Upload
robertbabu
View
219
Download
0
Embed Size (px)
Citation preview
8/10/2019 Final Copy End Term Evaluation Report
1/45
THE ROTARY CLUB OF KITGUM
END TERM EVALUATION REPORT
MOTHER AND CHILD HEALTH project-MCH-p
BY FRANCIS ODWONG AND ROBERT BABU
7/22/2014
An end-term/terminal evaluation report for a mother and child health project implemented by the Rotary
Club of Kitgum in hard to reach rural locations within the district. The project lasted for sixteen months (April
2013-June 2014. The evaluation was meant to demonstrate the successes, challenges, best practices and
lessons learnt in the project implementation for future programming by the club and its stakeholders as well
as to offer accountability on the performance of the club in this project.
8/10/2019 Final Copy End Term Evaluation Report
2/45
END TERM EVALUATION REPORT
July 22, 2014
2
1)
AcknowledgementNen Anyim Skyline Uganda acknowledges all those who participated in the end term evaluation exercise in Lamit
Pajong, Akuromo and Okuti parishes in Kitgum district for offering their time for the activity. We also acknowledge the
leadership of the Rotary Club of Kitgum and the technical staff who worked in the Mother and Child Health project fo
the cooperation and support rendered to the evaluation team during the exercise. We highly appreciate the projectsdonor representative for her invaluable contribution to the evaluation exercise.
Our heartfelt appreciation also goes to the field data collection team including Atimango Vicky, Komakech Moses, Ochan
Francis, and Ogwal Tom Peter for their dedication in the exercise.
This Evaluation would not have happened without the technical and financial assistance from Mount Airy Rotary
Foundation through the Rotary Club of Kitgum. Your continued support to relief world suffering including in Northern
Uganda is highly acknowledged.
8/10/2019 Final Copy End Term Evaluation Report
3/45
END TERM EVALUATION REPORT
July 22, 2014
3
2)Executive summarya)
Background:
The Rotary Club of Kitgum with part funding from Mount Airy Rotary Club implemented a Mother and Child Health
project in Akwang, Mucwini and Orom Sub Counties in Kitgum districts from April 2013 to June 2014. In order to
maximize the work of the project with the target communities, the Club in June 2014 contracted Nen Anyim Skyline Co
Limited (a development consultancy company) to undertake an end term evaluation to document successes, challenges
lessons learnt and best practices registered by the project.
b)
Purpose:
To establish objective information on the successes and lessons learnt among others by Rotary Club Kitgum in the
implementation of this project. The information shall be used to determine the efficiency and effectiveness of the
strategies used by Rotary Club Kitgum in planning and implementation of the project for replication, improved
programming, accountability and reference.
c)
Objectives:
To report on the level of achievement of the project objectives according to the expected results listed in the logica
framework. To highlight lessons learnt, best practices, and challenges faced during the implementation of the Mothe
and Child Health project.
d)
Methodology:
The evaluation applied the survey (cross-sectional) study design using both quantitative and qualitative data collection
and analysis techniques. Data were collected through beneficiary interviews, Focus Group Discussions (FGDs), Key
Informant Interviews (KIIs), review of the projects statistics and official health recordsplus other relevant documents. A
sum of 3 FGDs, 15 KIIs and 76 beneficiary interviews were conducted.
e) Key findings, conclusion and recommendations:
Most of the end of project output targets on Mother and Child Health were attained. However there were serious
shortfalls in the performance for some important targets. The Maternal and Child Health project greatly contributed to
the improvement of maternal and child health through increased ANC attendance, vaccination, family planning and
deliveries at the health facilities. The mothers have been empowered in better hygiene practices and seek timely healt
care for themselves and their children.
The project performed satisfactorily on the targets it set prior to the intervention. Some of the achievements registered
in the project far exceeded the targets such as awareness on family planning, change in the health seeking behaviors o
women, and use of the referral system for women at risk and in emergency. A couple of other targets were
unfortunately not attained especially the one on vaccination for DPT3 and measles.
The project also applied a lot of innovation and creativity in its approach by engaging key stakeholders and
partners which ensured synergy, efficiency and effectiveness.
8/10/2019 Final Copy End Term Evaluation Report
4/45
END TERM EVALUATION REPORT
July 22, 2014
4
TABLE OF CONTENT
1) Acknowledgement ..............................................................................................................................................2
2) Executive summary .............................................................................................................................................3
3) Acronyms ...........................................................................................................................................................6
1. CHAPTER I ..........................................................................................................................................................7
1.1 Background ....................................................................................................................................................7
1.2 The project background .......................................................................................................................................... 7
1.3 Project Objectives ................................................................................................................................................... 7
1.4 Project Activities ..................................................................................................................................................... 8
1.5 Objectives of the Evaluation ............................................................................................................................9
1.6 Scope of work .................................................................................................................................................9
1.6.1 Project Design ..................................................................................................................................................... 9
1.6.2 Project Implementation ...................................................................................................................................... 9
1.6.3 Project Performance and Impacts .................................................................................................................... 10
1.6.4 Conclusions and Recommendations for Future Activities ................................................................................ 10
2. Chapter II: Methodology ................................................................................................................................... 11
2.1 Study Design .......................................................................................................................................................... 11
2.2 Study area and Population: ................................................................................................................................... 11
2.3 Sample Size ........................................................................................................................................................... 11
2.4 Data Collection Methods ...................................................................................................................................... 11
2.5 WCA Interviews ..................................................................................................................................................... 12
2.6 Focus Group Discussions (FGDs) ....................................................................................................................... 12
2.7 Key Informant Interviews (KII) .......................................................................................................................... 12
2.8 Data Management, Analysis and report writing ................................................................................................... 12
2.9 Quality control ...................................................................................................................................................... 12
2.10 Ethical considerations ........................................................................................................................................... 13
3. CHAPTER III ...................................................................................................................................................... 14
3.1 FINDINGS AND ANALYSIS .............................................................................................................................. 14
3.2 Demographic information ..................................................................................................................................... 14
3.3 THE PROJECT DESIGN ............................................................................................................................................ 14
3.4 IMPLEMENTATION ................................................................................................................................................ 15
8/10/2019 Final Copy End Term Evaluation Report
5/45
END TERM EVALUATION REPORT
July 22, 2014
5
3.5 RELATIONSHIP WITH STAKEHOLDERS ............................................................................................................... 18
3.6 Challenges faced during the project implementation ...................................................................................... 21
3.7 PROJECT PERFORMANCE AND IMPACTS .............................................................................................................. 22
3.7.2 State of the local referral system .................................................................................................................. 24
3.8 The level of sustainability/self-reliance achieved by the project ......................................................................... 28
4. CHAPTER IV ...................................................................................................................................................... 30
4.1 CONCLUSION AND RECOMMENDATIONS ............................................................................................................. 30
4.2 Performance on targets .................................................................................................................................... 30
4.2.4 The project design ......................................................................................................................................... 31
4.2.5 The project implementation ......................................................................................................................... 31
4.2.8 Project performance and impact .................................................................................................................. 32
4.3 RECOMMENDATIONS, INSIGHTS AND LESSONS LEARNT...................................................................................... 34
APPENDICES ............................................................................................................................................................ 36
ANNEX I ............................................................................................................................................................................. 36
ANNEX II ............................................................................................................................................................................ 37
ANNEX III ........................................................................................................................................................................... 39
ANNEX IV ........................................................................................................................................................................... 43
8/10/2019 Final Copy End Term Evaluation Report
6/45
END TERM EVALUATION REPORT
July 22, 2014
6
3)AcronymsS/NO ACRONYMS IN-FULL
1.
AIDS Acquired Immune Deficiency Syndrome
2.
ANC Ante Natal Care
3.
ARTI Acute Respiratory Tract Infection4.
CAO Chief Administrative Officer
5.
DHO District Health Officer
6.
DSC District Services Commission
7.
FGD Focus Group Discussion
8.
HC Health Centre
9.
HIV Human Immune Virus
10.
KDLG Kitgum District Local Government
11.
KII Key Informant Interview
12.
