Embed Size (px)
Citation preview

Scientifi c American Surgery DOI 10.2310/7800.2092
12/14
© 2014 Decker Intellectual Properties Inc
gastrointestinal tract and abdomen
F I S S U R E , F I S T U L A , A N D A B S C E S S E S
Elisa H. Birnbaum, MD, FACS, FASCRS, and Ira J. Kodner, MD, FACS, FASCRS
Fissure
An anal fi ssure is a small tear within the anal canal distal to the dentate line. Approxi-mately 90% of anal fi s-sures are located in the posterior anal canal. Anterior fi ssures are more common in women. Fis-sures can be character-ized as acute or chronic [see Figure 1]. Acute fi s-sures are small tears in the anal mucosa. They usually respond to med-ical treatment and typically resolve within 4 to 6 weeks. Chronic fi ssures or anal ulcers have been present for longer periods of time. They are associated with sentinel tags, rolled mucosal edges, and hypertrophic anal papilla at the fi ssure apex. Chronic fi ssures are less likely to heal with medical management. Fissures found laterally or in multiple loca-tions within the anal canal may be indicators of other dis-ease processes. Infl ammatory bowel diseases such as Crohn disease, syphilis, and tuberculosis and even squamous cell carcinomas can cause ulcers within the anal canal [see Figure 2]. An anal ulcer seen in an aberrant location warrants further investigation.
etiology
Constipation, diarrhea, straining, and heavy lifting are leading causes of fi ssures. A small tear occurs in the anal mucosa at the dentate line. The underlining internal anal sphincter muscle is exposed and irritated with further passage of stool. Over time, the internal anal sphincter may
become hypertonic from involuntary spasm. The majority of fi ssures are caused by straining during passage of a consti-pated stool. Patients with chronic fi ssure pain may not be able to recall the inciting event.
symptoms
Acute
There is typically a history of acute pain that began after passage of a constipated stool. This pain may continue even if the bowel movements are soft and is often described as a sharp, tearing, or searing pain that occurs after the passage of stool and lasts a few minutes. Occasionally, patients will complain of hours of throbbing pain and the desire to avoid having a bowel movement. Bleeding is usually minimal and frequently noticed on the toilet paper. The blood is bright red and can occasionally drip into the toilet. Many patients are seen in the physician’s offi ce thinking that these symptoms are hemorrhoids. A thrombosed external hemor-rhoid can be painful, but there is usually a visible external thrombosis. Internal hemorrhoids may bleed with bowel movements but rarely cause pain.
Chronic
Anal fi ssure symptoms that last 8 to 12 weeks are consid-ered chronic. There is frequently a visible external sentinel tag, which may be confused with external hemorrhoids. A
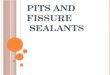
Fissure
InternalSphincterMuscle
HypertrophiedAnal Papilla
SentinelSkin Tag
ACUTE FISSURE CHRONIC FISSURE
Figure 1 Chronic anal fi ssures, as opposed to acute fi ssures, are characterized by hypertrophy of the anal papilla, a sentinel skin tag, rolled skin edges, and exposed internal anal sphincter muscle.
ANTERIOR
POSTERIOR
Acute and Chronic Anal Fissure
Crohn DiseaseUlcerative Colitis
SyphilisTuberculosis
LeukemiaCancer
HIV
Crohn DiseaseUlcerative Colitis
SyphilisTuberculosis
LeukemiaCancer
HIV
Acute and Chronic Anal Fissure
Figure 2 The location of anal fi ssures suggests their cause.40

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 2
Approach to the Patient with Fissure,Abscess, or Fistula
Patient has fissure, abscess, or fistula
Lesions are classified as perianal, ischiorectal, supralevator, or intersphincteric.Clinical manifestations: constant perianal pain, sometimes with fever, chills, or malaise; purulent discharge occasionally occurs, and systemic toxicity rarely develops. Visual inspection usually suffices for diagnosis. Management: surgical drainage, usually in office but sometimes in OR.
Anorectal abscess
Lesions are classified as intersphincteric, transsphincteric, suprasphincteric, or extrasphincteric.Clinical manifestations: small opening in perianal skin, surrounding induration, ongoing drainage.Management: surgical unroofing of entire fistula tract (fistulotomy), except in select cases (e.g., anterior fistulas in women) in which partial unroofing is recommended; closure of internal opening with advancement flap is an option. Ligation of intersphincteric fistula tract (LIFT) may be done for patients in whom continence is compromised.
Fistula in ano
Clinical manifestations: pain, minor bright-red bleeding, split in anoderm (usually in midline). Chronic fissure is signaled by hypertrophic anal papilla, sentinel skin tag, and exposed internal sphincter muscle. Visual inspection suffices for diagnosis.Management: for acute fissures, nonoperative measures (e.g., fiber, stool softeners); for chronic fissures, if such nonoperative measures fail, lateral internal sphincterotomy (alternatives: topical NTG, topical nifedipine, topical diltiazem, botulinum toxin injection).
