Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Fatal Pandemic (H1N1) 2009 Influenza A Virus Infection in aPennsylvania Domestic CatE. R. Campagnolo1,2, J. T. Rankin2, S. A. Daverio3, E. A. Hunt4, J. R. Lute5, D. Tewari6, H. M. Acland6,S. R. Ostrowski1, M. E. Moll2, V. V. Urdaneta2 and S. M. Ostroff2
1 Centers for Disease Control and Prevention, Office of Public Health Preparedness and Response, Office of Science and Public Health Practice,
Atlanta, GA, USA2 Pennsylvania Department of Health, Bureau of Epidemiology, Harrisburg, PA, USA3 Williamsport West Veterinary Hospital, Williamsport, PA, USA4 Pennsylvania Department of Health, Bureau of Community Health Systems, Williamsport, PA, USA5 Pennsylvania Department of Health, Bureau of Laboratories, Exton, PA, USA6 Pennsylvania Department of Agriculture, Pennsylvania Veterinary Laboratory, Harrisburg, PA, USA
Impacts
• Report of the earliest laboratory-confirmed pandemic pH1N1 fatality in a
domestic cat associated with influenza-like illness in a Pennsylvania family.
• Risk of exposure of domestic cats to pet owners ill with influenza-like illness
(ILI) during the peak period of the fall wave of 2009 pH1N1 in
Pennsylvania.
• Information presented will assist veterinary care providers and pet owners
in understanding the clinical features of this disease in domestic cats and
the potential for transmission of infection to pets from infected humans.
Introduction
Influenza A virus is an important respiratory pathogen
known to affect both humans and animals. Although aqua-
tic birds are considered to be the natural reservoir for most
influenza A viruses, many subtypes are relatively species-
specific and non-pathogenic to humans. Pigs can become
simultaneously infected with multiple influenza A sub-
types, including those found in humans, providing oppor-
tunities to recombine viral genetic segments and producing
new strain variants. This occurred in early 2009, when a
newly recognized recombinant influenza A/H1N1 variant,
composed of genetic segments from humans, pigs and
birds, was detected in two children in southern California
(Garten et al., 2009). This virus quickly spread throughout
North America and the rest of the world, and by June 2009
was termed a pandemic virus by the World Health Organi-
zation and is now referred to as pandemic H1N1 (pH1N1).
Although pH1N1 is thought to have originated in
mammalian (swine) viruses, once it had adapted to pro-
Keywords:
Pandemic; pH1N1; zoonoses; cat; fatal;
influenza A virus; veterinary public health;
pneumonia; influenza-like illness;
cardiomyopathy; Pennsylvania
Correspondence:
Dr. Enzo R. Campagnolo. Career
Epidemiology Field Officer, Pennsylvania
Department of Health, Northwest District
Office, 19 McQuiston Drive, Jackson Center,
PA 16133, USA. Tel.: 724 662 6081;
Fax: 724 662 6086; E-mail: [email protected]
Received for publication August 03, 2010
doi: 10.1111/j.1863-2378.2011.01390.x
Summary
We report the earliest recognized fatality associated with laboratory-confirmed
pandemic H1N1 (pH1N1) influenza in a domestic cat in the United States.
The 12-year old, indoor cat died on 6 November 2009 after exposure to multi-
ple family members who had been ill with influenza-like illness during the peak
period of the fall wave of pH1N1 in Pennsylvania during late October 2009.
The clinical presentation, history, radiographic, laboratory and necropsy find-
ings are presented to assist veterinary care providers in understanding the fea-
tures of this disease in cats and the potential for transmission of infection to
pets from infected humans.
Zoonoses and Public Health
500 Published 2011. This article is a US Government work and is in the public domain in the USA. • Zoonoses Public Health. 58 (2011) 500–507

duce human infection the virus caused sporadic infections
in other animal species. Starting in August 2009, labora-
tory-confirmed pH1N1 infection began to be reported in
swine (Pereda et al., 2010; ProMED, 2009a), in several
domestic species (cats, ferrets, dogs, turkeys), and in a
cheetah (USDA, 2009, 2010; AVMA, 2010; USDA-APHIS,
2010, ProMED, 2009b,c). These reports demonstrate that
pH1N1 can be anthroponotic (i.e. carried by humans and
transmitted to animals). In these cases, there was close
interaction between the infected animals and their human
owners, some of whom were reported to have influenza-
like illness (ILI). Although it has become apparent that
humans can transmit pH1N1 to animals, it has yet to be
established whether or not the spread of pH1N1 can be
bidirectional.
The first recognized case of laboratory-confirmed
pH1N1 illness in a domestic cat occurred in Iowa on 30
October 2009 (Sponseller et al., 2010; ProMED, 2009d);
this cat survived the infection and recovered. The earliest
fatal case of pH1N1 in a domestic cat occurred 1 week
later in Pennsylvania on 6 November 2009. The infection
was confirmed by the United States Department of Agri-
culture (USDA), National Veterinary Services Laborato-
ries (NVSL) in Ames, Iowa.
