced primary infertility for years. Andrologic history re-vealed no abnormalities except for severely impaired semenvariables. This couple remained childless involuntarily, andthey experienced their childlessness as a great burden. Re-cent semen analysis confirmed earlier results (0.1 � 106
spermatozoa/mL). The karyotype was 46,XY. Screening forY chromosome microdeletions revealed an AZFc deletion.
Case 4Case 4 is a 43-year-old third-degree relative (III-20) of
case 1. His parents are nonconsanguineous, and he has threehealthy brothers and a sister. He and his 42-year-old femalepartner had experienced primary infertility for many years.Their medical doctor informed them that they would not beable to conceive.
Andrologic history revealed surgical correction of aninguinal hernia at 5 years of age. Andrologic examinationshowed nonobstructive azoospermia: Both testicles have asmall volume, the volume of ejaculate was normal, and theserum FSH level was high. The karyotype was 46,XY, andscreening for microdeletions of the Y chromosome revealedabnormalities.
Case 5Case 5 is a male third-degree relative of case 1 (III-31)
who has primary infertility. He is 44 years of age, and hisparents are nonconsanguineous. He has four sisters, twounaffected brothers, and one brother with infertility. He hadsurgical correction of a varicocele, but his semen variablesremained impaired (10 � 106 spermatozoa/mL). Andrologichistory and examination showed no additional abnormalities.The karyotype is 46,XY, and no microdeletions of the Ychromosome were detected.
Case 6Case 6, the brother of case 5, is a 43-year-old man (III-33)
with severely impaired sperm variables. Andrologic historyshowed torsion of the right testicle, impaired semen vari-ables (0.1 � 106 spermatozoa/mL) and an increased serumconcentration of FSH. The karyotype is 46,XY, and nomicrodeletions of the Y chromosome were detected.
Relative III-24 and his wife experienced primary infertil-ity for 8 years because of presumed female factor. After IVF,they conceived female twins, now 5 years of age. The semenvariables at the time of IVF were reported to be within thenormal range. No other male relatives in this family reportedfertility disorders. Some of the male relatives who did notreport a fertility disorder agreed to have andrologic evalua-tion (III-1, III-11, III-13, III-15, III-24, and III-35; Fig. 1).
Examination of these healthy fertile men revealed no abnor-malities except for a variocele in III-35.
Routine fertility screening of the partners of the affectedmen revealed no abnormalities. No female family membershave reported fertility disorders, and no developmental dis-orders or malformations have been reported in this family.
DNA AnalysisNo markers of the X chromosome segregated with the
disease in the family.
DISCUSSION
We observed a family with a cluster of male relatives whohave severe OAT or azoospermia. The heterogeneity of theandrology-related diagnosis in this family might indicate thatthe fertility problems in this family are not due to a singledisorder. However, except for the one man with an AZFcmicrodeletion, chance alone probably does not explain thiscluster of men with severe OAT or azoospermia (probabilityof 2 � 10�6). Molecular analysis with X-linked markersshows that the impaired spermatogenesis in this pedigree isnot due to an X-linked disorder. Therefore, although a mul-tifactorial etiology cannot be excluded completely, the ped-igree suggests the existence of an autosomal dominant traitfor a disorder with severely impaired spermatogenesis.
Reports of familial nonsyndromic male factor infertilitysuggest that inheritable male factor infertility results fromautosomal recessive disorders (3–5). However, it seemslikely that autosomal dominant or X-linked male factor in-fertility also exist. The ectrodactyly, ectodermal dysplasiaand cleft lip-palate syndrome; myotonic dystrophy; the Kall-mann syndrome; and the Aarskog syndrome are associatedwith male factor syndrome infertility and have an autosomaldominant or X-linked inheritance. In 1979, Chaganti andGerman reported on a man with nonsyndromic infertilitywho had an infertile maternal uncle and whose maternalsister had an infertile son (9). They postulated that a gene formeiotic disturbance is segregating in their family. Amongpatients undergoing ICSI, we have observed some smallfamilies in which brothers, maternal uncles, and sons ofmaternal sisters have nonsyndromic male factor infertility(unpublished data). In addition, the large family presentedhere has widespread nonsyndromic male factor infertility.
In conclusion, the family discussed here may show anautosomal dominant factor of male infertility with sex-lim-ited expression. Further molecular research, especiallygenomic wide screening for linkage, in this family and othersmay reveal the genes involved. We believe that the familyhistory of infertile males should not be limited to first-degreerelatives but should also include questions about the fertilityof all second- and third-degree relatives.
References1. Kremer JAM, Tuerlings JHAM, Borm G, Hoefsloot LH, Meuleman EHJ,
Braat DDM, et al. Does ICSI lead to a rise in the frequency of microde-
FERTILITY & STERILITY� 417

letions in the AZF region of the Y chromosome in future generations?Hum Reprod 1997;12:687–91.
2. De Kretser DM. Male infertility. Lancet 1997;349:787–90.3. Budde WJ, Verjaal M, Hamerlynck JV, Bobrow M. Familial occurrence of
azoospermia and extreme oligozoospermia. Clin Genet 1984;26:555–62.4. Lilford R, Jones AM, Timothy O, Thornton J, Mueller R. Case-control
study whether subfertility is familial. BMJ 1994;309:570–3.5. Meschede D, Lemcke B, Behre HM, De Geyter CH, Nieschlag E, Horst
J. Clustering of male infertility in the families of couples treated withintracytoplasmic sperm injection. Hum Reprod 2000;15:1604–8.
6. Hoefsloot LH, Tuerlings JHAM, Kremer JAM, Meuleman EJH. PCR
analysis of Y chromosome deletions in subfertile men. Lancet 1997;349:1400.
7. Miller SA, Dykes DD, Polesky HF. A simple salting out procedure forextracting DNA from human nucleated cells. Nucl Acids Res 1988;16:1215.
8. Dib C, Faure S, Fizames C, Samson D, Drouot N, Vignal A, et al. Acomprehensive genetic map of the human genome based on 5,264microsatellites. Nature 1996;380:152–4.
9. Chaganti RSK, German J. Human male infertility, probably geneticallydetermined, due to defective meiosis and spermatogenetic arrest. Am JHum Genet 1979;31:634–41.
418 Tuerlings et al. Familial OAT Vol. 77, No. 2, February 2002













![Autosomal recessive ichthyosis with limb reduction defect ... · including autosomal dominant, autosomal recessive and X-linked inheritance [1,2]. Associated cutaneous and extracutaneous](https://img.pdfslide.net/doc/110x75/5ec8c9b91adfdf12ab3e663c/autosomal-recessive-ichthyosis-with-limb-reduction-defect-including-autosomal.jpg)