Embed Size (px)
Citation preview

Brit. J. Ophthal. (I 975) 59, i66
Filarial worm (Loa loa) in the anterior chamberReport of two cases
OLABOPO OSUNTOKUN AND OYIN OLURINDepartment qf Ophthalmology, University College Hospital, Ibadan, Nigeria
The adult Loa loa filarial worm wanders in the sub-cutaneous tissues of man and it is not uncommon forit to wander into the periorbital tissues and eyelidsand often into the subconjunctival tissues where it canbe seen moving rapidly across the conjunctival sac.It is because of such appearances in the conjunctivalsac that it is often referred to as "the African eyeworm". In such an environment Loa loa worms,though a nuisance, do not normally adversely affectvision.Few cases of intraocular parasitism by the adult
filarial worm have been reported in the literature(Wright, 1934; Nayar and Pillai, 1932; Chatterji,1954; Mishra, 1958; Rose, I966) and such reportsdocument adult filaria (Wuchereria bancrofti) in eitherthe vitreous or anterior chamber. This communicationreports Loa loa filarial worms in the anterior chamberin two patients. We are not aware of any previousreport of the Loa loa filarial worm in the anteriorchamber in man.
Case I, a 22-year-old Nigerian woman, came to theOphthalmology Clinic of University College Hospital,Ibadan, with a 6-months' history of pain, itching, and asensation of "a worm eating away her right eye".
ExaminationThere was no perception of light in the right eye, but theeye was white and the cornea was translucent with discreteopacities. A live and active thread-like worm was seen in theanteior chamber. The light seemed to excite it and itsmovements became more vigorous, coiling and uncoilingand thrashing about. The anterior chamber appeared tobe lined by a fibrous membrane which completely oc-cluded the pupil.Examination of peripheral blood samples for Microfilaria
was negative. The total white cell count was 12,420/CU.mm. with eosinophilia 26 per cent., neutrophils 50 percent., lymphocytes 22 per cent., and monocytes 2 per cent.Examination of a skin snip for Microfilaria was alsonegative. A general physical examination showed no ab-normality. There was no lymphadenopathy. There wereno palpable subcutaneous nodules. The chest and heartwere normal and there was no hepatosplenomegaly.
Address for reprints: Olabopo Osuntokun, D.O., F.M.C.S. (Nig.),Department of Ophthalmology, University College Hospital, Ibadan,Nigeria.
TreatmentSince the eye was blind and appeared to be causing dis-comfort, it was excised under local anaesthesia and fixedin formol saline.
Pathological reportMacroscopical examination showed partial collapse of theanterior chamber, a hazy cornea, and total retinal detach-ment with subretinal gelatinous exudate. There was aworm in the anterior chamber which had the features of amale Loa loa.
Microscopical examination showed some vascularizationof the peripheral cornea. The back of the cornea and theanterior surface of the iris and lens were lined by a fibrousmembrane which occluded the chamber angle. The irisand ciliary body were oedematous, and the lens showedanterior subcapsular fibrosis. The retina was totallydetached, disorganized, and degenerate, and showedneovascularization into the vitreous on one side. The sub-retinal space contained haemorrhagic albuminous exudate.
Case 2, a 15-year-old Nigerian schoolgirl, was referredto the Ophthalmology Clinic because of pain and feelingsof worm movements in her right eye for 5 months, andblindness in the same eye for i month. She had receivedtreatment with diethycarbamazine (banocide) and piritonfor some days before she came to the hospital.
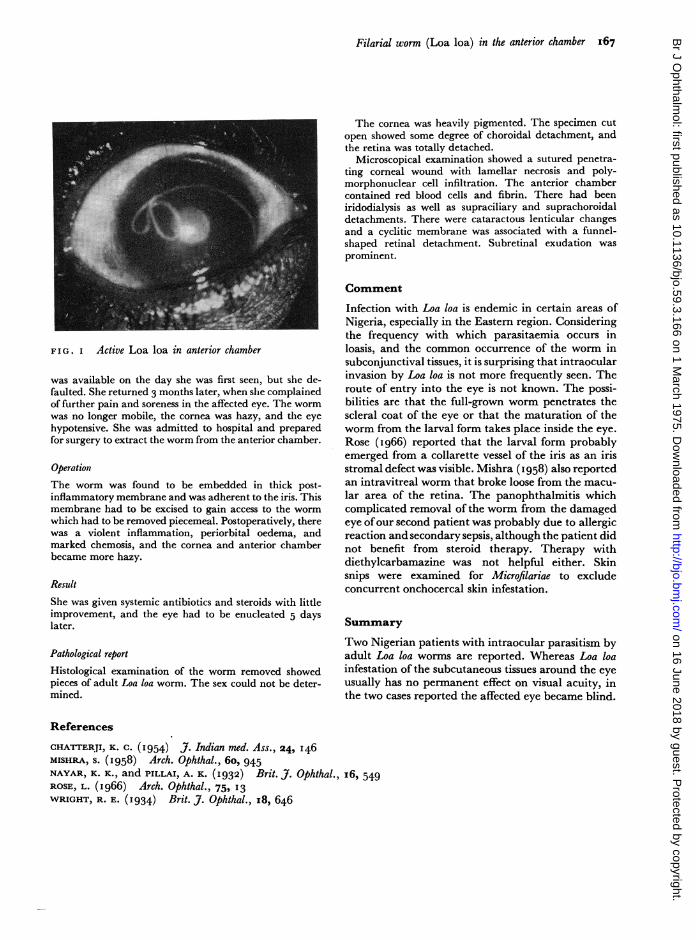
ExaminationThere was no perception of light in the right eye and thevisual acuity in the normal left eye was 6/4. TIhe right eyeshowed slight conjunctival injection; the cornea was clear,and, there was a very active worm in the anterior chamber(Figure). Minimal flare and cells were present in theanterior chamber. The lens was opaque.
