Embed Size (px)
Citation preview

Five cases of cutaneous Rosai-Dorfman disease
H. V. Pitamber* and W. Grayson†‡
*Division of Dermatology, Department of Medicine, University of the Witwatersrand, †Division of Anatomical Pathology, School of Pathology,
University of the Witwatersrand, and ‡National Health Laboratory Service, Johannesburg, South Africa
Summary Rosai-Dorfman disease (RDD), previously known as sinus histiocytosis with massive
lymphadenopathy, is a benign, idiopathic histiocytic proliferative disorder. It
commonly affects lymph nodes, but any organ of the body may be involved.
Histological findings include characteristic large, pale, histiocytic cells (Rosai-Dorfman
cells) exhibiting cytophagocytosis. Immunohistochemically, these histiocytes are
positive for S-100 protein and CD68, but stain negatively for CD1a. On electron
microscopy, Birbeck granules are absent. RDD limited to the skin is rare, less than 30
cases having been reported to date. We present five further cases of purely cutaneous
RDD. Three presented as solitary nodules and one as a large, well-circumscribed
plaque. The fifth patient, who was HIV positive, had a rosacea-like facial eruption.
Introduction
In 1969, Rosai and Dorfman described a clinicopatho-
logical entity in which severely enlarged cervical lymph
nodes were infiltrated by large histiocytes exhibiting
cytophagocytosis.1 The patients had fever, leukocytosis
and hypergammaglobulinaemia. These authors named
the condition sinus histiocytosis with massive lympha-
denopathy (SHML).1 By 1988, when it was apparent
that lymph nodes were not always affected and that any
organ of the body may be involved, the designation
Rosai-Dorfman disease (RDD) was preferred.2 Lymph
node involvement alone is found in 57% of patients,
15% present with extranodal disease only, and in 28%
of patients both nodal and extranodal sites are
involved.3 The skin and the upper respiratory tract are
the most common extranodal sites, each involved in
approximately 11% of cases.3
RDD limited to the skin (now referred to as cutaneous
RDD)4 is rare, with only 29 cases documented to date.3–20
We report five new cases of cutaneous RDD. Three
presented as solitary nodules and one as a large, well-
circumscribed plaque. The fifth patient, who was
infected with the human immunodeficiency virus
(HIV), had a rosacea-like facial eruption.
Case reports
Five cases of RDD limited to the skin were diagnosed
between 1997 and 2001 by the Division of Dermatology
(cases 2 and 3) and by the Division of Anatomical
Pathology of the University of the Witwatersrand (cases
1, 4 and 5).
All five patients were South African. The clinical
details, treatment and follow-up are summarized in
Table 1. The age of onset varied from 28 to 67 (mean
45.4) years and the duration of the disease ranged from 4
to 36 (mean 19.3) months. In three cases (cases 1, 4 and
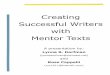
5), the lesions consisted of solitary nodules. Case 2 had a
large (8 cm · 4 cm), solitary, oval, hyperpigmented
plaque with an infiltrated raised border in the right
groin (Fig. 1a). The lesions in case 3 consisted of multiple
erythematous papules confined to the face (Fig. 1b).
All patients were asymptomatic and in good health,
with no associated lymphadenopathy or extranodal sites
of involvement apart from the skin.
Laboratory investigations
In cases 2 and 3 investigations consisted of a full
blood count, erythrocyte sedimentation rate (ESR),
Correspondence: W. Grayson, Division of Anatomical Pathology, N.H.L.S.,
PO Box 1038, Johannesburg 2000, South Africa.
Tel.: 27 11 489 8476. Fax: 27 11 489 8512.
E-mail: [email protected]
Accepted for publication 27 August 2002
Clinical dermatology • Original article
� 2003 Blackwell Publishing Ltd • Clinical and Experimental Dermatology, 28, 17–21 17

urea and electrolytes, liver function tests and serum
protein electrophoresis, as well as Epstein-Barr virus
(EBV) and human herpesvirus-6 (HHV-6) serology.
