Embed Size (px)
Citation preview
"Fast tracking" ED patients with chest pain: Integrating the chest pain evaluation unit and the observation unit Author: Susan C. Finefrock, RN, MS, CEN, Columbus, Ohio
R ul ing out a cardiac event in pa t ients who come , to the e m e r g e n c y d e p a r t m e n t with ches t pa in
has always b e e n a challenge. It has b e e n reported that 4% of pa t i en t s wi th acu te myocardial infarctions (MIs) are inadver ten t ly d i scharged from the emergency de- pa r tmen t na t ionwide . 1 Even pa t i en t s for w h o m a quick d iagnos is of acu te MI is m a d e by a d iagnos t ic EKG, posi t ive cardiac enzyme tes t results, or both of- t en differ in their presenta t ion, history, and symptoms, m a k i n g initial ED triage difficult. Five years ago pa t i en t s who came to Riverside Methodis t Hospi tal ' s Emergency Depar tmen t (a tert iary hospital emer- gency d e p a r t m e n t wi th 65,000 visits per year) wi th symptoms sugges t ive of heart d isease would either be admi t t ed to a critical care or s t ep -down un i t or be sen t home. Often admiss ion to the hospital was later found to be u n n e c e s s a r y when, after a 3- or 4-day stay, the pa t i en t was found not to have a cardiac problem. The pa t i en t lost valuable work t ime and exper ienced u n n e c e s s a r y expense . Conversely, pa t ien ts wi th ini- tial nond iagnos t i c EKGs and wi th normal cardiac en- zyme levels could inadver ten t ly be released from the e m e r g e n c y d e p a r t m e n t before their MI could be detected.
The Chest Pain Evaluation Unit (CPEU) In January 1993, our e m e r g e n c y depa r tmen t opened a f ive-bed Chest Pain Evaluat ion Unit (CPEU) wi th in the confines of the e m e r g e n c y depar tment . The first CPEU cons is ted of five des igna t ed s tretchers and a small nu r ses ' s ta t ion at one end of the emergency de- par tment . In J anua ry 1994, we moved to a self- con ta ined un i t tha t consis ts of five private rooms and a large nurses ' station. This un i t is wi th in easy access of the tr iage area and the a m b u l a n c e en t rance and is the point of ent ry for all pa t i en t s wi th ches t pa in or its equivalent . The pr imary purposes of the CPEU are the rapid ident i f ica t ion of pa t i en t s wi th acute MIs and the
Ms. Finefrock is assistant nurse manager, Observation Unit, and education coordinator, Emergency Department, Riverside Method- ist Hospitals, Columbus, Ohio.
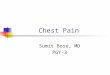
t imely admin is t ra t ion of thrombolytic agents . The uni t is staffed by two regis tered nurses and a t echn ic ian who has been cross- t ra ined to perform EKGs. Approx- imately 350 pa t ien ts come to the CPEU each month. Approximately 58% of the pa t ients go to the Observa- t ion Unit for 12 to 18 hours, and 28% of the pa t ients are directly admi t ted to the hospital (Figure 1).
The F.D Observation Unit The ED Observat ion Unit at Riverside is an 18-bed moni tored uni t ad jacen t to the e me r ge nc y depart-
For reprints, write Susan C. Finefrock, RN, MS, CEN, Emergency Department, Riverside Methodist Hospitals, 3535 Olentangy River Rd., Columbus, OH 43214. J EMERG NURS 1995;21:417-22 Copyright �9 1995 by the Emergency Nurses Association. 0099-1767/95 $5.00 + 0 18/1/66841
Discharged
Observed 58%
Figure 1 ED disposition of patients with chest pain.
October 1995 4 17

JOURNAL OF E M E R G E N C Y NURSING/Finefrock
ment. The observation unit provides the ED physician with a third option for low-risk patients with chest pain. Use of this unit allows a short-term period of cardiac monitoring, serial measurements of cardiac enzymes and EKGs, and possible stress testing. The unit consists of three connecting units (A, B, and C). Observation units A and B contain 13 hardwired monitored rooms, and Observation. C contains five nonmenitored rooms. Each room is equipped with a hospital bed, color television, reclining chair, overbed table and nightstand, telephone, and suction and ox- ygen equipment. There is a bathroom in each unit and separate nurses' stations. Equipment necessary for a code is readily available. Meals are served through the hospital dietary services. If all units are full, staffing consists of four registered nurses and two technicians.
N u r s e s are e n c o u r a g e d t o o v e r u t i l i z e t h e C P E U r a t h e r t h a n u n d e r u t i l i z e it, a n d t h e s t a f f i s n e v e r t o s e c o n d - g u e s s t h e t r i a g e n u r s e ' s d e c i s i o n . A l l n u r s e s are a w a r e o f h o w a p a t i e n t , s " s t o r y " c a n c h a n g e f r o m t r i a g e to t h e m a i n t r e a t m e n t a r e a .