Anal fissure

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 3
large internal hypertrophic anal papilla may be present, leading to confusion with internal hemorrhoids. Patients with chronic anal fi ssure continue to complain of anal pain, although they may also complain of diffi culty with hygiene and perianal itching. The pain may be described as more of a throbbing, aching pain after bowel movements, and, occasionally, patients will not have pain at all.
examination
Patients who are seen for anal fi ssures typically have a classic history. Physical examination may be diffi cult because the patient has a tender anal canal and may be fear-ful of worsening pain. A digital rectal examination is rarely necessary at the initial evaluation. Inspection of the anal canal can be done in the prone jackknife or lateral decubitus position by gentle retraction of the perianal skin. A posterior fi ssure can often be seen as a simple tear in the anoderm. If there is a posterior sentinel tag, the fi ssure is usually visible just below the tag. Treatment should be started without further examination. A digital rectal examination is not necessary if a fi ssure is visualized as it will only worsen the patient’s pain. If a digital rectal examination is possible, spasm of the anal sphincter and increased pain with gentle pressure on the fi ssure will be noted. Anoscopic and procto-sigmoidoscopic examination can be delayed until resolution of the acute pain.
Patients with chronic fi ssures may not be as tender and may allow a more thorough examination. A chronic fi ssure has the appearance of a deeper ulcer with fi brosis of the internal anal sphincter and occasionally heaped-up mucosal edges around the fi ssure. Patients typically have a posterior sentinel tag, which has the appearance of a skin tag. An internal hypertrophic anal papilla may be palpable within the anal canal. Pain on digital rectal examination is gener-ally not as severe, and there is typically less anal spasm.
treatment
Medical
Two thirds of patients can be successfully treated with conservative measures.1 Increasing the fl uid and fi ber is gen-erally the fi rst step to managing the patient’s constipation. Fiber supplements, stool softeners, and laxatives may be added to improve bowel function. Patients who have chroni c diarrhea need to try to control the watery bowel movements because they act as a chemical irritant. Patients who develop an anal fi ssure after straining and heavy lifting need to cur-tail those activities until the symptoms have resolved. Symp-tomatic relief may be obtained with warm tub soaks after bowel movements.2 Topical lidocaine is very short acting and does not provide any signifi cant relief. The practice parameters set forth by the American Society of Colon and Rectal Surgeons state that medical management should be the fi rst-line treatment for anal fi ssures because there are few side effects and patients can be successfully treated in this manner.3
Topical nitroglycerin (0.2% NTG) and nifedipine (2%) have been shown to decrease pain, with variable rates.4–9 A very small amount is applied to the anoderm every 4 to 6 hours for 4 to 6 weeks. Headache is the primary side effect and is dose related.4,10 For patients with cardiac disease and
migraine headaches, these topical agents should be used cautiously. Healing rates are variable and range from 48 to 78%, although a recent Cochrane report concluded that topical NTG is only marginally better than placebo.10 Fissure recurrence after topical treatments is higher when compared with outcomes after surgery. The symptoms of chronic fi ssures are less likely to resolve with medical management, but nonetheless, medical management should be attempted before surgical intervention.
Patients whose symptoms do not resolve with medical management and who are not candidates for lateral sphinc-terotomy may improve with injection of botulinum toxin.11–13 There is no consensus on the dosage, site of administration, or effi cacy of this treatment. Typically, 50 to 100 units of botulinum toxin is diluted with 1 mL of sterile saline and injected in 0.2 mL aliquots. Most reports discuss injection of botulinum toxin into the internal anal sphincter around or near the fi ssure. The effects of botulinum toxin are not immediate, and patients should be counseled that it can take up to 3 days before the full effects are felt. Healing rates are reported to be between 60 and 80%.11–13 The most common side effect is temporary incontinence to fl atus, which can occur in up to 18% of patients.12,13 Fecal incontinence can occur in up to 5% of patients, but given that the effects wear off in 3 months, this typically improves with time. Recurrent symptoms may occur, but patients can be retreated success-fully. Patients in whom symptoms of anal fi ssure do not improve with botulinum toxin should be referred for surgery.
Surgical
Operative treatment of fi ssure disease consists of a lateral internal anal sphincterotomy.14,15 A lateral internal anal sphincterotomy is preferable to a posterior sphincterotomy to avoid a keyhole deformity. The sphincterotomy can be done in either an open (under direct visualization) or closed fashion.16,17 Surgical choice depends on the patient’s symptoms, fi ndings, and the experience of the operating surgeon.
Surgery can be done with local or regional anesthesia. A prone-fl exed position is preferable [see Figure 3]. The
Figure 3 Operative management of ulcer/fi ssure disease. The patient is positioned on the operating table in the prone-fl exed position, with a soft roll under the hips.