Serological tests for syphilis and HIV were performed
in cases 2, 3 and 5. Abnormal findings are shown in
Table 1.
The two patients (cases 2 and 3) who showed a
polyclonal gammopathy also had positive HHV-6 serol-
ogy and their EBV serology was indicative of a past
infection. Case 3 was HIV positive.
Skin biopsies
Multiple punch biopsies (cases 2 and 3) and excisional
biopsies (cases 1, 4 and 5) were routinely processed and
stained with haematoxylin and eosin. Additional paral-
lel sections were obtained for immunohistochemistry,
namely, S-100 protein (1 : 500; DAKO, Glostrup,
Denmark), CD68 (1 : 100; DAKO, Glostrup, Denmark)
and CD1a (undiluted; Immunotech, Marseille, France).
Ultrastructural examination was performed on addi-
tional punch biopsies taken from cases 2 and 3, and
tissue was sampled from the remainder of the gross
specimen in case 4.Tab
le1
Ro
sai-
Do
rfm
an
dis
ease
lim
ited
toth
esk
in:
clin
ica
l,la
bo
rato
rya
nd
ad
dit
ion
al
pa
tho
log
ica
lfi
nd
ing
sin
fiv
eca
ses.
Cas
eA
ge⁄s
ex⁄r
ace
Cuta
neo
us
lesi
on(s
)an
dsi
te
Dura
tion
(month
s)La
bora
tory
findin
gs
Additio
nal
his
tolo
gic
alfe
ature
sTr
eatm
ent
and
cours
e
148⁄M
⁄WSo
litar
y,in
dura
ted
nodule
(�1
cm);
left
should
er
36
NA
Exci
sion
246⁄F
⁄BSo
litar
y,hyp
erpig
men
ted
pla
que
(8·
4cm
);right
gro
in
18
ESR
47
mm
⁄hH
HV
-6+
veEB
VIg
M–v
e;
IgG
+ve
Poly
clonal
gam
mopat
hy
6an
d12
month
sla
ter:
few
erRD
cells
,
acco
mpan
ied
by
xanth
om
atous
mac
rophag
esan
dm
arke
dder
mal
fibro
sis
Topic
alst
eroid
s;par
tial
invo
lution
at12
month
s
328⁄F
⁄BM
ultip
leer
ythem
atous
pap
ule
s;fa
ce4
HH
V-6
+ve
EBV
IgM
–ve;
IgG
+ve
HIV
+ve
Poly
clonal
gam
mopat
hy
Topic
alst
eroid
s;im
pro
vem
ent
at2
month
s
467⁄F
⁄BSo
litar
ynodule
(1.5
cm);
scal
p?
NA
Scat
tere
dag
gre
gat
esof
neu
trophils
Exci
sion
538⁄F
⁄BSo
litar
y,in
trad
erm
alnodule
(3cm
);
mons
pubis
?H
IV–v
eST
S–v
eEx
tensi
on
of
infiltra
tein
tosu
bcu
tis
Exci
sion
M¼
ma
le;
F¼
fem
ale
;W
¼w
hit
e;B¼
bla
ck;
NA
¼n
ot
av
ail
ab
le;
ES
R¼
ery
thro
cyte
sed
imen
tati
on
rate
;H
HV
-6¼
hu
ma
nh
erp
esv
iru
s6
;E
BV¼
Ep
stie
n-B
arr
vir
us;
RD¼
Ro
sai-
Do
rfm
an
;?¼
un
kn
ow
n;
HIV
¼h
um
an
imm
un
od
efici
ency
vir
us;
ST
S¼
sero
log
ica
lte
sts
for
syp
hil
is.
Figure 1 (a) Hyperpigmented plaque with infiltrated edge, located
in the right groin in case 2. (b) Erythematous papular facial
eruption in case 3.
Cutaneous Rosai-Dorfman disease • H. V. Pitamber and W. Grayson
18 � 2003 Blackwell Publishing Ltd • Clinical and Experimental Dermatology, 28, 17–21

Pathological findings
Histological findings were similar in all five cases.
