Embed Size (px)
Citation preview
Gail Andrew, MDCM, FRCP(C)
Clinical Professor, Department of Pediatrics, University of Alberta
Medical Director FASD Clinical Services, Glenrose Rehabilitation Hospital, Alberta Health Services
Fetal Alcohol Spectrum Disorder : FASD
ELLA Course 2018
• Describes the range of deficits that can result from prenatal alcohol
exposure (PAE) causing damage to fetal cells, especially developing
brain cells
•Presents as life long difficulties: intelligence, learning (math and
reading) attention and impulsivity, higher level language (predicting,
inferencing, sequencing), memory, motor planning,
behavioral/emotional/social regulation, executive functions (flexible
thinking, inhibiting, shifting) that impacts judgment and decision making
based on past experiences
• History: • Biblical (Job 13.7) and art references
• First articles: 1968 & 73 linking brain damage from PAE to disability
• Slow translation from research to practice
• Guidelines: Institute of Medicine 1996, Canadian 2005 & 2015, DSM 5
• Prevalence: • 2 to 5 % general population: underestimated, lack of diagnostic capacity
• Higher in high risk: foster care 34%, justice 25 %, African studies (May)
• Risk: • Alcohol use in pregnancy: prevention messaging without blaming;
societal role “Have a Dry 9”
• No ethnic group spared but stigma and attitude (Frameworks study)
• SDOH: poverty, multigenerational trauma, lack of supports
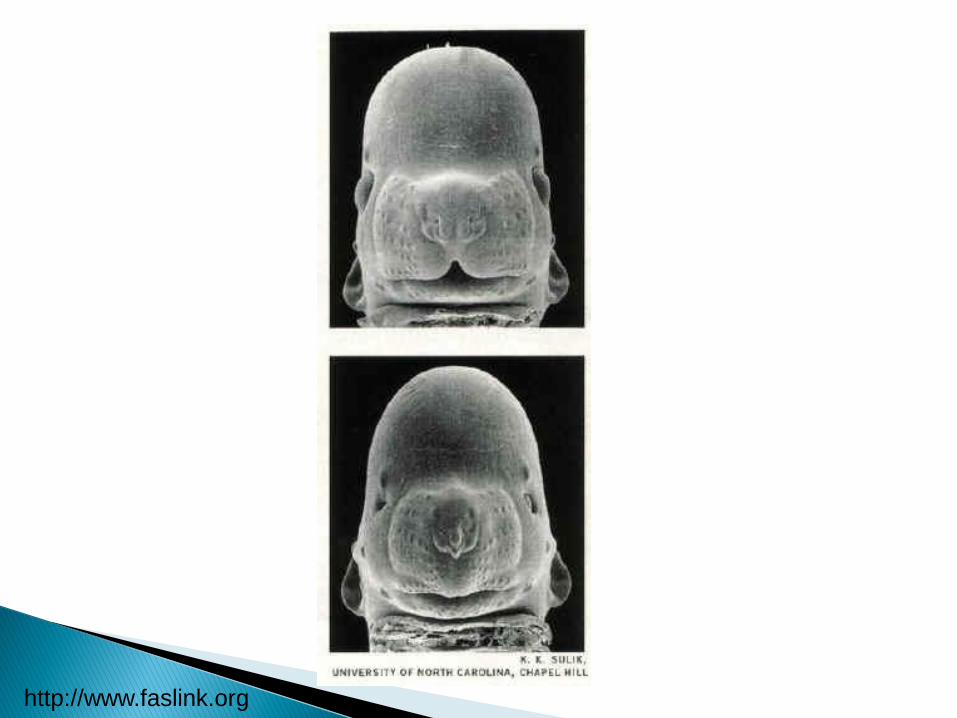
• Animal models (Weinberg, Sulik, Thomas)
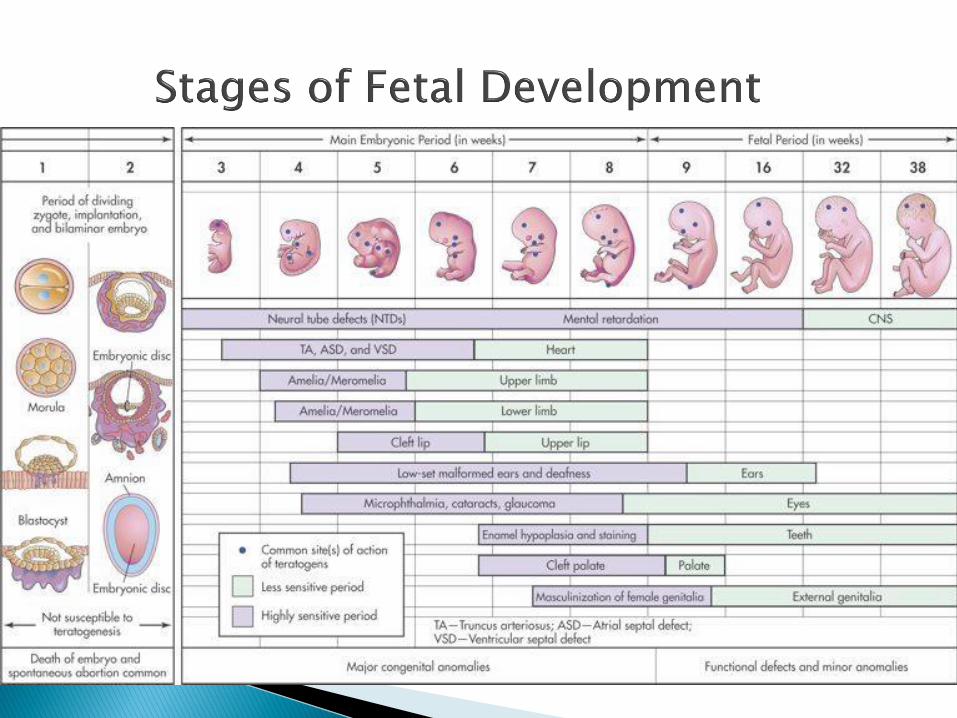
• Spectrum of damage depends on amount, binge pattern, timing
in gestation, maternal and fetal genetic and epigenetic factors,
maternal nutrition and stress
• Control all variables in the rat lab vs real life?
• What about safety of low level drinking - need data!
• Facial features of FAS impacted day 19 to 21 (slides)
• Protective factors: Choline and iron supplements?
• ARBD: total body disorder/multisystem involvement with later
impact on adult immune and metabolic diseases, possibly early
onset dementia, shorter life span (slide)
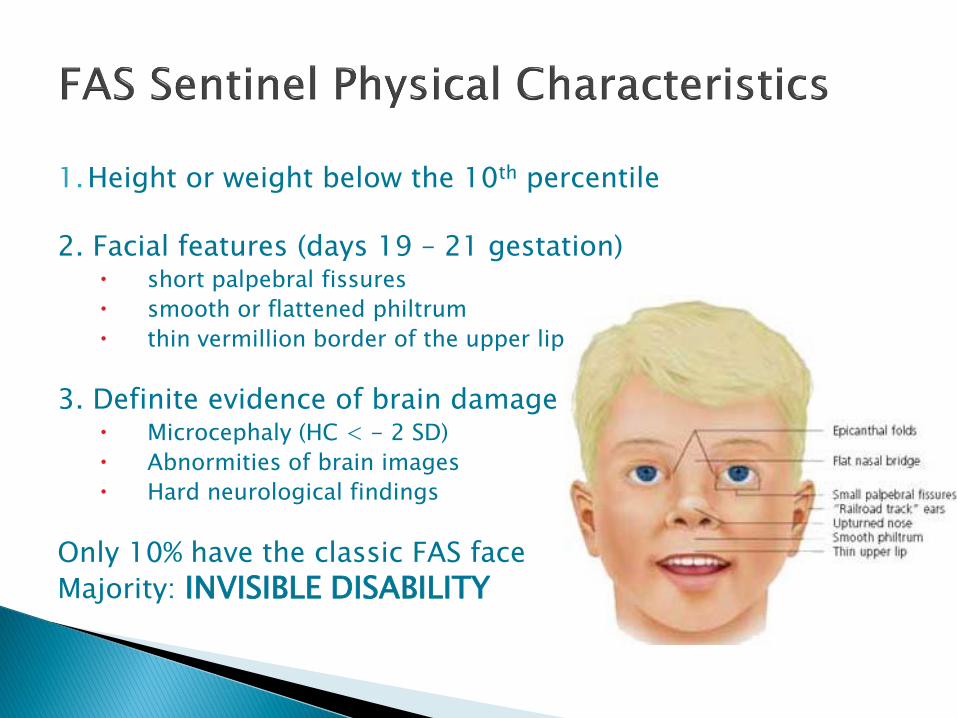
1.Height or weight below the 10th percentile 2. Facial features (days 19 – 21 gestation)
short palpebral fissures
smooth or flattened philtrum
thin vermillion border of the upper lip