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 4
can a large sentinel tag, if hygiene is an issue. If done, care should be given to avoid additional transection of underly-ing muscle. A controlled anal stretch has been recommended by some authors. This procedure, done either manually or with pneumatic balloon dilatation, stretches both the inter-nal anal sphincter and the external anal sphincter. Despite the efforts to control the amount of stretch, this procedure causes burst injury to the anal sphincters and may increase the likelihood of posttreatment fecal incontinence. Anal stretch is not a recommended procedure.15
Postoperative care is relatively simple. Patients are instructed to remain on the high-fl uid and -fi ber diet. It is recommended that they take a stool softener or fi ber supple-ment in addition to laxatives for several weeks after surgery. Pain control can be immediate, and it is recommended that minimal narcotics be used. Soaking in a tub of warm water may help alleviate some postoperative discomfort. Patients should expect to have a slight increase in postoperative discomfort if excision of sentinel tags, hypertrophic anal papillas, or hemorrhoids is done concurrently. Simply show-ering or soaking after a bowel movement is all that is neces-sary for anal hygiene. Antibiotics and medicated wipes are not necessary.
Urinary retention is one of the most common complica-tions and can be avoided by decreasing the amount of fl uid given in the perioperative period. There should be very little postoperative pain almost immediately after surgery. If the patient does complain of signifi cant pain, especially in the presence of fever or urinary hesitancy, one must assume that the site may be infected. Urgent evaluation, removal of
buttocks are taped apart. Local anesthetic is injected after short-acting intravenous sedation is given to the patient [see Figure 4]. Placement of a medium Hill-Ferguson retractor allows visualization of the fi ssure and palpation of the hypertrophic internal anal sphincter. The groove between the internal and external anal sphincter should be easily palpated. The anal fi ssure is typically visible in the posterior or anterior quadrant. If there are any stigmata of Crohn dis-ease, a sphincterotomy should not be performed. The lateral sphincterotomy can be performed as a closed procedure using a No. 11 blade and digital palpation of the muscle [see Figure 5]. An open procedure with clear identifi cation of the internal anal sphincter before transection may be a safer option [see Figure 6]. A 1 cm incision is made in the lateral perianal skin over the intersphincteric groove. A curved hemostat is inserted into the intersphincteric groove, and the lower one third to one half of the internal anal sphincter is elevated into the incision. Division of the muscle is done with the cautery for hemostasis. The internal sphincter is divided, but the external sphincter, anoderm, and longitudi-nal muscle remain intact. If a rent is made in the anal mucosa, it should be repaired with a dissolvable suture to prevent a potential fi stula. Pressure is maintained for several minutes to ensure hemostasis. Digital examination should confi rm adequate transection of the hypertrophic sphincter. The sphincterotomy wound is left open.
Excision of an acute fi ssure is not necessary, nor is it necessary to excise a posterior chronic ulcer. Both acute and chronic fi ssures will generally heal with simple sphincter-otomy. A large hypertrophic anal papilla can be excised, as
a b
Figure 4 Operative management of ulcer/fi ssure disease. (a) Five milliliters of bupivacaine is injected into subcutaneous tissue. (b) Ten milli-liters of local anesthetic is injected deep into the sphincter muscle on each side of the anal canal.

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 5
follow-up
Most patients have no pain on their postoperative evalu-ation 2 to 4 weeks after the procedure. A digital rectal examination should confi rm good healing of both the lateral sphincterotomy site and the posterior fi ssure. A small defect may be palpable in the lateral sphincterotomy site.
Abscesses
Anorectal abscesses most often originate from cryptoglandular infections within the anal canal. It is pre-sumed that the small crypts at the dentate line become obstructed, lead ing to a localized infection. The infection develops along the ducts leading from the inter-nal crypts and follows the path of least resis-tance. These abscesses are classifi ed as perianal, ischiorectal, intersphincteric, or supralevator based on the location of the infection [see Figure 7].21 Perianal abscesses can also be associated with trauma, malignancy, Crohn disease [see Figure 8], fi ssure, tuberculosis, and actinomycoses. Infec-tions can also occur after anal surgery for hemorrhoids or fi ssures.
Perianal and ischiorectal abscesses account for the major-ity of cryptogenic infections. A perianal abscess is present at the anal verge. Ischiorectal abscesses tend to be larger and more complex. They present as a tender, fl uctuant fullness lateral to the anal canal. Supralevator abscesses occur above the levator ani muscles. These rare infections are diffi cult to diagnose as there is generally not a palpable external mass. Patients with supralevator abscesses present with severe rectal pain and may have a fl uctuant intrarectal mass on digital rectal examination.
symptoms
Patients with anorectal abscesses may present with a variety of symptoms ranging from pain, erythema, fl uctuant mass, and fevers. Occasionally, there are no external fi nd-ings, and patients complain of deep-seated internal rectal pain. The abscess is the acute phase of infection, and most patients present to the emergency department or their physicians with complaints of pain. Spontaneous rupture can occur, which decompresses the infection, relieving some of the symptoms of pain. A patient with a partially drained abscess will present with seropurulent discharge.
treatment
Once the diagnosis is made, the treatment for anorectal abscesses is drainage. A very superfi cial abscess may be drained in the offi ce or emergency department. More complex, deeper abscesses and recurrent infections should be drained in the operating room. In general, laboratory evaluation is not necessary unless the patient shows signs of systemic sepsis. It is also not necessary to obtain a computed
any sutures, antibiotics, and close observation are indicated. If the lateral sphincterotomy site is infected, a small drain should be placed to manage the sepsis rather than débridement of normal tissue.
