Embed Size (px)
Citation preview
Law and Human Behavior, Vol. 29, No. 5, October 2005 ( C© 2005)DOI: 10.1007/s10979-005-7120-2
Family Representative Payeeship and Violence Riskin Severe Mental Illness
Eric B. Elbogen,1,2 Jeffrey W. Swanson,1 Marvin S. Swartz,1
and Richard Van Dorn1
Although representative payeeship is prevalent among people with mental illness andshows promise to positively influence clinically relevant outcomes, research also sug-gests this legal mechanism could be implemented in ways that are problematic. Thecurrent study examined whether family representative payeeship was associated withelevated risk of family violence perpetrated by persons with severe mental illness(SMI). Data were collected every 4 months for 1 year in structured interviews withN = 245 persons with SMI who received disability benefits. Multivariate analysesshowed that substance abuse, history of violence, frequency of family contact, andfamily representative payeeship were associated with elevated odds of family violence.Analyses also showed family contact and family representative payeeship had a cu-mulative effect on increasing the predicted probability of family violence (controllingfor covariates such as violence history and substance abuse). The data shed light onthe potential for family representative payeeship to be associated with increased riskof interpersonal conflict and violence in SMI.
KEY WORDS: representative payeeship; family violence; mental health services; mandated communitytreatment; social security administration.
There are many laws that impact upon the lives of people with severe mental ill-ness (SMI), and of these, perhaps the most frequently encountered is representativepayeeship (Monahan et al., 2005; Skoler & Allbright, 2000). Based on 2003 datafrom the Social Security Administration (SSA), an estimated 800,000 individualswith psychiatric disabilities are assigned a representative payee (RP) (SSA, 2003a,2003b). A RP is an individual or institution that directly receives disability checksand ensures a disability recipient meets basic needs (food, shelter, and clothing) andobtains proper medical, dental, and eye care (Kochhar & Scott, 1995; SSA, 2004a,2004b). Discretionary funds that remain after basic needs have been covered arelimited, usually less than $100. Although not a chief function of the RP, the RP
1Duke University Medical Center, Durham, North Carolina.2To whom correspondence should be addressed at Box 3071, Duke University Medical Center, Durham,North Carolina 27710; e-mail: [email protected].
563
0147-7307/05/1000-0563/1 C© 2005American Psychology-Law Society/Division 41 of the American Psychological Association
564 Elbogen, Swanson, Swartz, and Van Dorn
may use discretionary funds as leverage to improve treatment adherence (Luchins,Roberts, & Hanrahan, 2003). Because of these many roles and responsibilities, RPsof persons with SMI can be instrumental in reducing risk of homelessness, ensuringbasic health needs are met, and facilitating socialization. As a result, the effects ofRPs on symptoms and hospitalizations in SMI can be thought of as secondary, viathe aforementioned functions (Hanrahan et al., 2002).
Research confirms RPship promise to positively influence clinically relevantoutcomes in SMI. Empirical research has shown that persons with SMI with RPsexperience decreased victimization (Stoner, 1989), are less likely to become home-less (Rosenheck, Lam, & Randolph, 1997), participate more in treatment (Ries &Comtois, 1997), and spend fewer days in psychiatric hospitals (Luchins et al., 1998).The impact of having RPs on substance use in mentally ill populations is less clear, assome studies have shown that monetary reinforcement increased abstinence amongdually diagnosed patients (Shaner et al., 1997), whereas other studies show no ef-fect of RP enrollment on reducing substance abuse (Rosenheck et al., 1997). Re-searchers showed that individuals with SMI who were assigned a RP (usually afamily member) displayed much higher levels of treatment adherence, comparedto other subjects (Elbogen, Swanson, & Swartz, 2003a). Reis and Comtois (1997)found enhanced treatment adherence among outpatients with dual diagnoses whohad RPs compared to those without.
However, there may be potential downsides to the RP arrangement in SMI. Inparticular, some research suggests that RPship can lead to interpersonal conflict andpossibly violence. In one study, researchers found no evidence that RPs pervasivelyinterfered with the therapeutic relationship between people with SMI and RP casemanagers; however, 44% of the RP case managers reported incidents in which dis-ability recipients became verbally abusive in response to the issues concerning man-agement of their funds (Dixon, Turner, Krauss, Scott, & McNary, 1999). Elbogen,Swanson, and Swartz (2003b) showed that recent violence and fights were associ-ated with warnings made by RPs to clients with SMI that if clients did not adherewith treatment, they would not receive their disability funds. Although not directlyexamining RPship, financial dependence has been demonstrated to be related to in-creased risk of violence behavior perpetrated by people with SMI (Swanson et al.,1997).