LC Local Council
13.
LQAS Lot Quality Assurance Sampling
14.
MC Management Committee15.
MCH Mother and Child Health
16.
MDG Millennium Development Goal
17.
M&E Monitoring and Evaluation
18.
NGOs Non-Governmental Organizations
19.
NMS National Medical Stores
20.
PC Project Coordinator
21.
PHC Primary Health Care
22.
PMTCT Prevention of Mother to Child Transmission
23.
RC Rotary Club
24.
RCK Rotary Club of Kitgum
25.
RDT Rapid Diagnostic Test26.
TBA Traditional Birth Attendants
27.
VHT Village Health Team
28.
WASH Water, Sanitation and Hygiene
29.
WCA Women of Child Bearing Age
30.
WHO World Health Organization
8/10/2019 Final Copy End Term Evaluation Report
7/45
END TERM EVALUATION REPORT
July 22, 2014
7
1.
CHAPTER I
1.1
Background
1.2
The project backgroundSimon Lawoko, Foundation Chair of Kitgum Rotary, emailed M. Goldwasser from Rotary Club Mount Airy
about having a project focused on saving lives of mothers and children in March 2011. Nurse Practitioner
Rudolf Schachner, long experienced in working in Africa, was consulted on the best way to do this. In May
2011, the Kitgum President Sunday Abwola and project coordinator Simon Lawoko contacted and set up
meetings with the District Health Officer and District Education Officer. Several talks with the District
health Officer (DHO), representatives of health centers, an experienced local midwife, as well as members
of the Village Health Teams (VHTs) and Traditional Birth Assistants (TBAs) took place. The group approved
the project idea and assured cooperation. Kitgum Rotary Officers and the DHO determined where to begin
the project, then took the idea to the Kitgum Rotary Club for discussion and approval. The club selectedthis project from 5 project ideas. During meetings with Kitgum officers, the DHO and Health Unit
Management Committee agreed to attend seminars and oversee the Health Centers and VHT's. The DHO
offered to find an office in Kitgum for the team. Members of the assessment team submitted a plan of
action and budget for approval. In 2013 and 2014, Rotary Club Kitgum undertook the 15 months project in
Kitgum district with funds from Rotary Foundation.
1.3Project Objectives
1.3.1 The main objective of the project was to improve the health situation for mothers and children in
the rural areas of Kitgum district (Northern Uganda). The project would contribute to the
Millennium Development Goals 4 (Reducing Child Mortality Rates) and 5 (Improving materna
health). The Specific Objective of the project was to provide an increased access to Mother and
Child Health Care services to the local population in difficult to reach areas of Kitgum district by
mobile outreach.
The following three results were to be achieved:
1.3.1.1Establishment of a mobile outreach system for MCH-services in eight villages in the rural areas of
Kitgum.
1.3.1.2
Pregnant woman and mothers of young children practice hygiene and health prevention according
to WHO guidelines in eight villages in the rural districts of Kitgum.
1.3.1.3Local decision makers are aware and support the regular MCH services by the mobile Outreach
team. They will contribute to the sustainability and long term running of the ambulance.
1.3.1.4
The following indicators would be used to assess the achievement of the above mentioned
objective and results:
1.3.2 Indicators for project objective
8/10/2019 Final Copy End Term Evaluation Report
8/45
END TERM EVALUATION REPORT
July 22, 2014
8
1.3.2.150 percent of all deliveries are attended by a skilled midwife in Kitgum district by the end of April
2014.
1.3.2.265 percent of women will have at least three ANC visits by the mobile outreach team in the rura
areas of Kitgum district by the end of April 2014.
1.3.2.3
The local population is aware of the possibility of a referral system for woman at risk and
emergencies in the rural areas of Kitgum district till the end of April 2014.
1.3.3 Indicators for result No. 1
1.3.3.1Eight pre-selected villages in the rural districts of Kitgum are visited twice per month by the mobile
outreach team till the end of April 2014.
1.3.3.2Monthly numbers of daily medical consultations of pregnant women in the rural areas of Kitgum
district till the end of April 2014.
1.3.3.3
85 percent of children have a DPT3 and measles vaccination in the rural areas of Kitgum district by
the end of April 2014.
1.3.3.430 percent of all women at a child bearing age are aware about methods of family planning.
1.3.4 Indicators for result No. 2
1.3.4.1Number of education units for mothers in the rural areas of Kitgum district until the end of April
2014 performed by VHT's.
1.3.4.2 Five VHTs per parish receive a training of at least six days until the end of April 2014.
1.3.4.3
Women in the rural districts of Kitgum are aware of the basics of hygienically disease prevention.
1.3.5 Indicators for result No. 3
1.3.5.1
Running costs of the ambulance are budgeted by the DHO for the financial year 2014/2015.
1.3.5.2At least four radio broadcasts will be held in local radio station to inform about the health services
the MCH-Team is providing in the rural areas of Kitgum district.
1.3.5.3Number of participatory meetings with at least 20 participants.
1.4
Project Activities1.4.1 A mobile clinic consisting of 1 midwife, 2 nursing assistants, 1 double comprehensive nurse and 1
driver offers basic health and ANC services at rural areas by mobile outreach. In total 4 parishes
were selected and in total 8 spots were visited regularly per month.
1.4.2 Activities include:
1.4.3 Training of VHTs and TBAs to provide health education in family planning, nutrition, sanitation and
vaccination to reduce infections, malnutrition, high birth rates and disease.
8/10/2019 Final Copy End Term Evaluation Report
9/45
END TERM EVALUATION REPORT
July 22, 2014
9
1.4.4 Neonatal consultations to ensure detection of complications in pregnancy and necessary referrals
to functional health centers or hospitals.
1.4.5 Scheduled immunization, mosquito nets, counseling, retro-viral & anti-malarial drugs to reduce
illness and death, transmission of HIV-AIDS and low birth-weight infants
1.4.6
Capacity building and linkages with community based networks, upgrading and strengthening the
Health Center staff will mean better health care for women and children and sustainability of the
project.
1.5
Objectives of the Evaluation
1.5.1 Objective: To report on the level of achievement of the project objectives according to the results
listed in the logical framework.
1.5.2 The evaluation of the Project was done in order to generate objective information on the successes
and failures of Rotary Club Kitgum. The information will be used to determine the efficiency and
effectiveness of the strategies used by Rotary Club Kitgum for planning and implementation of the
current project, for the formulation of future project proposals and for the incorporation of Rotary
Club Kitgum's methodologies in other projects.
1.5.3
The recommendations of the evaluation report should further enable Rotary Foundation
International to assist Rotary Club Kitgum in improving its decision-making processes and technical
and financial management.
1.6
Scope of workThe evaluation addresses the following issues in the report:
1.6.1 Project Design
1.6.1.1Considers the effect of the project design on reducing maternal and child mortality.
1.6.1.2Considers how realistic the project objectives, as defined by the Logical Framework, were.
1.6.1.3Considers if the organizational framework was suitable for the implementation of the project and if
Rotary Club Kitgum had the right staff, budget, equipment and management capacity to achieve
the project objectives.
1.6.2
Project Implementation1.6.2.1
Comments on the implementation strategy, procedures and planning methods used by Rotary Club
Kitgum.
1.6.2.2Determines the efficiency of implementation by a comparison of the costs incurred and the results
achieved.
1.6.2.3Comments on the role and performance of RC Kitgum and local partners, the beneficiaries and
other stakeholders in the implementation of Rotary Club Kitgum.
8/10/2019 Final Copy End Term Evaluation Report
10/45
END TERM EVALUATION REPORT
July 22, 2014
10
1.6.2.4Assesses the technical and managerial potential and efficiency of Rotary Club Kitgum and other
stakeholders.
1.6.2.5Reports on how much external factors have influenced project implementation.
1.6.2.6Assesses the monitoring and reporting competence of Rotary Club Kitgum.
1.6.2.7
Assesses the technical and managerial competence of Rotary Club Kitgum technical staff and
Rotary Club Kitgum Steering committee and make recommendations on how these may be
improved.