In this report, we describe the clinical features of the
illness observed in this cat, including necropsy findings,
to enhance awareness among veterinary clinicians about
this disease and to increase their index of suspicion about
the diagnosis in pets presenting with cardio-respiratory
illness, especially during periods of high influenza activity
in the community.
Case Report
On 5 November 2009, a previously healthy 12-year-old
domestic short-haired (DSH), orange tabby neutered
male cat, was brought to a veterinary clinic in north
central Pennsylvania with a respiratory illness (tachyp-
noea with dyspnoea), anorexia and lethargy. The pet
owner reported to the attending veterinarian that the ill-
ness was first noticed on 3 November 2009; the owner
expressed concern about the possibility of the cat having
pH1N1 infection because all human household members
had flu symptoms in the 2–3 weeks preceding the cat’s
illness. The cat was kept indoors 100% of the time, with
no opportunities for exposure to people or animals out-
side the home environment. The cat was reportedly a
very sociable and affectionate animal, inclined to sit
close to its owners, and often seeking face-to-face con-
tact with humans. Two dogs and a tortoise living in the
same home as the cat were reported as healthy. The pet
owners provided no history of coughing, sneezing, rhin-
orrhea, or conjunctivitis in the cat, nor were any of
these clinical signs observed by the attending veterinar-
ian.
There were four human household members living in
the home with the sick cat (Table 1). All four were
reported to have respiratory illness typical of influenza
with dates of onset between 19 October 2009 and 4
November 2009. On 1 November 2009, the 18-year-old
male household member was seen in the local hospital
emergency department and was clinically diagnosed with
pH1N1 infection. During this period, human pH1N1 ill-
ness was widespread in all regions of Pennsylvania, and
therefore no specimens were collected by the attending
physician to confirm this diagnosis. Of the 3697 speci-
mens submitted to the Pennsylvania state public health
laboratory for testing between 1 October 2009 and 26
November 2009, a total of 2542 (69%) were positive for
influenza virus, and 99% of the positive specimens were
characterized as pH1N1 (Pennsylvania Department of
Health Bureau of Laboratories BOL, 2009). The other
household members did not seek health care for their ill-
ness.
Clinical examination
Upon examination of the cat, the veterinary practitioner
noted difficulty in breathing, described as rapid, shallow
breathing, along with expiratory wheezing and slightly
harsh broncho-vesicular sounds on auscultation. The oral
mucous membranes were described as medium pink. The
cat was tachycardic with a heart rate of 200 beats/minute
(normal: 120–140), which was described as regular and
without murmur. The resting respiratory rate was signifi-
cantly elevated at 100 breaths per minute (normal: 16–
40). The rectal temperature was 102 �F at the time of the
examination (normal: 98.5–101.5 ± 1�F).
Table 1. Onset of respiratory illness in human household members
and pet cat, October 2009 to November 2009
Onset of respiratory
illness
Age
(years) Gender Clinical signs
19 October 2009 1.5 Female Fever, cough, congestion,
diarrhoea
23 October 2009 18 Female Congestion, cough,
malaise
28 October 2009 18 Male Fever, cough, congestion,
vomiting, arthralgia
3 November 2009 12 Male
(cat)
Tachypnoea, dyspnoea,
anorexia, lethargy
4 November 2009 49 Male Fever, cough, congestion,
nausea, arthralgia
E. R. Campagnolo et al. Fatal Pandemic (H1N1) 2009 Influenza A in a Domestic Cat
Published 2011. This article is a US Government work and is in the public domain in the USA. • Zoonoses Public Health. 58 (2011) 500–507 501

Clinical laboratory findings
A venous blood sample was collected from the cat and
analyzed in-house for a blood profile which included a
complete blood count (CBC) and blood chemistry
(Table 2). The only abnormalities noted were a slightly
low blood phosphorus of 2.8 mg/dL (normal: 3.1–7.5),
and a slightly elevated blood glucose of 161.0 mg/dL
(normal: 71–159).
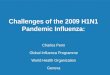
Radiology
Dorsal and lateral thoracic radiographs were obtained.
The thoracic radiographs (Fig. 1) showed bilateral mot-
tled, mixed bronchial–interstitial and alveolar patterns
throughout the majority of the dorsal lung fields, consis-
tent with the clinical signs of compromised respiratory
function. The heart silhouette was distinct, and did not
appear to be enlarged or misshapen. A more consolidated
appearing area of soft-tissue/fluid density was evident cra-
nial to the heart and mediastinum. There was no appar-
ent deviation of the trachea or of the heart.
The cat was clinically diagnosed as having a respiratory
infection, and was administered 0.5 mL of procaine peni-
cillin-G subcutaneous by the veterinarian and dispensed
an oral antibiotic (Clavamox 125 mg tablets) to be taken
twice a day, according to standard hospital protocols. The
cat was then discharged from the veterinary hospital and
taken home by its owner.