3. Definite evidence of brain damage Microcephaly (HC < - 2 SD)
Abnormities of brain images
Hard neurological findings
Only 10% have the classic FAS face
Majority: INVISIBLE DISABILITY
http://www.faslink.org
• Human Research U of A, NeuroDevNet (KBH)
• Brain differences: neuroimaging studies (slide)
• Brain dysfunction: measuring brain impairments (Rasmussen)
• Biomarkers: meconium testing, eye movements (ethics)
• Interventions: caregiver training, environment supports, specific
programs (Pei)
• Compounding factors routed in SDOH: postnatal trauma,
neglect, abuse, exposure to domestic violence, multiple moves
with lack of attachment in foster care system
• Prevention opportunities: pilot projects PCAP, CATCH
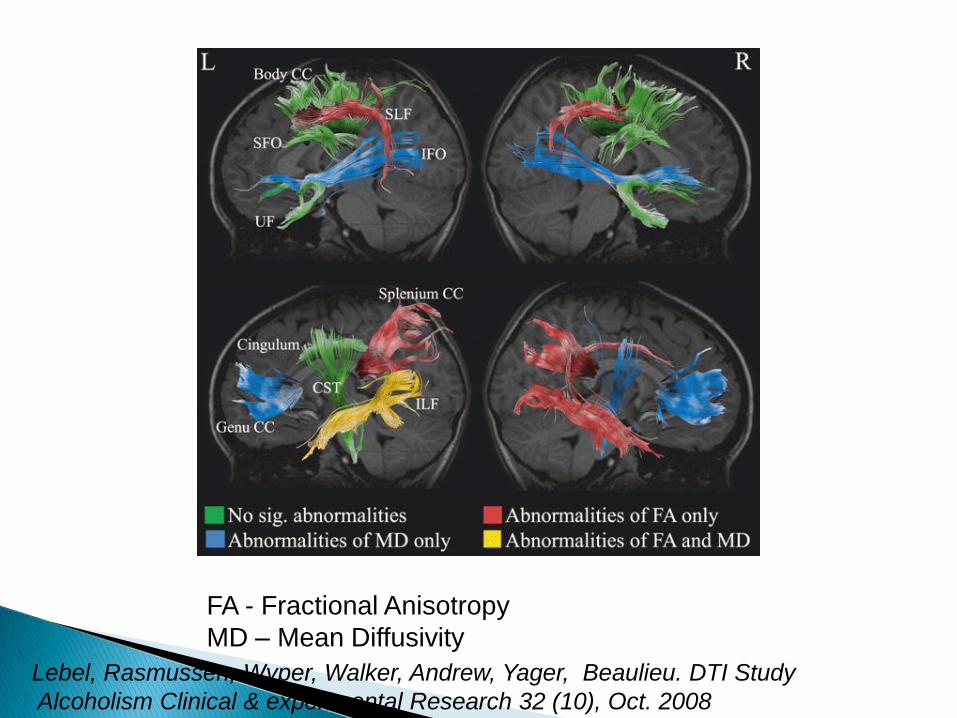
Lebel, Rasmussen, Wyper, Walker, Andrew, Yager, Beaulieu. DTI Study
Alcoholism Clinical & experimental Research 32 (10), Oct. 2008
FA - Fractional Anisotropy
MD – Mean Diffusivity
• Screening tools: under research (NBST, Assante corrections)
• Clinical history: struggling in learning (math, reading
comprehension) and adaptive function, mental health (>60 %
have ADHD)
• Suspicion or confirmation of PAE: how much is too much?