1.6.3
Project Performance and Impacts
1.6.3.1Determines how far Rotary Club Kitgum has realised the objectives defined by the Logica
Framework and compare the project activities with the project documents.
1.6.3.2Determines the contribution of Rotary Club Kitgum towards the accessibility to health services for
women.
1.6.3.3
Reports on the attitude of local population to participate in the project.1.6.3.4Measures the knowledge level of women at child bearing age in hygiene and disease prevention.
1.6.3.5Examines the attitude towards family planning.
1.6.3.6Examines womens attitude towards ANC1 to ANC3 visits.
1.6.3.7Examines the attitude to give birth at Health Centre.
1.6.3.8Determines the capacity of VHTs and TBAs to perform health education.
1.6.3.9Assesses the willingness of the government to take over the project.
1.6.3.10 Assesses the level of sustainability/ self-reliance achieved by the project beneficiaries.
1.6.3.11 Reports on womens participation/ involvement in the design and the realization of the project.
1.6.3.12 Assesses the effectiveness of the training courses provided by RC Kitgum to VHTs.
1.6.4 Conclusions and Recommendations for Future Activities
1.6.4.1Summarise the consultants findings on the following issues:
1.6.4.2Policies, structure, management, staffing RC Kitgum.
1.6.4.3Objectives of RC Kitgum.
1.6.4.4Reporting, monitoring and oversight,
1.6.4.5Roles of the different stakeholders and relationships with the key actors, local administration
other NGOs and donors.
1.6.4.6The effects of external factors on the implementation of RC Kitgum.
8/10/2019 Final Copy End Term Evaluation Report
11/45
END TERM EVALUATION REPORT
July 22, 2014
11
2. Chapter II: Methodology
2.1
Study Design
The study employed the cross sectional design (survey) by applying a mix of selected qualitative and
quantitative techniques to obtain data on the process and impact of the project in selectedparishes/villages in Kitgum District. It also involved review of relevant project documents like the overal
project statistics and official statistics.
2.2
Study area and Population:
The study was conducted in the four parishes1where the project was implemented. The study population
included Women of Child Bearing Age (WCA) numbering some 2,436 women and girls, VHTs and TBAs
engaged in the project implementation. The study also interviewed various other stakeholders such as the
project staff, the project donor, the project consultant and members of the RCK management committee.
The women and girls mentioned above constituted the projects direct beneficiaries whereas the other
stakeholders provided the project with all kinds of support ranging from financial aid, oversight and
implementation.
2.3Sample Size
The LQAS sampling technique was applied to ensure that the minimum quality standards of the data
collected were met. A sample size of 83 Women/Girls of Child Bearing Age whereby each of four parishes
were set to provide at least 20 of these respondents. Given the study population size (2,436) a standard
sample size of 332 was arrived at on the basis of 95% confidence level and +/- 10% confidence interval
Since there was four study areas/parishes (referred to as lots according LQAS) the standard sample size
was divided by four to obtain the actual LQAS sample size of 83 respondents which was finally used. Onceat the study areas, the enumerators applied non-probability/purposive technique to identify suitable
respondents to realize the calculated sample size for WCA. Purposive sampling is not the best alternative
out there (due to non-existent/inadequate sampling frame) but it served the purpose well enough since
the respondents were fairly homogenous.
2.4
Data Collection Methods
Primary data were collected from the respondents by Field Research Assistants and the consultants using
specific sets of tools. FGD and Key Informant Interview guides were used for collecting qualitative data
Photo documentation and field observation of the implemented activities and changes in the behavior of
the target groups like use of WASH facilities2stemming from the projects intervention was applied.
The FGD guide was applied for qualitative data collection with VHTs and TBAs who were trained by the
project and participated actively in its implementation. A varied KII guide was used to collect qualitative
1Pajong-Mucwini, Lamit-Akwang, Okuti and Akurumo in Orom sub-county
2Latrines, rubbish pits and utensil drying stands etc.
8/10/2019 Final Copy End Term Evaluation Report
12/45
END TERM EVALUATION REPORT
July 22, 2014
12
data from various key informants of the project including the project staff, members of the Clubs
management committee, the project donor, government focal person and the project consultant.
2.5WCA Interviews
A questionnaire was used to collect quantitative/qualitative primary data from WCA by the field researchassistants/enumerators. This tool covered issues regarding the project design, implementation and
outcomes to which the respondents competently provided responses.
The research assistants were inducted on the questionnaire through brainstorming and role plays. The RAs
were also prompted to administer the tool among themselves to clarify any lingering inconsistencies.
2.6Focus Group Discussions (FGDs)
Focus Group Discussions (FGDs) were held with the Village Health Teams (VHTs) and Traditional Birth
Attendants (TBAs) in the projects target areas. The discussions focused mostly on the implementation of
the project including the roles of these health workers within the project. Three FGDs were conducted in
Lamit, Pajong and Akurumo with an average of eight (8) participants for each session. The FGDs were
conducted by the consultants themselves.
2.7Key Informant Interviews (KII)
KIIs were addressed to Clubs Management Committee, the project staff, the Local Government Foca
Person, and the respective sub-county leaders and health center personnel. This particular interview was
intended to collect data on the project design, implementation and impact from a vantage point of view of
the respective offices.
2.8
Data Management, Analysis and report writing
Data was entered directly into the computer using Epi data software. Data entry was done daily from
commencement of data collection. The entered data were then synchronized by the consultants for
analysis. After entry and cleaning, validated data were then exported to SPSS 21.0 and analysis done. Uni-
variate analysis of the data was applied to the data producing relevant descriptive statistics. The data were
disaggregated according to project activity, demographic characteristics and target areas to get specific
details on performance of the project. The Atlas software was used for the analysis of data from FGDs and
other qualitative data.
2.9
Quality controlThis was ensured right from the design of the data collection tools through to data collection, data coding,
analysis and interpretation. The consultants recruited and inducted qualified field data
collectors/enumerators. The Lot Quality Assurance Sampling LQAS that was used for the selection of
participants for the beneficiary interviews minimized bias and ensured a representative sample size of the
target population.
8/10/2019 Final Copy End Term Evaluation Report
13/45
END TERM EVALUATION REPORT
July 22, 2014
13
The study in the design of the relevant tools borrowed from the health industry scoring standards
including the WHO guidelines on hygienic practices.
The tools were reviewed by peers including MCH-Care practitioners from agencies working on the same to
ensure that they address the key issues in MCH-care. The tools were pre-tested for feasibility and re-designed where necessary to suit the circumstances identified.
The draft evaluation report was validated by all the relevant stakeholders and reviewed by peers before a
final copy was written.
2.10
Ethical considerations
Confidentiality was guaranteed by concealing the identity of the respondents such as not recording their
names on the tools. A cover letter was written and shared with respondents to seek their informed
consent to participate in the exercise before it commenced.
The evaluation team ensured sensitivity to local cultural and social issues which might have jeopardized
the exercise. For example young women and girls who participated in the exercise were talked to in open
places (outside the ear-shot of onlookers) to avoid antagonizing their male guardians.
The report was shared with stakeholders who participated in the exercise to reassure them that it was a
true reflection of the information they provided.
8/10/2019 Final Copy End Term Evaluation Report
14/45
END TERM EVALUATION REPORT
July 22, 2014
14
3.
CHAPTER III
3.1
FINDINGS AND ANALYSIS
3.2
Demographic informationMost of the WCA-respondents were within the age 20-29 years (43/57% respondents) and 30-39 years
(28/37% respondents). Only five respondents were teenage girls of child bearing age. Each of the four
project sites/parishes across the three sub-counties3in Kitgum district provided a fairly equal number of
respondents. The respondents came from a sum total of fifteen villages from within the four target
parishes.
A significant number 50% of the WCA-respondents never had any formal education and a fairly large
number 42% studied only up to the primary level of education. Less than 10% attained more than primary
level of education.Over 10% of the women interviewed had produced more than eight children. The rest had between 1-7
biological children.