The following day (6 November 2009), the cat was
brought back to the veterinary clinic with progressive ill-
ness, including increased anorexia and worsening respira-
tory symptoms, which included rapid shallow abdominal
breathing, suggestive of pneumonia or acute congestive
heart failure, although no cyanosis was observed. In
response, the veterinarian administered a fluoroquinolone
antibiotic (Baytril 22.7 mg/mL), 1 mL intramuscular and
subcutaneous fluid treatment with 100 mL of sterile 0.9%
NaCl saline and admitted the cat to the clinic for obser-
vation.
Because of the pet owner’s concerns about possible
pH1N1 illness in the household, the attending veterinar-
ian contacted the Pennsylvania Department of Agriculture
(PDA) for guidance. Although there was no apparent
nasal discharge, based on advice from PDA, nasal swabs
were collected from the ill cat and submitted to the Penn-
sylvania Department of Health Bureau of Laboratories
(BOL) for pH1N1 testing. To accomplish this, several
attempts at nasal and nasopharyngeal swabbing were per-
formed due to lack of nasal discharge.
While under observation, the cat died unexpectedly
later on the day of 6 November 2009. When first admit-
ted, kennel staff reported the cat as alert and sitting in his
cage, which appeared clean. The cat had used its litter
box, and had eaten a small portion of the canned food
provided. About 30 min later, the cat was noted to be
agonal and was lying on its side with the contents of the
cage having been disturbed as if there had been a seizure
or excessive thrashing. The cat vomited the recently eaten
food and expired a few minutes later.
Necropsy findings
On 7 November 2009, a necropsy was performed on the
cat by the attending veterinarian. There was no evidence
of cyanosis, and the oral mucus membranes were
observed to be pink. However, the cat’s heart and lungs
appeared grossly abnormal. The ventricular walls were
thickened with a corresponding decrease in heart chamber
size, compatible with the common pathologic condition
of feline hypertrophic cardiomyopathy (fHCM). The
lungs appeared mottled, but there was no evidence of
pulmonary oedema, nor was there presence of pulmonary
or pleural fluid. The entire bronchial tree (i.e. trachea,
bronchi and lungs) and heart were submitted, along with
the nasal swabs collected on November 6, to the BOL for
pH1N1 testing. Frozen lung tissue from the cat was also
submitted for histopathologic and microbiologic analysis
to the Pennsylvania Veterinary Laboratory.
Table 2. Blood profile for cat with respiratory illness, 5 November
2009
Complete blood count Blood chemistry
RBC 8.41 M/lL BUN 16.0 mg/dL
HCT 42.7% CREA 1.4 mg/dL
HGB 12.8 g/dL PHOS 2.8 mg/dL*
MCV 50.8 fL CA 8.8 mg/dL
MCH 15.28 pg TP 7.0 g/dL
MCHC 30.1 g/dL ALB 3.3 g/dL
RDW 19.7% GLOB 3.7 g/dL
%RETIC 0.3 ALT 62.0 U/L
RETIC 29.2 K/lL ALKP 52.0 U/L
WBC 8.09 K/lL TBIL 0.1 mg/dL
%NEU 76.5 CHOL 160.0 mg/dL
%LYM 11.6 AMYL 861.0 U/L
%MONO 8.9 GLU 161.0 mg/dL*
%EOS 2.4
%BASO 0.6
NEU 6.19 K/lL
LYM 0.94 K/lL
MONO 0.72 K/lL
EOS 0.19 K/lL
BASO 0.05 K/lL
PLT 302.0 K/lL
MPV 10.2 fL
PDW 17.9%
PCT 0.3%
*Denotes an abnormal value.
Fatal Pandemic (H1N1) 2009 Influenza A in a Domestic Cat E. R. Campagnolo et al.
502 Published 2011. This article is a US Government work and is in the public domain in the USA. • Zoonoses Public Health. 58 (2011) 500–507

Diagnostic laboratory testing
Influenza virology
The nasal swabs collected on 6 November 2009 were
transferred to individual sterile Universal Transport
Media (UTM) tubes (3 mL, Diagnostic Hybrids, Athens,
OH, cat #) and shipped overnight on frozen cold packs
to the BOL. On receipt, the swabs in UTM were mixed
vigorously for 30 s then manually extracted for viral RNA
using QIAamp Viral RNA Mini kit (QIAGen Sciences,
Maryland) following the manufacturer’s protocol. The
extract from each specimen was then tested by real time
RT-PCR (rRT-PCR) for influenza virus using the CDC
Swine Influenza Protocol (CDC, 2010). These specimens
were found to be below the detection limit used to iden-
tify 2009 influenza pH1N1 viral RNA and were read as
negative.
The necropsy tissues were received at the BOL for fur-
ther testing on 10 November 2009. The heart had already
been cut open but the tongue, trachea, bronchi and lungs
were intact. Using aseptic technique, four specimens were
collected for rRT-PCR analysis: a swab specimen from the
interior surface of the trachea; a tissue specimen (approx-
imately 5-mm square by 1- to 2-mm thick) from the
heart interior spanning a portion of the ventricles and
atria; a swab specimen from the interior of both branches
of bronchi; and a combined tissue specimen from both
lungs. Remaining tissue was frozen at )20�C, and then
subsequently transferred to )70�C freezer 24 h later.