Incontinence to fl atus occurs in approximately 10% of patients.18–20 For many, this resolves over time. Seepage of stool (< 7%) and frank incontinence (< 0.1%) are rare and diffi cult to manage postoperative complications. It is best to avoid these complications by proper preoperative evalua-tion of patients. Any patient with complaints of diarrhea or mild seepage should not undergo sphincterotomy if at all possible. Particular attention should be paid to women who have had vaginal deliveries with episiotomies or tears because their anal sphincters may be compromised. Care must be taken when dealing with patients with Crohn dis-ease as these patients may have a history of anal disease or may develop anal disease in the future. Posterior sphincter-otomy or excision of posterior chronic fi ssures should be avoided because of the risk of keyhole deformities. This deformity may cause prolonged anal seepage because of the confi guration of the scar tissue gaping posteriorly.
Figure 5 Operative management of ulcer/fi ssure disease. Shown is the closed approach to posterior lateral internal sphincterotomy. A No. 11 blade is inserted in the intersphincteric groove and moved upward to the level of the dentate line. Medial movement of the blade divides a portion of the internal sphincter muscle. The anoderm and the other anal muscles are not divided.

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 6
a b c
Figure 6 Operative management of ulcer/fi ssure disease. Shown is the open approach to posterior lateral internal sphincterotomy. (a) The triad of the ulcer complex is visualized. (b) Once the hypertrophied band of internal sphincter muscle is identifi ed, a 1 cm incision is made in the posterolateral aspect of the perianal skin. (c) The hypertrophied band is elevated into the wound and divided with the electrocautery.
Supralevator
Ischioanal Perianal Intersphincteric
a b
Figure 7 Anorectal abscesses are classifi ed according to the space in which they develop.
Figure 8 Operative management of abscess and fi stula. Shown are alternatives for treating abscess or fi stula associated with Crohn dis-ease. In Crohn disease, multiple perianal and perineal fi stulas and abscesses may be seen, often in atypical locations. (a) Abscesses may be drained by placing a small mushroom-tipped catheter as close to the anus as possible. A Malecot catheter should not be used. (b) In some settings, it is appropriate to place a seton between internal and external openings. The seton may then be left in situ for a time for drainage and for prevention of further disease progression.
tomographic (CT) scan or magnetic resonance image (MRI) to confi rm the diagnosis. Preoperative antibiotics are not needed for the majority of patients. The American Heart Association recommends that patients with prosthetic heart valves, previous endocarditis, and congestive heart disease and heart transplant patients should receive preoperative antibiotics.22 Patients with signifi cant cellulitis, immuno-compromise, and diabetics are often given preoperative antibiotics as well.23
It is preferable to do the incision and drainage procedures under local or regional anesthesia in the operating room. Positioning the patient in the prone-fl exed position allows
for access to the anal canal [see Figure 3]. The buttocks are taped open for better visualization. Incision and drainage close to the anal verge in the region of fl uctuance is the treat-ment of choice for perianal and ischiorectal abscesses. If a superfi cial fi stula is identifi ed at the time of operation, a fi stulotomy may be performed [see Figure 9].24 If an internal opening is not identifi ed, a small incision should be made over the most fl uctuant area closest to the anal verge. This allows decompression of the abscess and, if the abscess does not heal completely, a short fi stula tract. Placement of a

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 7
a
b
c
ExternalSphincterMuscle
InternalSphincterMuscle
Figure 9 Operative management of abscess and fi stula. Shown is a fi stulotomy in a patient with cryptoglandular abscess/fi stula. (a) The fi stula tract is carefully probed, a decision is made about which muscle and how much muscle to cut, and the tract is incised. (b) Once the tract is open, the involved crypt is excised. (c) The defect is marsupialized by sewing skin to the tract.
a b
are best managed in the operating room.26 Aspiration of the postanal space with a 16-gauge needle may confi rm the presence of purulent material within the postanal space. An incision is then made in the perianal skin posterior to the anal verge and opened into the anal canal in the posterior midline. This procedure typically divides the superfi cial and subcutaneous internal and external anal sphincter. Counterincisions and drains may be necessary to drain the horseshoe infections in the ischiorectal fossa if they are present [see Figure 11].