Laboratorv investigationsThese included microscopical examination of thick andthin blood films. Skin snips showed no Microfilariae. Thetotal white blood cell count showed I4 per cent. eosino-philia.
Treatment and progressThe patient was asked to report a week later for extractionof the worm from the anterior chamber, because no bed
on 16 June 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.3.166 on 1 March 1975. D
ownloaded from
Filarial worm (Loa loa) in the anterior chamber 167
FIG. I Active Loa loa in anterior chamber
was available on the day she was first seen, but she de-faulted. She returned 3 months later, when she complainedof further pain and soreness in the affected eye. The wormwas no longer mobile, the cornea was hazy, and the eyehypotensive. She was admitted to hospital and preparedfor surgery to extract the worm from the anterior chamber.
OperationThe worm was found to be embedded in thick post-inflammatory membrane and was adherent to the iris. Thismembrane had to be excised to gain access to the wormwhich had to be removed piecemeal. Postoperatively, therewas a violent inflammation, periorbital oedema, andmarked chemosis, and the cornea and anterior chamberbecame more hazy.
ResultShe was given systemic antibiotics and steroids with littleimprovement, and the eye had to be enucleated 5 dayslater.
Pathological reportHistological examination of the worm removed showedpieces of adult Loa loa worm. The sex could not be deter-mined.
The cornea was heavily pigmented. The specimen cutopen showed some degree of choroidal detachment, andthe retina was totally detached.
Microscopical examination showed a sutured penetra-ting corneal wound with lamellar necrosis and poly-morphonuclear cell infiltration. The anterior chambercontained red blood cells and fibrin. There had beeniridodialysis as well as supraciliary and suprachoroidaldetachments. There were cataractous lenticular changesand a cyclitic membrane was associated with a funnel-shaped retinal detachment. Subretinal exudation wasprominent.
Comment
Infection with Loa loa is endemic in certain areas ofNigeria, especially in the Eastern region. Consideringthe frequency with which parasitaemia occurs inloasis, and the common occurrence of the worm insubconjunctival tissues, it is surprising that intraocularinvasion by Loa loa is not more frequently seen. Theroute of entry into the eye is not known. The possi-bilities are that the full-grown worm penetrates thescleral coat of the eye or that the maturation of theworm from the larval form takes place inside the eye.Rose (I966) reported that the larval form probablyemerged from a collarette vessel of the iris as an irisstromal defect was visible. Mishra (1958) also reportedan intravitreal worm that broke loose from the macu-lar area of the retina. The panophthalmitis whichcomplicated removal of the worm from the damagedeye ofour second patient was probably due to allergicreaction and secondary sepsis, although the patient didnot benefit from steroid therapy. Therapy withdiethylcarbamazine was not helpful either. Skinsnips were examined for Microfilariae to excludeconcurrent onchocercal skin infestation.
Summary
Two Nigerian patients with intraocular parasitism byadult Loa loa worms are reported. Whereas Loa loainfestation of the subcutaneous tissues around the eyeusually has no permanent effect on visual acuity, inthe two cases reported the affected eye became blind.
References
CHATTERJI, K. C. (I954) J. Indian med. Ass., 24, I46MISHRA, S. (I 958) Arch. Ophthal., 6o, 945NAYAR, K. K., and PILLAI, A. K. (1932) Brit. J. Ophthal., I6, 549ROSE, L. (I966) Arch. Ophthal., 75, 13WRIGHT, R. E. (I934) Brit. J. Ophthal., I8, 646
on 16 June 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.3.166 on 1 March 1975. D
ownloaded from