All four specimens were transferred aseptically to indi-
vidual sterile tubes of UTM. The two tissue specimens in
UTM were processed using sterile 15 mL conical tissue
grinders (VWR International). The two swab specimens
were processed as described previously. Aliquots of the
tissue or swab supernatant solution were then manually
extracted and tested for 2009 influenza pH1N1 as
described above. All four necropsy specimens tested posi-
tive for the 2009 pH1N1 virus. Confirmatory tests were
repeated using fresh extracts.
On 18 November 2009, the remaining frozen cat tissue
samples were shipped from the BOL to the United States
Department of Agriculture (USDA), National Veterinary
Services Laboratories (NVSL) in Ames, Iowa. The clinical
specimens were tested by rRT-PCR for the presence of
the influenza matrix gene and for the pandemic neur-
aminidase gene (NVSL-SOP-BPA-9024, 2009; NVSL-SOP-
BPA-9034, 2010; NVSL-SOP-BPA-9035, 2010).
Samples were also inoculated onto Madin–Darby
Canine Kidney cells for virus isolation. Isolated viruses
were tested by both PCRs. The hemagglutinin, neuramini-
dase, and matrix genes were sequenced and found to be
the 2009 pandemic H1N1 virus. On 20 November 2009,
positive Matrix PCR, positive N1 PCR, positive virus iso-
lation, and genetic sequencing results were reported out
by NVSL for all tissue samples, including heart, tongue,
trachea, bronchi and lungs.
The lung tissue submitted to the Pennsylvania Veteri-
nary Laboratory (PVL) was also examined for bacterial
infection by culture, and for mycoplasma spp. infection
by PCR (Harasawa et al., 1986) with negative findings.
Immunohistochemistry
Immunohistochemistry was performed by the PVL using
a polyclonal swine influenza antibody purchased from
Iowa State University, a Dako LSAB2 HRP staining sys-
tem, and NovaRED� chromagen. Histopathology of the
lung section showed moderately severe diffuse acute fibr-
inous pneumonia showing strands of fibrin in alveolar
spaces, bronchi and bronchioles. A few inflammatory cells
including neutrophils and macrophages were also located
(b)
(a)
Fig. 1. Left lateral (a) and ventrodorsal (b) radiographic views of a
12-year-old neutered domestic cat with pH1N1 virus infection, 5
November 2009 (2 days after the onset of first clinical signs).
E. R. Campagnolo et al. Fatal Pandemic (H1N1) 2009 Influenza A in a Domestic Cat
Published 2011. This article is a US Government work and is in the public domain in the USA. • Zoonoses Public Health. 58 (2011) 500–507 503

in the alveolar spaces, bronchi and bronchioles. Both
macrophages and bronchiolar epithelial cells in the lung
tissue section showed staining of influenza antigen further
confirming the lung infection with H1N1 influenza virus.
Contacts
At the time the ill cat was seen and hospitalized at the
veterinary clinic, six staff members were present in the
hospital. There were also three dogs that were caged in
the same observation room as the sick cat. Neither the
veterinary hospital staff, nor the hospitalized animals, at
any time developed ILI.
Discussion
This case report suggests that infection with pandemic
H1N1 influenza virus may be associated with severe and
fatal illness in domesticated cats. The Pennsylvania cat
became ill near the peak of pH1N1 activity during the fall
2009 wave, and most likely was infected by ill humans in
the household.
The gross necroscopy findings suggested to the attend-
ing veterinarian that the cat had underlying cardiac dis-
ease. Because heart tissue was not submitted for
histopathologic evaluation, it is not clear whether the
cat’s sudden death resulted from pH1N1 influenza-associ-
ated myocarditis or from pH1N1 influenza exacerbating
the underlying cardiac disease. The former is a well
known and fatal complication of influenza infections in
humans (Nolte et al., 2000; Greaves et al., 2003; Kitaura
et al., 2003; Kuiken and Taubenberger, 2008; Bratincsak
et al., 2010; Gross et al., 2010), and should be considered
in mammals kept as family pets and exposed to humans
with ILI.
Sudden death has been reported in both humans and
animals infected with influenza A virus. During the resur-
gence and spread of Highly Pathogenic Avian Influenza
H5N1 in Asia in 2004, this occurred in big cats at a zoo
in Thailand (FAO, 2010; WHO, 2010), when two tigers
and two leopards fed fresh chicken carcasses died unex-
pectedly, and H5N1 virus was identified in tissue samples
collected at necropsy (AVMA, 2009; WHO, 2010). In
humans, there have also been reports of sudden pH1N1
paediatric deaths in the absence of ILI, primarily linked
to fulminant viral myocarditis (Nolte et al., 2000; Gross
et al., 2010). The possibility that pH1N1-infected domes-
tic cats can also experience sudden death from viral
myocarditis should be further assessed if more tissue
specimens are made available from suspected cases.