Postoperative care is relatively simple. Antibiotics are not necessary except in patients with signifi cant cellulitis. Patients are instructed to use a pad as necessary and that the drainage and pain should decrease in several days. Pain medication, stool softeners, and laxatives are given to patients, and they are instructed to shower or take warm tub soaks for perianal hygiene. Most patients return to the offi ce within 2 to 4 weeks. The mushroom catheter can be removed at that time if the drainage is minimal. If an internal opening is identifi ed, the mushroom catheter should be left in place and the fi stula should be addressed.
After drainage of a perianal abscess, one of three things may occur: (1) the abscess may heal spontaneously, and the patient will have no further symptoms; (2) the abscess heals but recurs in the future, most likely due to a recurrent abscess along a fi stula tract; or (3) the abscess does not heal, and the patient develops a chronic draining fi stula in ano. Unfortunately, there is no defi nitive way to predict who will develop a fi stula. Recurrent abscess rates after incision and drainage can be as high as 50%. The recurrences are most likely due to the formation of fi stulae. Horseshoe abscesses are associated with increased rates of fi stulization ranging from 18 to 50%.26,27
Figure 10 Operative management of abscess and fi stula. Shown is drainage of an ischiorectal abscess. Such abscesses may be palpated above the anorectal ring, even though their location is more inferior. (a) The abscess is incised. (b) A mushroom-tipped catheter is placed.
small No. 10 mushroom catheter into the cavity allows for drainage and avoids unnecessary pain and trauma caused by packing [see Figure 10].25 The catheter can be removed several weeks later when the infection resolves. An alterna-tive would be to make an elliptical incision over the fl uctu-ant area decompressing the abscess. The incision should be large enough to decompress the cavity. Packing is not necessary and leads to undue pain. If an internal opening is identifi ed and the fi stula tract goes deep to the sphincter, drainage can be maintained with the placement of a seton. A small vessel loop is preferable to a cutting seton. The non-reactive Silastic allows for drainage of the purulent material and is well tolerated by patients.
An intersphincteric abscess is best treated by identifying the internal crypt and dividing the internal anal sphincter within the anal canal. Supralevator abscesses are rare and are the most diffi cult to identify and treat. If recognized, they are best treated by internal drainage rather than cross-ing the levator plate. This minimizes the complexity of the fi stula tract should one form after drainage.
A deep postanal space abscess may lead to a horseshoe-type abscess with fl uctuant areas on either side of the anal canal. Patients present with deep rectal pain or coccygeal pain and complain of diffi culty with defecation. A high degree of suspicion and fullness on digital rectal examina-tion helps make the diagnosis. These complex abscesses

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 8
InternalOpening Fistula Tract
ExternalOpening
Probe
ab c
Figure 11 Operative management of abscess and fi stula. Shown is the surgical treatment of a horseshoe fi stula. (a) The main posterior tract of the fi stula is identifi ed by probing. (b) The posterior tract is opened, and drains are placed laterally. (c) The posterior tract is marsupialized.
Fistula
An anal fi stula occurs as the chronic form of perianal abscess. It is a communication (tract) from the anal canal to the perianal skin. Pa-tients complain of drain-age, swelling, and pain at an external drainage site. Most patients will give any history of prior perianal abscess with either surgical or spon-taneous drainage. Fistu-las are classifi ed based on anatomic course relative to the anal sphincter (inter-, trans-, supra-, and extrasphincteric) [see Figure 12]. They can also be classifi ed as simple or complex.28 Simple fi stulas are predominantly low trans- or intersphincteric fi stulas, which are relatively easy to treat. Complex fi stulas are high trans-, supra-, or extrasphincteric abscesses and horseshoe abscesses, which are more diffi cult to identify and treat. Patients with infl ammatory bowel dis-ease and anterior fi stulas in woman are considered complex fi stulas and deserve special consideration. These patients may already have compromised sphincters from previous injury and are prone to fecal incontinence if aggressive surgery is undertaken.
treatment
In the acute phase, drainage of the abscess is important. This is best done under anesthesia in the operating room. Local anesthesia may be used for simple abscess fi stula dis-ease. Regional or general anesthesia is preferable for com-plex fi stulas and patients with multiple or recurrent tracts.
A prone-fl exed position with the buttocks taped apart is preferable and makes visualization easy. The internal open-ing may be identifi ed using a combination of probes and injection of saline, hydrogen peroxide, or dye. Goodsall’s rule can be used as a guide to fi nd the internal opening, but it is imperative not to form a false passage if the internal opening is not identifi ed [see Figure 13].
The external opening is identifi ed, and the fi stula tract may be palpated heading toward the anal canal. The internal opening may be felt as a small dimple within the anal canal. Anoscopic examination may reveal purulent material or mucus at the internal opening. A small probe can be passed from the external opening toward the internal opening. Occasionally, the probe can be passed from the internal opening more easily. Care is taken to avoid forcing the probe or creating false passages. Sharp angulation of the tract may prevent the probe from passing easily. In this instance, injection of dye, peroxide, or even saline may be done by inserting a 16-gauge angiocatheter through the external opening while visualizing the internal anal canal. Fistulog-raphy is rarely necessary and is reserved for more complex and long tracts.
