Embed Size (px)
Citation preview

Familial risks for colorectal cancer show evidence on recessive inheritance
Kari Hemminki1,2* and Bowang Chen
1
1Division of Molecular Genetic Epidemiology, German Cancer Research Center, Heidelberg, Germany2Department of Biosciences at Novum, Karolinska Institute, Huddinge, Sweden
Recent molecular genetic data have become available on a reces-sive inheritance in colorectal cancer (CRC). We wanted to searchfor evidence for recessive inheritance from a population-basedfamily data set, which is not sensitive to reporting or ascertain-ment bias. The nationwide Swedish Family-Cancer Database cov-ered 10.3 million individuals whose invasive CRCs ofadenocarcinoma histology were followed from 1991 to 2000. Ageof the offspring and parental populations was limited to less than69 years. Standardized incidence ratios (SIRs) were calculated forsite-specific CRC in offspring whose parents or siblings were diag-nosed with CRC. A total of 6,774 offspring were recorded withCRC, whose risk was 2.13 when a parent was diagnosed with CRCand it was 2.75 when a sibling was affected. The SIRs for right-sided colon cancer were 7.53 among siblings and 3.66 among off-spring of affected parents, giving a 1.8-fold excess familial riskamong siblings. Colon cancer among the 0- to 68-year-old popula-tion accounted for about 25% of all colon cancers. Examination ofall cancers in family members of the affected siblings did notreveal large contribution by known syndromes, such as hereditarynonpolyposis colorectal cancer. The most likely explanation to thehigh risk of right-sided colon cancer among siblings is a recessiveinheritance, which would account for 0.75% of all CRCs. Its highprevalence and predilection to right-sided colon suggest that onlya small proportion of this familial aggregation could be due toMYH mutations.' 2005 Wiley-Liss, Inc.
Key words: familial risk; sibling risk; colorectal cancer; right-sidedcolon cancer; adenocarcinoma
The importance of family history for colorectal cancer (CRC)has been shown in numerous epidemiologic studies.1–4 The mostcommon Mendelian condition, hereditary nonpolyposis colorectalcancer (HNPCC), features a relatively early onset (average,45 years) and preferential involvement of the right-sided colon.1 Ithas been estimated to account for 3% of all CRC in Finland5,6 andaround 1% in Sweden and the United States,7–9 the variationdepending on many parameters, including the age structure of thestudied population and the existence of founder mutations. Fami-lial adenomatous polyposis (FAP), Peutz-Jeghers syndrome, fami-lial juvenile polyposis and Cowden’s disease are other syndromesin which CRC may be a manifestation.1,10–12 All these Mendelianconditions follow a dominant mode of inheritance at the popula-tion level, although at the cellular level they require inactivationof both alleles of the relevant genes, typical of tumor suppressorgenes; the inactivation of the second allele is a somatic event.Recent data show that biallelic germline mutations in the MYHgene also increase the risk of CRC, typical of a recessive condi-tion. Biallelic mutations have been detected in about 0.5% of thescreened CRC patients and in a higher percentage of polyposispatients.13–16 Few late-onset recessive cancers are known at anysite, probably because these conditions are difficult to recognizeclinically. Unbiased population level data would be required forthe estimation of the prevalence of recessive conditions in CRC orin other cancers.