All of the ED registered nurses and technicians rotate through the CPEU and Observation Units. At the end of the observation process (usually 12 to 18 hours), the patient 's condition is reevaluated either by the ED physician, the patient 's attending physician, or a cardiologist. Disposition can then be safely made. 2
Patients in the Observation Unit meet medical- surgical or step-down criteria and patients with chest pain comprise 46% of the patient population. The length of stay varies for patients with chest pain, de- pending on the time of day they arrive in the CPEU and whether they are scheduled for stress testing. The most commonly ordered stress tests are the sestamibi (Cardiolite) thallium stress test and the stress echocar- diogram. We do not schedule routine treadmill stress testing. Our 12- to 18-hour protocol for observation of a patient with chest pain includes serial measure- ments of cardiac enzyme concentrations (creatine ki-
nase MB subunit) and EKGs at 0, 6, and 12 hours, and possible stress testing. Because services of our non- invasive laboratory are only available to patients from 7 AM to noon, Monday through Saturday, patients must wait until that time for stress testing even though they have had enzyme tests and EKGs earlier in their stay. An average of 75% of all of our Observation Unit patients (not just cardiac patients) are discharged and 25% are admitted. For low-risk patients with chest pain (most patients who go to the Observation Unit are low risk), the discharge rate is 90%. The physician who writes the transfer orders for the patient also writes the time when the patient 's condition is to be reevaluated by the ED or attending physician. This is usually after the third testing of enzyme levels and EKGs or after the stress test results are known.
Triage guidelines for patients who arrive with chest pain were purposely formulated to be broad so that the triage nurse has substantial leeway in decid- ing where patients should have initial evaluation--the main emergency department or the CPEU. Only experienced ED nurses are assigned to the triage area (triage nurses must have worked in the emergency department for at least 6 months). Nurses are encour- aged to overutilize the CPEU rather than underutilize it, and the staff is never to second-guess the triage nurse's decision. All nurses are aware of how a patient 's "story" can change from triage to the main treatment area. If, after the patient has been evaluated by the CPEU registered nurse and ED physician, it is believed that the patient 's symptoms are noncardiac in origin, the patient is transferred to the main treat- ment area and to another primary nurse. This ensures a more steady flow through the CPEU. A certain amount of flexibility must be built into the system to account for times when the main emergency depart- ment is busy and the CPEU is not or vice versa.
The CPEU is protocol driven, and we have succeeded in shortening our "door-to-drug" time for thrombolytic agents from 72 minutes 18 months ago to less than 30 minutes. Our staff was charged with designing the new CPEU and establishing protocols and developing a chest pain assessment form (Figure 2), staffing patterns, patient/staff education tools, re- search, and community outreach. An intensive edu- cational program was launched before the CPEU was opened to provide all ED nurses with the educational background necessary for evaluating patients with chest pain and interpreting their EKGs. Nurses first completed a self-learning cardiac module that in- cluded a videotaped presentation by one of the ED physicians on cardiac anatomy and physiology, dys- rhythmia, EKG interpretation, and complications as- sociated with specific infarcts. The module included