3.3
THE PROJECT DESIGN
3.3.1
Womens participation/ involvement in the design and the realization of the project
More than a third of the beneficiaries acknowledged that they were consulted at the design of the project
This according to them was done through community meetings organized by their local leaders in
collaboration with the local health officials and members of the Rotary Club of Kitgum.
Most of the target group interviewed intimated that they were not engaged by the implementation team
to improve the project implementation process.
3.3.2
Effectiveness of the project according to various stakeholders
More than three quarters of Women and Girls of Child Bearing Age interviewed thought that the project
addressed the specific concerns pertaining to mother and child health in the target areas.
The project satisfied the pressing health needs of the target population according to the WCA interviewed
They pointed out that there was need for vaccination of children, counselling on family planning, access to
VCT services, and attendance of ANC visits by pregnant mothers which the project specifically addressed.
The projects Local Government focal person observed that the project was holistic in its approach to
mother and child health covering key components like ANC, immunization, family planning and referra
according to government policy. She also noted that despite its mandate, the project provided emergency
services to all and normal services to PWDs and the elderly. A VHT member in Okuti parish, Orom sub-
county qualified these claims in the following statements;
3Orom (Okuti and Akurumo), Mucwini (Pajong) and Akwang (Lamit/Tumangu)
8/10/2019 Final Copy End Term Evaluation Report
15/45
END TERM EVALUATION REPORT
July 22, 2014
15
Lokom and Lachom are hard to reach areas and the implementing team penetrates up to there. You
find children of up to five years of age not immunized yet and it is through the project that we have
started reaching out to such children. There are very many patients in those areas and the project really
helped them. Other activities like ANC, PMTCT for all mothers who cannot come here, those mothers
are really glad to have the RCK operating here.
A VHT member in Pajong, Lagot Mucwini sub-county also noted;
The biggest benefit that RCK brought was accessibility to health services i.e. before they came, women
used to go for ANC up to Mucwini, and even for vaccination they had to come up to HC here but now all
this has stopped because RCK now goes to them, even those who used to complain of distance and
those who were lazy, that excuse is no longer there.
Another VHT member from Akurumo parish who participated in an FGD conducted there opined that the
maternal and child mortality rates have drastically reduced with the intervention of the project. She noted;
Prior to the project implementation the neighboring villages here experienced frequent mother and
child death resulting from risky deliveries and lack of vaccination respectively. But as I speak now this
has tremendously reduced because pregnant mothers are promptly counseled through repeated ANC
visits on what to do to ensure their safety and that of their babies before and after deliveries
The VHTs talked to in the study also noted how positively the project has changed the health seeking
behaviour of WCA. A VHT member in Tumangu/Lamit parish echoed this view in the following words;
Today with the help of the project, women are more aware aboutwhat to do in order to protect theirhealth and that of their babies. Mothers strictly follow the vaccination schedules to ensure that their
children get all the recommended vaccines. They also pay early and regular ante natal visits compared
to before the intervention
However the project did not attain its target of ensuring that 50% of all deliveries were carried out by a
qualified health worker at a health facility. By April 2014 the projects target area recorded only an average
of 20% level of professionally attended deliveries4.
3.4
IMPLEMENTATION
3.4.1
Implementation strategies and procedures
The project management team developed a work plan in consultation with the clients, government
agencies and other stakeholders to ensure effectiveness5. The beneficiaries therefore knew before hand
the time and place (designated locations) of arrival of the project treatment team.
4Official District Health Statistic ANNEX I
8/10/2019 Final Copy End Term Evaluation Report
16/45
END TERM EVALUATION REPORT
July 22, 2014
16
The Project Coordinator pinned on her office wall a chart indicating all the activities to be implemented
under the project for specific periods of time.
The relationship among the implementing team was great. The staff members were motivated, disciplined
and professional in doing their job. The donor representative noted;
Florence(the PC) trained a cohesive and dedicated team which showed up on time for work, had open
communication with her staff, and promoted trust and loyalty. She is an excellent leader. The midwife
Alicewas an excellent role model as well, with a good work ethic. Job, the bookkeeper was bright and
believe honest.
3.4.2
Attitude of the local people towards the project
Most 68/91% of the WCA interviewed were aware of the MCH project by the RCK, the rest had no idea.
Almost all 85% of those who knew about the project were interested in it. 81% of those WCA who showed
interest in the project participated in it in one way or the other. Their participation in order of importanceinvolved receiving treatment, health education, immunization, and ANC among others.
Almost all the Key Informants interviewed indicated that they were involved in the MCH project in
different ways. For example the village leaders (LC Is) indicated that they were involved in mobilizing the
community to sweep and organize the venue for the treatment sites and to look for seats for the health
workers when they go for outreach and encouraging the community to send the women and children for
treatment. The health facility staff also indicated several ways in which they were involved in the MCH
project. A Health Assistant in one of the local HC II noted;
I go with them to the field and perform the duty of records. I conduct tallying like number of
immunization, record and register out patients. I also record child immunization card, date of return
visits and many other things in immunization card. At times I do RDT6as well as mobilization. Other
staff members handle immunization, ANC, checking children under five and sometimes Adults, relevant
of complicated cases. They pick us and we go and check patients and we also immunize children.
3.4.3
Participation gaps noted in the project by some stakeholders
The beneficiaries thought they could have participated in the project more by getting a platform within the
project to share their opinions with the implementing team. They also highlighted the idea of havingadequate access to information as another way by which they could have been better involved in the
project.
5Visits/treatment days were scheduled for the various project sites on a weekly basis; Pajong on Tuesday, Akurumo on Wednesday,
Lamit on Thursday and Okuti on Friday6Rapid Diagnostic Tests
8/10/2019 Final Copy End Term Evaluation Report
17/45
END TERM EVALUATION REPORT
July 22, 2014
17
Most key informants interviewed expressed the opinion that they were adequately involved in the MCH
project because they were engaged in the services that they could offer. A VHT from Akurumo parish,
Orom sub-county noted;
I think the involvement is already adequate because we have always worked as a team. They havehelped us a lot because this is a hard to reach area. They were also the ones who give us gas cylinder
for the fridge, sometimes when we run out of vaccines and since they come here weekly they bring
some to us from town. We also use their data from the field as part of our outreach activities data.
However some of the Sub County and parish leaders expressed mixed feelings about their involvement in
the MCH project and its core activities and suggested not being adequately engaged. A parish leader who
took part in the interviews noted;
I think RCK feared to adequately involve the parish chiefs in their activities because of financial issues,
they imagined we would be expensive and so excluded us from their activities completely.
3.4.4
The project monitoring
To their credit, the designers of the project put together the relevant project documents one would need
to monitor a project. There was the projectslogical frame highlighting key indicators, the projects budget
outlining the different costs and the projects work plan among others. Apparently the Project Coordinator
indicated to the evaluation team that a monitoring tool (checklist) was used by the steering committee
and other stakeholders to monitor the project implementation.
The donor was adequately represented in monitoring the projects implementation which involved their
representative travelling with the field team to most of the projects locations.
However reporting on the progress of the project covered strictly the core aspects of the project i.e.
expected outputs and outcomes. The reports could have covered intervening factors during
implementation, status of the budget and other broader issues on mother and child health in the district
among others.
3.4.5
Support that WCA received from the project
56/78% of those interviewed received at least some form of support from the MCH project, 16% did not.
The support included treatment for minor ailments (38%), receipt of Primary Health Care materials like
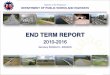
mama-kits and immunization against TT for mothers and the five killer diseases for children under five(22%), receipt of contraceptives and access to ANC and basic medical tests. Mentioned was also made of
access to ambulance and counseling services provided by the project.
8/10/2019 Final Copy End Term Evaluation Report
18/45
END TERM EVALUATION REPORT
July 22, 2014
18
Figure 1Source: Overall project statistics Annex II
The rate of immunization remained low for most of the project period except for de-worming and vitamin
A which started high, dipped for some 5 months and then rose again to record levels. Vaccination for the
six killer diseases did not exceed 20 children for each of the 15 project months. Crucially the project did
not reach the 85% vaccination target for children eligible for DPT-HepB+Hib1 but vaccinated only 9% by
June 2014.