A recessive condition would be indicated if cancer risksbetween siblings of unaffected parents were higher than thosebetween offspring and parents, assuming that environmentalcauses of familial aggregation can be excluded, which appears tobe the cases for CRC; the familial clustering of CRC is mainlydue to heritable causes.17 The literature on familial CRC has beenreviewed until year 2000, and no higher overall familial risks havebeen noted for siblings than for offspring and parents.3 However,
the authors point out that the largest study of their review, withmedically verified data on cases and probands, did find a signifi-cantly higher risk for siblings than for offspring of affectedparents.18 In the present study, we examine specifically the ques-tion about a recessive inheritance in CRC, using the updatednationwide Swedish Family-Cancer Database.19 The Database isthe largest of its kind in the world and the unique aspects are prac-tically complete coverage, registered family relationships andfully medically verified diagnoses of all cancers. Other advantagesof the present study compared to the previous ones are large popu-lation size, adherence specifically to adenocarcinoma and consid-eration of colonic subsites and different probands. Thecombination of these features have never been covered before in aprevious family study on CRC, including previous ones from theDatabase.8,18,20–23
Material and methods
The Swedish Family-Cancer Database includes all persons bornin Sweden after 1931 with their biologic parents, totaling over 10.3million individuals.19 The offspring population included 6.86 mil-lion individuals. Cancers were retrieved from the nationwide Swed-ish Cancer Registry from 1958 to 2000. Family history informationwas collected on all first-degree relatives (parents, siblings and chil-dren). Follow-up of offspring was started on 1 January 1991 andterminated on death, emigration, or the closing data of the study(31 December 2000), whichever came first. A parental probandcould be diagnosed between 1991 and 2000. The Family-CancerDatabase has some gaps in parent-offspring links among those bornbetween 1932 and 1940 who died between 1960 and 1991. How-ever because the current follow-up was started from 1991, the lack-ing parental links due to mortality from cancer should not bias thepresent estimates. A 4-digit diagnostic code according to the 7thversion of the International Classification of Disease (ICD-7) wasused. ICD codes 153.0 to 153.3 and 154.0 were used for CRC.Based on the codes, the anatomical location of colon was classifiedas right-sided sections (codes 153.0 and 153.1) and left-sided sec-tions (codes 153.2 and 153.3). The splenic flexure was the dividingline between the left and right locations. Colon cancers of unknownanatomical site were not classified by subsite. The histologic classi-fication of CRC was used to define adenocarcinoma as a pathologicanatomic diagnosis (PAD) code 096; only CRC with adenocarci-noma histology was considered. Because we only covered adeno-carcinoma histology, the term ‘‘CRC’’ later in the text refers toCRC with this histology only. The percentage of cytologically orhistologically verified cases by site, sex and age at diagnosis forcolon cancer was 98% and for rectal cancer 99%.
The maximal age in the offspring population was 68 years; forcomparability, we also limited the age of the parental populationto 68 years. Siblings were defined as the offspring of a common
Grant sponsor: the Deutsche Krebshilfe; Grant sponsor: the SwedishCancer Society.*Correspondence to: Division of Molecular Genetic Epidemiology,