• Confirming PAE: working with birth mothers in how to ask the
question, nonjudgmental and supportive with PCAP program,
information from records, reliable reports, problem in adult diagnosis,
adoptions and foster care
• Diagnostic capacity: multidisciplinary team; 12 FASD service networks
in Alberta, CMC Alberta government commitment ( slide)
• Growth deficiency noted but not part of diagnosis
• Facial analysis by visual or computer analysis of digital photographs
• See visuals
• < 10 % have any facial features = invisible disability
• Brain assessment of 10 brain domains by multidisciplinary team (Pediatrician, Psychologist, SLP,OT, Social Worker) trained on FASD and differential diagnosis of developmental disability and mental health
• Indirect team members: mentors, case workers, teachers, mental health professionals
• Cost: $4000 per case
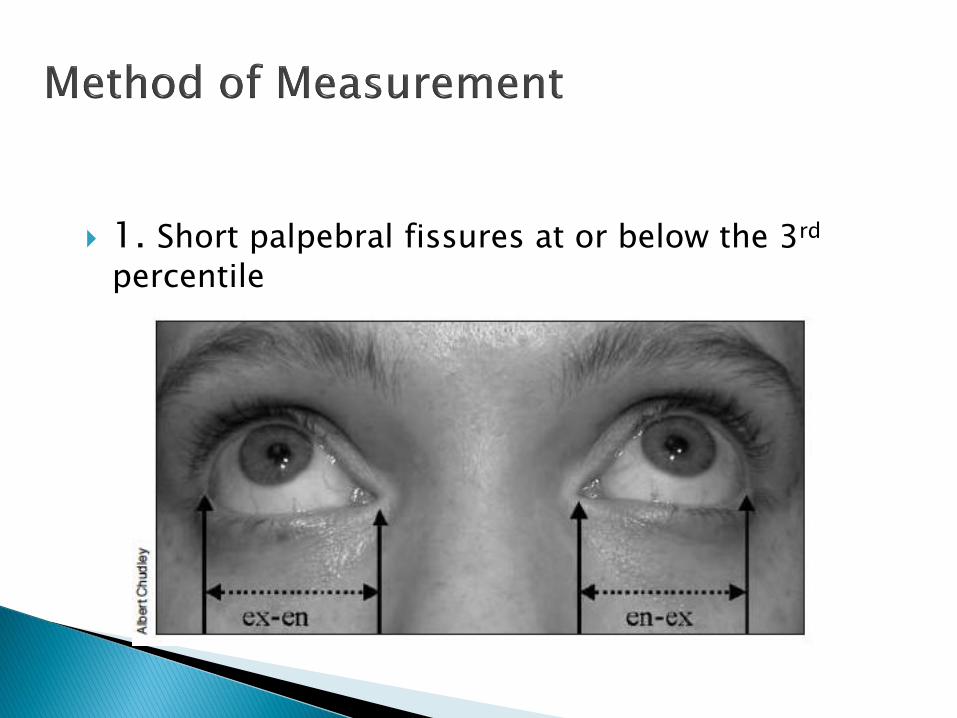
1. Short palpebral fissures at or below the 3rd
percentile
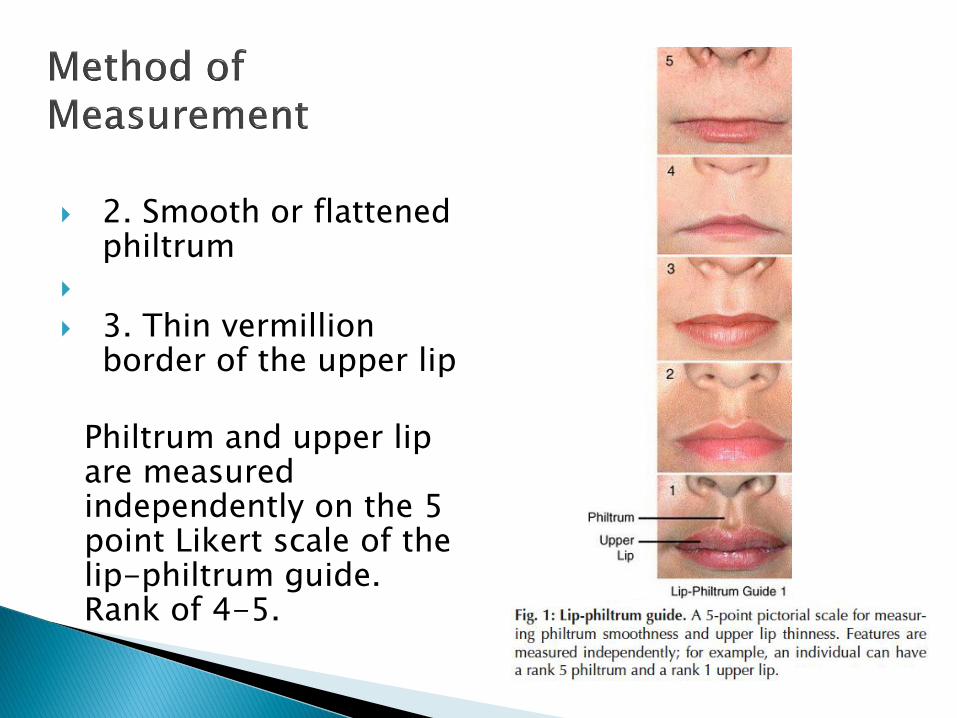
2. Smooth or flattened philtrum
3. Thin vermillion border of the upper lip
Philtrum and upper lip
are measured independently on the 5 point Likert scale of the lip-philtrum guide. Rank of 4-5.
• Core deficit: impaired adaptive functioning skills for day to
day living impacts independence at all ages and in adult
transitions to employment, housing, safety, quality of life
• Secondary disabilities or Primary from PAE?
• Mental health: Anxiety 15%, Depression 10% up to 50%
in adults, Attachment disorder 15%, PTSD 12%, ADHD
>60%
• School dropout
• Justice system involvement
• Than and Jonsson IHE AB 2015: life time cost per person $1.8
million, not capturing loss of productivity and caregiver stress
• Cost to prevent 1 case of FASD using PCAP model $742,000
• Butler 2014: total cost $9.7 billion per year in Canada with
• Justice 40%
• Health 21%
• Education 17 %
• Social services 13%
• Other 9%
• Newborn and infancy:
• Document PAE and monitor for NAS and ARBD
• Caregiving situation: child welfare or PCAP for birth mother
• Monitor development, optimize environment, caregiver
education, prevent postnatal trauma
• Toddler and preschooler:
• Possible delays in development: speech, quality of play
• Dysregulated: busy, easily over stimulated, impulsive,
safety, sleep issues
• Not specific for FASD diagnosis
