Embed Size (px)
Citation preview

Fatal Drug Reactions in Patients Admitted to Surgical
Services
Bruce Armstrong, MB, DPhil, MRACP,’ Waltham, Massachusetts
Barbara Dlnan, RN, Waltham, Massachusetts
Hershel Jick, MD, Waltham, Massachusetts
Although the frequency of fatal drug reactions in medical inpatients has been studied in detail [I], little is known about their frequency in surgical pa- tients. A recent special survey which included pa- tients admitted to surgical services has allowed us to estimate the frequency of drug-related deaths in a defined population of surgical inpatients. The deri- vation of this estimate is described in this report.
Methods
This report is based on a special survey conducted in twenty-four Boston area hospitals from January to No- vember 1972. The survey involved interviewing approxi- mately 25,000 consecutive patients admitted to general medical and surgical wards and has been described in detail elsewhere [2]. Nurse interviewers obtained information on demographic characteristics of each patient, drugs taken before admission, diagnoses at discharge, and the outcome of the hospitalization in terms of survival. In addition, a summary of the hospital course was obtained after dis- charge. Excluded from the survey were those patients who had been hospitalized during the three months immedi- ately before the current admission, those less than twenty or more than seventy-five years of age, or those who could not be interviewed (for medical reasons). In addition, an unknown number of patients who were hospitalized for less than 72 hours were missed because of a variable time lag between admission and interview.’
The present investigation was limited to patients ad- mitted to the surgical services of twenty-two of the
From the Boston Collabwative Drw Swveillance Prooram. Boston Universitv Medical Center, Waltham, Massa&setts. This wori w&supported by Us Public Health Service Contract NOl-GM4-2148 from the National Institute of General Medical Sciences.
Reprint requests should ba addressed to Hershel Jick, MD. the Boston Collaborative Drug Surveillance Program, 400 Totten Pond Road, Waltham, Massachusetts 02154.
* National Health and Medical Research Council of Australia Clinical Sciences Fellow (Epidemiology).
twenty-four hospitals, a total of 3,748 men (average age, 46.9 years) and 6,533 women (average age, 44.4 years). Two hospitals were excluded because of difficulties in obtaining further detailed information regarding their patients. All but two of the hospitals included were community general hospitals, and these accounted for 89 per cent of the sur- gical patients studied.
For the purpose of this evaluation, all twenty nine pa- tients who died in hospital were identified and their case summaries were reviewed in detail. The complete hospital case record was also reviewed when there was insufficient information in the case summary on the events leading to death or when it appeared that an adverse effect of a drug may have contributed to death (a total of 19 patients).
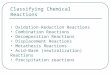
The summaries from a random sample of 200 of the 10,281 patients were also reviewed to determine the nature of the principal surgical procedure performed (if any). The percentage distribution of these procedures is shown in Table I. Gynecologic surgery accounted for approximately 21 per cent of the admissions, which explains in part the excess of women in the whole group. Approximately 14 per cent of the patients had no surgical procedure during the monitored admission despite being admitted to a surgical service.
Results
Eleven men and eighteen women died in hospital. Nine of the deaths were from disseminated cancer in patients who had no surgical procedure in their final admission. The other twenty deaths occurred in pa- tients who had surgery and who would not have been expected to die from their disease during the current hospitalization. Nine of these surgically treated pa- tients died as a result of complications developing at the operation site (6 with infection and 3 with hem- orrhage). The remainder died after other morbid events developed in the postoperative period (pul-
Volume 132, Nevembw 1976 643

