Embed Size (px)
Citation preview

Clinical Radiology (1983) 34, 405-411 0009-9260/83/00460405502.00 © 1983 Royal CoUege of Radiologists
Flexion and Extension Radiography of the Lumbar Spine: A Comparison With Lumbar Discography RICHARD C. QUINNELL* and HAROLD R. STOCKDALEt
Department of Orthopaedic Surgery, University Hospital, Nottingham and t Department of Medical Physics, City Hospital, Nottingham
Four methods of quantifying relative intervertebral body movement from static flexion/extension radio- graphs are reviewed and the ability of each of these techniques to indicate the site(s) of disc degeneration is compared with that of lumbar discography. Of the methods examined, that of measuring the linear displace- ment of one vertebra in the antero-posterior plane was found to be the most accurate method of indicating disc degeneracy. None of the methods examined was free from artefacts. With regard to the clinical usefulness of flexion/extension radiography, we discuss two separate situations. Firstly, the taking of a single set of flexion/extension radiographs is concluded to be of little value in the management of patients with low back pain. Secondly, flexion/extension radiography, on a serial basis, is considered to be of possible value in specific situations (for example, follow-up of a spinal fusion).
The use of fiexion/extension radiography of the lumbar spine has been reported by several authors. Bakke (1931) was the first to document in detail a radiological assessment of the spine in flexion and extension. Several other authors have discussed the need to quantify flexion and extension films with a view either to improving individual patient manage- ment or to carrying out an epidemiological study of spinal dynamics of normal or abnormal subjects (Wiles, 1935, Gianturco, 1944; Melamed and Ansfield, 1947, Begg and Falconer, 1949, Tanz, 1953 ; Rosen- berg, 1955; Israel, 1959; Hoag et al., 1960; Ho, 1962; Lindahl, 1966; Pennal et al., 1972).
Many different geometrical constructions have been proposed whereby it ought to be possible to quantify reliably the spinal dynamic behaviour. How- ever, few of these approaches are in regular clinical use.
We have assessed four such constructions on flexion/extension radiographs and we discuss the ability of each to detect the presence of disc degenera- tion, a definitive diagnosis being given by lumbar discography. We conclude that, from flexion/exten- sion radiographs, little reliable information can be obtained. As a consequence, we feel that there is a clear need to discuss the place of flexion/extension radiography in individual patient management.
*Present address: Department of Orthopaedic Surgery, Derbyshire Royal Infirmary, Derby.
$ Present address: Department of Medical Physics (Nuclear Medicine), Royal Liverpool Hospital.
PATIENTS AND METHODS
Lateral radiographs of the lumbar spine, including the upper sacrum, were taken in the extremes of flexion and extension in 30 patients with mechanical disorders of the low back. Each patient was examined in the sitting position. The radiographs were quantified using four analytical constructions, the first two of which were variants of a common principle. Each of these methods is described in detail by the original authors but we will summarise the salient points.
Methods I and II
The range of excursion was established at each disc level from L1 to $1 by measuring the change in angulation between adjacent vertebrae at the extremes of flexion and extension. These measure- ments were obtained as follows. The extension radio- graph is secured to a horizontal viewing box and a sheet of paper is held firmly on the upper portion of this film. Next, the flexion film is laid on top of the extension film with the sacra superimposed. A line is then drawn on the sheet of paper along the upper edge of the flexion film. By slightly rotating the flexion film, the two L5 vertebra images can be superimposed and a second line, again alongthe upper edge of the flexion film can be drawn on the paper. The angle between these lines is the angular excursion at the L5-S1 disc space. Similar measurements can be made at each lumbar disc space. These findings