Additional microscopic features observed in some of
the cases are shown in Table 1. In all cases the
epidermis was normal, while the dermis contained
sheets of large, pale histiocytic cells with a dense
background infiltrate of lymphocytes and plasma cells
(Fig. 2a). Lymphoid follicles with reactive germinal
centres were present. The histiocytes (Rosai-Dorfman
cells) displayed phagocytosis of lymphocytes, plasma
cells and occasional polymorphonuclear leucocytes
(Fig. 2b); they showed diffuse cytoplasmic and nuclear
staining for S-100 protein, were weakly immunoreac-
tive for CD68, but stained negatively for CD1a.
Follow-up biopsies in case 2, taken 6 and 12 months
after initial presentation, showed a paucity of large
histiocytic cells, with predominant dermal fibrosis and
conspicuous aggregates of xanthomatous macrophages
(Table 1).
Electron microscopy showed large histiocytic cells
with ill-defined, undulating cell membranes and abun-
dant cytoplasm containing engulfed lymphocytes and
plasma cells. Some of the ingested mononuclear cells
were present within phagocytic vacuoles. Birbeck
granules were absent.
Discussion
Purely cutaneous RDD is rare, with less than 30 cases
reported to date. In 1978, Thawerani and coworkers
reported the first case in a 48-year-old man with a
solitary nodule on the shoulder and hypergammaglob-
ulinaemia.21
The lesions in cutaneous RDD may be solitary or
multiple. They usually present as papules,5,7 nod-
ules5,6,16,18,20 or plaques,4,13,15,17,19 or as a combina-
tion of these.4,10–12,17 Cutaneous RDD has also presented
as subcutaneous masses (panniculitis)7,10,13 and has
mimicked a breast mass.9,22 Three of our patients
presented with solitary nodules, two of which were
superficial, while the third had a deeper component
involving the subcutis. One patient had a large, solitary,
granuloma annulare-like plaque with a raised infiltrated
edge. Previous cases most resembling ours were multiple
giant granuloma annulare-like plaques reported by
Scheel et al.13 and a solitary hyperpigmented plaque
reported by Child et al.15 Our patient with a rosacea-like
papular facial eruption differed from the case of Ang
et al.,4 in whom an acneiform eruption consisted of
comedones and cystic nodules. Our patient was HIV
positive and is, to our knowledge, the second case of
isolated cutaneous RDD in an HIV-positive patient. The
first reported case presented as nasal nodules.18
Histological findings in RDD are characteristic and
essentially similar in all sites. A dense histiocytic
infiltrate is accompanied by a background infiltrate of
lymphocytes and plasma cells; lymphoid follicles with
germinal centres may occur.22,23 The large histiocytic
cells (Rosai-Dorfman cells) have indistinct, �feathery�borders, abundant pale eosinophilic cytoplasm and large
vesicular nuclei, exhibiting the phenomenon of emperi-
polesis (cytophagocytosis of lymphocytes and plasma
cells).3,22,23 Less often, the cytoplasm may contain
neutrophils and red blood cells.4,15 These histiocytes
stain positively for S-100 protein and CD68, but
negatively for CD1a, which confirms the diagno-
sis.3,17,19 Ultrastructurally, the large histiocytes show
Figure 2 (a) Sheets of pale histiocytes surrounded by dense dermal infiltrate of lymphocytes and plasma cells; lymphoid follicle on the left
(haematoxylin and eosin, ·230). (b) Rosai-Dorfman cell showing cytophagocytosis of lymphocytes, plasma cells and a neutrophil
(haematoxylin and eosin, ·736).
Cutaneous Rosai-Dorfman disease • H. V. Pitamber and W. Grayson
� 2003 Blackwell Publishing Ltd • Clinical and Experimental Dermatology, 28, 17–21 19

undulating villous cytoplasmic processes and emperi-
polesis. Birbeck granules are absent,3 ruling out the
possibility of Langerhans cell histiocytosis.8,16 Histolog-
ical features were similar in all our cases. The large
histiocytes, several exhibiting emperipolesis, stained
positively for S100 protein and CD68 but negatively
for CD1a, and the absence of Birbeck granules con-
firmed the diagnosis of RDD.