German Cancer Research Center, Im Neuenheimer Feld 580, 69120Heidelberg, Germany. Fax: þ49-62-21-42-1810.E-mail: [email protected] 30 August 2004; Accepted after revision 17 December 2004DOI 10.1002/ijc.20938Published online 9 February 2005 in Wiley InterScience (www.
interscience.wiley.com).
Int. J. Cancer: 115, 835–838 (2005)' 2005 Wiley-Liss, Inc.
Publication of the International Union Against Cancer
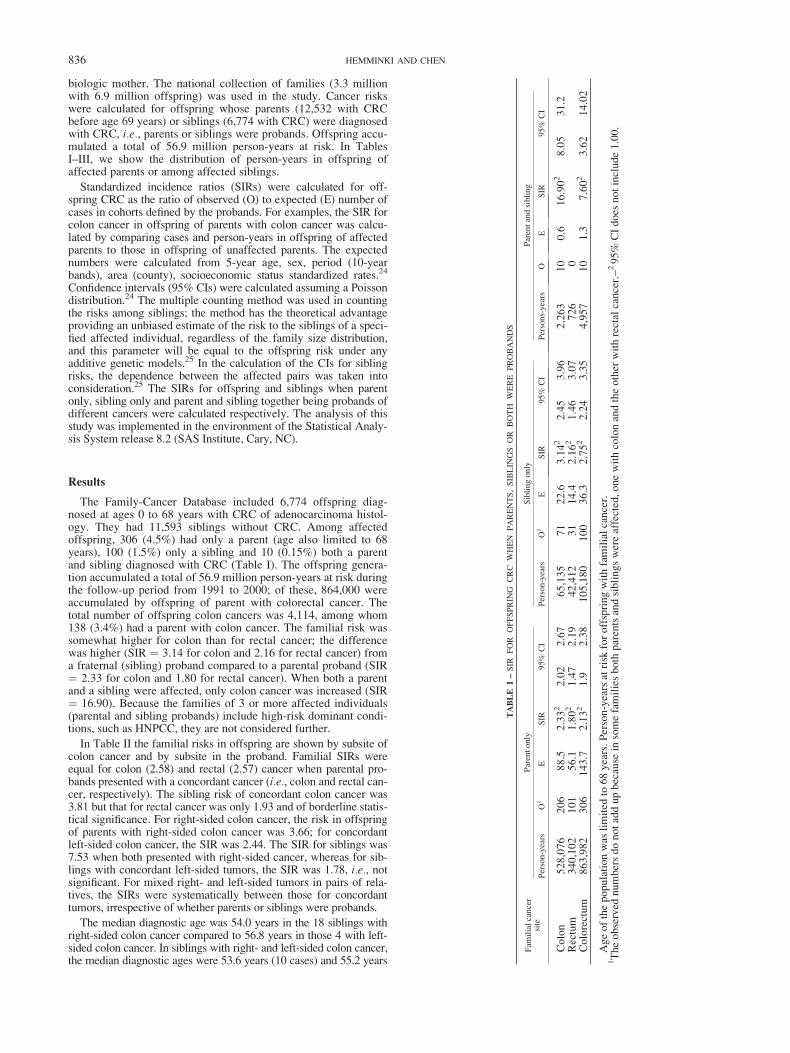
biologic mother. The national collection of families (3.3 millionwith 6.9 million offspring) was used in the study. Cancer riskswere calculated for offspring whose parents (12,532 with CRCbefore age 69 years) or siblings (6,774 with CRC) were diagnosedwith CRC, i.e., parents or siblings were probands. Offspring accu-mulated a total of 56.9 million person-years at risk. In TablesI–III, we show the distribution of person-years in offspring ofaffected parents or among affected siblings.
Standardized incidence ratios (SIRs) were calculated for off-spring CRC as the ratio of observed (O) to expected (E) number ofcases in cohorts defined by the probands. For examples, the SIR forcolon cancer in offspring of parents with colon cancer was calcu-lated by comparing cases and person-years in offspring of affectedparents to those in offspring of unaffected parents. The expectednumbers were calculated from 5-year age, sex, period (10-yearbands), area (county), socioeconomic status standardized rates.24
Confidence intervals (95% CIs) were calculated assuming a Poissondistribution.24 The multiple counting method was used in countingthe risks among siblings; the method has the theoretical advantageproviding an unbiased estimate of the risk to the siblings of a speci-fied affected individual, regardless of the family size distribution,and this parameter will be equal to the offspring risk under anyadditive genetic models.25 In the calculation of the CIs for siblingrisks, the dependence between the affected pairs was taken intoconsideration.25 The SIRs for offspring and siblings when parentonly, sibling only and parent and sibling together being probands ofdifferent cancers were calculated respectively. The analysis of thisstudy was implemented in the environment of the Statistical Analy-sis System release 8.2 (SAS Institute, Cary, NC).
Results
The Family-Cancer Database included 6,774 offspring diag-nosed at ages 0 to 68 years with CRC of adenocarcinoma histol-ogy. They had 11,593 siblings without CRC. Among affectedoffspring, 306 (4.5%) had only a parent (age also limited to 68years), 100 (1.5%) only a sibling and 10 (0.15%) both a parentand sibling diagnosed with CRC (Table I). The offspring genera-tion accumulated a total of 56.9 million person-years at risk duringthe follow-up period from 1991 to 2000; of these, 864,000 wereaccumulated by offspring of parent with colorectal cancer. Thetotal number of offspring colon cancers was 4,114, among whom138 (3.4%) had a parent with colon cancer. The familial risk wassomewhat higher for colon than for rectal cancer; the differencewas higher (SIR ¼ 3.14 for colon and 2.16 for rectal cancer) froma fraternal (sibling) proband compared to a parental proband (SIR¼ 2.33 for colon and 1.80 for rectal cancer). When both a parentand a sibling were affected, only colon cancer was increased (SIR¼ 16.90). Because the families of 3 or more affected individuals(parental and sibling probands) include high-risk dominant condi-tions, such as HNPCC, they are not considered further.