418 Volume 21, Number 5
Finefreck/IOURNAL OF L'MIERGENCY NURSING
PHYSICIAN
'O EOIS' A'ION ITOC EO i EOMA'N tE'O ONSET OF SYMPTOMS THAT PROMPTED THIS VISIT: DATE:
FOR SYMPTOMS PERSISTING �9 24 HRSMEDICAL ATTENTION WAS SOUGHT: I MODE OF ONSET
[ ] ASYMPTOMATIC I [ ] SUDDEN STATUS AT ONSET
[ ] REST [ ] EXERTION I--] AWAKENED FROM SLEEP
[ ] . ASSOCIATED SYMPTOMSt~IGN8
[ ] DYSPNEA [ ] DIAPHORESIS CHEST DISCOMFORT W1TH:
[]DEEP BREATHING B [ ] PALPATION
[ ] ASYMPTOMATIC []PAIN
SEVERITY (1-10 SCALE
ASSOCIATED SYMPTOMS
q DYSPNEA DIAPHORESIS
' DATE TIME WEIGHT(PT. STATED) AGE ~'~
CARDIOLOGIST (IF ANY)
I SEEN BY ED ATTENO'NG I [ ] AMBULATORY [~EMS []HELICOPTER<
TIME: DURATION: (HRS) (MIN)
[ ] YES[~] NO DATE: TIME:
b=I[ STERNAL [ ] EPIGASTR~C [ ] LEFT CHEST [ ] RIGHT CHEST [ ] NECK/JAW
[ ] NAUSEA [ ] VOMITING
[ ] GRADUAL E~]STUTTERING (INTERMITTENT) C~JAUrf I R E U E F MEASURES PTA
[ ] BACK [ ] PRESSURE/HEAVINESS [ ] INDIGESTION [ ] REST EFFECTIVE? [~LUE []BURNING [ ] INDESCRIBABLE YES[] NOF-'] []RUE [ ] SHARP OR STABBING [ ] ACHE I[~NTGSL YES[] NO~] []SHOULDER []CONSTANT [ ] CRUSHING
[ ] I~ERMI'R'Ekrf [ ] OTHER
[ ] SYNCOPE [ ] EXTREME FATIGUE [ ] NEAR SYNCOPE [ ] PALPITATIONS
[ ] CHANGES IN POSITION [ ] EXERCISE/ACTIVITY
LOCA~ON OF PAIN
[ ] STERNAL [ ] EPIGASTRIC [ ] LEFT CHEST [ ] RIGHT CHEST
110) []NECK [ ] BACK
[ ] NAUSEA [ ] VOMITING
OUAUTY OF PAIN CHEST DISCOMFORT WITH:
[ ] LUE [ ] PRESSURE/HEAVINESS [ ] INDESCRIBABLE [ ] DEEP BREATHING [ ] RUE [ ] BURNING [ ] ACHE [ ] PALPATION [~SHOULDER [ ] SHARP OR STABSING [ ] CRUSHING [ ] CHANGES IN POSITION
[ ] CONSTANT [ ] OTHER [ ] EXERCISE/ACTIVITY [ ] INTERMITTENT [ ] [ ] INDIGESIION ] [ ]
[ ] SYNCOPE [ ] EXTREME FATIGUE [ ] NEAR SYNCOPE [ ] PALPITATIONS
- - _~"~ RGIES [ ] NONE
[ ] MI [ ] DIABETES ~PROCEDURES DATES: [ ] PACEMAKER [ ] SMOKER(PPD x YRS)= PACK YRS I I I HEART CATH [~ ANGINA I~ PREVIOUS CARDIAC ARREST I [ ] STRESS TEST [ ] HTN r--]CVA/TIA [ ] COPD I [ ] ANGIOPLASTY [ ] KNOWN HIGH CHOLESTEROL [ ] FAMILY HX I [ ] CABG [ ] PERIPHERAL VASCULAR DISEASE [ ] OTHER J ~ ] OTHER
MENTAT1ON SKIN CHEST WALL CARDIAC RESPIRATORY
[~ALERTIORIENTED [~WARM [--]DRY [ ] PAIN ON [~WNL [~CLEARBIL [ ] LETHARGIC [ ] PALE PALPATION [ ] MUFFLED [ ] CONFUSED [ ] FLUSHED _ _ [ ] MURMUR [ ] HALES [~ UNCONSCIOUS [--]DIAPHORETIC LOCATION [~ CLICiORUB [ ] RHONCHI [ ] [ ] CYANOTIC [ ] RUB [ ] ABSENT
[ ] COOL ~-~OTHER [~OXIMETER _ _ ABDOMINAL [ ] SOFT [ ] NONTENDER ~OTHER __
[ ~ W N L []ABNORMAL [ ] RHYTHM INITIAL VS BP _ _ P _ _
[ ] REVIEWED BY DR _ _ _ _ TIME /" SIGnAl UN~ \
EMERGENCY DEPARTMENT CHEST PAIN EVALUATION UNIT ~ I I P P L E M E N T A L A S S E S S M E N T
< B L %I;EEIX,
[~] EDEMA
R
/ J
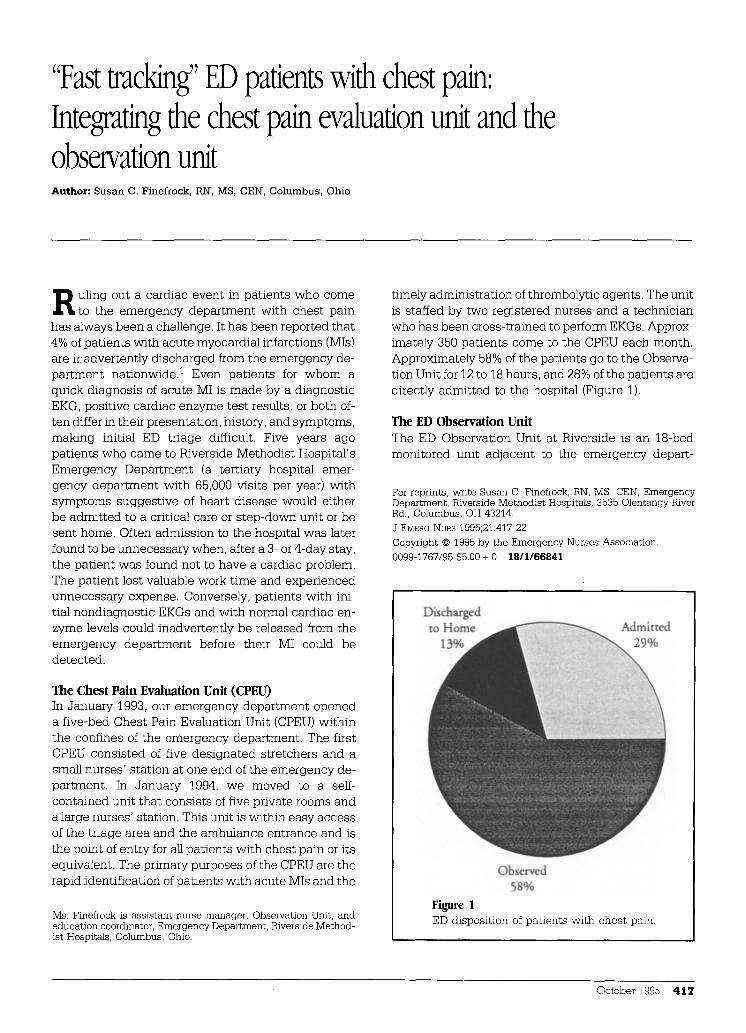
Figure 2 Riverside Methodist Hospitals CPEU supplemental assessment form. PT, Patient; PTA, prior to admission; NTG SL, nitroglycerin sublingual; MI, myocardial infarction; PPD, packs per day; HTN, hypertension; CVA/TIA, cerebrovascular accident/transient ischemic attack; COPD, chronic
obstructive pulmonary disease; HX, history; CABG, coronary artery bypass graft; WNL, within normal limits; BIL, bilateral; R, right; L, left; VS, vital signs; BP, blood pressure; P, pulse; R, respiration. Used with permission.