Family RP (FRP) arrangements may be especially vulnerable to increased con-flict. Empirical research corroborates that money matters are among one of the topreasons for family arguments and that family arguments are among the top stressorsin households potentially leading to relapse (Buchkremer, Stricker, Holle, & Kuhs,1991). Financial difficulty is a frequently endorsed problem among the families withmembers with psychiatric disabilities (Altman, Cooper, & Cunningham, 1999), afinding has been replicated across many different cultures (see, e.g., Canive et al.,1996). With respect to violence risk in SMI, research has shown that family membersare more likely to be the victim of violence perpetrated by a person with SMI com-pared with non-relatives (Estroff, Zimmer, Lachicotte, & Benoit, 1994). Moreover,persons with SMI are four times more likely to become violent toward a familymember when they are financially dependent upon him or her (Estroff, Swanson,Lachicotte, Swartz, & Bolduc, 1998). For these reasons, FRP arrangements might
Representative Payeeship and Violence Risk 565
inadvertently enhance risk of family violence (and thereby negate any potentialbenefits associated with RPship). The aim of this paper is to investigate whetherFRP arrangements are associated with elevated risk of family violence perpetratedby persons with SMI.
METHOD
Sample
Data were collected as part of a randomized study of the effectiveness of outpa-tient commitment for persons with SMI (Swartz et al., 2001). The analysis presenteduse baseline assessments made prior to random assignment and data collected ev-ery 4 months for 1 year from (N = 245) subjects. Respondents were patients whohad been involuntarily admitted to one of four hospitals and who were awaiting dis-charge on outpatient commitment to one of nine counties in north central NorthCarolina. Formal eligibility criteria were as follows: (1) involuntary hospital admis-sion; (2) age 18 years or older; (3) diagnosis of a psychotic disorder or major af-fective disorder; (4) currently receiving Social Security Disability Income (SSDI) orSupplemental Security Income (SSI) from the SSA. After institutional review boardapproval was obtained, potentially eligible patients were identified from daily hos-pital admission records. While these patients were still hospitalized, research staffmet them to describe the study and to obtain their consent to participate. Of identi-fied eligible patients, about 12% refused. Rates of refusal did not significantly varyby sex, race, or diagnosis.
It is important to note that this sample does not necessarily represent all per-sons with SMI, but would generalize more narrowly to individuals with SMI whohave recently experienced involuntary hospital admission and would meet NorthCarolina criteria for outpatient commitment (indication of “danger” to self or other,including “grave disablement”). The subjects resemble populations that are some-times referred to as “revolving door” clients: persons with a history of state mentalhospital admissions, who are deemed likely to decompensate to a point of compro-mised safety without ongoing treatment in the community, and whose illness impairstheir ability to seek and adhere voluntarily to recommended treatment.
Materials
Family Violence
Violence was assessed every 4 months over the course of 1 year by subject-report using items adapted from the antisocial personality section of the NIMH Di-agnostic Interview Schedule (Robins, Helzer, Croughan, & Ratcliff, 1981; Swanson,Holzer, Ganju, & Jono, 1990) as modified for use in the Duke Mental Health Study(Swanson et al., 1997). Specifically, patients were asked whether they engaged inany physical fighting or actions causing bodily injury to a family member or whetherthey used a lethal weapon such as a stick, club, blunt object, knife, sharp object,firearm, or explosive to harm or threaten a family member in the previous 4 months.
566 Elbogen, Swanson, Swartz, and Van Dorn
Responses of “yes” were coded as an endorsement of family violence. This defini-tion approximates that used in the MacArthur Violence Risk Assessment Study(Monahan, Steadman, Silver, & Appelbaum, 2001; Steadman et al., 1998, 2000),although a distinction between sexual versus non-sexual assault was not availablein this data.
Family Representative Payeeship
Data were collected at baseline regarding whether the subjects received SSIand/or SSDI and whether someone else managed his or her disability checks. If thesubject reported that anyone managed his or her SSI and/or SSDI, the subject wasasked who that was and whether this individual was a member of his or her family(parent, sibling, spouse, or other relative).
Family Contact
At baseline, 4, 8, and 12 months, subjects were asked “How often did you gettogether with a member of your family?” and provided the following responses: 0 =not at all, 1 = less than once a month, 2 = once a month, 3 = once a week, and 4 =once a day. Subject’s responses for each data collection point over the year of theyear were averaged to create a variable connoting family contact.
Clinical and Demographic Variables
Data were collected in interviews with subjects as well as from a systematic re-view of hospital records, which involved examination of clinical assessments, treat-ment progress notes, and the legal section of the chart. Data on diagnosis (psychoticversus affective diagnosis), age, gender, ethnicity, marital status, urban vs. rural res-idence, and income were collected from these sources. Substance use was defined asany use of alcohol or illicit drugs at least occasionally during the year of the study.Functional impairment was measured using the Global Assessment of FunctioningScale (GAF), coded systematically by clinical research interviewers trained to a highdegree of inter-rater reliability.
Analysis
Data were collected from these multiple sources and entered onto SAS version8.0. When data was skewed, Wilcoxon–Mann–Whitney non-parametric procedureswere used to test for group differences. In particular, average family contact indi-cated skewed distributions when analyzed and was therefore transformed into a di-chotomous variable (“high family contact” denoting subjects above the median and“low family contact” denoting subjects below the median). The following analyseswere conducted. Descriptive analyses reporting clinical and demographic charac-teristics of subjects are first presented. Then, logistic regression was used to providebivariate associations between variables and family violence.