The aetiology of RDD remains uncertain. Two hypo-
theses have been proposed; a disturbance of cell-mediated
immunity,24 and a primary viral infection.11,15,24,25 The
immunohistochemical findings in RDD confirm the
presence of functionally activated macrophages; the acti-
vation possibly following an immune or infectious
challenge.26 EBV and HHV-6 have been implicated in
RDD.25 Luppi et al. detected a very unusual pattern of
late HHV-6 viral antigen expression in two cases
of RDD.27 Serological tests for HHV-6 were positive in
two of our cases. However, serological tests alone are not
conclusive for an aetiological role; Levine et al. recom-
mend in situ hybridization to detect HHV-6 in the
tissues.25 Both of these patients also had serological
evidence of past EBV infection, and a polyclonal gamm-
opathy. The frequent association of polyclonal gammop-
athy with RDD is supportive of an exaggerated
immunological response to an infectious agent in this
disorder.
Cutaneous RDD has a good prognosis and tends to
resolve spontaneously over months to years.4 Cutane-
ous lesions usually do not require treatment but surgical
excision may be indicated for cosmetic reasons or
symptomatic relief.4,12,15,28 Cutaneous lesions have
also responded to radiotherapy12 and thalidomide.29
Acknowledgements
We thank Prof. E. J. Schulz, Division of Dermatology,
Department of Medicine, University of the Witwaters-
rand, for her assistance with this article. We also thank
Mrs L. van der Walt, Electron Microscopy Unit, National
Health Laboratory Service (NHLS), and Mr G. Hall
(NHLS) and Mr E. Liebenberg (University of the Witwa-
tersrand) for the microphotography.
References
1 Rosai J, Dorfman RF. Sinus histiocytosis with massive
lymphadenopathy: a newly recognized benign clinico-
pathological entity. Arch Pathol 1969; 87: 63–70.
2 Foucar E, Rosai J, Dorfman RF. Sinus histiocytosis with
massive lymphadenopathy. Current status and future
directions. Arch Dermatol 1988; 124: 1211–4.
3 Foucar E, Rosai J, Dorfman RF. Sinus histiocytosis with
massive lymphadenopathy (Rosai-Dorfman disease):
review of the entity. Semin Diagn Pathol 1990; 7:
19–73.
4 Ang P, Tan SH, Ong BH. Cutaneous Rosai-Dorfman disease
presenting as pustular and acneiform lesions. J Am Acad
Dermatol 1999; 41: 335–7.
5 Tsang WY, Chan JK, Yu HC, Chow LT. Extranodal Rosai-
Dorfman disease: an uncommon cause of persistent nodule
in the ear. J Laryngol Otol 1992; 106: 249–51.
6 Chu P, LeBoit PE. Histologic features of cutaneous sinus
histiocytosis (Rosai-Dorfman disease): study of cases both
with and without systemic involvement. J Cutan Pathol
1992; 19: 201–6.
7 Puppin D Jr, Chavaz P, Harms M. Histiocytic lymphop-
hagocytic panniculitis (Rosai-Dorfman disease): a case
report. Dermatology 1992; 184: 317–20.
8 Perrin C, Michiels JF, Lacour JP et al. Sinus histiocytosis
(Rosai-Dorfman disease) clinically limited to the skin.
J Cutan Pathol 1993; 20: 368–74.
9 Mac-Moune Lai F, Lam WY, Chin CW, Ng WL. Cutaneous
Rosai-Dorfman disease presenting as a suspicious breast
mass. J Cutan Pathol 1994; 21: 377–82.
10 Skiljo M, Garcia-Lora E, Tercedor J et al. Purely cutaneous
Rosai-Dorfman disease. Dermatology 1995; 191: 49–51.
11 Perez A, Rodriguez M, Febrer I, Aliaga A. Sinus histiocy-
tosis confined to the skin: case report and review of the
literature. Am J Dermatopathol 1995; 17: 384–8.
12 Annessi G, Gianetti A. Purely cutaneous Rosai-Dorfman
disease. Br J Dermatol 1996; 134: 749–53.