October 1995 419
OURNAL OF EWIERGENCY NURSING/Finefrock
Stage I Stage 11 Stage Il l (After Triage) Stage IV Slagr V (After Triage) (After Triage) (A fler Triage) (After Triage)
Actual Time F r ~ e 0 to 5 minutes 5 to [5 minutes 15 to 30 minutes 30 to 60 minutes 60 - 120 minutes
Desired O u t c ~ e s Initial uloge by RN Physlci~ a s s c s ~ t Cardiology at bedside Admissi~ bed k n ~ n H & P completed T a k ~ to treatment area ECG ~ a l ~ t e d Tr~tmenl p l ~ established Relief of chest pain Relief of chest pain Psalms status assessed Atlcndlng/Cardlology c~suited Re. rye m~itored i n - h ~ bed. as H ~ staff notified of admiasi~ IJb results available CPEU protocols initiated 5 minutes to respond indicated Report called
Dx: Cardiac vs, n~ardiac. If cardiac, I ~ risk vs, high risk
Discharge planning Identify risk factors C~tact admitting if acute MI Begin to as~ss di~harge needs Tr i sec t to Critical Ca~ Unit M ~ e 1o E.t if n~c~rdiac Tr i sec t to OBS if going to s ~ o w n M ~ e to OBS if a~diagnoshe YKO. I ~ dsk a pare f r ~ "referral plbcnl"
Pati~at Ed~afion: Explain proced~a P.xplain pr~odures ExplaLq p/~edures Explain pt~eau(r I~piain pr~c~lmes K a ~ l e ~ g e Deficit Allay flags Aliay f~ rs Allay fears Aliay fears Allay f ~ t a
TestCPrccedu~s/Mcds ECG Cardiac mmltoring Pads* ox lm e ay 2 L O 2
Cardiac m~i to l ing Serial ECOs as indicated ST segment m~itori~g IV access -labs drawn from IV access Lab s~adies poriahlr chest x-ray Meds: Nitrates, ASA Thrombolyfie ordered, if indicated Prepare for cam lab. ff indicated
Cardiac m~i tormg ST ~ g m ~ t nRmitoring Meals as ~ red : Nitroglycerin Heparin Morphine sulfate Beta h i .he r s C a l r ehexmel bl~kers Thr~bolyt ic
ST acgmem mtmito~ A*~ss ~apo.se to m~s Ch~k lab results
Cardiac m~itoring ST segm~t r a ~ i l o f ~ Aa~ss ~sponse to reeds C%~k hh ~ s u ~
C~aulta Cardiology * i f indica~d Cardinlogy at bedside MSS i f indicated
Mobibty Bedreat Be31est Bedrest Bedrest Bedfast
Nehitlo. NFO NPO NPO NFO NFO
%3 Yes No 3-11 Ye~ No I l-7 Yes No
%3 Yea No 7-3 Yea No 3-11 Yes NO 3-11 Yes No 11-7 Y e s ~ N o l l - 7 Y e s N o
of aursmg ~ , nor ts il memt to tale p~e~ebce over phys i e~ orders.