We employed multivariate logistic regression to determine whether FRP wassignificantly related to family violence in the presence of possible covariates,

Representative Payeeship and Violence Risk 567
including substance abuse, diagnosis, GAF, age, ethnicity, and gender. These wereselected because of previous research linking various demographic and clinical fac-tors to being assigned a RP (Conrad et al., 1998; Elbogen, Swanson, Swartz, & Wag-ner, 2003). So, if we found that FRP was related to family violence, we wanted toensure the FRP variable was not merely serving as a proxy for these other char-acteristics, some of which may be related to family violence. Conversely, it is alsoimportant to note that marital status, urban vs. rural residence, and income have notbeen shown to be related to RPship in the extant literature and bivariate analyses ofthe current data showed they were unrelated to family violence. Including these ascovariates therefore made less sense, and further, these extra variables would serveto add to chances of over-fitting the final multivariate model. Consequently, we de-cided to omit these from analyses in order to ensure an accurate representation ofrelationships in the data.
Because data were collected in the context of a clinical experiment, we con-trolled for variables associated with the randomization of OPC, including violencehistory, and amount of OPC days during the year (called “OPC dose”). Finally, weexamined the cumulative effect of FRP and family contact by running three separateanalyses with different comparison groups in order to ensure findings generalizedacross different multivariate models.
Odds ratios (OR) produced by this technique estimate the average change inthe odds of a predicted event (e.g., violent behavior) associated with exposure to arisk factor or protective factor. For independent variables measured on a continuousscale or ranking, the OR indicates the change in event likelihood per unit change inthe predictor. Odds ratio confidence intervals (CI) above 1 indicate a significantpositive effect at p < .05; conversely, odds ratio CI below 1 indicate a significantnegative effect at p < .05. The CIs indicate the range within which the true ORwould fall with 95% probability. For a detailed explanation of logistic regressionand its application to psychiatric studies, see Fleiss, Williams, and Dubro (1986) andHosmer and Lemeshow (1989).
RESULTS
Gender was evenly divided (44.5% female, 55.5% male) in the sample. Ap-proximately half the sample was between ages 18 and 39 and half were older than40 years of age (M = 40.28, SD = 10.68). Most (66.9%) of the sample members wereAfrican-American while 33% were Caucasian. Although a majority of the partici-pants lived in the city (60.8%), a substantial proportion lived in rural areas and smalltowns. Marital status was mostly single (80.4%), with 20% of the sample membersmarried. Forty-four percent of the sample reported an income below $6,000 a year.
About one-fourth of the participants (27.7%) had primary affective disorders(mood disorders such as depressive and bipolar disorder) while 72.2% were diag-nosed with primary thought disorders (psychotic disorders such as schizophreniaand schizoaffective disorder). Approximately one-third of the sample (32.7%) hadco-occurring substance abuse and mental disorder. Scores on the GAF indicatedsubjects were representative of a severely impaired population of people with SMI(M = 29.9, SD = 18.4).