• Connect to EIP, caregiver education re environment
• Kindergarten ages 5 to 6 presentation
• Behavior regulation difficulties: ADHD pattern, appear
oppositional but not understanding, cannot do transitions
• Language delays: not understanding
• Poor social skills: immature play, not getting social cues
• May not qualify for PUF funding but need teacher training
to create right environment
• Kindergarten ages 5 to 6 intervention
• Caregiver training, stable placements
• Education supports
• Targeted medications for ADHD
• Mental health if attachment and trauma issues
• Grades 3 to 5; ages 8 to 10 prime diagnosis age group
• Not keeping up academically: math, reading
comprehension, language demands of learning
• ADHD pattern, often mislabeled OCD
• Immature socially, poor perspective taking, being bullied
• Cannot organize without help, need constant reminders
• More problems in unstructured times of recess/recreation
• Not learning from consequences
• Unable to generalize information
• Poor regulation, cannot self calm
• Grades 3 to 5 ages 8 to 10 interventions
• Consistent strategies across all settings
• Stability of placement, support caregivers with respite
• School supports to address areas of struggle: modified
math, help with reading comprehension and technology for
written output
• Social skills and self regulation training but recognizing the
communication deficits in FASD
• Targeted medications for ADHD
• Adolescence presentations • Not keeping up academically: school avoidance • Impulsive behavior: school expulsion • ADHD pattern; often mislabeled ODD • Immature socially: risk of gravitating to wrong crowd and
victimization or isolation (on line social network increasing exploitation risk)
• Gap increasing: age expectations versus ability to function independently
• Emerging mental health with anxiety, depression, low self esteem, self harm, substance use, pregnancy risk, STD
• Adolescence interventions lacking! • Trouble with the law: set up, not understanding • Lack of training in the youth justice system • PCHAD caregiver rights vs youth • May lack advocate if a youth in foster care in group home • Need “WRAP” around team: PHCP, MH, School,
caregiver • Irony: youth not wanting/trusting supports • Transition planning: guardianship but who leads this if
youth is living in a group home?