%3 Yes No 3-11 Yes No I I-7 Yes No _ _
Progressing o~t Track? (Civic Oor
Iota: "Ibis is not ~ all laclulive h~
%3 Yes No 3-11 Yes- No 11-7 Yes N o
Source: Liad~ Shah, RN, Clcvehnd Clink (Cricieal Pathway f o ~ f )
~ F ~ n d a E ~ . A l i R i ~ h t ~ R ~ c d , 1994 P e m t i a s i ~ t o u s c f o ~ a t g r ~ t c d b y ClcvciandCiinie, 1994
A:XPaOtway.mi~
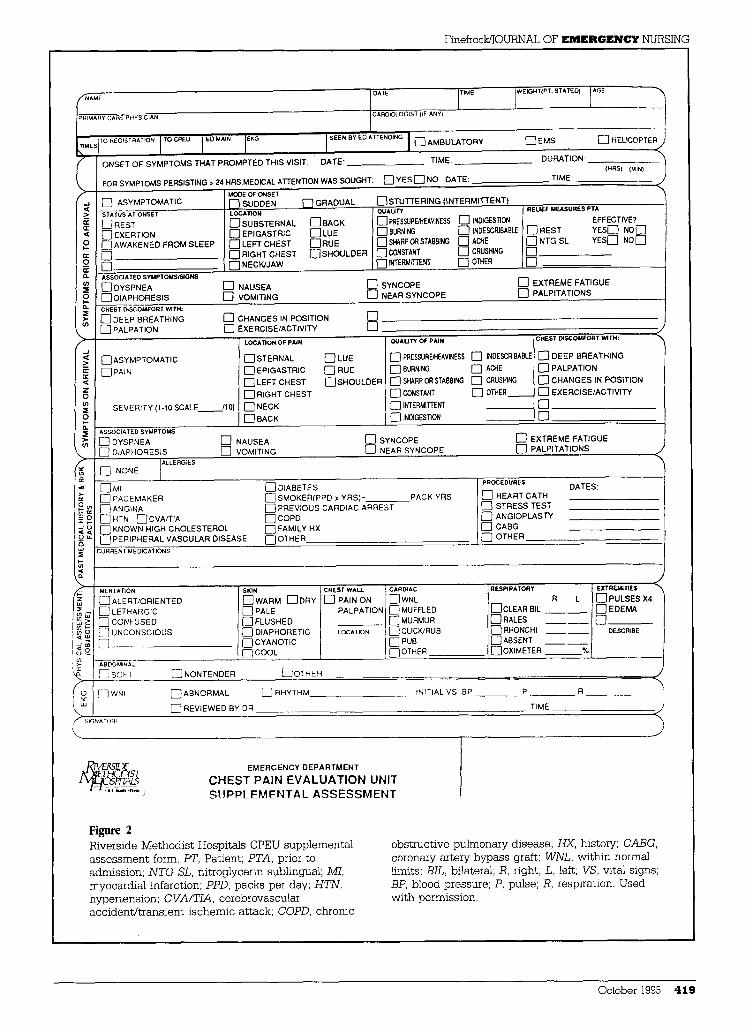
Figure 3 CPEU clinical protocol for chest pain/acute MI. H & P, History and physical examination; Dx, diagnosis; MI, myocardial infarction; OBS, observation; 02,
oxygen; ASA, acetylsalicylic acid (aspirin); MSS, Medical Social Services; NPO, nothing by mouth. Used with permission.
a pretest and posttest on EKG interpretation. The module learning was followed by a day long program on cardiac care that included cardiac diagnostic test- ing, cardiology input for acute MI, correlations of acute
T h r o m b o l y t i c a g e n t s c o u l d b e o r d e r e d on a "hot l ine" d irec t ly f rom t h e p a t i e n t ' s CPEU r o o m to a p h a r m a c i s t a n d t h e n w o u l d b e h a n d - d e l i v e r e d b y cour ier to t h e p r i m a r y r e g i s t e r e d n u r s e w i t h i n 10 m i n u t e s .
MI with clinical presentation, nursing care of the pa- tient with acute MI, educating the patient with chest pain, differentiating diagnoses of chest pain, and case studies with practice sessions on EKG interpretation. The ED physicians, nurses, and cardiologists collabo-
rated in designing the educational programs. Now the nurses in the CPEU determine the priority for notifi- cation of the ED physician on the basis of patient pre- sentation and EKG interpretation.
Two major systems problems were identified by the task force before the CPEU opened: registration of the CPEU patients and obtaining thrombolytic drugs from the pharmacy. Through the concerted efforts of the team members, we developed a fast registration process that allowed us to obtain a charge plate from the computer before obtaining all of the patient data normally required for registration. We could then send blood specimens to the laboratory, order x-ray films, and so forth. Registration is now completed after the patient's initial treatment has been started and when it is more convenient for the patient and the CPEU staff. The pharmacy launched an extensive educa- tional program for its staff (pharmacists, technicians, and transport) so that thrombolytic agents could be ordered on a "hot line" directly from the patient 's CPEU room to a pharmacist and then would be hand- delivered by courier to the primary registered nurse within 10 minutes. Both systems have worked well.