568 Elbogen, Swanson, Swartz, and Van Dorn
Table 1. Bivariate and Multivariate Associations with Family Violence (N = 245)
Bivariate association Multivariate modelof family violence with of family violence
each variable individually including all variables
OR CI p-Value OR CI p-Value
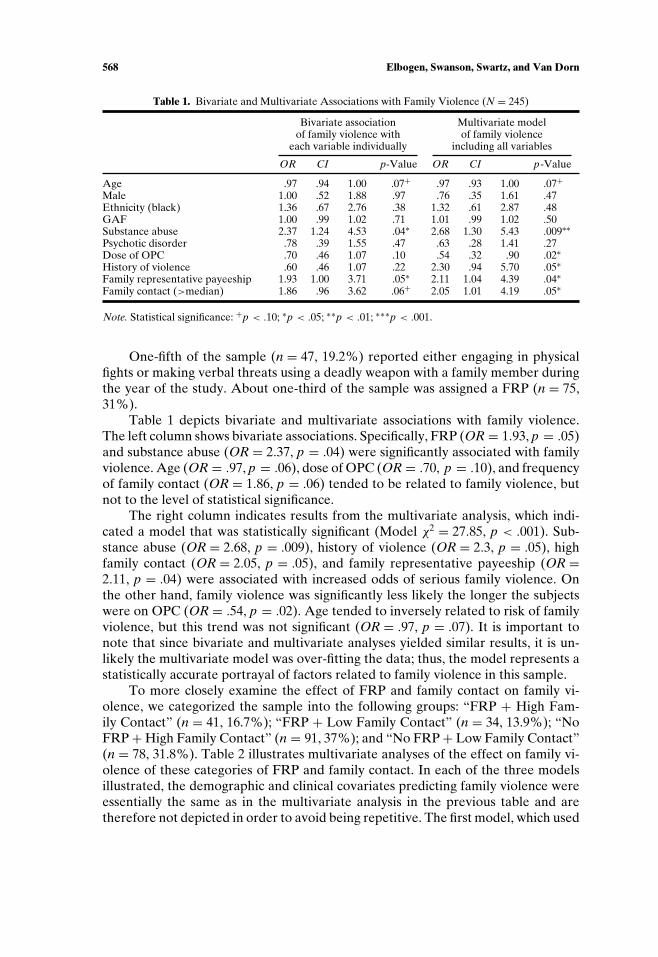
Age .97 .94 1.00 .07+ .97 .93 1.00 .07+Male 1.00 .52 1.88 .97 .76 .35 1.61 .47Ethnicity (black) 1.36 .67 2.76 .38 1.32 .61 2.87 .48GAF 1.00 .99 1.02 .71 1.01 .99 1.02 .50Substance abuse 2.37 1.24 4.53 .04∗ 2.68 1.30 5.43 .009∗∗Psychotic disorder .78 .39 1.55 .47 .63 .28 1.41 .27Dose of OPC .70 .46 1.07 .10 .54 .32 .90 .02∗History of violence .60 .46 1.07 .22 2.30 .94 5.70 .05∗Family representative payeeship 1.93 1.00 3.71 .05∗ 2.11 1.04 4.39 .04∗Family contact (>median) 1.86 .96 3.62 .06+ 2.05 1.01 4.19 .05∗
Note. Statistical significance: +p < .10; ∗p < .05; ∗∗p < .01; ∗∗∗p < .001.
One-fifth of the sample (n = 47, 19.2%) reported either engaging in physicalfights or making verbal threats using a deadly weapon with a family member duringthe year of the study. About one-third of the sample was assigned a FRP (n = 75,31%).
Table 1 depicts bivariate and multivariate associations with family violence.The left column shows bivariate associations. Specifically, FRP (OR = 1.93, p = .05)and substance abuse (OR = 2.37, p = .04) were significantly associated with familyviolence. Age (OR = .97, p = .06), dose of OPC (OR = .70, p = .10), and frequencyof family contact (OR = 1.86, p = .06) tended to be related to family violence, butnot to the level of statistical significance.
The right column indicates results from the multivariate analysis, which indi-cated a model that was statistically significant (Model χ2 = 27.85, p < .001). Sub-stance abuse (OR = 2.68, p = .009), history of violence (OR = 2.3, p = .05), highfamily contact (OR = 2.05, p = .05), and family representative payeeship (OR =2.11, p = .04) were associated with increased odds of serious family violence. Onthe other hand, family violence was significantly less likely the longer the subjectswere on OPC (OR = .54, p = .02). Age tended to inversely related to risk of familyviolence, but this trend was not significant (OR = .97, p = .07). It is important tonote that since bivariate and multivariate analyses yielded similar results, it is un-likely the multivariate model was over-fitting the data; thus, the model represents astatistically accurate portrayal of factors related to family violence in this sample.
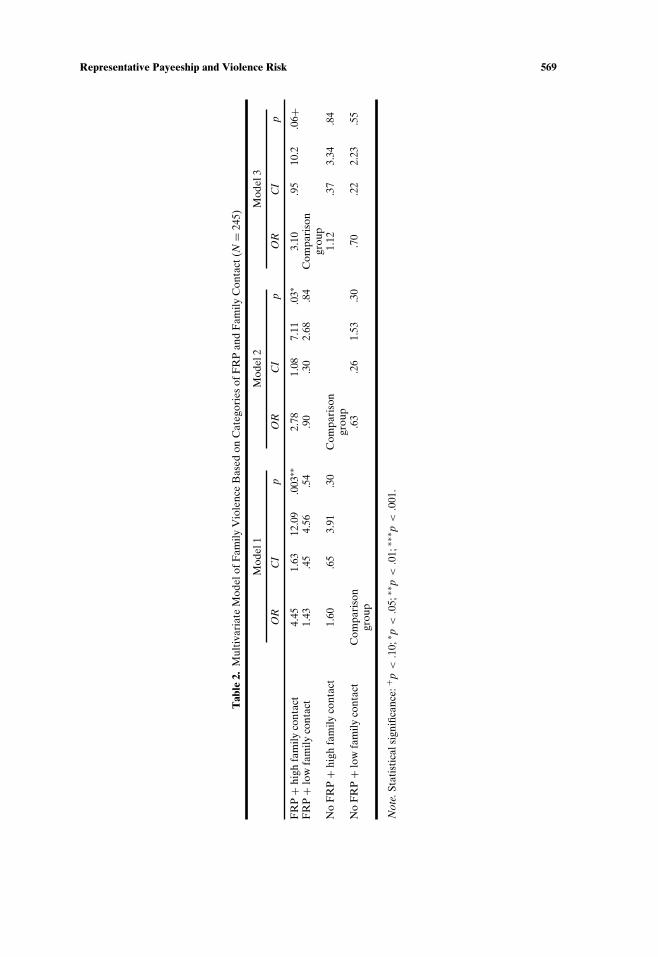
To more closely examine the effect of FRP and family contact on family vi-olence, we categorized the sample into the following groups: “FRP + High Fam-ily Contact” (n = 41, 16.7%); “FRP + Low Family Contact” (n = 34, 13.9%); “NoFRP + High Family Contact” (n = 91, 37%); and “No FRP + Low Family Contact”(n = 78, 31.8%). Table 2 illustrates multivariate analyses of the effect on family vi-olence of these categories of FRP and family contact. In each of the three modelsillustrated, the demographic and clinical covariates predicting family violence wereessentially the same as in the multivariate analysis in the previous table and aretherefore not depicted in order to avoid being repetitive. The first model, which used
Representative Payeeship and Violence Risk 569
Tab
le2.