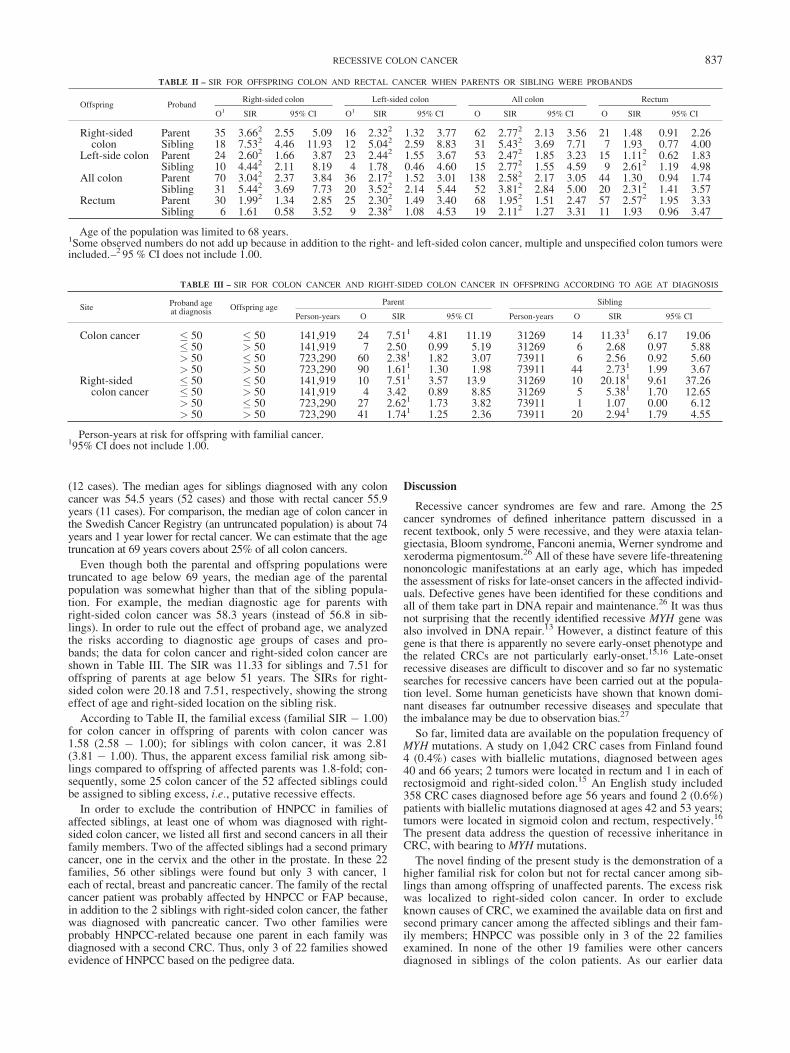
In Table II the familial risks in offspring are shown by subsite ofcolon cancer and by subsite in the proband. Familial SIRs wereequal for colon (2.58) and rectal (2.57) cancer when parental pro-bands presented with a concordant cancer (i.e., colon and rectal can-cer, respectively). The sibling risk of concordant colon cancer was3.81 but that for rectal cancer was only 1.93 and of borderline statis-tical significance. For right-sided colon cancer, the risk in offspringof parents with right-sided colon cancer was 3.66; for concordantleft-sided colon cancer, the SIR was 2.44. The SIR for siblings was7.53 when both presented with right-sided cancer, whereas for sib-lings with concordant left-sided tumors, the SIR was 1.78, i.e., notsignificant. For mixed right- and left-sided tumors in pairs of rela-tives, the SIRs were systematically between those for concordanttumors, irrespective of whether parents or siblings were probands.