3.5RELATIONSHIP WITH STAKEHOLDERS
3.5.1
Government
The project had a good relationship with relevant government agencies like the DHO, the political
leadership and the local health centres. The government assigned to the project one of its senior nursing
officer to ensure that the projects intervention addresses the districts health priorities regarding MCH
and collaborated with RCK Kitgum during the entire process of project design and recruitment of staff. A
member of RCK management committee noted;
They (government) were very supportive, during the initial planning we plann ed together as a team
even the project design we did together. We also did the interview for staff recruitment t together, the
CAO, the DSC, the DHO and even the traffic police sent representatives when we were recruiting the
driver and the other staff as well.
0
100
200
300
400
500
600
NUMBEROFCHILDRENVACC
INATED
PROJECT DURATION 2013/14
RATE OF IMMUNIZATION DURING THE PROJECT IN THE TARGET AREAS
BCG
DPT-HepB+Hib1DPT-HepB+Hib2
DPT-HepB+Hib3
Measles
Polio "0"
Polio 1
Polio 2
Polio 3
Vitamin A < 5yrs.
Deworming < 5 yrs.
8/10/2019 Final Copy End Term Evaluation Report
19/45
END TERM EVALUATION REPORT
July 22, 2014
19
The project was offered a well furnished office space at the district health department as well as two
nursing assistants/midwives. The district paid the bill for office utilities such as electricity and water for the
entire project period and helped to build a solid relationship with Rotary club international. The clubs
treasurer noted;
The DHO and the LC5 also wrote to the donor an acknowledgement letter that they received the
money in the Bank Account of Rotary Club of Kitgum and also that they have received the vehicle
bought which was a very good gesture of cooperation.
The project worked in collaboration with the relevant district health staff in the target areas whereby it
provided these personnel the necessary facilitation. The projects Local Government Focal person noted;
The project management gave allowances to the district health staff it engaged in some of its
activities hence motivating them to dedicate themselves to the project
The district also provided the project with drugs and antigens needed during some of its field visits. One of
the projects Nursing Assistant noted;
When we were procuring drugs from the NMS, the CAO gave us the Tin number for the district because
NMS does not sell drugs to anyone.
The local government further facilitated the project to secure an ambulance for its operations. The clubs
treasurer pointed out;
When we were buying the vehicle, we used the local government and we were exempted from paying
tax and we saved over 52 million Uganda shillings. The local government also helped us to register the
car as an ambulance further helping us to save a lot of money.
3.5.2
The donor
The donor was closely involved with the project right from the design through to implementation. The
donor representative from Mount Airy Rotary Club expressed the functional relationship she had with the
Kitgum team in the following terms;
Rudolf Schachner, myself and Simon Lawoko, past President and Club Foundation Chair for Kitgum
Rotary discussed various possibilities for projects and presented them to the Rotary Club Kitgum whichselected the Mother/Child Mobile Clinic project
The donor representative also revealed how they fully played their role as an important stakeholder of the
project to ensure its success. She noted;
8/10/2019 Final Copy End Term Evaluation Report
20/45
END TERM EVALUATION REPORT
July 22, 2014
20
I filled the Rotary Application form and raised the needed 30,000, which our District matched, as did
the Foundation. Mr. Sunday Abwola, the project point person and Past President of Rotary Kitgum and
I corresponded by email on various hiring and payment issues
However on one occasion the implementing team crucially omitted the donors opinion on the need todivert funds within the project.
3.5.3
The local health structures
The project worked with the existing health structure including the local health centre staff, VHTs and
TBAs. These health personnel helped the project implementing team in vaccination, dispensing medicine,
counselling and health education among others. One of the projects Nursing Assistants noted;
The local health facilities and personnel have been very supportive of our work, we normally notify the
VHTs of our coming so they can mobilize the community in time. They also willingly came with us for
the outreach program in the community. I do not think we could have realized the project outcomes if it
were not for them
3.5.4
The Management Committee-MC of RCK
The Project Coordinator noted how supportive the management committee had been during the course of
the projects implementation. She underlined the MCs willingness to provide them the necessary
autonomy at the same time offering support supervision both at office and in the field, as well as giving
feedback on their periodic monthly reports. She intimated;
The Management Committee has been so reliable, they responded fast to our calls ensuring that
activity implementation goes on smoothly
A Nursing Assistant also noted;
Most of the committee members were committed because when we make a work plan we follow it
through. What I like most is that sometimes members surrendered their own vehicles and we would use
them to go to the field to conduct our monitoring activities.
However it was also indicated that the committee did not adequately execute all of its oversight roles for
example in monitoring field activities. A committee member pointed out;
May be we did not support them enough in one way or the other, we were supposed to have a
monthly support visit but we turned it to quarterly instead. You know we are a loose group like
Teachers, bankers, business men and because of that we do not have much time to go about all this
activities but at least we managed to do it quarterly.
Staff appraisal was also not well followed through by the Management Committee. An MC member noted;
8/10/2019 Final Copy End Term Evaluation Report
21/45
END TERM EVALUATION REPORT
July 22, 2014
21
Theother thing was on the staff appraisal. In the first year we failed to do this, we were supposed to
receive appraisal from the Project Coordinator of the lower staff which she did in the second year and
she gave us a report. Then the PC who was supposed to be appraised by the Rotarians was never
appraised. She was later appraised by the consultant but we never got the report.
3.6
Challenges faced during the project implementation
The target group for the most part did not experience any serious challenge during the implementation of
the project safe for lapses in time keeping by the treatment team, limited access to the services by adults
(especially adult males), limited drugs, and long distances to the treatment centers.
The Project Coordinator (a Registered Nurse, with over twenty years of experience) indicated that the
staffing for the project was rather low as they had to do several assignments including consultation, clinica
work, immunization and dispensing of drugs every other treatment day.
The PCs view resonated with those of the projects clients on drug shortages. She noted;
Sometimes during implementation we could not offer patients the drugs they needed after diagnosis
and prescription which was rather frustrating for all those involved
At the same time, she lauded the indefatigable district offices and relevant personnel who came to the aid
of the project in this regard from time to time.
The Technical staff and the steering committee also cited some challenges faced during the implementation o
the program. One of the project staff noted;
We nearly gave up going back to certain areas because mobilization was very poor. You go there and
meet no body which is quite a waste of resources. When the team brings us the statistics from the field,
areas like Pajong had zero attendance twice. We then moved fast and held stakeholders meetings
which made us realize it was as a result of misinformation because the community thought we were
only doing immunization but when we clarified then they started coming in big numbers.
The project also encountered some political challenges as well as conflicting with the local health priorities
in Lamit (one of its target areas) where there was an ongoing epidemic of the nodding syndrome disease.
A key informant from the area noted;
In otherareas like Tumangu there was political interference because their priority was in managing
nodding syndrome so they refused to make a shelter for us at first. Then when we went and talked to
them they realized our work was also important.
The VHT for their part noted inadequate facilitation as a major challenge they experienced during the
project implementation. This included limited operational gears (transport means/bicycles, gumboots,
8/10/2019 Final Copy End Term Evaluation Report
22/45
END TERM EVALUATION REPORT
July 22, 2014
22
torches, raincoats, and umbrella), low stipends and little or no refreshments on treatment days, though
they conceded that the Club provided them with eight pieces of soap as token of appreciation on a regular
basis. A VHT participant in an FGD in Akurumo noted;
During rainy seasons the mud in this area is at knee level which makes our operation especially duringemergency at night quite nightmarish. It would have been quite helpful if the Club considered providing
us with gumboots, torches, umbrellas and rain coats for operations of this nature
Some of the planned activities were not fully implemented due to one reason or another. An important
stakeholder of the project pointed out the low level of implementation of planned seminars for loca
stakeholders in MCH in service training. She noted;
The budget for the Project Manager in Germany was high. He did not complete the 4 Seminars for
local stakeholders in MCH in service training for which 2920 was allocated, but completed one only. He
said that he was going to do the other three in May, a month before the project ended. I expected theseminars to be spread out over the length of the project so they could impact the success of the
project.