Mul
tiva
riat
eM
odel
ofF
amily
Vio
lenc
eB
ased
onC
ateg
orie
sof
FR
Pan
dF
amily
Con
tact
(N=
245)
Mod
el1
Mod
el2
Mod
el3
OR
CI
pO
RC
Ip
OR
CI
p
FR
P+
high
fam
ilyco
ntac
t4.
451.
6312
.09
.003
∗∗2.
781.
087.
11.0
3∗3.
10.9
510
.2.0
6+F
RP
+lo
wfa
mily
cont
act
1.43
.45
4.56
.54
.90
.30
2.68
.84
Com
pari
son
grou
pN
oF
RP
+hi
ghfa
mily
cont
act
1.60
.65
3.91
.30
Com
pari
son
1.12
.37
3.34
.84
grou
pN
oF
RP
+lo
wfa
mily
cont
act
Com
pari
son
.63
.26
1.53
.30
.70
.22
2.23
.55
grou
p
Not
e.St
atis
tica
lsig
nific
ance
:+p
<.1
0;∗ p
<.0
5;∗∗
p<
.01;
∗∗∗ p
<.0
01.
570 Elbogen, Swanson, Swartz, and Van Dorn
the group “No FRP + Low Family Contact” as the comparison, shows that individ-uals in the “FRP + High Family Contact” Group were over four times more likelyto indicate family violence relative to the comparison group (OR = 4.45, p = .003).
To ensure this finding was not an artifact of a comparison group chosen arbi-trarily, we ran two further regressions using different comparison groups. The sec-ond model, which used the group “No FRP + High Family Contact” as the com-parison, again shows that the same clinical and demographic variables as above areassociated with odds of serious family violence. Individuals in the “FRP + HighFamily Contact” Group were significantly more likely to indicate family violencerelative to the comparison group (OR = 2.78, p = .03). This association was weakerthan the previous model, suggesting that family contact does have bearing on vio-lence risk.
Finally, when the “FRP + Low Family Contact” Group served as a compari-son, clinical and demographic variables retain their association with family violence.However, while individuals in the “FRP + High Family Contact” Group tended tohave increased risk of family violence, this association was no longer statisticallysignificant (OR = 3.10, p = .06). That comparing FRP with and without family con-tact did not yield statistically significant results in terms of association with violenceindicates the FRP arrangement itself has significant impact on the risk of familyviolence.
DISCUSSION
Although empirical studies attest to potential benefits of representative payee-ship in SMI (e.g., Ries & Comtois, 1997; Rosenheck et al., 1997), the current datashed light on the potential for family representative payeeship to be associated withincreased risk of interpersonal conflict and violence. Controlling for clinical and de-mographic covariates, FRP arrangements were found to be significantly associatedwith elevated risk of family violence. The findings were also consistent with otherresearch showing that risk of violence is related to accessibility of family and victims(Binder & McNeil, 1986); thus, in the current data, greater family contact portendedenhanced violence risk as in previous studies (Estroff et al., 1994). Further, model 2in Table 2 illustrates that FRP independently contributed to violence risk; in otherwords, people with High Family Contact + FRP had higher odds of family violencerisk than people with High Family Contact + no FRP. Overall, the results supportfindings from other studies implying that RP arrangements are associated with stressand conflict in the lives of people with SMI (Dixon et al., 1999; Elbogen et al., 2003b;Estroff et al., 1998; Swanson et al., 1997).
The findings suggest a relationship between RPship and family violence; how-ever, it is important to consider there are several mechanisms that may link thesetwo variables. One possibility is that family conflict is a specific response to thefact that RPship is frequently misunderstood and sometimes intentionally misused.At the time of RP assignment, SSA caseworkers describe the arrangement but arenot trained to ensure the FRP, and disability recipient fully comprehend the pa-rameters of the arrangement. Not surprisingly, investigations into complaints of RP
Representative Payeeship and Violence Risk 571
abuse consume a disproportionate amount of caseworker time at SSA offices na-tionally (SSA, 1997). SSA audits reveal that most complaints result from lack ofknowledge about the function and limits of the RP and that additional training andeducation for RPs and disability recipients is needed (SSA, 1997). The remainingcases involve intentional exploitation, often the result of disability recipients not un-derstanding the RP arrangement and thereby being vulnerable to such misuse (SSA,2002, 2004a). While such cases are relatively rare, people with SMI can be victim-ized, which has been shown to be a predictor of violence in SMI (Hiday, Swanson,Swartz, Wagner, & Borum, 2001; Swanson et al., 2002).