The median diagnostic age was 54.0 years in the 18 siblings withright-sided colon cancer compared to 56.8 years in those 4 with left-sided colon cancer. In siblings with right- and left-sided colon cancer,the median diagnostic ages were 53.6 years (10 cases) and 55.2 years
TABLE
I–SIR
FOR
OFFSPRIN
GCRC
WHEN
PARENTS,SIBLIN
GS
OR
BOTH
WERE
PROBANDS
Fam
ilialcancer
site
Parentonly
Siblingonly
Parentandsibling
Person-years
O1
ESIR
95%
CI
Person-years
O1
ESIR
95%
CI
Persons-years
OE
SIR
95%
CI
Colon
528,076
206
88.5
2.332
2.02
2.67
65,135
71
22.6
3.142
2.45
3.96
2,263
10
0.6
16.902
8.05
31.2
Rectum
340,102
101
56.1
1.802
1.47
2.19
42,412
31
14.4
2.162
1.46
3.07
726
0Colorectum
863,982
306
143.7
2.132
1.9
2.38
105,180
100
36.3
2.752
2.24
3.35
4,957
10
1.3
7.602
3.62
14.02
Ageofthepopulationwas
limited
to68years.Person-yearsatrisk
foroffspringwithfamilialcancer.
1Theobserved
numbersdonotaddupbecause
insomefamiliesboth
parentsandsiblingswereaffected,onewithcolonandtheother
withrectalcancer.–295%
CIdoes
notinclude1.00.
836 HEMMINKI AND CHEN
(12 cases). The median ages for siblings diagnosed with any coloncancer was 54.5 years (52 cases) and those with rectal cancer 55.9years (11 cases). For comparison, the median age of colon cancer inthe Swedish Cancer Registry (an untruncated population) is about 74years and 1 year lower for rectal cancer. We can estimate that the agetruncation at 69 years covers about 25% of all colon cancers.
Even though both the parental and offspring populations weretruncated to age below 69 years, the median age of the parentalpopulation was somewhat higher than that of the sibling popula-tion. For example, the median diagnostic age for parents withright-sided colon cancer was 58.3 years (instead of 56.8 in sib-lings). In order to rule out the effect of proband age, we analyzedthe risks according to diagnostic age groups of cases and pro-bands; the data for colon cancer and right-sided colon cancer areshown in Table III. The SIR was 11.33 for siblings and 7.51 foroffspring of parents at age below 51 years. The SIRs for right-sided colon were 20.18 and 7.51, respectively, showing the strongeffect of age and right-sided location on the sibling risk.
According to Table II, the familial excess (familial SIR � 1.00)for colon cancer in offspring of parents with colon cancer was1.58 (2.58 � 1.00); for siblings with colon cancer, it was 2.81(3.81 � 1.00). Thus, the apparent excess familial risk among sib-lings compared to offspring of affected parents was 1.8-fold; con-sequently, some 25 colon cancer of the 52 affected siblings couldbe assigned to sibling excess, i.e., putative recessive effects.
In order to exclude the contribution of HNPCC in families ofaffected siblings, at least one of whom was diagnosed with right-sided colon cancer, we listed all first and second cancers in all theirfamily members. Two of the affected siblings had a second primarycancer, one in the cervix and the other in the prostate. In these 22families, 56 other siblings were found but only 3 with cancer, 1each of rectal, breast and pancreatic cancer. The family of the rectalcancer patient was probably affected by HNPCC or FAP because,in addition to the 2 siblings with right-sided colon cancer, the fatherwas diagnosed with pancreatic cancer. Two other families wereprobably HNPCC-related because one parent in each family wasdiagnosed with a second CRC. Thus, only 3 of 22 families showedevidence of HNPCC based on the pedigree data.
Discussion
Recessive cancer syndromes are few and rare. Among the 25cancer syndromes of defined inheritance pattern discussed in arecent textbook, only 5 were recessive, and they were ataxia telan-giectasia, Bloom syndrome, Fanconi anemia, Werner syndrome andxeroderma pigmentosum.26 All of these have severe life-threateningnononcologic manifestations at an early age, which has impededthe assessment of risks for late-onset cancers in the affected individ-uals. Defective genes have been identified for these conditions andall of them take part in DNA repair and maintenance.26 It was thusnot surprising that the recently identified recessive MYH gene wasalso involved in DNA repair.13 However, a distinct feature of thisgene is that there is apparently no severe early-onset phenotype andthe related CRCs are not particularly early-onset.15,16 Late-onsetrecessive diseases are difficult to discover and so far no systematicsearches for recessive cancers have been carried out at the popula-tion level. Some human geneticists have shown that known domi-nant diseases far outnumber recessive diseases and speculate thatthe imbalance may be due to observation bias.27
So far, limited data are available on the population frequency ofMYH mutations. A study on 1,042 CRC cases from Finland found4 (0.4%) cases with biallelic mutations, diagnosed between ages40 and 66 years; 2 tumors were located in rectum and 1 in each ofrectosigmoid and right-sided colon.15 An English study included358 CRC cases diagnosed before age 56 years and found 2 (0.6%)patients with biallelic mutations diagnosed at ages 42 and 53 years;tumors were located in sigmoid colon and rectum, respectively.16
The present data address the question of recessive inheritance inCRC, with bearing toMYH mutations.