As part of the differential diagnosis, a co-infection with
Feline Calicivirus (FVC) and/or Feline Herpesvirus I
(FHV-I) was also considered. Together, these pathogens
are responsible for approximately 80–90% of all feline
respiratory disease complex, and could have exacerbated a
co-infection with pH1N1, possibly leading to the cat’s
demise. Histopathology ruled out infection with FHV-I
because of the absence of intra-nuclear inclusion bodies
or syncitia in the lung tissue samples; these findings are a
hallmark of herpesvirus infection. FCV infection was also
ruled out because of the absence of clinical signs com-
monly observed with this disease, such as lameness and
ulceration of the tongue, mouth and palate.
Regardless of the cause of death in this cat, veterinari-
ans should remain alert to the possibility of pandemic
influenza virus infection in animals during periods of
community influenza activity. The index of suspicion
should be especially high when concomitant ILI is
reported in their human contacts.
Until recently, domestic cats had been considered rela-
tively resistant to influenza virus infections (Hinshaw
et al., 1981; Lohr et al., 2010). Current reports indicate
that cats, naturally or experimentally infected with Highly
Pathogenic Avian Influenza Virus H5N1, exhibit clinical
signs indicating both a respiratory and systemic involve-
ment (Kuiken et al., 2004; Rimmelzwaan et al., 2006;
Klopfleisch et al., 2007; Lohr et al., 2010). To date, there
have been too few documented cases of laboratory-con-
firmed pH1N1 infection in domestic cats to describe a
‘typical’ clinical presentation of pH1N1 infection. Table 3
represents a compilation of clinical signs in laboratory-
Table 3. Clinical signs reported in domestic cats with laboratory-confirmed 2009 pH1N1 influenza, USA, October 2009 to January 2010
State
Human
ILI Anorexia Cough Cyanosis Death Dehydration Dyspnoea Fever Lethargy Rhinorrhea Sneezing Wheezing
OR 4 4 4 4 4 4 4 4
OR 4 4 4 4 4 4 4
PA 4 4 4 4 4 4 4
IA 4 4 4 4
CA 4 4 4 4
CO 4 4 4
CO 4 4 4
UT 4 4
Total 8 (100%) 2 (25%) 1 (12.5% 1 (12.5%) 3 (37.5%) 4 (50%) 4 (50%) 0 (0%) 3 (37.5%) 5 (62.5%) 5 (62.5%) 2 (25%)
Fatal Pandemic (H1N1) 2009 Influenza A in a Domestic Cat E. R. Campagnolo et al.
504 Published 2011. This article is a US Government work and is in the public domain in the USA. • Zoonoses Public Health. 58 (2011) 500–507

confirmed pH1N1 infections reported from October
2009 through January 2010 in domestic cats by the
AVMA (2009) and by the Pennsylvania cat’s attending
veterinarian.
All pet cats (100%) in Table 3 had contact with
humans with reported ILI, and three (37.5%) died. The
most common clinical signs were dyspnoea (50%), rhin-
orrhea (nasal discharge) (62.5%) and sneezing (62.5%);
100% of cats had at least one respiratory symptom, simi-
lar to what is seen with pH1N1 infection in other animal
species, particularly swine. Histopathology conducted on
the lung tissues samples obtained from the two feline
fatalities in Oregon indicated that both domestic cats had
necrotizing bronchointerstitial pneumonia (Lohr et al.,
2010).
The two large dogs living in the same household as the
sick Pennsylvania cat were reported as healthy. Although
also susceptible to pH1N1 infection, and exposed to the
same ill humans, the dogs did not develop any clinical
signs of illness. The varying degree of contact with house-
hold members could explain this difference, as could dif-
ferential susceptibility of dogs and cats to the 2009
pH1N1 virus. As the two dogs never exhibited clinical
signs of illness, veterinary clinical follow up and serologi-
cal testing to search for evidence of pH1N1 infection were
not pursued.
Antiviral drugs were not administered to the sick cat
despite concerns of pH1N1 infection. Oseltamivir has
not been approved by the Food and Drug Administra-
tion (FDA) for use in pets; however, extra-label use by
veterinarians is allowed on a case-by-case basis, under
the provisions of the Animal Medicinal Drug Use Clarifi-
cation Act (AMDUCA) of 1994 (FDA, 1994; AVMA,
2007). The AVMA guidelines indicate that decisions
regarding the use of oseltamivir in animals should be
based on both the severity of the animal’s illness and the
veterinarian’s clinical judgment. Many veterinary practi-
tioners did not prescribe antiviral drugs during the
H1N1 pandemic out of concern about the potential for
the development of antiviral drug resistance due to inap-
propriate or excessive use. Another concern was that
oseltamivir is the only influenza antiviral drug with wide
applicable use in humans, for whom use of oseltamivir is
associated with reduced mortality in severely ill persons.
However, based on documented fatalities associated with
pH1N1 infection in companion animals that were not
administered antivirals, consideration should be given to
defining situations better where antiviral administration
may be appropriate.
