FEMTOSECOND LASER CATARACT SURGERY. Revolution, Evolution, or No Solution? Making Sense of the Literature Ken Lipstock, M.D. Richmond, Virginia. F. emtosecond laser provides an ultrafast burst of energy. Argon, excimer, and Nd: YAG lasers: nanosecond (10 ) pulses - PowerPoint PPT Presentation
FEMTOLASER CATARACT SURGERY
FEMTOSECOND LASER CATARACT SURGERYRevolution, Evolution, or No
Solution?Making Sense of the Literature
Ken Lipstock, M.D.Richmond, Virginia1emtosecond laser provides
an ultrafast burst of energy.
Argon, excimer, and Nd: YAG lasers: nanosecond (10 ) pulses
Femtosecond: 10 second
Excimer: photoablates
Argon: photocoagulates
Nd: YAG and Femtosecond: photodisrupt. Their light energy can be
absorbed by optically clear tissue and create microcavitation
bubbles that cause an acoustic shock wave that incises the target
tissue.
F-9-15Femtosecond lasers ultrafast pulse allows smaller amounts
of energy to provide similar power output to the NdYag. This
results in much smaller cavitation bubbles therefore reduced
collateral damage to adjacent tissues.Femtosecond laser first FDA
approved for LASIK flaps in 2001 and then approved for cataract
surgery in 2010.
With guidance systems (OCT or Scheimpflug-like technology) it is
used to make: Cataract clear corneal incisions and limbal relaxing
incisions
Capsulorhexis
Lens fragmentation/softening; a pretreatment prior to
phacoemulcification and/or irrigation/aspiration.Mistrust but
VerifyWe are witnessing one of the most intense marketing campaigns
ever in Ophthalmology.And this is a sentence from a scientific
study in a respected peer reviewed journal!
Is Femtolaser Cataract Surgery the most important evolution
since the transition to phacoemulsification?
Much has been claimed but how much is substantiated?
In the following presentation I will review the literature to
try to shed some light on the subject. Since the vast majority of
journal articles are written by those with financial ties to the
femtosecond companies, the authors of the journal articles will be
color coded red for financial ties and green if not. (The lead
author will be in red if at least one of the authors has financial
ties.)It has automated, computer-guided laser precision with
minimal collateral tissue damage......with emerging evidence of
......greater precision and accuracy of the anterior capsulotomy,
and more stable and predictable positioning of the intraocular
lens.CompanyMode of dockingImagingLensSxAlcon, Ca.Curved glass at
first, now uses soft contact interfaceOCT
LensARPrivately HeldOrlando, Fl.2 piece non contact
interfaceScheimpflug-likeCatalysAMO, Ca.Liquid-optics
interfaceOCTVictusB & LCurved glass
interfaceOCTCapsulorhexisHypothesis: a capsulorhexis (rhexis)
should overlap the IOL optic approximately .5 mm symmetrically 360
degrees and be larger than 4 mm . This will give a better and more
consistent effective lens position (ELP) because of less asymmetric
contractile force from the fibrosing anterior capsule on the IOL.
The IOL should then not position more anteriorly or posteriorly
than anticipated or with decentration or tilt. A better ELP leads
to:
Closer to targeted spherical equivalent and less cylindera.
Better uncorrected distance vision (UCDVA)
2. Less higher order aberrations like spherical aberration and
tilta. Better corrected distance vision (CDVA)b. Better quality of
vision with less glare, halos, and better contrast
sensitivity.1,2,37Claim of the Femtolaser Companies:The femto
anterior capsulotomy is more precise (consistent) and more accurate
than a manual curvilinear capsulorhexis (CCC).Better size, more
circular, better centered thus better overlap of the IOL. And
better overlap yields less IOL decentration and tilt and better
anterior-posterior position. 4,5
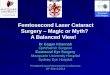
45Assymetric OverlapDecentered IOLCCC vs. Femto ButtonsFriedman;
JCRS; 2011Kranitz; JRS; 2011 Continuous curvilinear capsulorhexis
(CCC) technique was developed simultaneously by Neuhann in Germany
and Gimbel in Canada around 1987. 6,7 Prior rhexis techniques (eg.