13 Scheel MM, Rady PL, Tyring SK, Pandya AG. Sinus
histiocytosis with massive lymphadenopathy: presenta-
tion as giant granuloma annulare and detection of
human herpesvirus 6. J Am Acad Dermatol 1997; 37:
643–6.
14 Hafner O, Gerstel C, Bertsch HP, Vakilzaden F. Kutane
sinushistiozytose (Rosai-Dorfman-erkrankung). Hautarzt
1998; 49: 392–6.
15 Child FJ, Fuller LC, Salisbury J, Higgins EM. Cutaneous
Rosai-Dorfman disease. Clin Exp Dermatol 1998; 23: 40–2.
16 Haung HY, Yang CL, Chen WJ. Rosai-Dorfman disease
with primary cutaneous manifestations – a case report.
Ann Acad Med Singapore 1998; 27: 589–93.
17 Quaglino P, Tomasini C, Novelli M et al. Immunohistologic
findings and adhesion molecule pattern in primary pure
cutaneous Rosai-Dorfman disease with xanthomatous
features. Am J Dermatopathol 1998; 20: 393–8.
18 Perry BP, Gregg CM, Myers S et al. Rosai-Dorfman disease
(extranodal sinus histiocytosis) in a patient with HIV. Ear
Nose Throat J 1998; 77: 855–8.
19 Kang JM, Yang WI, Kim SM, Lee MG. Sinus histiocytosis
(Rosai-Dorfman disease) clinically limited to the skin. Acta
Derm Venereol 1999; 79: 363–5.
20 Chuan KL, Tan PH, Hwang SG, Ong BH. Cutaneous Rosai-
Dorfman disease – a pathologic review of 2 cases. Singapore
Med J 2000; 41: 122–5.
Cutaneous Rosai-Dorfman disease • H. V. Pitamber and W. Grayson
20 � 2003 Blackwell Publishing Ltd • Clinical and Experimental Dermatology, 28, 17–21

21 Thawerani H, Sanchez RL, Rosai J, Dorfman RF. The
cutaneous manifestations of sinus histiocytosis with massive
lymphadenopathy. Arch Dermatol 1978; 114: 191–7.
22 Ng SB, Tan LHC, Tan PH. Rosai-Dorfman disease of the
breast: a mimic of breast malignancy. Pathology 2000; 32:
10–5.
23 Carbone A, Passannante A, Gloghini A et al. Review of
sinus histiocytosis with massive lymphadenopathy (Rosai-
Dorfman disease) of head and neck. Ann Otol Rhinol
Laryngol 1999; 108: 1095–104.
24 Olsen EA, Crawford JR, Vollmer RT. Sinus histiocytosis
with massive lymphadenopathy. J Am Acad Dermatol 1988;
18: 1322–32.
25 Levine PH, Jahan N, Murari P et al. Detection of human
herpesvirus 6 in tissues involved by sinus histiocytosis with
massive lymphadenopathy (Rosai-Dorfman disease).
J Infect Dis 1992; 166: 291–5.
26 Eisen RN, Buckley PJ, Rosai J. Immunophenotypic char-
acterization of sinus histiocytosis with massive lympha-
denopathy (Rosai-Dorfman disease). Semin Diagn Pathol
1990; 7: 74–82.
27 Luppi M, Barozzi P, Garber R et al. Expression of human
herpesvirus-6 antigens in benign and malignant lympho-
proliferative diseases. Am J Pathol 1998; 153: 815–23.
28 Komp DM. The treatment of sinus histiocytosis with mas-
sive lymphadenopathy (Rosai-Dorfman disease). Semin
Diagn Pathol 1990; 7: 83–6.
29 Viraben R, Dupre A, Gorguet B. Pure cutaneous histiocy-
tosis resembling sinus histiocytosis. Clin Exp Dermatol
1988; 13: 197–9.
Cutaneous Rosai-Dorfman disease • H. V. Pitamber and W. Grayson
� 2003 Blackwell Publishing Ltd • Clinical and Experimental Dermatology, 28, 17–21 21