Although there was no evidence that the cat transmit-
ted the virus back to people or to the other animals in
the household, this potential exists. Therefore, veterinary
hospital staff should always make use of good infection-
control practices when handling animals potentially har-
bouring a zoonotic or animal-to-animal transmissible dis-
ease. These practices include the use of exam gloves and
other personal protective equipment, as appropriate, a
dedicated Infectious disease exam room that is sanitized
between animals, and careful hand Hygiene when
handling animals or when cleaning up after pets (CDC,
2009a,b, AVMA, 2010). Pet owners and veterinary hospi-
tal staff diagnosed with pH1N1 infection, or exhibiting
clinical signs of ILI, should limit their close contact expo-
sure to pets, and should practice appropriate respiratory
protection, and hand sanitation.
During an influenza pandemic, it would be advisable
for veterinary public health staff to establish a standard
series of influenza-related health questions for veterinary
clinical staff to ask if pets or pet owners are exhibiting
ILI. This would provide the opportunity for trained veter-
inary staff to discuss with pet owners ways of reducing
spread of infection. In order to limit exposure to other
animals, co-workers, or other clients, appointments for
pets with ILI could be scheduled towards the time of the
work day, when such exposure would be minimal.
Although not generally feasible in most practice settings,
a separate entrance and respiratory isolation area could
be made available for animals with respiratory illness.
Nasopharyngeal swabs are generally considered to be
the optimal specimens for animals with suspected influ-
enza. However, nasopharyngeal swabbing was difficult in
the Pennsylvania cat as there was no nasal discharge and
the swabs turned out to be negative. In circumstances
where the index of suspicion for influenza is high and
nasal discharge is minimal, consideration should be given
to obtaining specimens by means of nasal washes, and
collecting specimens from other sites, including the oro-
pharynx, for influenza testing.
Conclusion
We report the earliest laboratory-confirmed feline fatality
from the pH1N1 virus in the United States and postulate
that the abrupt death of this previously healthy in-door
domestic cat from Pennsylvania, presented to a veterinary
clinic with mild respiratory signs, suggests a cardiac com-
ponent to this pH1N1 infection, similar to what has been
document in big cats and humans as the gross appearance
of the heart during the necropsy/autopsy. Veterinary
practitioners may want to consider the findings presented
in this report while formulating a differential diagnosis
when confronted with a domestic cat with similar clinical
signs during a period of human pH1N1 illness.
Furthermore, the ‘One Health’ concept (Marano and
Pappiaoanou, 2004; AVMA, 2008; One Health Initiative,
2008; Hristovski et al., 2010), which includes the merging
E. R. Campagnolo et al. Fatal Pandemic (H1N1) 2009 Influenza A in a Domestic Cat
Published 2011. This article is a US Government work and is in the public domain in the USA. • Zoonoses Public Health. 58 (2011) 500–507 505

of perspectives from the human and the veterinary medi-
cal disciplines, was exemplified by this investigation. This
particular case underlined the importance of the coopera-
tion, collaboration, and interactions between human pub-
lic health, veterinary public health, medical and veterinary
diagnostic laboratories, and the veterinary medical
practice, when dealing with cases of an emerging zoonotic
disease.
Acknowledgements
We thank the following for their contributions to this inves-
tigation: Dr. David V. Daverio, Dr. Sabrina L. Swenson, Dr.
Andre‘ C. Weltman, Dr. Kumar Nalluswami, Dr. Amy J.
Nesselrodt, Dr. Kirsten Waller, Dr. Virginia M. Dato, Mr.
Owen Simwale, Ms. Jamie Orres and Mr. Jerry Grabigel.
References
AVMA, 2007: Extralabel Drug Use (ELDU). An Information
Outline of the Animal Medicinal Drug Use Clarification Act
(AMDUCA). Brochure, Schaumburg, IL.
AVMA, 2008: One Health: A New Professional Imperative.
One Health Initiative Task Force: Final Report. July 15.
Schaumburg, IL.
AVMA, 2009: Public Health: Frequently Asked Questions
About 2009 H1N1 Flu Virus. Available at: http://www.
avma.org/public_health/influenza/new_virus/default.asp
(accessed on 15 April 2010).
AVMA, 2010: Public Health: Frequently Asked Questions
About 2009 H1N1 Flu Virus. Available at: http://www.
avma.org/public_health/influenza/new_virus/new_flu_
virus_faq_pet_owners.asp (accessed on 15 April 2010).
Bratincsak, A., H. G. El-Said, J. S. Bradley, K. Shayan, P. D.
Grossfeld, and C. R. Cannavino, 2010: Fulminant myocardi-
tis associated with pandemic H1N1 influenza A virus in
children. J. Am. Coll. Cardiol. 55, 928–929.
CDC, 2009a: H1N1 Flu (Swine Flu). Available at: http://
www.cdc.gov/h1n1flu/ (accessed on 14 January 2010).
CDC, 2009b: Compendium of Measures to Prevent Disease
Associated with Animals in Public Settings, 2009.
MMWR.National Association of State Public Health Veteri-
narians, Inc. (NASPHV), Atlanta, GA, USA. May1/Vol.58/
No.RR-5.
CDC, 2010: H1N1 Flu (Swine Flu): Resources for Laboratories.
CDC Protocol of Realtime RTPCR for Swine Influenza
A(H1N1). Available at: http://www.cdc.gov/h1n1flu/lab/
(accessed on 5 May 2010).