Some stakeholders also feared that poor timing of some of the project activities could have diminished
their impact for the project. One of the project partners noted;
The capacity building training of TBAs in 3-5 day workshops, budget 4672 USD, took place way too late
-over half-way through the project, so the effect was diluted.
The project also faced competition with other NGOs implementing similar projects in the area. In Pajongparish, Mucwini sub-county, the evaluation team witnessed Marie stopes (an NGO) providing reproductive
health services to the same target beneficiaries. The funding partner representative qualified this claim in
the following words;
The numbers served in the areas with poor roads, and the competing NGO were low. When the team
had holidays, the villagers were not served. This results in the villagers not being certain when to
attend the clinics.
3.7
PROJECT PERFORMANCE AND IMPACTS
3.7.1 Access to health services for women
More than three quarters of women asked asserted that the coming of the project resulted into significant
increase in access to health services by mothers and children. A lesser number 21% thought the project did
not bring much change in access to health services by mothers and children in the area. A woman
respondent from Pajong parish, Lagot A village in Mucwini sub-county noted;
8/10/2019 Final Copy End Term Evaluation Report
23/45
END TERM EVALUATION REPORT
July 22, 2014
23
To a large extent most women now go to the Health Center except those who are really unable but
also those ones endeavor to go to HC after delivery.
A VHT member highlighted the gradual increase in the turnout of women on treatment days in the
following words;
I think the attendance increases by the week. When we first started you would only see 10 patients in
a day but right now you can see for yourself. In the past children would not even be vaccinated, they did
not value vaccination or ANC or even delivering at H/C but the number has increased a lot.
The intervention of the project has led to a remarkable increase in access to health services for mothers
and children according to more than half of the women interviewed. A fifth of the women interviewed also
thought the health status of mothers and their children improved as a consequence of the project. A
significant number also opined that womens attitude towards regular ANC visits has improved overtime.
Figure 2 Source: Overall project statistics ANNEX II
The chart above provides a general outlook on the trend of morbidity for mothers and children in the
project area. It indicates that the overall level of morbidity by common diseases steadily declined during
the project period especially for intestinal worms, malaria and ARTI (Acute Respiratory Tract Infection).
0
100
200
300
400
500
600
REPORTED
CASES
DURATION OF THE PROJECT 2013/14
TOP TEN CAUSES OF MORBIDITY IN THE PROJECT'S TARGET AREA
MALARIA
ARTI
INTESTINAL WORMS
ACUTE DIARRHOEA
EYE INFECTION
SKIN DISEASES
SEVERE MALNUTRITION
DYSENTRY
TRAUMA
PNEUMONIA
8/10/2019 Final Copy End Term Evaluation Report
24/45
END TERM EVALUATION REPORT
July 22, 2014
24
Figure 3 Overall project statistics ANNEX II
The graph above shows a general rise in the health seeking behavior of women in the project target areas.
ANC re-attendance particularly skyrocketed during the project period which demonstrates the effect the
project had on the attitude of the target group.
The Local Government project focal person reechoed the above situation asserting;
Before the project was implemented, pregnant womens attitude toward attendance of ANC was very
low due to long distance from the nearest health facility but this has markedly improved with the
coming of the project
3.7.2 State of the local referral system
About three quarters of the respondents expressed awareness of an existing referral system in their
communities. This according to them involved the use of ambulance, hiring of Boda-bodaby caregivers
and writing referral letters by the VHTs among others.
The state of roads was commented on by the projectsgovernment focal person as a serious draw back onthe existing referral system. She noted;
KDLG is trying its best to achieve MDG targets 4&5 for maternal and child health but is handicapped
by poor infrastructure such as telecommunication and roads which makes referral of pregnant mothers
in hard to reach areas to deliver at the health center nearly impossible
0
10
20
30
40
50
60
70
01
-Apr
01-May
01-Jun
0
1-Jul
01
-Aug
01
-Sep
01
-Oct
01
-Nov
01
-Dec
01-Jan
01
-Feb
01
-Mar
01
-Apr
ATTENDANCERATES
PROJECT DURATION 2013/14
KEY INDICATORS FOR MOTHER AND CHILD HEALTH IN THE PROJECT AREAS
ANC 1
ANC 4
ANC re-attendance
Family planning
IPT 1
IPT 2
8/10/2019 Final Copy End Term Evaluation Report
25/45
END TERM EVALUATION REPORT
July 22, 2014
25
Setting up a health centre nearer to where its clients are settled, building motorable access roads, and
establishing and ambulance service came out strong as some of the ways of enhancing the health seeking
behaviour among women at risk and emergency. Health education was also considered by the
respondents to be effective in getting women at risk and emergency to seek health care. Others
recommended making the existing health facilities more reliable and building a strong referral network to
encourage the above category of women to seek medical help.
The two charts above show that at the start of the project both pregnant and non-pregnant women had a
more positive attitude towards TT vaccination. A steady decline was recorded for both categories
plummeting to rock bottom mid-way the project. Thereafter a steady positive change was noted in
womens attitudes towards the end of the project.
Figure 4 Source: Overall project statistics ANNEX II
The chart above also represents a positive improvement in the attitude of women towards healthy life
choices like PMCT in the above case.
010
20
30
40
50
60
70
01-Apr
01-Jun
01-Aug
01-Oct
01-Dec
01-Feb
01-Apr
TT VACCINATION FOR
NON PREGNANT WOMENTT 1
TT 2
TT 3
TT 4
TT 5 05
10
15
20
25
30
35
01-Apr
01-Jun
01-Aug
01-Oct
01-Dec
01-Feb
01-Apr
TT VACCINATION FOR
PREGNANT MOTHERS
DURING THE PROJECT TT 1
TT 2
TT 3
TT 4
TT 5
0
5
10
15
20
25
30
35
40
NUMBER
TESTED
THE PROJECT DURATION 2013/14
PREGNANT WOMEN TESTED ON HIV IN THE PROJECT AREAS
8/10/2019 Final Copy End Term Evaluation Report
26/45
END TERM EVALUATION REPORT
July 22, 2014
26
3.7.3
Hygiene and disease prevention
Most of the mothers in the target areas seemed to have received health education on hygiene and disease
prevention under the project as indicated by 81% of those interviewed.
The key to good personal health according to 40% of the WCA interviewed was having and properly using
the main WASH facilities i.e. pit latrine, rubbish pit, and utensil stand among others. A significant number
22% of those asked also thought personal hygiene and grooming were key ingredients to good personal
health.
In order to live in a clean and healthy environment the respondents thought it would be realized by having
the relevant WASH facilities, cleaning ones compound, proper use of the WASH facilities and cleaning
water holding containers among others.
To ensure good personal health the WCA asked intimated that one ought to in orderofimportance wear
clean clothes, bathe frequently, cut their finger nails, wash hands often, exercise, eat balanced diet, live
within a clean compound and drink clean water among others.
3.7.4
Attitude towards family planning
Three quarters of the WCA interviewed were sensitized about family planning. The key message that they
got from the sensitization included child spacing, use of contraceptives and the advantages of Family
Planning among others.
Most of the WCA interviewed indicated that to control pregnancy they would in order of importance use
pills, implants, and condoms among others. 7% of the women interviewed did not know what they would
do to control pregnancy. Another 7% interesting thought they would abstain during their menstruation
period to avoid getting pregnant.
Varied opinions were put across regarding family planning by the WCA interviewed; generally they thought
the practice is good for the health of mother and child, and for the economic well being of the family.
Some thought their husbands should be excluded from the arrangement because they would most likely
refuse to comply. Others expressed fears for the side effect of Family Planning especially the prospect of
becoming barren. The women interviewed noted that most men and the community elders are opposed to
practice citing that its against procreation which they consider a duty of man and women in a marriage.
3.7.5
Current use of family planning methods among WCA
More than half of the women questioned were using some kind of family planning method/contraceptive.Significantly 41% did not use any family planning method. The reasons why some women would not use
any family planning method range from fear of side effects, lack of awareness, their husbands refusal, and
dislike for the practice among others.