While in the CPEU and Observation Units, our patients have a dysrhythmia monitor and a continu-
4 2 0 Volume 21, Number 5
Finefrock/JOURNAL OF EMERGENCY NURSING
Singe I l l (Alger Triage) Stage IV (After Triage) Stage V (After TrisgO stage VI (ARcr Triage) stage Vl l (Afar Triage) Stage Vlf l (After Triage)
15 - 30 minutes 30 * 120 minutes 6 houri from ptln ~ s c t 12 hoofs f r ~ pahz rosa 14 hours from pare onset Post stress test
Dr wti~z| OBS mders, Relief of chest pain Pai~w.r P a i o f ~ P.azYmea negative Negative stress t~st e.allod to OBS. Lab reglits available Patient able to verhally explain Patient able to verbally explain N~di sga~ t l c ECG R ~ i n s pain f r ~
�9 l n ~ " patinas and stepdown T ~ t plan established for tv~tmteat plan and r a t i ~ l c , t~catracnt plan lind e n t i t l e . Patlant painfree " i n l e t , p a t i ~ U ~ v ~ t h t i chservatioaal cc~r~
wiU net have of den Doetcr writes O1~ orders for Pallmt trlmsfencxl to OBS "inter~" patimt of choice ~ release
0r admit
Trealmeat plan inenfified l~a t i fy cardiac risk f ~ t o n Continued a s ~ s ~ t of di~harge Continued a s s e s s o r of discharge C| a s s e s s o r of discharge T ~ plan identified needs needs needs
Expisin procedu~s Teaching T ~ h l n 8 T ~ h i n 8 Teaching I3lacharge teaching Allay* f ~ n Explain proc, edur~ Explain procedures Explain pr~edures Explain p r~edu~s Fo l io -up appointmeat
Allay l e a n Allay f~ rs Allay fears Allay fears Di~harge packet l : o l l ~ . u p call in 3 days
C ~ d h g monitofil~ Cardiac monitoring Cardiac monitoring Cardiac mmitormg Csrdh~ ~ i t o ~ n g Cardiac m ~itoring ST #r monitoring ST legateat monitoring ST ~etnl~t m~itof ing ST segment m~i to l ing ST segm~l m ~ i ~ ST segment m~itofmg A t l a s ~sponec to reeds A ~ ~sponst to reeds Asscu respon~ to reeds Assess ~spon~ to reeds As~ss nspon~ to reeds Assess respoosr to reeds
EKG EKG Sirras Test C P ~ CPK/MB
MSS ff need idea6fied
OBS patient - BRP OBS pttiaat - BRP BRP BRP BRP BRP �9 latedat" - Bedrest "latet~ml" - Bed~st uatH r ~
evMuatlon
OBS Patient - No cardiac Stlm OBS pathaR - NC~ NCS NCS NCS if no stress testing ordered NCS (NO;) "In.r im" - NPO ~ t l l r ~ NFO except for water 4 hours p f i~ "laterlm" - NPO evalua6on to suess lesliag
7-3 Yr No 3-11 Yea No I I-7 Yes No
7-3 Yel No
3-n re; No 11-7 Yes" No"
7-3 Yes No
3-II Yes No 11-7 Yes No
Note: This is not an all-lncluslve list of aunisg ~re , nor is it meant to take p~cdcncr over physici~ ~ders,
Source: Linda Shah, RN, Cleveland Clinic {critic*] Pathway f o ~ t )
�9 Cl~elmul Clinic F ~ d a t i ~ , All Rights R c ~ e d , 1994 P e ~ i s s i ~ to u ~ f o c a l g e l l e d by Clevel~d Clinic. 1994