A different, more general mechanism connecting violence and RPship could in-volve a lack of autonomy associated with not controlling one’s own money (see gen-erally, Elbogen, Soriano, Van Dorn, Swanson, & Swartz, 2005). Researchers foundthat nearly 30% of a sample of persons with SMI perceived that family membershad warned them that if they did not attend treatment, they would not have accessto their SSI/SSDI (Elbogen et al., 2003b). The study further found that factors thathad nothing to do with finances or treatment (e.g., race) accounted for how thesewarnings were given; thus, RPs could use finances in ways that are perceived to bearbitrary or coercive. Further, RPs can foster an atmosphere of dependency. Estroff,Patrick, Zimmer, and Lachicotte (1997) found disability income adversely affectedincentive to work and function independently. If this is the case for receiving SSDIor SSI, consider the impact RPship might have on fostering a dependency role forpeople with psychiatric disabilities, a situation in which one has less control overtheir lives. If people with SMI want someday to manage their own money but arevulnerable to remaining dependent on the RP indefinitely, then RPship may feedresentment of and anger toward those who control their money (Dixon et al., 1999;Rosenheck, 1997).
Finally, the association between RPship and violence could be an artifact ofmethodology employed. In particular, we could not statistically control for everyunobserved variable that might correlate with RPship and violence. For example,people with SMI placed under RPship might be more violence prone in the firstplace. And since RP status was not controlled with randomization, we cannot ruleout the possibility that findings might reflect that a sicker group of patients (who, asa result, have RPs) are more likely to be violent. Although we took steps to includevariables that have in previous research shown to potentially relate to both RP andviolence (e.g., substance abuse, violence history, age), this list was not exhaustive ofother unidentified covariates that may also explain the relationship between RP andviolence.
Since the current study used a sample of persons with SMI, one needs to usecaution when generalizing the results to all disability recipients with psychiatric dis-abilities. It is also important to note the information on family violence was self-reported. Thus, while it is certainly possible that there was a tendency to underre-port violence, when family violence was revealed, it is very likely, this was accurateand it is difficult to imagine reasons for fabrication of such information. Addition-ally, we did not confirm if family violence was specifically targeting the FRP. Whilesuch information would be useful, limiting focus to such information would miss animportant point: if a family environment is conflicted due to financial issues, then
572 Elbogen, Swanson, Swartz, and Van Dorn
the factor that exacerbates stress may be the FRP arrangement itself, rather thanthe individual person who is the FRP.
We also did not ask if the family violence immediately resulted from an argu-ment over money; the current findings attest the need to investigate these importantquestions in future studies. It is important to consider that some subjects had othertypes of RPs (2 had legal guardians, 12 had clinicians, and 10 had friends). Sincewe were unable to conceive of how these arrangements would be related to exac-erbation of family violence, it was unclear that considering “other RP” would addto the specific analyses we conducted in this paper (i.e., if we were instead lookingat the relationship between RPship and general violence risk, then including suchdata would be warranted). Still, we wanted to make sure the data from this groupof subjects did not affect findings, so we did rerun the multivariate models exclud-ing subjects with “other RP” and found the same significant findings and trends asdescribed in Tables 1 and 2.
Similarly, it is possible that, while the vast majority of subjects were referring toRPs formally assigned by the SSA, a few cases may have involved “informal” payeearrangements in which the family member managed the subjects SSI/SSDI but wasnot officially assigned by the SSA as RP. Post hoc analyses showed that 10 subjectsindicated that a family member managed their money but did not directly receiveSSI/SSDI from SSA (suggesting an informal payee arrangement). Still, analyses us-ing the other 65 “formal” RPs showed the same significant results as above with re-spect to family violence; thus, this distinction did not appear to affect interpretationof the data. A final issue involves our operationalization of family contact, which weshould note really provides an approximate measure of family contact since we didnot calculate the exact number of days or hours per week that the subject reportedinteracting with his or her family.
To date, there have been few efforts to understand how RPship is implementedfor people with SMI. To our knowledge, this is the first empirical study to addressFRP arrangements in SMI. Even though the current findings do not demonstrateconclusively that RP status leads to increased family violence risk in SMI, the datawarrant investigation into how FRPs are implemented. If family members or peoplewith SMI do indeed perceive financial arguments or fights to be a major problem ofRPship, it may be important to increase chances that “financial management byRPs is designed to be negotiated in a way that ensures that the patient is involvedas much as possible in decisions about how money is to be allocated” (Monahanet al., 2001a, p. 1200). For now, the present study implies that interpersonal conflictmay arise within FRP arrangements and underscores the need for further researchinto the impact of a legal mechanism that affects the lives of a substantial numberof people with SMI and their families.