can opener) led to 100% anterior capsular tears during cataract
surgery and CCC tear rate approached 0%. 8 Prior to CCC capsular
tears led to IOLs with haptics commonly with one in the bag and one
in the sulcus or with both in the sulcus. Scientific
BackgroundContinuous Curvilinear Capsulotomy: A Revolutionary
Change for IOL Positioning9Assia, Apple (Oph 1993) showed:
Bag-Sulcus Fixation mean Decentration= .64 .39mm (range up to
1.76mm)Note: 1 SD =66.6% thus: 1.0mm decentration was common
Bag-bag Fixation mean Decentration= .18 .09IOLMean dec.Mean
tiltAkkin (1994)0.151.1Hayashi (1997)MZ60BD0.27 .152.62
1.33SI30NB.30 .162.53 1.36MA60BM.30 .152.71 1.84Mutlu (1998)0.28
.142.83 .89Kim (2001)MZ60BD0.31 .152.67 .84SI-30NB0.32 .182.61
.83AcrySof MA60BM0.33 .192.69 .87Taketani (2004)AcrySof MA30BA0.30
.173.43 1.55Baumeister (2005)CeeOn 911A0.24 .133.03 1.79PhacoFlex
SI-400.23 .133.26 1.69CeeOn 911A0.29 .212.34 1.81AcrySof MA60BM0.24
.102.32 1.41Mutlu (2005)AcrySof SA30AL0.34 .082.70 .55AcrySof
MA30BA0.39 .132.72 .84Rosales (2006)UNKNOWN0.25 .28.87 2.16de
CastroUNKNOWN0.34 .192.34 .97Baumeister (2009)AR40C0.19 .122.89
1.46Z90000.27 .162.85 1.36Hayashi (2014)H60M0.25 .174.88
1.45MA60BM0.28 .164.85 1.5210Mean IOL decentration 0.28 .16 mm and
tilt 2.61 1.2Mean follow-up= 12.2 months Range= 3 to 48 months
Clinical Studies in the CCC Era Measuring IOL Decentration and
TiltHow Much Does 0.28 .16mm Decentration and 2.6 1.2 Tilt Effect
Vision?Let`s look at the Non-Femto Literature first.Would even less
decentration and tilt provide better UCVA and CDVA?Would even less
decentration and tilt provide better contrast sensitivity and less
glare and halos?Would even less decentration and tilt have more or
less effect depending on whether the IOL is spherical, negative
aspheric, neutral aspheric, accommodating, multifocal?Remember:
Femto Companies Claim Better Rhexis Better ELP Better Vision
Better Vision can mean both smaller refractive error and better
quality of CDVA.
Okada has shown that a better rhexis does NOT lead to a Smaller
Refractive Error (spherical equivalent or cylinder.)
Okada (Oph 2014) : Does the Rhexis Circularity or Centration
effect Post-op Refractive Error? 93 eyes Phaco mostly by residents
Pre-op spherical equivalent -7.75 to +4.50 Alcon Spherical IOL
(SN60AT)Results for One Month and 1 yearMeasurements: Rhexis
Circularity (comparison to perfect circle; ratio 1.0=perfect)
Rhexis (not IOL) Decentration from pupil center Complete Overlap of
Rhexis (360 over the IOL Optic) yes or no
111 Monthmean1 Yearmean from 1 month 1 yearCircularity.83 .01.87
.03p < .001Decentration (mm).30 .14.23 .13p < .001360 overlap
(% of eyes)88%90%p = .02Okada Results (Contd):(StabilizationChange
from 1 Month to 1 Year)Over time the rhexis became more circular,
less decentered and with more overlap.Circularity of Rhexis NO
significant correlation of circularity with post-op target
spherical equivalent at 1 month or 1 year
NO significant correlation of circularity with post-op cylinder
at 1 month or 1 yearOkada Results (Contd)Decentration of Rhexis
NO correlation with change in cylinder from 1 month to 1 year.