%3 Yes No 3-11 Y e l No 11-7 Yes No*
%3 Yes No
3 -n r e . No I I-7 Yes No
7 3 Yes No 3-11 Yes No 11-7 Yes No
A:~Pathwty.mi~
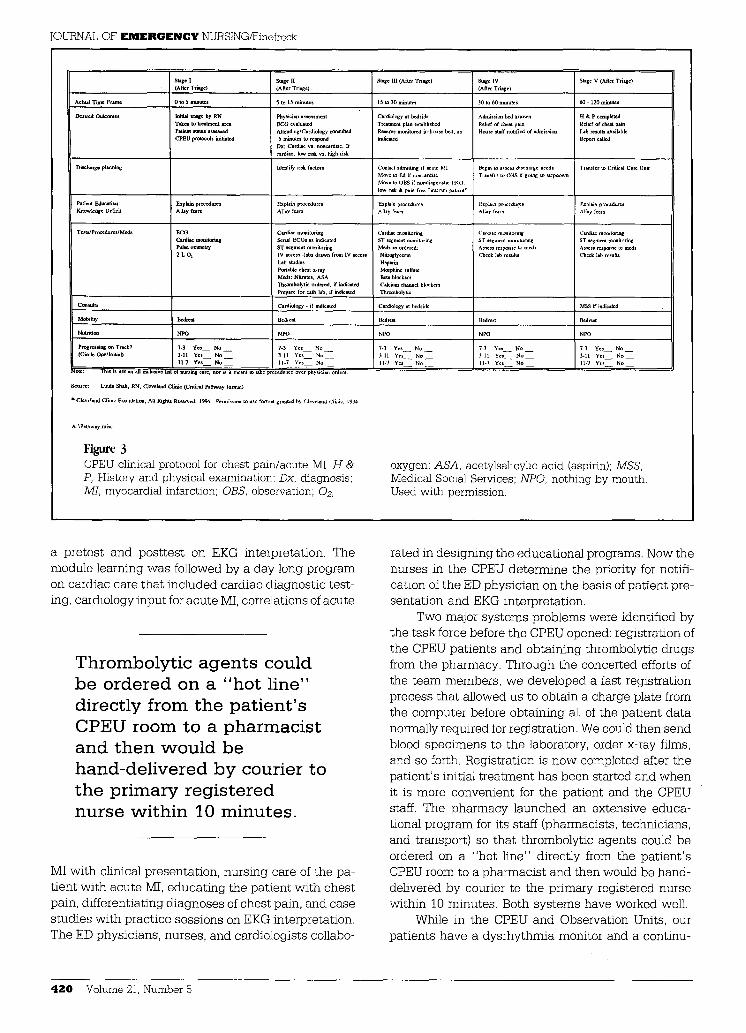
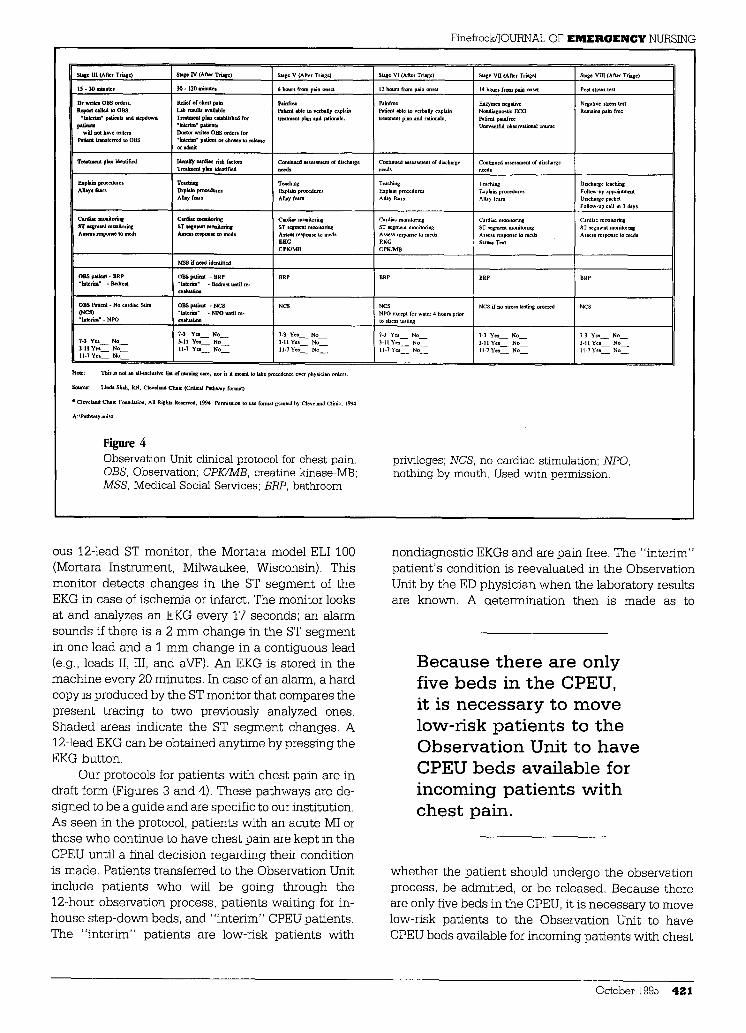
Figure 4 Observation Unit clinical protocol for chest pain. OBS, Observation; CPK/MB, creatine kinase-MB; MSS, Medical Social Services; BRP, bathroom
privileges; NCS, no cardiac stimulation; NPO, nothing by mouth. Used with permission.
ous 12-lead ST monitor, the Mortara model ELI 100 (Mortara Instrument, Milwaukee, Wisconsin). This monitor detects changes in the ST segment of the EKG in case of i schemia or infarct. The monitor looks at and analyzes an EKG every 17 seconds; an alarm sounds if there is a 2 mm change in the ST segment in one lead and a 1 mm change in a contiguous lead (e.g., leads II, III, and aVF). An EKG is stored in the machine every 20 minutes. In case of an alarm, a hard copy is produced by the ST monitor that compares the present t racing to two previously analyzed ones. Shaded areas indicate the ST segment changes. A 12-lead EKG can be obtained anytime by pressing the EKG button.
Our protocols for pat ients with chest pain are in draft form (Figures 3 and 4). These pathways are de- s igned to be a guide and are specific to our institution. As seen in the protocol, pat ients with an acute MI or those who continue to have chest pain are kept in the CPEU until a final decision regarding their condition is made. Patients transferred to the Observation Unit include pat ients who will be going through the 12-hour observation process, pat ients wai t ing for in- house s tep-down beds, and "interim" CPEU patients. The "inter im" pat ients are low-risk pat ients with
nondiagnost ic EKGs and are pain flee. The "interim" pa t ien t ' s condition is reevaluated in the Observation Unit by the ED physic ian when the laboratory results are known. A determinat ion then is made as to
B e c a u s e t h e r e are o n l y f ive b e d s in t h e CPEU, it is n e c e s s a r y to m o v e l o w - r i s k p a t i e n t s to t h e O b s e r v a t i o n Uni t to h a v e CPEU b e d s a v a i l a b l e for i n c o m i n g p a t i e n t s w i t h c h e s t pain .
whether the pat ient should undergo the observation process, be admitted, or be released. Because there are only five beds in the CPEU, it is necessary to move low-risk pat ients to the Observation Unit to have CPEU beds available for incoming pat ients with chest
October 1995 421
JOURNAL OF EMERGENCY NURSING/Finefrock
pain. If the CPEU is full, n e w pa t ien ts are evaluated in the e m e r g e n c y d e p a r t m e n t and CPEU protocols are followed.