• Adult presentations
• Presenting symptoms: mental health issues, in trouble with
the law, homelessness, no skills or cannot hold
employment, substance abuse, partner violence
• Difficulty in connecting to prenatal exposure to alcohol as
primary cause
• Adult FASD diagnosis: retrospective history, provide
mentor to the individual through the assessment process
and to connect to supports and services
• Adults with FASD interventions
• Interventions across many systems: PDD/AISH, housing,
supported employment, FASD informed mental health,
addictions and legal services.
• Why does FASD come in contact with the LAW?
• Need for system navigation: cliffs and gaps
• Parenting with FASD: Step by Step
• Physical health issues of aging with FASD
• Caregiver education on FASD: Coaching Families, FASD
networks, internet-based “Strongest Families FASD.com”,
Strategies not Solutions
• Understanding your child’s needs and strengths
• Set up the home and community environment
• Consistency, structure, predictability, avoid over stimulating
experiences, repetition, reminders, reward the positive
behaviors, demonstrate what is expected when dealing with a
negative behavior, reduce your language of explanation, more
visual cues
• Connect to social skills groups that are FASD informed
• Use visuals and play based rather than cognitive behavioral talk
therapy approach in mental health sessions
• Educational System
• Training on FASD in university Bed ore curriculum
• Modifications in classes: IPP in inclusive learning ,
Strategies or Opportunity programs, transition to life skills
and employability options in high school, post secondary
modifications
• “Professionals with Parachutes” training
• MILE and ALERT programs
• WRAP program: in school mentor and trainer
• No education=no job=no money=risk of contact with the
law and cycle of recidivism
• Judicial System
• Training on FASD at all levels from the cop to judge
• Consider brain impairment in FASD at all stages from
arrest to sentencing to probation
• Preventing entry into the justice system
• Recidivism prevention
• NCR debate
• Sleep disorders very common: sleep hygiene, routines,
sensory avoidance, no screen time, look for iron deficiency and
breathing difficulties, role of stress and bullying, Melatonin
• Mental health comorbidities: ADHD, Anxiety, depression,
aggression but look at environment first, start low go slow, side
effects versus benefit, long term side effects as adults in very
young children
• Nonmedical interventions: attachment and trauma therapy
that is FASD informed and culturally sensitive, cognitive
behavioral therapy
• Prevention: at all levels, cost driven $9.7 billion per year in
Canada (2014), but cannot measure human costs
• Need to address SDOH
• Prevention conversation social responsibility of all
• Improve access to diagnosis at younger ages and less cost
• Develop accurate biomarkers for PAE
• FASD informed education, addictions, mental health
systems and legal process systems
• Improved access and navigation to services and supports
for FASD: Kids Brain Health grants

FASD
Opportunities To Break The Cycle
FASD References
Overview:
Hanlon-Dearman A, Green C, Andrew G, LeBlanc N, Cook J: Anticipatory Guidance for Children and Adolescents with FASD: Practice Points for Primary Health care Providers. J Popul Ther Clin Pharmacol 22 (1): e27-e56 (2015)
Wilhoit L, Scott D, Simecaka B: FASD: Characteristics, Complications and Treatment. Community Mental Health J 53: 711-718 (2017)
Caputo C, Wood E, Jabbour L. Impact of fetal alcohol exposure on body systems: a systematic review. Birth Defects Research108: 174-180. (2016)
FASD References
Diagnosis:
Cook J et al: FASD: A guideline for diagnosis across the lifespan (Canadian Guidelines update 2015. CMAJ 2015 DOI: 10.1503/cmaj. 141593