It did correlate with the change in spherical equivalent between 1
month and 1 year (p=.03).
But Bottom Line:
NO significant correlation of Decentration with post-op target
spherical equivalent at 1 month or 1 year.
NO significant correlation of Decentration with post-op cylinder
at 1 month or 1 year.
Okada Results (Contd)16360 Overlap vs. Incomplete Overlap
NO correlation with change in spherical equivalent between 1
month and 1 year. It did correlate with change in cylinder between
1 month and 1 year.
But Bottom Line:
NO significant correlation of Overlap with post-op target
spherical equivalent at 1 month and 1 year
NO significant correlation of Overlap with post-op cylinder at 1
month and 1 year
Okada Results (Contd) Rhexis Centration and Circularity and
Overlap do not correlate with Post-op Refractive error.
Rhexis Centration and Overlap do play some role in stability of
refraction but not enough to effect the average post-op refractive
error at one year.Conclusion:Effect of IOL Position on Quality of
Vision
Remember, Femto companies hypothesize: Better Overlap Better IOL
Position Better Vision
Okadas Study Showed: Better Overlap Does Not Better Refractive
Error
Question: Could Better Overlap Better Quality of Vision
Lower order Aberrations: myopia, hyperopia, astigmatism
Higher Order Aberrations (HOAs): coma, spherical aberration,
trefoil, etc. can effect the quality of vision. These are measured
with a wavefront analyzer.
Decentration and Tilt may effect Aspheric IOLs more than
spherical IOLs so we will spend some time reviewing this subject
now.
19Remember this:
The larger the pupil the more HOAs there are.
The pupil size increases in dim light and decreases with
age.
55 years old (cataract age) pupil diameter:Bright
mesopic=3.2mmMesopic=4.0mmLow Mesopic= 5.0mm12Effect of IOL
Position on Quality of Vision (Contd) The First Negative Aspheric
IOL was Tecnis (Pharmacia now AMO). Holladay and Piers did the
early theoretical research for Pharmacia. Basic Idea:
A. The amount of total eye spherical aberration could be
manipulated with an IOL because spherical aberration unlike other
HOA`s like coma and trefoil is not very sensitive to the position
of the IOL (rotation, decentration and tilt). However decentration
and tilt could still possibly effect the results.
B. The cornea has positive asphericity and this is stable
despite aging. It is approximately +.27. The lens has negative
asphericity to balance the cornea so the total eye spherical
aberration is minimized. The lens becomes more positively aspheric
after age 40 causing more total eye positive asphericity.
41 y.o. 6.0mm pupil mean s.a.=.1065 y.o. 6.0 pupil mean
s.a=.1913Effect of IOL Position on Quality of Vision (Contd)
Aspheric IOLsA spherical IOL has positive asphericity which
increases the spherical aberration of the eye. Pharmacia developed
a -.27 negative aspheric IOL (Tecnis) to eliminate total eye
spherical aberration and thereby improve the quality of vision eg.,
contrast sensitivity. Tilt and decentration can induce HOA`s but
much more in a negative aspheric IOL than a spherical IOL.
Question: Would tilt and decentration be a problem with negative
aspheric IOL`s?Holladay and Piers (JRS 2002)
They calculated the Modular Transfer Function (MTF) at different
amounts of tilt and decentration. MTF is a mathematical/theoretical
calculation of contrast (the contrast of an image relative to the
contrast of the object traveling through an optical medium). This
relates to quality of vision.