We have found that pa t i en t s are more recept ive to pa t i en t t e a c h i n g w h e n they are transferred to the
Observa t ion Unit. This is probably related to a variety
of factors: the Observat ion Unit is a less stressful and quieter e n v i r o n m e n t than the emergency depar tment ; the observat ion rooms are comfortable; pa t i en t s are now pa in free; and initial educa t ion has b e e n done by the CPEU staff. We are developing an educat ional packet for pa t ien ts who arrive with ches t pain. This packe t will inc lude information on cardiac risk factors, a schedule for wellness classes, defini t ion of terms mos t f requently used in the emergency depa r tmen t and hospital set t ing, and d iagnost ic test ing. We also w a n t to send each pa t i en t home with a wallet-sized, l amina ted copy of his or her EKG. The nurses in the Observat ion Uni t make a 3-day follow-up te lephone
T h e 1 2 - l e a d ST m o n i t o r h a s b e e n s h o w n to d e t e c t p a i n - f r e e i s c h e m i a a n d in farc t s in o t h e r ED s e t t i n g s . H o w e v e r , m o r e r e s e a r c h is n e e d e d to d e t e r m i n e t h e c o s t b e n e f i t of t h i s t e c h n o l o g y .
call to all pa t i en t s wi th ches t pa in who were in the Observat ion Unit. This has b e e n very well received by pa t ien ts and their families. Pat ients also express high sat isfact ion wi th their CPEU experience.
We have succeeded in m a i n t a i n i n g an efficient ED-controlled CPEU and Observat ion Unit, and we believe that our pa t ien ts wi th ches t pa in receive comprehens ive , cost-effective care in a t imely man- ner. Missed diagnosis of acu te MI is the lead ing liti- gat ion cost for the e m e r g e n c y depa r tmen t s and our
observat ion protocol has virtually e l imina ted that problem.
The "5 -minu te EKG" (within 5 minu t e s of com- ing into the e m e r g e n c y d e p a r t m e n t an EKG is taken and read by the CPEU nurse) is the dr iving force in our CPEU protocols. The ED staff also expresses h igh sat- isfaction wi th the t eam approach in the CPEU, the close associa t ion wi th the cardiologists, and the m a n y opportuni t ies for learning.
We con t inue to evaluate our 12- to 18-hour Observat ion Uni t protocol. It has b e e n our exper ience that pa t ien ts in the Observat ion Unit who are "ruled in" for an acu te MI on the bas is of cardiac enzyme test results do so by hav ing an e levated creat ine ki- nase-MB level at the 6-hour mark. Studies have examined the efficacy of u s i ng different cardiac markers such as myoglobin, Troponin T, and Troponin 14-6 at t imes other t han 0 to 6 hours and 12 hours. 7 We
have also ident if ied infarcts and i schemia earlier in the observat ion process as a result of ST changes recog- n ized by the con t inuous 12-lead ST monitor. The 12- lead ST moni tor has been shown to de tec t pain-free i schemia and infarcts in other ED set t ings, s, 9 How-
ever, more research is needed to de te rmine the cost benef i t of this technology.
Our CPEU a nd observat ion protocols have worked well, bu t we will con t inue to reevaluate pa t ien t outcomes, research, and cost to be s t mee t the needs of our clientele and our inst i tut ion.
I thank Anthony Joseph, MD, FACEP, for his expertise in observational medicine, and the CPEU Task Force members for their hard work and commitment to this project.
References
1. Lee TH, Weisberg M, Cook F, et al. Evaluation of creat- ine kinase and creatine kinase-MB for diagnosing myocar- dial infarction. Arch Intern Med 1987;147:115-21. 2. Finefrock S. Stretching the healthcare dollar: the ED ob- servation unit. J EMERG NURS 1994;20:487-90. 3. Rusnak RA, Stair TO, Hansen K, et al. Litigation against the emergency physician: common features in cases of missed myocardial infarction. Ann Emerg Med 1989;18:1029-34. 4. Tucker JF, Collins RA, Anderson A J, et al. Value of serial myoglobin levels in the early diagnosis of patients admitted for acute myocardial infarction. Ann Emerg Med 1994;14: 704-8. 5. Kelly PA, et al. Myoglobin detects early myocardial infarction more rapidly than creatine kinase-MG or tropo- nin-T irrespective of day I electrocardiogram diagnosis [Ab- stract]. J Am Cell Cardiol 1994;23:78A. 6. Adams JE, Ladenson JH, Jaffe AS. Similar sensitivities of cardiac troponin I and MB creatine kinase for detection of acute myocardial infarction [Abstract]. J Am Coil Cardioi 1994;23:78A. 7. Gibler WB, Lewis LM, Erb RE, et al. Early detection of acute myocardial infarction in patients presenting with chest pain and non-diagnostic ECGs: serial CK-MB sam- pling in the emergency department. Ann Emerg Med 1990;19:1359-66. 8. Fesmire FM, Smith EE. Continuous 12-lead electrocar- diograph monitoring in the emergency department. Am J Emerg Med 1993;11:54-9. 9. Fu GY, Joseph A J, Antalis G. Application of continuous ST-segment monitoring in the detection of silent myocardial ischemia. Ann Emerg Med 1994;23:1113-5.
4 2 2 Volume 21, Number 5