3.7.6 Womens attitude towards ANC1 to ANC3 visits.
8/10/2019 Final Copy End Term Evaluation Report
27/45
END TERM EVALUATION REPORT
July 22, 2014
27
All the women interviewed were pro antenatal visit citing numerous benefits among them protecting the
health of the mother and child, handling complicated pregnancies, and PMCT services to mentioned but a
few.
One VHT member from Orom subcounty, Okuti parish noted;
Yes in a way that the mothers down in the village started seeing the importance of ANC and family
planning. They started getting cards, they started coming in large numbers for revisits. If you compare
with the previous years, the numbers just keep increasing. In fact Locom and Lokom have biggest the
numbers for return dates than any other villages.
3.7.7
WCA attitude towards giving birth at the Health Centre
The study revealed that most women in the target area would pay antennal visits to the local health unit
when pregnant. The women interviewed cited sudden labor pain, long distance to the nearest health
facility and poor transport means among others as the reasons for home deliveries. The women asked did
not consider home delivery as the next best alternative but asserted that it only happened due to
unavoidable circumstances.
The women interviewed expressed a good level of appreciation of the merits of delivering at a health
facility. The advantages of Health Centre delivery according to them included limited chances of infection,
attendance by qualified and competent personnel, access to relevant materials like the mama-kits, free
counselling, and fast and quality services which reduces excessive pain.
3.7.8
The capacity of VHTs and TBAs to perform health education
VHTs trained and mentored by the project engaged in health education for the target community as
expected. The WCA 69% interviewed acknowledged that they attended health sensitization meetings
conducted by VHTs.
84% of the women who attended the health education sessions organized by VHTs seemed satisfied by
their capacity to deliver the sensitization contents. The VHT members interviewed also demonstrated their
competence to the evaluation team on how they conducted health education sessions in their
communities. A VHT member in at the FGD conducted in Akurumo parish noted;
A lot has improved regarding our work for mothers and children; we now handle them in a more
professional way compared to before, we also know how to read the symptoms and signs of common
diseases that afflict mothers and children in the area
The Key Informants interviewed at the health facilities expressed mixed feelings about the work and
commitment of VHTs. The in-charge of Akilok HC II positively noted;
They do it(their work) well because they have taken long and they are always within the community
and they are continuously trained by various agencies. Given any new disease outbreak they always get
trained so I think they are competent enough
8/10/2019 Final Copy End Term Evaluation Report
28/45
END TERM EVALUATION REPORT
July 22, 2014
28
Others expressed reservation on the commitment and work of the VHTs. For example the Akilok in-charge
noted;
Considering that this is a rainy season many of the VHTs find it difficult to juggle between their private
work and the work of Rotary Club so normally they come late.
Some VHT members were not competent enough to deliver the services expected of them. A HC staff in
Akilok HC II, Okuti parish pointed out;
Sometimes the VHTs do not know how to administer certain drugs like vaccines whereby some of the
children get swollen arms and end up being taken to the hospital so this has to improve. There are
some VHTs who are more active than others so to me I think more effort should be put on the active
ones so they can reach more people
3.8
The level of sustainability/self-reliance achieved by the project
A third of the women interviewed thought the project initiatives would not be sustained after the closure
of the project. The remaining two thirds thought the project initiatives would be sustained or were not
sure altogether. The donor representative expressed the fears he observed in the beneficiaries should the
project leave in the following words;
The villagers themselves are quite attached to the clinic and do not want it to end.
A significant percentage 29% of the women/girls of child bearing age were of the opinion that continuity of
the projects initiatives could only be ensured by extending the timeframe of the project a little forward.
Others suggested that the government should set up a health facility in the respective areas which would
offer similar services.
When the WCA were asked about what they would do to sustain access to important supplies and
materials like the mama-kits and mosquito nets after the project, they responded that the project has to
continue for them to access these things or they would have to turn to their local health centers or
purchase them. Others mooted the idea for proper maintenance of some of the re-usable materials in this
package as a way out for them among others.
However some key informants at the health facilities noted that they would use the government PHC
funds to maintain some of the equipments that were donated to them by rotary club like the gas cylinders
A health center staff asked on this matter noted;
We have resources like the PHC funds that we can use for that and the district also helps to refill the
gas cylinder. We shall still use the PHC resources or we improvise with what the district can offer. Like
for gas cylinder we shall resort to using charcoal stove
8/10/2019 Final Copy End Term Evaluation Report
29/45
END TERM EVALUATION REPORT
July 22, 2014
29
The projects Local Government focal person noted that KDLG will sustain the projects initiatives by re
absorbing the projects personnel especially the midwives into its mainstream structure, ensuring the
districts yearly (FY) health planning caters for these hard to reach areas/project locations. She also
pledged that the relevant government agencies would provide post project monitoring of the projects
locations.
Evidently the government was setting up health facilities in the areas where RCK implemented the MCH
project particularly in Tumangu/Lamit and Akurumo where HC IIs were under construction. The Treasurer
of RCK steering committee noted;
In areas where we have worked i.e. Akuromo and Tumangu the government has now built health
centers, and also recruited staff to work in those health centers including one of our midwives to work
there full time
The District Local Government also indicated readiness to meet some of the operation costs of RCKespecially on their ambulance services. The Clubs Treasurer intimated;
They have included fuel for our ambulance in their budget for this financial year, they already have
four ambulances that they budget for so plus this one there are now five ambulances budgeted for by
the district this financial year.
8/10/2019 Final Copy End Term Evaluation Report
30/45
END TERM EVALUATION REPORT
July 22, 2014
30
4.
CHAPTER IV
4.1
CONCLUSION AND RECOMMENDATIONS
4.2
Performance on targets
4.2.1
Project objectives
4.2.1.1The projects target areas registered 32% safe deliveries (at HC) against the set project target of
50%. This was a commendable accomplishment on the part of the project as it achieved more than
half of its target. Regrettably the baseline data for this target at the start of the project was not
available to the evaluation team though the needs assessment conducted prior to the intervention
presented a rather needy situation.
4.2.1.2Up to 40% ANC re-attendance was recorded during the project period against the project target of
65%. This by all means is a good level of performance well over fifty percent of the project target.
Though this statistic was not specifically for all the stages of ANC visits but only for re-attendance itstill remain a good measure of this target.
4.2.1.3At least three quarters of the local population in the projects target area were aware of the
possibility of a referral system for woman at risk and emergencies. This implies a commendable
level of achievement in creating awareness on the same in the local community.
4.2.2
Result I
4.2.2.1The target parishes/treatment centers were visited once a week or four times a month unless
otherwise which demonstrates an excellent performance against the set target of two visits per
month to the project locations. The project also covered far more than the planned sixteen (16)
villages but 39-40 villages. This can be put at more than 200% coverage which was a stunningachievement by the project.
4.2.2.2A remarkably low percentage 9% (317 children
8/10/2019 Final Copy End Term Evaluation Report
31/45
END TERM EVALUATION REPORT
July 22, 2014
31
4.2.4
The project design
4.2.4.1RCK consulted with the target community to establish the exact challenges of mother and child
health that they faced. The club did this through community meetings and a needs assessment
This kind of initiative at the formulation of a project is recommended to ensure the effectiveness of
a given intervention.
4.2.4.2The project addressed the specific needs of the target group/communities in as far as mother and
child health is concerned. This is quite reassuring of the possible positive long term outcomes for
mother and child health that the intervention promises.
4.2.4.3The project in addition to its mandate reached out to other groups including emergency cases, the
elderly and PWDs in desperate need of medical services. This demonstrates the flexibility exercised
within the project to ensure that it addresses emerging issues related to its mandate.
4.2.4.4There has been a noticeable positive change in the health seeking behavior of WCA in the target
areas of the project implying an improvement in the health situation of the mother and child.
4.2.5
The project implementation
4.2.5.1To a large extent the implementation team was transparent in its dealings during the project
implementation especially by involving most of the key stakeholders in the process. The project
implementing team was disciplined, motivated and professional under the competent leadership of
a seasoned nursing officer (PC).