Surgical treatments most commonly consist of unroofi ng the fi stula tract (fi stulotomy). The probe is passed through the fi stula tract and palpated under the skin. A fi stulotomy is performed if the tract is superfi cial and does not involve a signifi cant portion of the external sphincter. This unroofs the fi stula tract and allows it to heal by secondary intention. The chronic granulation tissue is curetted and cauterized. The internal opening should be destroyed with the cautery. It is not necessary to perform a fi stulectomy or removal of the epithelialized tract. Fistulectomies are generally avoided to minimize destruction of the external anal sphincter. If the fi stula tract involves a signifi cant portion of the external anal sphincter, a partial fi stulotomy should be performed. This

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 9
entails division of the fi stula tract from the external opening to the anal sphincter. At the level of the anal sphincter, a seton can be placed through the remainder of the fi stula tract. This allows the external portion of the fi stula to heal and minimizes injury to the external anal sphincter. The seton facilitates drainage and will help guide future sur-gery.29 The internal and external openings will not heal as long as the seton is in place. An advancement fl ap or ligation of intersphincteric fi stula tract (LIFT) procedure can be done to close the internal opening after removal of the seton. A cutting seton can be used to gradually unroof transsphinc-teric tracts. The gradual tightening of the seton causes fi brosis and minimal separation of the anal sphincter. Some patients may experience pain caused by tightening the seton, and some reports note an increased risk of fecal incontinence.30 The success rate with superfi cial fi stulotomy ranges from 90 to 97%. Higher recurrence rates are associ-ated with complex fi stulas, failure to identify the internal opening, and Crohn disease. Postoperative alterations in continence range from 0 to 70% of patients. Risk factors
a b
c d
Figure 12 Fistula in ano is classifi ed on the basis of its relation to the anal sphincter muscles. Shown are (a) intersphincteric fi stula, (b) transsphincteric fi stula, (c) suprasphincteric fi stula, and (d) extrasphincteric fi stula.
Curved Tract
Straight Tract
Transverse Line 3 cm
Figure 13 Goodsall’s rule. An external opening seen posterior to a line drawn transversely across the perineum will originate from an internal opening in the posterior midline. An anterior opening will originate in the nearest crypt (for fi stulas within 23 cm of the anus).40

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 10
a
Internal Opening of Fistula Tract External Opening of
Fistula Tract
External AnalSphincterMuscles
FistulaTract
Tip of Probe
Internal Opening of Fistula Tract
Fistula Tract Exposed inIntersphincteric Groove
Probe in Fistula Tract
External Opening of Fistula Tract
Internal AnalSphincter Muscles
Intersphincteric Groove
include preoperative incontinence, recurrent disease, previ-ous vaginal deliveries, previous surgical treatment of the anal fi stula, and complex fi stulas.
Several newer procedures have been devised to treat fi stula tracts that are not amenable to fi stulotomy. Fibrin glue is a fairly simple concept with low incontinence rates. The internal and external openings need to be identifi ed to ensure that the tract is completely fi lled with the glue. The glue is injected into the tract using a specialized catheter and allowed to set up prior to moving the patient. Healing rates using fi brin glue are variable and range from 10 to 67%.31,32
Bioprosthetic fi stula plugs have been designed for use in chronic fi stula tracts. These are typically placed after the
infection has been controlled with a noncutting seton. Sev-eral confi gurations of the fi stula plug are available. The plug is passed through the fi stula tract, and the internal opening is secured with a suture. The internal opening is generally closed with a suture, and the external opening is left open for drainage. The bioprosthetic material acts as a matrix for ingrowth of fi brin, and the procedure can be done with little morbidity. The success rates for closure of fi stula tracts range from 50 to 70% and may relate to the length of follow-up.33,34 Dislodgment of the plug is felt to be a primary cause of failure.35
More recently, a surgical procedure called LIFT has been popularized [see Figure 14].36,37 This procedure can be done
Figure 14 Ligation of intersphincteric fi stula tract. (a) Identify the fi stula tract and probe in the intersphincteric groove. (b) Divide the fi stula tract after removal of the probe.
Internal Opening of Fistula Tract
Divided Fistula Tract
External Opening ofFistula Tract
Tie
Tie
b
Internal Opening ofFistula Tract External Opening of
Fistula Tract
Intersphincteric Groove
Divided Fistula Tract

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 11
Incision
a
Rectal Fistula
bFistula in Mucosal Flap
Mucosal Flap
Cut Edge of Circular Muscle
Fistula
Flap Advanced overReconstructed Perineal Body
Portion of Flap withFistula Excised
c
Flap Sutured in Place
d
Figure 15 Advancement fl ap. (a) Create a broad-based mucosal fl ap. (b) Dissect the fl ap 4 cm above the internal fi stula opening. (c) After closing the muscularis over the internal fi stula, advance the fl ap. (d) Secure the fl ap.
under local or regional anesthesia on an outpatient basis. A seton is placed fi rst and left in place for approximately 8 weeks to allow the fi stula tract to fi brose. At the time of surgery, a probe is passed through the fi stula tract. A small incision is made in the intersphincteric groove while palpat-ing the probe. The tract is then isolated, ligated, and divided within the intersphincteric groove. There is no division of the anal sphincter. The internal opening may be sutured closed and the external opening widened for drainage. Small series have been published in the literature, with variable rates.36,37 Often the internal opening will close, and a shortened external tract can then be divided at a second procedure.