FAO, 2010: H5N1 in Cats. Available at: http://www.fao.org/
avianflu/en/wildlife/wild_animals.htm (accessed on 23 April
2010).
FDA, 1994: Animal Medicinal Drug Use Clarification Act
(AMDUCA) of 1994. Federal Food, Drug, and Cosmetic Act
(FD&C Act). January 25. Washington, DC.
Garten, R. J., C. T. Davis, C. A. Russell, B. Shu, S. Lindstrom,
A. Balish, W. M. Sessions, X. Xu, E. Skepner, V. Deyde, M.
Okomo-Adhiambo, L. Gubareva, J. Barnes, C. B. Smith, S.
L. Emery, M. J. Hillman, P. Rivailler, J. Smagala, M. de
Graaf, D. F. Burke, R. A. M. Fouchier, C. Pappas, C. M.
Alpuche-Aranda, H. Lopez-Gatell, H. Olivera, I. Lopez, C.
A. Myers, D. Faix, P.J. Blair, C. Yu, K. M. Keene, P. D.
Dotson Jr., D. Boxrud, A. R. Sambol, S. H. Abid, K. St.
George, T. Bannerman, A. L. Moore, D. J. Stringer, P.
Blevins, G. J. Demmler-Harrison, M. Ginsberg, P. Kriner, S.
Waterman, S. Smole, H. F. Guevara, E. A. Belongia, P. A.
Clark, S. T. Beatrice, R. Donis, J. Katz, L. Finelli, C. B.
Bridges, M. Shaw, D. B. Jernigan, T. M. Uyeki, D. J. Smith,
A. I. Klimov, and N. J. Cox, 2009: Antigenic and genetic
characteristics of swine-origin 2009 A(H1N1) influenza
viruses circulating in humans. Science 325, 197–201.
Greaves, K., J. S. Oxford, C. P. Price, G. H. Clarke, and T.
Crake, 2003: The prevalence of myocarditis and skeletal
muscle injury during acute viral infection in adults: mea-
surement of cardiac troponins I and T in 152 patients with
acute influenza infection. Arch. Intern. Med. 163, 165–168.
Gross, E. R., J. W. Gander, A. Reichstein, R. A. Cowles, C. J.
Stolar, and W. Middlesworth, 2010: Fulminant pH1N1-09
influenza-associated myocarditis in pediatric patients.
Pediatr. Crit. Care Med. 12, 1–3.
Harasawa, R., H. Mizusawa, and K. Koshimizu, 1986: A reli-
able and sensitive method for detecting mycoplasmas in cell
cultures. Microbiol. Immunol. 30, 919–921.
Hinshaw, V. S., R. G. Webster, B. C. Easterday, and W. J.
Bean, 1981: Replication of avian influenza A viruses in
mammals. Infect. Immun. 34, 354–361.
Hristovski, M., A. Cvetkovik, I. Cvetkovik, and V. Dukoska,
2010: Concept of one health – a new professional impera-
tive. Maced. J. Med. Sci. 3, 229–232.
Kitaura, Y., H. Deguchi, F. Terasaki, A. Ukimura, H. Morita,
and T. Tatsumi, 2003: Influenza myocarditis–pathophysio-
logy and developmental mechanism of myocarditis. Nippon
Rinsho. 61, 1945–1952.
Klopfleisch, R., P. U. Wilf, W. Uhl, S. Gerst, T. Harder, E. Sta-
rick, T. W. Vahlenkamp, T. C. Mettenleiter, and J. P. Teifke,
2007: Distribution of lesions and antigen of highly patho-
genic avian influenza virus A/Swan/Germany/R65/06
(H5N1) infection in domestic cats after presumptive infec-
tion by wild birds. Vet. Pathol. 44, 261–268.
Kuiken, T., and J. K. Taubenberger, 2008: Pathology of human
influenza revisited. Vaccine 26 (Suppl 4), D59–D66. Review.
Kuiken, T., G. Rimmelzwaan, D. van Riel, G. van Amerongen,
M. Baars, R. Fouchier, and A. Osterhaus, 2004: Avian H5N1
influenza in cats. Science 306, 241.
Lohr, C. V., E. E. DeBess, R. J. Baker, S. L. Hiett, K. A. Hoff-
man, V. J. Murdoch, K. A. Fischer, D. M. Mulrooney, R. L.
Selman, and W. M. Hammill-Black, 2010: Pathology and
viral antigen distribution of lethal pneumonia in domestic
cats due to pandemic (H1N1) 2009 influenza A virus. Vet.
Pathol. 47, 378–386.
Fatal Pandemic (H1N1) 2009 Influenza A in a Domestic Cat E. R. Campagnolo et al.
506 Published 2011. This article is a US Government work and is in the public domain in the USA. • Zoonoses Public Health. 58 (2011) 500–507

Marano, N., and M. Pappiaoanou, 2004: Historical, new, and
reemerging links between human and animal health. Emerg.
Infect. Dis. 10, 2065–2066.