4.2.5.2The target beneficiaries i.e. WCA were fully aware of the project and actively participated in it
especially by attending and receiving treatment/vaccination for themselves and their babies.
4.2.5.3The project was well received and owned by the beneficiaries and their communities who
thoroughly utilized the services it offered.4.2.5.4
Notably the project fully engaged the respective health workers like in-charges, health assistants
and VHTs in its areas of operation and at the district level. This ensured quality health service
delivery coming from the project as well as enhancing its chances for sustainability.
4.2.5.5The activities that the project implemented met the expectations of the beneficiaries and other
stakeholders and largely fulfilled the promises of the project as outlined at its launch. This
underlines the trust that the Club has built in the community with the implementation of this
project.
4.2.5.6Some planned activities were not fully implemented whereas another took so long to implement.
These discrepancies would certainly diminish the desired effect expected of the respectiveactivities.
4.2.5.7The monitoring system was found to be wanting despite the availability of supporting documents
like the logical framework. This would deprive the various project stakeholders from continually
providing the right kinds of responses to challenges and opportunities that emerged during the
implementation.
8/10/2019 Final Copy End Term Evaluation Report
32/45
END TERM EVALUATION REPORT
July 22, 2014
32
4.2.5.8The internal control system for the project needed to be tightened so as to ensure timely and
effective communication between stakeholders regarding resource utilization among others.
4.2.5.9Beneficiary opinion on the project implementation was not seriously sought on an ongoing basis
which deprived the project of valuable ideas to continuously tune itself to the needs of the target
communities.
4.2.5.10 Local leaders at the village level were more involved in the project implementation than their
sub-county level counterparts. This situation does not augur well for accountability within the
project and the necessary political support.
4.2.6
Relationship with stakeholders
The project enjoyed an excellent relationship with the government which involved sharing of personnel,
office space, medical supplies and procuring an ambulance for the project among others. This relationship
facilitated the achievement of the project goals a great deal.
The project could have done more to engage other partners involved in implementing similar interventions
in its target areas. This would have ensured even more efficiency in the delivery of its stated objectives.
4.2.7
Challenges
4.2.7.1The project had to co-opt some personnel from the district health structure to supplement its
limited staff capacity (number). This posed a potential risk for the project as these government
functionaries are expected to be at their stations full time.
4.2.7.2There was inadequate drug supply on some occasions during the project imp lementing teams field
trips/treatment days. Again the project had to rely on government to supplement its stock whichmight have turned out not quite reliable.
4.2.7.3The sub-county leaders in Akwang/lamit parish were less than impressed with the projects choice
of intervention as the apparently most feared cause of child morbidity (the nodding syndrome) did
not get the attention it deserved. This disparity in opinion between the sub-county leadership and
the project management sapped away at the opportunity for synergy.
4.2.7.4The VHTs were not adequately motivated to secure their total commitment in the project. This
probably explains their reluctance to take initiative to further the projects cause like organizing
frequent education units for mothers.
4.2.7.5
Poor infrastructure in terms of communication and transport was a barrier in the projectimplementation and will continue to jeopardize access to health services for mothers and children
even after the project.
4.2.8
Project performance and impact
4.2.8.1Overall the project performed well in terms of addressing the problem of inaccessibility to vita
health services for the mother and child in hard to reach areas.
8/10/2019 Final Copy End Term Evaluation Report
33/45
END TERM EVALUATION REPORT
July 22, 2014
33
4.2.8.2The intervention resulted into visible positive outcomes in the health situation of mothers and
children. The rates of morbidity and mortality from common illnesses dropped markedly during the
project highlighting the success registered by the project.
4.2.8.3The counseling and sensitization that the project offered through its health workers on hygiene,
family planning and antenatal care visits significantly on a positive note changed the health seeking
behavior of WCA in the project area.
4.2.8.4The project revived the referral system in the target areas by building the capacity of the local
health service structure and offering ambulance service which will continue to operate in the
project areas long after the closure of the project.
4.2.8.5Though most women are now aware and willing to practice various family planning methods, men
and the elderly are still reluctant and sometimes against the idea of FP. This calls for continued
effort to break conservatism with regards to procreation for the benefit of individual households
and the entire community.
4.2.8.6
Despite the sensitization of community members on the maintenance of both personal and
environment hygiene there appears to be a reluctance to seriously practice the awareness that has
been imparted in these communities implying a recurrence of already diminished common
illnesses.
4.2.8.7WCA in the target areas now have adequate awareness of the benefits of HC deliveries and a
positive attitude to go with it. This is bound to cut back the rampant maternal and child mortality
that arise from poorly conducted deliveries.
4.2.9
The capacity of VHTs
The VHTs trained and mentored by the project are today better skilled and prepared to provide healthservices for the mother and child. They have acquired both soft and hard skills in their domain of work
making them more resourceful and reliable to protect the health of the mother and child.
However there is still need for further training of VHTs to provide some basic health services that they are
mandated to carry out in their areas of operation.
4.2.10
The project sustainability
The project beneficiaries do not trust the government to carry forward the projects initiatives in the
manner that the RCK conducted it.
The beneficiaries will not be able on their own to sustain the supply of some of the materials they received
from the project like the mama-kit in the short run.
The relevant government agencies have the necessary resource and political will to carry out some of the
projects initiatives like the ambulance service for hard to reach areas.
8/10/2019 Final Copy End Term Evaluation Report
34/45
END TERM EVALUATION REPORT
July 22, 2014
34
4.3RECOMMENDATIONS, INSIGHTS AND LESSONS LEARNT.
4.3.1 The technical staff and the steering committee established that carrying out an integrated
approach to implementation of activities can produce excellent results as it was the case with this
project. The project offered a whole package for mother and child health making the intervention
quite effective and meaningful.
4.3.2 Having a good working relationship with key stakeholders is crucial for the success of a project.
Given the cordial relationship the project enjoyed with the relevant government offices, it was in
position to address so many of the challenges that it faced for better results.
4.3.3 Good collaboration with the local leadership and engaging the existing relevant structures like VHTs
and TBAs is crucial for the success of a project.
4.3.4 Concrete baseline data against which the project targets are set must be established (through a
thorough needs assessment exercise) and made accessible to all relevant stakeholders. This would
ensure effective monitoring and accountability among the projects stakeholders.
4.3.5
A project being implemented should also monitor and document the performance of otheractors/partners undertaking similar interventions in its target area/with its target beneficiaries.
This would enhance efficiency and maximize the expected project outcomes.
4.3.6 Support visits/follow-up and mentoring should be provided to trainees under every project so that
they are properly engaged in rolling out the skills and knowledge they gained for the benefit of the
community members.
4.3.7 Flexibility within a project is highly recommended as it would allow for unforeseen circumstances
and ensure that emerging needs are continually addressed within a project.
4.3.8 Adequate dialogue has to happen between stakeholders to ensure that they are on the same page
during project implementation. This would enhance collaboration, ownership of project outcomesby stakeholders and project sustainability in the long run.
4.3.9 During the implementation of this project it was noted that building of trust and confidence among
beneficiaries was important for sustenance of a project outcomes and project ownership among
beneficiaries.
4.3.10 The suitability and capacity of the personnel hired to implement the project must be carefully
considered. This is to ensure that activities are implemented adequately and on time. Untimely and
inadequate implementation of planned activities would diminish their effects for the project.
4.3.11 It is important to make community participation a reality than just for its own sake. This would
ensure undivided support and commitment by the beneficiary community to the projectscause.4.3.12 A proper monitoring plan or framework with clear baseline data, indicators, targets, responsible
persons, and timeframe among others is highly recommended for every project to measure
progress towards set objectives and goals.
4.3.13 A consumer/client feedback mechanism ought to be established within a project for timely and
appropriate response. This would enhance the effectiveness of a given intervention and ensure
that emerging challenges within the project are addressed on a continual basis.
8/10/2019 Final Copy End Term Evaluation Report
35/45
END TERM EVALUATION REPORT
July 22, 2014
35
4.3.14 A stakeholder analysis and