McLachlan K, Andrew G, Pei J, Rasmussen C. Assessing FASD in Young Children: Exploring Clinical Complexities and Diagnostic Challenges. J Popul Ther Clin Pharmacol 22 (1) e108-e124; 2015
Kable J, Mukherjee R. Neurodevelopmental Disorder associated with prenatal exposure to alcohol (ND-PAE): A proposed diagnostic method of capturing the neurocognitive phenotype of FASD. European Journal of Medical Genetics 60; 49-54 (2017)
Kable J, O’Connor M, Carmichael- Olson H, Paley B, Mattson S, Anderson S, Riley E. Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure (ND-PAE): Proposed DSM-5 Diagnosis. Child Psychiatry Hum Dev 47: 335-346 (2016)
FASD References
Diagnosis: Flannigan K, Pei, J, Andrew G, Rajani H, McFarlane A,
O’Riordan T, Symes B, Rasmussen C. Deferred Diagnosis in children assessed for FASD. Applied Neuropsychology:Child https://doi.org/10.1080/2122965.2018.1427094
Goh P, Doyle L, Glass L, Jones K, Riley E, Coles C, Hoyme E, Kable J, May P, Kalberg W, Sowell E, Wozniak J, Matttson S. (CIFAS group from NIAAA)
A Decision Tree to Identify Children affected by Prenatal Alcohol Exposure. The Journal of Pediatrics 177: 121-127 (2016)
Bakhireva L et al. Challenges of diagnosing FASD in foster and adopted children. Alcohol 67: 37-43 (2018)
FASD References
Assessment Domains:
Enns L, Taylor N. Factors predictive of FASD: Neuropsychological assessment. Child Neuropsychology 24:203-225. (2018)
Bakhireva L, Garrison L, Shresta S, Sharkis J, Miranda R, Rogers K: Challenges of diagnosing FASD in foster and adopted children. Alcohol 67: 37-43 (2018)
Singer A, Aylsworth A, Coredero C, et al Daniels J. Prenatal Alcohol Exposure in relation to Autism Spectrum Disorder: Findings for the Study to Explore Early Development (SEED)
FASD References
Epigenetic Mechanisms:
Lussier A, Weinberg J, Kobor M. Epigenetic studies of FASD: Where are we now? Epigenemonics 9 (3) 291-311 (2017)
Varadinova M, Boyadjieva N. Epigenetic mechanisms: A possible link between autism spectrum disorders and FASD. Pharnacohol Research 102: 71-80 (2015)
FASD References
Interventions:
Pei J, Baugh L, Andrew G, Rasmussen C. Intervention recommendations and subsequent access to services following clinical assessment for FASD. Research in Developmental Disabilities 60: 176-186 (2017)
Petrenko C, Alto M. Interventions in FASD: An international perspective. Eurpoean Journal of Medical Genetics 60: 79-91 (2017)
Strongest Families Institute: Parenting strategies on line: www.strongestfamilies.com also see evaluation: Hundert A et al . Usability testing of guided internet based parent training for challenging behavior in children with FASD. J Popul Ther Clin Pharmacol 23 (1) e60-e76 (2016)
FASD References
Caregiver Needs:
Bobbitt S, Baugh L, Andrew G, Cool J, Green C, Pei J, Rasmussen C. Caregiver needs and stress in caring for individuals with FASD. Research in Developmental Disabilities 55: 100-113. (2016)
Medications:
Goril S, Zalai D, Scot L, Shapiro C. Sleep and melatonin secretion abnormalities in children and adolescents with FASD. Sleep Medicine 23: 59-64 (2016)
FASD References
Biomarkers:
Bager H, Christensen L, Husby S, Bjerregaard L. Biomarkers for Prenatal Alcohol Exposure: A Review. Alcoholism Clinical and Experimental Research 41: 251-261 (2017)
Prevalence:
Lange S, Probst C, Gemel G, Rehm J, Burd L, Popova S. Global prevalence of FASD among children and youth. A systematic review and meta-analysis. JAMA Pediatr. Doi:10.1001/jamapediatrics e1-e9 (2017)
Strongestfamilies.com provides families with strategies on behavioral management strategies and uses a coaching model
Albert resources: Strategies not Solutions: booklet that gives practical ideas for caregivers and was produced by expert consultation in the Edmonton and across Alberta: access and download at www/region6fasd.ca as a pdf or www.child.alberta.ca/ to order copies





