Amount of tilt and decentration of Tecnis where the MTF (quality
of vision) becomes worse than a spherical IOL:
Decentration= 4mm Tilt= 7
Holladay used monochromatic light for his calculations. In 2007
Piers corrected the calculations based on the more physiologic
polychromatic light we experience:
14Decentration= .8mmCompare to 0.28 .16mm actual mean
decentration of IOLs with a CCCTilt= 10Compare to 2.6 1.2 actual
mean tilt of IOLs with a CCC1516
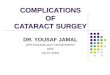
Ignore top dotted line (theoretical IOL with all HOAs
corrected)Solid line= TecnisDashed line= Spherical
IOLlawlesslawlessDecentrationTiltPolychromatic MTFPolychromatic
MTF.28
.442.63.8Decentration .28 .16 .44mmNote: Minimal effect on MTF
for most patients.0.8Tilt 2.6 1.2 3.8 Note: Tilt effects MTF even
less than decentration.10Piers GraphSpherical aberration was less
with Tecnis at all pupil sizes (the bigger the pupil the larger the
difference).
Total HOA`s were lower with Tecnis only if pupil 6.0 mm (most
cataract patients pupils are smaller) and coma and trefoil were no
different at all pupil sizes.
Even though spherical aberration was less, Tecnis gave no
improvement in CDVA photopic with high contrast charts or mesopic
low contrast charts.
Tecnis gave no improvement in Contrast Sensitivity photopic or
mesopic.
Kohnen`s team in Germany 17,18,19A series of intraindividual
studies (same patient with one eye spherical IOL and other eye
Tecnis).Aspheric IOL Clinical Studies5. Were these less than
expected results with Tecnis due to tilt and decentration?
a) The Kohnen group measured it: Tecnis: decentration= 0.27
.16mm (as expected from other studies)tilt= 2.9 1.5 (as expected
from other studies)(Decentration and Tilt of Spherical IOLs studied
were almost exactly thesame.)
b) Multiple Regression Analysis showed no statistically
significant correlation between decentration or tilt with the HOAs.
ie, Decentration and Tilt were not the reason why Tecnis performed
worse than expected.
c) This is consistent with the Piers graphs: Decentration and
Tilt with a CCC are too small to significantly effect HOAs even
with negative aspheric IOLs.
Kohnen (Contd)So why didnt Tecnis eyes see better? They had
significantly less spherical aberration and we know decentration
and tilt were too small to effect that impact. Puzzling.
Possible explanations:
a) Pupil size: average pupil in the study in mesopic conditions
was 3.8mm. Negative spherical correcting IOLs have a much larger
effect in pupils 6.0mm.
b) Interactions with other HOAs. It is not just spherical
aberration we are dealing with. Some HOAs may interact with others
in a negative or positive way.
Take home message: Factors effecting quality of vision are
complex. (Marketing companies may use that to their advantage.)
Negative aspheric IOLs are not significantly effected by
decentration and tilt for most patients.20Neutral Aspheric IOL
StudiesDeveloped Several Years Later
Concept 1. Do not add or subtract from the total eye spherical
aberration.
2. Neutral aspheric IOLs may not actually decrease the total eye
spherical aberration but they are less effected by decentration and
tilt than negative spherical IOLs.
Model Eye Study calculation of MTF with Decentration; comparing
Aspheric, Neutral Aspheric, & Spherical IOLs.Two pupil sizes
and three types of IOLs. Verticle lines = .3 and .4mm decentration
from the literature. (Mean and with one standard deviation.)
Monochromatic light (Holladay) was used. Slope should be less
narrow as per Piers/ Polychromatic light.Decentration has no effect
on neutral aspheric and spherical IOL.. Tecnis is more beneficial
in larger pupil.21
ModulationTecnisNegative AsphericModulationSoft PortNeutral
AphericModulationSpheric.4.4.4.4Eppig (JCRS 2009) 21Modulation
Modulation ModulationTilt has minimal effect on Tecnis even with
monochromatic MTF calculations.22
Swedish Multicenter Double masked study of 80 patients with
Tecnis in one eye and Neutral aspheric Akreos in the other.
Results (3 months post-op): Total HOA`s less for Tecnis for 4, 5
and 6mm pupils (p