The novel finding of the present study is the demonstration of ahigher familial risk for colon but not for rectal cancer among sib-lings than among offspring of unaffected parents. The excess riskwas localized to right-sided colon cancer. In order to excludeknown causes of CRC, we examined the available data on first andsecond primary cancer among the affected siblings and their fam-ily members; HNPCC was possible only in 3 of the 22 familiesexamined. In none of the other 19 families were other cancersdiagnosed in siblings of the colon patients. As our earlier data
TABLE II – SIR FOR OFFSPRING COLON AND RECTAL CANCER WHEN PARENTS OR SIBLING WERE PROBANDS
Offspring ProbandRight-sided colon Left-sided colon All colon Rectum
O1 SIR 95% CI O1 SIR 95% CI O SIR 95% CI O SIR 95% CI
Right-sided Parent 35 3.662 2.55 5.09 16 2.322 1.32 3.77 62 2.772 2.13 3.56 21 1.48 0.91 2.26colon Sibling 18 7.532 4.46 11.93 12 5.042 2.59 8.83 31 5.432 3.69 7.71 7 1.93 0.77 4.00
Left-side colon Parent 24 2.602 1.66 3.87 23 2.442 1.55 3.67 53 2.472 1.85 3.23 15 1.112 0.62 1.83Sibling 10 4.442 2.11 8.19 4 1.78 0.46 4.60 15 2.772 1.55 4.59 9 2.612 1.19 4.98
All colon Parent 70 3.042 2.37 3.84 36 2.172 1.52 3.01 138 2.582 2.17 3.05 44 1.30 0.94 1.74Sibling 31 5.442 3.69 7.73 20 3.522 2.14 5.44 52 3.812 2.84 5.00 20 2.312 1.41 3.57
Rectum Parent 30 1.992 1.34 2.85 25 2.302 1.49 3.40 68 1.952 1.51 2.47 57 2.572 1.95 3.33Sibling 6 1.61 0.58 3.52 9 2.382 1.08 4.53 19 2.112 1.27 3.31 11 1.93 0.96 3.47
Age of the population was limited to 68 years.1Some observed numbers do not add up because in addition to the right- and left-sided colon cancer, multiple and unspecified colon tumors wereincluded.–2 95 % CI does not include 1.00.
TABLE III – SIR FOR COLON CANCER AND RIGHT-SIDED COLON CANCER IN OFFSPRING ACCORDING TO AGE AT DIAGNOSIS
SiteProband ageat diagnosis
Offspring ageParent Sibling
Person-years O SIR 95% CI Person-years O SIR 95% CI
Colon cancer � 50 � 50 141,919 24 7.511 4.81 11.19 31269 14 11.331 6.17 19.06� 50 > 50 141,919 7 2.50 0.99 5.19 31269 6 2.68 0.97 5.88> 50 � 50 723,290 60 2.381 1.82 3.07 73911 6 2.56 0.92 5.60> 50 > 50 723,290 90 1.611 1.30 1.98 73911 44 2.731 1.99 3.67
Right-sidedcolon cancer
� 50 � 50 141,919 10 7.511 3.57 13.9 31269 10 20.181 9.61 37.26� 50 > 50 141,919 4 3.42 0.89 8.85 31269 5 5.381 1.70 12.65> 50 � 50 723,290 27 2.621 1.73 3.82 73911 1 1.07 0.00 6.12> 50 > 50 723,290 41 1.741 1.25 2.36 73911 20 2.941 1.79 4.55
Person-years at risk for offspring with familial cancer.195% CI does not include 1.00.