Armstrong, Dinan, and Jick
TABLE I Distribution of Surgical Procedures
among 200 Randomly Selected
Surgical Admissions
Procedure Percentage
Hernia repair 7.5 Cholecystectomy 5.5 Hemorrhoidectomy 3.0 Urologic procedures 9.0 Hysterectomy 10.5 D & c* 5.5 Other gynecologic procedures 5.0 Other abdominal procedures 4.5 Breast surgery 2.5 Ligation and stripping of varicose veins 3.0 Reduction of fracture 3.5 Laminectomy 3.5 Other orthopedic procedures 9.0 Otorhinolaryngologic procedures 4.5 Minor thoracic surgery 1.5 Dental surgery 1.5 Miscellaneous minor procedures 7.5 No operative procedure 13.5
*D & C = Dilatation and curetage, with or without an- other minor gynecologic procedure.
monary embolism, 2; myocardial infarction, 2; in- tractable cardiac failure after valve replacement, 2; cerebrovascular accident, 2; other, 3). Among these deaths an adverse effect of a drug was considered after careful review of the entire hospital record to contribute to two deaths.
Case Reports
Case I. A sixty-seven year old woman underwent radical vulvectomy for carcinoma of the vulva and subsequently required skin grafting to an area of wound separation. Twenty-four days after the initial procedure, a lung scan showed evidence of infarction of the left lower lobe, and she was heparinized five days later after persistent unexplained fever. After ten days of laboratory-controlled heparin therapy, she suddenly collapsed, became pale, cold, and clammy, and her blood pressure was recorded as 80/50 mm Hg. A diagnosis of massive pulmonary embolism was made, and she was given intravenous fluids and a further intra- venous injection of heparin, presumably because her whole blood clotting time had been only 9 minutes on the pre- ceding day. She did not respond to treatment, however, and died after 2 hours. Necropsy revealed a tear in the capsule of the spleen with 4 1 of blood in the peritoneal cavity. The spleen was not enlarged but showed congestion and reti- culoendothelial hyperplasia. There was a small infarct in the lower lobe of the left lung but no evidence of recent embolism.
Case II. A sixty-three year old yoman underwent total hip replacement for osteoarthritis. Ten days postopera- tively she complained of weakness, convulsed, and became stuporous. Examination revealed a systolic blood pressure
of 90 mm Hg and no localizing neurologic signs. A diagnosis of massive pulmonary embolism with cerebral hypoper- fusion was made and she was given 125 mg of heparin in- travenously. During the next 30 minutes she regained normal consciousness and showed evidence of mild left hemiparesis. A further 75 mg of heparin was administered, and then intravenous protamine when her whole blood clotting time was noted to be 36 minutes. Shortly thereafter she complained of severe headache, had signs of raised intracranial pressure, and died. Necropsy revealed a large right cerebral infarct with hemorrhage into the occipital lobe and a small right subdural hematoma. Multiple large pulmonary emboli filled all the main branches of the pul- monary artery and there was bilateral pulmonary edema and hemorrhage.
In each of these cases, it appears that heparin may have contributed to the hemorrhage that led to the patient’s death. In this series, therefore, the death rate attributable to heparin therapy, and to adverse effects of drugs in gen- eral, was 0.19/1,000 of patients admitted to surgical services (approximate 95 per cent confidence limits, 0.02 to 0.71/ 1,000) or approximately 0.22/1,000 patients who underwent surgery (approximate 95 per cent confidence limits, 0.02 to 0,62/1,000). The overall death rate was approximately 2.2/1,000 patients who underwent surgery.
Comments
Because the major objective of this survey was to evaluate the relationship of outpatient drug use to the development of newly diagnosed disease, many seriously ill patients (for example, those who were hospitalized in the previous three months) were de- liberately excluded. In addition, patients undergoing major surgery usually performed at referral centers were underrepresented, and anyone who died under anesthesia or for other reasons early in the course of their hospitalization may have been missed.
For these reasons the results of this study relate only to a selected group of generally healthy surgical patients, aged twenty to seventy-five years, and ad- mitted mainly to community general hospitals. This group, though restricted, is nevertheless of unusual interest with regard to serious adverse drug effects since, in general, these patients would be expected to survive hospitalization. Death from any cause was uncommon among them and drug-related death appeared to have been a rare event. The frequency estimated from this study is 0.19 deaths/l,000 in- patients (95 per cent confidence limits, 0.02 to 0.71 deaths/l,OOO). Whereas the frequency of drug-related deaths may very well be higher in generally sicker patients who were excluded from this survey, the results in this comparatively healthy surgical popu- lation must be considered reassuring in that they suggest the scope of the problem is not alarmingly large.
644 The American Journal ol Surge7

Fatal Drug Reactions
Both of the drug-related deaths identified were in women more than sixty years old and were associated with heparin therapy. In the patient in case I, it is likely that heparin made a major contribution to the fatal outcome. in the patient in case II, although heparin probably contributed to the fatal cerebral hemorrhage, it is likely that she would have died from pulmonary embolism had this not occurred. These two patients serve to emphasize the need for alertness to possible complications of heparin therapy, par- ticularly in elderly women [3].
Summary
cent confidence limits, 0.02 to 0.71/1,000). Both
In a defined group of 10,281 generally healthy in- patients admitted to surgical services, two deaths were identified as being due in part to an adverse effect of a drug, for a rate of 0.19 drug-related deaths/l,000 surgical patients (approximate 95 per
Acknouhdgment: The following hospitals in Massachusetts participated in this study: Beth Israel Hospital, Beverly Hospital, Boston University Hospital, Boston Veterans Administration Hospital, Brockton Hospital, Cardinal Cushing Hospital, Emerson Hospital, Faulkner Hospital, Framingham Union Hospital, Lawrence Memorial Hospital, Leonard Morse Hospital, Malden Hospital, Marlboro Hospital, Mount Auburn Hospital, New England Medical Center Hospital, New England Memorial Hospital, Newton-Wellesley Hospital, Norwood Hospital, Quincy City Hospital, Salem Hospital, Sancta Maria Hospital, South Shore Hospital, Symmes Hospital, and Waltham Hospital.
References
2. Jick-Ii, Miettinen OS, Neff RK, Shapiro S. Heinonen OP: Coffee
1. Jick H: Drugs-remarkably nontoxic. N fngl J A&d 291: 824. 1974.
deaths occurred in women more than sixty years old and were due to hemorrhage associated with heparin therapy.
and myocardial infarction. N Eng/ J Aded 289: 63, 1973. 3. Jick H, Slone D, Borda IT, Shapiro S: Efficacy and toxicity of
heparin in relation to age and sex. N Engl J #ed 279: 284, 1968.
VOlumo 132. Novnnkr 1976 645