Nolte, K. B., P. Alakija, G. Oty, M. W. Shaw, K. Subbarao, J.
Guarner, W. J. Shieh, J. E. Dawson, T. Morken, N. J. Cox,
and S. R. Zaki, 2000: Influenza A virus infection compli-
cated by fatal myocarditis. Am. J. Forensic Med. Pathol. 21,
375–379.
NVSL-SOP-BPA-9024, 2009: 2009 H1N1 Influenza Virus Isola-
tion. Ames, Iowa.
NVSL-SOP-BPA-9034, 2010: Real-Time Rt-Pcr for the Detec-
tion of Swine Influenza Virus and Identification of Novel
N1 Subtypes in Clinical Samples. Ames, Iowa.
NVSL-SOP-BPA-9035, 2010: Amplification and Purification of
PCR Products for Direct Sequencing of Hemagglutinin,
Neuraminidase and Matrix Genes of Swine Influenza Virus.
Ames, Iowa.
One Health Initiative, 2008: One Health Initiative will Unite
Human and Veterinary Medicine. Available at: http://
www.onehealthinitiative.com/index.php (accessed on 2
February 2010).
Pennsylvania Department of Health Bureau of Laboratories
BOL, 2009: 2008/09 Influenza Virology Surveillance Data.
Pennsylvania Laboratory Information Management System
(LIMS) Available at: http://www.portal.state.pa.us/portal/
server.pt/community/laboratories/14158. (accessed 9 Apr
2010).
Pereda, A., J. Cappuccio, M. A. Quiroga, E. Baumeister, L.
Insarralde, M. Ibar, R. Sanguinetti, M. L. Cannilla, D.
Franzese, O. E. Escobar Cabrera, M. I. Craig, A. Rimondi,
M. Machuca, R. T. Debenedetti, C. Zenobi, L. Barral, R.
Balzano, S. Capalbo, A. Risso, and C. J. Perfumo, 2010:
Pandemic (H1N1) 2009 outbreak on a pig farm, Argentina.
Emerg. Infect. Dis. 16, 304–307.
ProMED, 2009a: Archive Number 20091020.3600. Available at:
http://www.promedmail.org/pls/apex/f?p = 2400:1001:2922
133396374024::::F2400_P1001_BACK_PAGE,F2400_P1001_
ARCHIVE_NUMBER,F2400_P1001_USE_ARCHIVE:1001,
20091020.3600,Y.
ProMED, 2009b: Archive Number 20091128.4079. Available at:
http://www.promedmail.org/pls/apex/f?p = 2400:1001:2922
133396374024::::F2400_P1001_BACK_PAGE,F2400_P1001_
ARCHIVE_NUMBER,F2400_P1001_USE_ARCHIVE:1001,
20091128.4079,Y.
ProMED, 2009c: Archive Number 20091115.3947. Available at:
http://www.promedmail.org/pls/apex/
f?p = 2400:1001:2922133396374024::::F2400_P1001_BACK_
PAGE,F2400_P1001_ARCHIVE_NUMBER,F2400_P1001_
USE_ARCHIVE:1001,20091115.3947,Y.
ProMED, 2009d: Archive Number 20091105.3816. Available at:
http://www.promedmail.org/pls/apex/
f?p = 2400:1001:::NO::F2400_
P1001_BACK_PAGE,F2400_P1001_PUB_MAIL_ID:1000,
79947.
Rimmelzwaan, G., D. van Riel, M. Baars, T. M. Bestebroer, G.
van Amerongen, R. Fouchier, A. Osterhaus, and T. Kuiken,
2006: Influenza A (H5N1) infection in cats causes systemic
disease with potential novel routes of virus spread within
and between hosts. Am. J. Pathol. 168, 176–183.
Sponseller, B. A., E. Strait, A. Jergens, J. Trujillo, K. Harmon,
L. Koster et al., 2010: Influenza pandemic (H1N1) 2009
virus infection in domestic cat. Emerg. Infect. Dis. 16, 534–
537.
USDA, 2009: Final results 2009 Pandemic H1N1 Influenza.
Available at: http://www.usda.gov/documents/
FINAL_RESULTS_2009_PANDEMIC_H1N1_INFLUENZA_
CHT.pdf (accessed on 8 April 2010).
USDA, 2010: Final Results 2010 Pandemic H1N1 Influenza.
Available at: http://www.usda.gov/documents/H1N1_INFLU-
ENZA_CHART_SAMPLES_FOR_CY2010_032210.pdf
(accessed on 8 April 2010).
USDA-APHIS, 2010: H1N1 Influenza. Available at: http://
www.aphis.usda.gov/newsroom/hot_issues/h1n1/ (accessed
on 2 February 2010).
WHO, 2010: H5N1 Avian Influenza: Timeline. Available at:
http://www.who.int/csr/disease/avian_influenza/timeline.pdf
(accessed on 23 April, 2010).
E. R. Campagnolo et al. Fatal Pandemic (H1N1) 2009 Influenza A in a Domestic Cat
Published 2011. This article is a US Government work and is in the public domain in the USA. • Zoonoses Public Health. 58 (2011) 500–507 507