837RECESSIVE COLON CANCER

have found no evidence for an environmental contribution to sib-ling risk, even for right-sided colon cancer,17 the results argue forthe existence of a recessive inheritance at this colonic subsite.Moreover, no evidence has been found for X-linked effects onCRC, which could mimic recessive effects.28 The median diagnos-tic age was 54.0 for the siblings diagnosed with right-sided coloncancer, which was about 2 years lower than that for left-sidedcolon or rectal cancer. However, the population in the presentstudy was truncated to age 68 years and younger and it covered anestimate of 25% of all colon cancer.
In the present work, we could estimate that in close to half ofall affected siblings with colon cancer the reason was a recessivedisease, assuming that no environmental causes contribute to thefamilial aggregation. However, because sibling analysis requires 2affected cases in a siblingship, it does not give a direct estimationon the proportion of CRC explained by this mode of inheritance.Instead, this can be done indirectly. According to the presentstudy, 3.4% of the offspring with CRC had a parent with CRC,corresponding to low-penetrance dominant inheritance.29 Suchlow-penetrance inheritance should contribute also 3.4% to siblingCRC, and the recessive component was 1.8 times large than theapparent dominant component. Thus, the apparent recessive inher-itance should contribute close to a similar proportion, 3.0% of
colon cancer up to age 68 years. Because the covered age groupaccounted for 25% of all colon cancers in Sweden, we could esti-mate that a minimum of 0.75% of all colon cancers could beexplained by this mode of inheritance. The sibling risk was highestamong those diagnosed before age 51 years, and it is likely thatthis mode of inheritance has only a marginal effect in the older(over age 69 years) population, which could not be covered in thisstudy. If unidentified sources of environmental causes contributeto familial aggregation specifically between siblings, the heritablecomponent will be smaller than the estimated 0.75%. At any rate,the proportion of recessive inheritance appears to be higher thanthat reported for MYH mutations. Moreover, MYH appeared tocause primarily tumors in the distal colon and in the rectum, oppo-site to the predominant proximal location of the recessive cancersnoted here. We assume that MYH mutations contribute to a smallextent to the apparent recessive results found, but the main part iscaused by yet unknown genetic mechanisms affecting youngsiblings.
Acknowledgements
The Family-Cancer Database was created by linking registersmaintained at Statistics Sweden and the Swedish Cancer Registry.
References
1. Lynch HT, de la Chapelle A. Hereditary colorectal cancer. N Engl JMed 2003;348:919–32.
2. Lichtenstein P, Holm N, Verkasalo P, Illiado A, Kaprio J, Koskenvuo M,Pukkala E, Skytthe A, Hemminki K. Environmental and heritable fac-tors in the causation of cancer. N Engl J Med 2000;343:78–85.
3. Johns LE, Houlston RS. A systematic review and meta-analysis of fam-ilial colorectal cancer risk. Am J Gastroenterol 2001;96:2992–3003.
4. Potter J. Colorectal cancer: molecules and populations. J Natl CancerInst 1999;91:916–32.
5. Aaltonen L, Salovaara R, Kristo P, Canzzian F, Hemminki A,Peltomaki P, Chadwick R, Kaariainen H, Eskelinen M, Jarvinen H,Mecklin J-P, Chapelle De La A. Incidence of hereditary nonpolyposiscolorectal cancer and the feasibility of molecular screening for thedisease. N Engl J Med 1998;338:14811–7.
6. Salovaara R, Loukola A, Kristo P, Kaariainen H, Ahtola H, EskelinenM, Harkonen N, Julkunen R, Kangas E, Ojala S, Tulikoura J, Val-kamo E, et al. Population-based molecular detection of hereditarynonpolyposis colorectal cancer. J Clin Oncol 2000;18:2193–200.
7. Samowitz WS, Curtin K, Lin HH, Robertson MA, Schaffer D, NicholsM, Gruenthal K, Leppert MF, Slattery ML. The colon cancer burdenof genetically defined hereditary nonpolyposis colon cancer. Gastro-enterology 2001;121:830–8.
8. Hemminki K, Li X. Familial colorectal adenocarcinoma and heredi-tary nonpolyposis colorectal cancer: a nation-wide epidemiologicalstudy from Sweden. Br J Cancer 2001;84:969–74.