Advancement fl ap repair is a sphincter-sparing repair [see Figure 15]. It has a high success rate in the treatment of com-plex fi stula tracts. These repairs are more involved, complex procedures with higher morbidity. A broad-based, thick mucosal and submucosal endoanal fl ap is created proximal
to the fi stula opening. Suture closure of the internal opening is done with dissolvable suture. The endoanal fl ap is then sutured to the anoderm with dissolvable suture. Care is taken to maintain good blood supply to the fl ap and to cre-ate a tension-free repair. Postoperative morbidity is gener-ally due to a subfl ap hematoma or infection. The success rate ranges from 70 to 90%.38,39 Posterior fi stulas, recurrent fi stu-las, and those related to Crohn disease are less successfully treated with an advancement fl ap.
Financial Disclosures: Elisa H. Birnbaum, MD, FACS, FASCRS, and Ira J. Kodner, MD, FACS, FASCRS, have no relevant fi nancial relationships to disclose.
References
1. Hananel N, Gordon PH. Re-examination of clinical mani-festations and response to therapy of fi ssure-in-ano. Dis Colon Rectum 1997;40:229–33.

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 12
2. Gupta P. Randomized, controlled study comparing sitz-bath and no-sitz-bath treatments in patients with acute anal fi ssures. Aust N Z J Surg 2006;76:718–21.
3. Perry WB, Dykes SL, Buie WD, Rafferty JF; Standards Prac-tice Task Force of the American Society of Colon and Rectal Surgeons. Practice parameters for the management of anal fi ssures (3rd revision). Dis Colon Rectum 2010;53:1110–5.
4. Evans J, Luck A, Hewett P. Glyceryl trinitrate vs. lateral sphincterotomy for chronic anal fi ssure: prospective, randomized trial. Dis Colon Rectum 2001;44:93–7.
5. Libertiny G, Knight JS, Farouk R. Randomised trial of topi-cal 0.2% glyceryl trinitrate and lateral internal sphincterot-omy for the treatment of patients with chronic anal fi ssure: long-term follow-up. Eur J Surg 2002;168:418–21.
6. Scholefi eld JH, Bock JU, Marla B, et al. A dose fi nding study with 0.1%, 0.2%, and 0.4% glyceryl trinitrate ointment in patients with chronic anal fi ssures. Gut 2003;52:264–9.
7. Carapeti EA, Kamm MA, Phillips RK. Topical diltiazem and bethanechol decrease anal sphincter pressure and heal anal fi ssures without side effects. Dis Colon Rectum 2000;43:1359–62.
8. Ezri T, Susmallian S. Topical nifedipine vs. topical glyceryl trinitrate for treatment of chronic anal fi ssure. Dis Colon Rectum 2003;46:805–8.
9. Bielecki K, Kolodziejczak M. A prospective randomized trial of diltiazem and glyceryl trinitrate ointment in the treatment of chronic anal fi ssure. Colorectal Dis 2003;5:256–7.
10. Nelson R, Thomas K, Morgan J, Jones A. Non surgical therapy for anal fi ssure. Cochrane Database Syst Rev 2012;2:CD003431.
11. Jones OM, Ramalingam T, Merrie A, et al. Randomized clinical trial of botulinum toxin plus glyceryl trinitrate vs. botulinum toxin alone for medically resistant chronic anal fi ssure: overall poor healing rates. Dis Colon Rectum 2006;49:1574–80.
12. Maria G, Brisinda G, Bentivoglio AR, et al. Infl uence of botulinum toxin site of injections on healing rate in patients with chronic anal fi ssure. Am J Surg 2000;179:46–50.
13. Menteçs BB, Irkörücü O, Akin M, et al. Comparison of bot-ulinum toxin injection and lateral internal sphincterotomy for the treatment of chronic anal fi ssure. Dis Colon Rectum 2003;46:232–7.
14. Richard CS, Greggoire R, Plewes EA, et al. Internal sphinc-terotomy is superior to topical nitroglycerine in the treatment of chronic anal fi ssure: results of a randomized, controlled trial by the Canadian Colorectal Surgical Trials Group. Dis Colon Rectum 2000;43:1048–104.
15. Nelson R. Operative procedures for fi ssure in ano. Cochrane Database Syst Rev 2010;(1):CD002199.
16. Arroyo A, Perez F, Serrano P, et al. Open versus closed lateral internal sphincterotomy performed as an outpatient procedure under local anesthesia for chronic anal fi ssure: prospective randomized study of clinical and manometric long-term results. J Am Coll Surg 2004;199:361–7.