ACKNOWLEDGMENTS
This work was supported by NIMH Grants MH48103 and MH51410 and by theJohn D. and Catherine T. MacArthur Foundation Research Network on MandatedCommunity Treatment. The authors wish to thank the state and community mental
Representative Payeeship and Violence Risk 573
health personnel, judges, clinicians, administrative staff, court, and law officers fromDurham, Vance, Franklin, Granville, Warren, Orange, Person, Chatham, and Guil-ford counties in North Carolina who participated in this study.
REFERENCES
Altman, B. M., Cooper, P. F., & Cunningham, P. J. (1999). The case of disability in the family: Impacton health care utilization and expenditures for nondisabled members. Milbank Quarterly, 77(1), 39–75.
Binder, R. L., & McNeil, D. E. (1986). Victims and families of violent psychiatric patients. Bulletin of theAmerican Academy of Psychiatry and the Law, 14, 131–139.
Buchkremer, G., Stricker, K., Holle, R., & Kuhs, H. (1991). The predictability of relapses in schizophrenicpatients. European Archives of Psychiatry and Clinical Neuroscience, 240(4–5), 292–300.
Canive, J. M., Sanz-Fuentenebro, J., Vazquez, C., Qualls, C., Fuentenebro, F., Perez, I. G., et al. (1996).Family psychoeducational support groups in Spain: Parents’ distress and burden at nine-monthfollow-up. Annals of Clinical Psychiatry, 8(2), 71–79.
Conrad, K. J., Matters, M. D., Hanrahan, P., Luchins, D. J., Savage, C., & Daugherty, B. (1998). Charac-teristics of persons with mental illness in a representative payee program. Psychiatric Services, 49(9),1223–1225.
Dixon, L., Turner, J., Krauss, N., Scott, J., & McNary, S. (1999). Case managers’ and clients’ perspectiveson a representative payee program. Psychiatric Services, 50(6), 781–786.
Elbogen, E. B., Soriano, C., Van Dorn, R., Swanson, J., & Swartz, M. (2005). Consumer perspectives onrepresentative payee use of disability funds to leverage treatment adherence. Psychiatric Services,56, 45–49.
Elbogen, E. B., Swanson, J. W., & Swartz, M. S. (2003a). Effects of legal mechanisms on perceived co-ercion and treatment adherence among persons with severe mental illness. Journal of Nervous andMental Disease, 191(10), 629–637.
Elbogen, E. B., Swanson, J. W., & Swartz, M. S. (2003b). Psychiatric disability, the use of financialleverage, and perceived coercion in mental health services. International Journal of Forensic MentalHealth, 2(2), 119–127.
Elbogen, E. B., Swanson, J. W., Swartz, M. S., & Wagner, H. (2003). Characteristics of third-party moneymanagement for persons with psychiatric disabilities. Psychiatric Services, 54(8), 1136–1141.
Estroff, S. E., Patrick, D. L., Zimmer, C. R., & Lachicotte, W. S. (1997). Pathways to disability in-come among persons with severe, persistent psychiatric disorders. Milbank Quarterly, 75(4), 495–532.
Estroff, S. E., Swanson, J. W., Lachicotte, W., Swartz, M., & Bolduc, M. (1998). Risk reconsidered: Tar-gets of violence in the social networks of people with serious psychiatric disorders. Social Psychiatryand Psychiatric Epidemiology, 33(Suppl 1), S95–S101.
Estroff, S. E., Zimmer, C., Lachicotte, W. S., & Benoit, J. (1994). The influence of social networks and so-cial support on violence by persons with serious mental illness. Hospital and Community Psychiatry,45, 669–679.
Fleiss, J. L., Williams, J. B., & Dubro, A. F. (1986). The logistic regression analysis of psychiatric data.Journal of Psychiatric Research, 20, 145–209.
Hanrahan, P., Luchins, D. J., Savage, C., Patrick, G., Roberts, D., & Conrad, K. J. (2002). Representativepayee programs for persons with mental illness in Illinois. Psychiatric Services, 53(2), 190–194.
Hiday, V. A., Swanson, J. W., Swartz, M. S., Wagner, H. R., & Borum, R. (2001). Victimization: A linkbetween mental illness and violence? International Journal of Law and Psychiatry, 24, 559–572.
Hosmer, D. W., & Lemeshow, S. (1989). Applied logistic regression. New York: John Wiley and Sons.Kochhar, S., & Scott, C. G. (1995). Disability patterns among SSI recipients. Social Security Bulletin, 58,
3–14.Luchins, D. J., Hanrahan, P., Conrad, K. J., Savage, C., Matters, M. D., & Shinderman, M. (1998). An
agency-based representative payee program and improved community tenure of persons with men-tal illness. Psychiatric Services, 49(9), 1218–1222.
Luchins, D. J., Roberts, D. L., & Hanrahan, P. (2003). Representative payeeship and mental illness: Areview. Administration and Policy in Mental Health, 30(4), 341–353.