9. Olsson L, Lindblom A. Family history of colorectal cancer in a Swedencounty. Fam Cancer 2003;2:87–93.
10. Eng C. Genetics of Cowden syndrome: through the looking glass ofoncology. Int J Oncol 1998;12:701–10.
11. Hemminki A, Markie D, Tomlinson I, Avizienyte E, Roth S, Loukola A,Bignell G, Warren W, Aminoff M, Hoglund P, Jarvinen H, Kristo P,et al. A serine/threonine kinase gene defective in Peutz-Jeghers syn-drome. Nature 1998;391:184–7.
12. Eng C. PTEN: one gene, many syndromes. HumMutat 2003;22:183–98.13. Al-Tassan N, Chmiel NH, Maynard J, Fleming N, Livingston AL,
Williams GT, Hodges AK, Davies DR, David SS, Sampson JR,Cheadle JP. Inherited variants of MYH associated with somaticG:C?T:A mutations in colorectal tumors. Nat Genet 2002;30:227–32.
14. Sampson JR, Dolwani S, Jones S, Eccles D, Ellis A, Evans DG,Frayling I, Jordan S, Maher ER, Mak T, Maynard J, Pigatto F, et al.Autosomal recessive colorectal adenomatous polyposis due to inheritedmutations of MYH. Lancet 2003;362:39–41.
15. Enholm S, Hienonen T, Suomalainen A, Lipton L, Tomlinson I,Karja V, EskelinenM,Mecklin JP, KarhuA, JarvinenHJ, Aaltonen LA.Proportion and phenotype of MYH-associated colorectal neoplasia in apopulation-based series ofFinnish colorectal cancer patients. AmJPathol2003;163:827–32.
16. Fleischmann C, Peto J, Cheadle J, Shah B, Sampson J, Houlston RS.Comprehensive analysis of the contribution of germline MYH varia-tion to early-onset colorectal cancer. Int J Cancer 2004;109:554–8.
17. Hemminki K, Chen B. Familial risk for colorectal cancers are mainlydue to heritable causes. Cancer Epidemiol Biomarkers Prev 2004;13:1253–6.
18. Carstensen B, Soll-Johanning H, Villadsen E, Sondergaard J, LyngeE. Familial aggregation of colorectal cancer in the general population.Int J Cancer 1996;68:428–35.
19. Hemminki K, Li X, Plna K, Granstr—m C, Vaittinen P. The nation-wide Swedish Family-Cancer Database: updated structure and fami-lial rates. Acta Oncol 2001;40:772–7.
20. Fuchs C, Giovannucci E, Colditz G, Hunter D, Speizer F, Willett W.A prospective study of family history and the risk of colorectal can-cer. N Engl J Med 1994;331:1669–74.
21. Planck M, Anderson H, Bladsrom A, Moller T, Wenngren E, Olsson H.Increased cancer risk in offsring of women with colorectal carcinoma:a Swedish register-based cohort study. Cancer 2000;89:741–9.
22. Hemminki K, Li X. Familial colorectal adenocarcinoma from theSwedish Family-Cancer Database. Int J Cancer 2001;94:743–8.
23. Dong C, Hemminki K. Modification of cancer risks in offspring bysibling and parental cancers from 2, 112,616 nuclear families. Int JCancer 2001;91:144–50.
24. Esteve J, Benhamou E, Raymond L.Statistical methods in cancerresearch, vol. 128. Lyon: IARC, 1994.
25. Hemminki K, Vaittinen P, Dong C, Easton D. Sibling risks in cancer:clues to recessive or X-linked genes? Br J Cancer 2001;84:388–91.
26. Vogelstein B, Kinzler K. The genetic basis of human cancer, 2nd ed.New York: McGraw-Hill, 2002.
27. Vogel F, Motulsky A. Human genetics: problems and approaches.Heidelberg: Springer, 1996.
28. Hemminki K, Li X. Gender effects in familial cancer. Int J Cancer2002;102:184–7.
29. Hemminki K, Czene K. Attributable risks of familial cancer from theFamily-Cancer Database. Cancer Epidemiol Biomarkers Prev 2002;11:1638–44.
838 HEMMINKI AND CHEN





