17. Wiley M, Day P, Rieger N, et al. Open vs. closed lateral internal sphincterotomy for idiopathic fi ssure-in-ano: a prospective, randomized, controlled trial. Dis Colon Rectum 2004;47:847–52.
18. Mentes BB, Ege B, Leventoglu S, et al. Extent of lateral internal sphincterotomy: up to the dentate line or up to the fi ssure apex? Dis Colon Rectum 2005;48:365–70.
19. Elsebae MM. A study of fecal incontinence in patients with chronic anal fi ssure: prospective, randomized, controlled trial of the extent of internal anal sphincter division during lateral sphincterotomy. World J Surg 2007;31:2052–7.
20. Ho KS, Ho KY. Randomized clinical trial comparing oral nifedipine with lateral anal sphincterotomy and tailored sphincterotomy in the treatment of chronic anal fi ssure. Br J Surg 2005;92:403–8.
21. Read DR, Abcarian H. A prospective survey of 474 patients with anorectal abscess. Dis Colon Rectum 1979;22:566–8.
22. Wilson W, Taubert KA, Gewitz T, et al. Prevention of infec-tive endocarditis. Guidelines from the American Heart Association: a guideline from the American Heart Associa-tion Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation 2007;116:1736–54.
23. North JH Jr, Weber TK, Rodriguez-Bigas MA, et al. The management of infectious and noninfectious anorectal com-plications in patients with leukemia. J Am Coll Surg 1996;183:322–8.
24. Cox SW, Senagore AJ, Luchtefeld MA, Mazier WP. Out-come after incision and drainage with fi stulotomy for ischiorectal abscess. Am Surg 1997;63:686–9.
25. Vasilveski CA. Anorectal abscesses and fi stulas. In: Wolff BG, Fleshman JW, Beck DE, et al, editors. The ASCRS textbook of colorectal surgery. New York: Springer; 2007. p. 192–214.
26. Held D, Khubchandani I, Sheets J, et al. Management of anorectal horseshoe abscess and fi stula. Dis Colon Rectum 1986;29:793–7.
27. Onaca N, Hirshberg A, Adar R. Early reoperation for perirectal abscess: a preventable complication. Dis Colon Rectum 2001;44:1469–73.
28. Parks AG, Gordon PH, Hardcastle JD. A classifi cation of fi stula-in-ano. Br J Surg 1976;63:1–12.
29. The Surgisis AFP anal fi stula plug: report of a consensus conference. Colorectal Dis 2008;10:17–20.
30. Ritchie RD, Sackier JM, Hodde JP. Incontinence rates after cutting seton treatment for anal fi stula. Colorectal Dis 2009;11:564–71.
31. Loungnarath R, Dietz DW, Mutch MG, et al. Fibrin glue treatment of complex anal fi stulas has low success rate. Dis Colon Rectum 2004;47:432–6.
32. Sentovich SM. Fibrin glue for all anal fi stulas. J Gastrointest Surg 2001;5:158–61.
33. Ky AJ, Sylla P, Steinhagen R, et al. Collagen fi stula plug for the treatment of anal fi stulas. Dis Colon Rectum 2008;51:838–43.
34. Ellis CN, Rostas JW, Greiner FG. Long-term outcomes with the use of bioprosthetic plugs for the management of com-plex anal fi stulas. Dis Colon Rectum 2010;53:798–802.
35. Champagne BJ, O’Connor LM, Ferguson M, et al. Effi cacy of anal fi stula plug in closure of cryptoglandular fi stulas: long-term follow-up. Dis Colon Rectum 2006;49:1817–21.
36. Rojanasakul A, Pattanaarun J, Sahakitrungruang C, Tanti-phlachiva K. Total anal sphincter saving technique for fi stula-in-ano; the ligation of intersphincteric fi stula tract. J Med Assoc Thai 2007;90:581–6.

Scientifi c American Surgery
12/14
gastro fi ssure, fi stula, and abscesses — 13
37. Bleier JL, Moloo H, Goldberg SM. Ligation of the intersphincteric fi stula tract: an effective new technique for complex fi stulas. Dis Colon Rectum 2010;53:43–6.
38. Perez F, Arroyo A, Serrano P, et al. Randomized clinical and manometric study of advancement fl ap versus fi stu-lotomy with sphincter reconstruction in the management of complex fi stula-in-ano. Am J Surg 2006;192:34–40.
39. Uribe N, Millán M, Minguez M, et al. Clinical and mano-metric results of endorectal advancement fl aps for complex anal fi stula. Int J Colorectal Dis 2007;22:259–64.
40. Beck DE. Hemorrhoids. In: Beck DE, editor. Handbook of colorectal surgery. 2nd ed. New York: Marcel Dekker; 2003. p. 325–44.
Acknowledgments
Figures 1, 5, and 7 through 13 Tom MooreFigures 14 and 15 Christine Kenney