Monahan, J., Bonnie, R. J., Appelbaum, P. S., Hyde, P. S., Steadman, H. J., & Swartz, M. S. (2001).Mandated community treatment: Beyond outpatient commitment. Psychiatric Services, 52(9), 1198–1205.

574 Elbogen, Swanson, Swartz, and Van Dorn
Monahan, J., Redlich, A. D., Swanson, J., Robbins, P. C., Appelbaum, P. S., Petrila, J., et al. (2005). Useof leverage to improve adherence to psychiatric treatment in the community. Psychiatric Services,56(1), 37–44.
Monahan, J., Steadman, H., Silver, E., & Appelbaum, P. (2001). Rethinking risk assessment: TheMacArthur study of mental disorder and violence. New York: Oxford University Press.
Ries, R. K., & Comtois, K. A. (1997). Managing disability benefits as part of treatment for persons withsevere mental illness and comorbid drug/alcohol disorders: A comparative study of payee and non-payee participants. American Journal on Addictions, 6(4), 330–338.
Robins, L. N., Helzer, J. E., Croughan, J., & Ratcliff, K. (1981). National Institute of Mental Health Di-agnostic Interview Schedule: Its history, characteristics, and validity. Archives of General Psychiatry,38, 381–389.
Rosenheck, R. (1997). Disability payments and chemical dependence: Conflicting values and uncertaineffects. Psychiatric Services, 48(6), 789–791.
Rosenheck, R., Lam, J., & Randolph, F. (1997). Impact of representative payees on substance use byhomeless persons with serious mental illness. Psychiatric Services, 48(6), 800–806.
Shaner, A., Roberts, L. J., Eckman, T. A., Tucker, D. E., et al. (1997). Monetary reinforcement of absti-nence from cocaine among mentally ill patients with cocaine dependence. Psychiatric Services, 48(6),807–810.
Skoler, D. L., & Allbright, A. L. (2000). Judicial oversight of the nation’s largest guardianship system:Caselaw on Social Security Administration representative payee issues. Mental and Physical Dis-ability Law Reporter, 24(1), 169–174.
SSA. (1997). Monitoring representative payee performance: Report—1997. Retrieved May 28, 2004, fromhttp://www.ssa.gov/oig/ADOBEPDF/audit htms/96-64201.htm.
SSA. (2002). Summary of financial related audits of representative payees for the social security ad-ministration. Retrieved May 28, 2004, from http://www.ssa.gov/oig/ADOBEPDF/audittxt/A-13-02-22096.htm.
SSA (2003a). SSI annual statistical report, 2002. Retrieved May 28, 2004, from http://www.ssa.gov/policy/docs/statcomps/ssi asr/2002/index.html.
SSA (2003b). Annual statistical report on the social security disability insurance program, 2002. RetrievedMay 28, 2004, from http://www.socialsecurity.gov/policy/docs/statcomps/di asr/2002/exp toc.html.
SSA. (2004a). Fraud and abuse in the supplemental security income program, U.S. House ofRepresentatives Ways and Means Committee. Retrieved May 28, 2004, from http://www.ssa.gov/oig/communications/testimony speeches/05202004testimony.htm.
SSA. (2004b). A guide for representative payees. Retrieved May 28, 2004, from http://www.ssa.gov/pubs/10076.html.
Steadman, H. J., Mulvey, E. P., Monahan, J., Robbins, P. C., Appelbaum, P. S., Grisso, T., et al. (1998).Violence by people discharged from acute psychiatric inpatient facilities and by others in the sameneighborhoods. Archives of General Psychiatry, 55(5), 393–401.
Steadman, H., Silver, E., Monahan, J., Appelbaum, P. S., Robbins, P. C., Mulvey, E. P., et al. (2000). Aclassification tree approach to the development of actuarial violence risk assessment tools. Law andHuman Behavior, 24, 83–100.
Stoner, M. R. (1989). Money management services for the homeless mentally ill. Hospital and Commu-nity Psychiatry, 40(7), 751–753.
Swanson, J. W., Estroff, S. E., Swartz, M. S., Borum, R., et al. (1997). Violence and severe mental disorderin clinical and community populations: The effects of psychotic symptoms, comorbidity, and lack oftreatment. Psychiatry, 60(1), 1–22.
Swanson, J. W., Holzer, C. E., Ganju, V. K., & Jono, R. T. (1990). Violence and psychiatric disorder in thecommunity: Evidence from the Epidemiologic Catchment Area Surveys. Hospital and CommunityPsychiatry, 41(7), 761–770.
Swanson, J. W., Swartz, M. S., Essock, S. M., Osher, F. C., Wagner, H. R., Goodman, L. A., et al. (2002).The social-environmental context of violent behavior in persons treated for severe mental illness.American Journal of Public Health, 92(9), 1523–1531.
Swartz, M. S., Swanson, J. W., Hiday, V. A., Wagner, H., Burns, B. J., & Borum, R. (2001). A randomizedcontrolled trial of outpatient commitment in North Carolina. Psychiatric Services, 52(3), 325–329.