406 C L I N I C A L R A D I O L O G Y
were compared, by inspection, with the normal range and pattern of angulation as described by Begg and Falconer (1949) (Method I) and also with the alternative description of normal angular displace- ment as given by Tanz (1953) (Method II). Begg and Falconer quoted the normal excursions as L5--S1 18 °, L4-L5 15 °, L3-L4 14 °, L2-L3 12°and L1-L2 10 °. Tanz, on the other hand, deduced the normal range of movement at each level for various age ranges and quoted a mean angulation and a standard deviation at each level for the age groups. We imposed the restrictions placed upon such predictions of normal behaviour suggested by Jirout (1957) on both methods. (Jirout proposed, in essence, that a regular incremental uniphasic movement is indicative of normality.) By including this latter proposal, an equal reduction of spinal movement at each vertebral level did not necessarily indicate abnormality.
Method III
We used the suggestion set out by Pennal e t al. (1972) in which a point of zero instant velocity was deduced. This is the point about which one vertebra appears to move in relation to its neighbours. The geometrical sequence used to deduce this point is rather complex: basically, the flexion film is laid on a viewing box and the extension film superimposed with the sacra coincident. Keeping the extension film firmly adhered to the viewing box, the flexion film is then removed and placed on top of the exten- sion film but now with the selected vertebra super- imposed. This procedure is then repeated by fixing the flexion film and removing the extension film.
.K
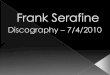
Fig. 1 - Geometrical construction for Method IV. Parallel lines WX and YZ are drawn on each vertebra equidistant from the vertebral centre, K.
The point of zero instant velocity can be deduced by recording the point of intersection of a line drawn through the central axis of the disc space as it changes its angulation on the individual flexion and extension image lay-outs.
Method IV
The fourth method of measurement involved an assessment of the forward motion of one vertebra with respect to the one below. However, this true horizontal displacement is, frequently, not reliably assessed directly from lateral radiographs for the following reasons. Firstly, the disc space may change shape when moving from flexion to extension. (The disc itself, in the normal, erect stance, may not have parallel upper and lower margins.) Consequently, it may be difficult to exclude disc tilting occurring dur- ing the relative linear displacement of the vertebrae. Secondly, the vertebral edges are frequently ill- defined due to the presence of osteophytes.
We deduced a method of measurement which avoided a direct observation of the true horizontal displacement but which gave a reasonably good approximation to this. Parallel lines WX and YZ were drawn on each vertebra as shown in Fig. 1. We measured the diagonal dimensions A and B and calculated the value of ~(A - B). This value can be shown to be proportional to the true horizontal displacement to a reasonable approximation and that its absolute value is less than the required displace- ment by about 10% for typical disc sizes seen on lateral lumbar radiographs (see Appendix).
We deduced disc generation by comparing our results against the normal values as suggested by Knutsson (1944) and Jirout (1957).
The use of the assessment of relative linear inter- body displacement to diagnose disc degeneration was first discussed by Knutsson (1944). However, it was not until the work of Morgan and King (1957) that the quantification of this construction was developed. Our geometrical construction differs from that of Morgan and King inasmuch as we were unable to share their confidence in reliably marking the verte- bral edges on the radiographs. Also, we felt that those cases of non-parallel-sided discs would not be adequately dealt with by their procedure.
In order to assess the quality of each of these four methods, we have examined the ability of each, independently, to select disc degeneration as against pressure-standardised lumbar discography (Quinnell e t al., 1980). The imaging criteria originally described by Erlacher (1952) were used to stage the discogram image in seven groups (Fig. 2). Groups 1 and 2 are

FLEXION AND EXTENSION RADIOGRAPHY OF THE LUMBAR SPINE 407
normal and increasing the group number indicates increasing degeneracy. (The annular tear described by Park et al. (1979) was included in Group 3.)
RESULTS
Flexion and extension radiographs of 30 sympto- matic individuals were quantified. We examined 111 discs: 22 at L 2 - L 3 , 30 at L3-I_6, 29 at L 4 - L 5
1 (1)(
2 (2),
6 (4)
Fig. 2 - Schematic diagram of the discogxam images. The projections are, left to right: lateral, antero-posterior and axial. Groups 1 and 2 represent normal discs. Groups 3, 4 and 5 show protruded discs of increasing severity. Groups 6 and 7 are indicative of disc degeneration. The original classification by Erlacher (1952) is shown in brackets. (This illustration was originally published by Quinnell and Stockdale (1982).)
and 30 at L 5 - S 1 . The low number of L 2 - L 3 discs was due to the fact that not all the radiographs included this particular disc. Also, one of L 4 - L 5 discs was excluded from our series because its edges were so poor ly defined on the image.
We were able to examine all 111 discs with Methods I, II and IV. However, Method III was only able to be used on 96 discs. This point is discussed further under the relevant subheading.
Method I
Using the angular displacement method set out by Begg and Falconer (1949), the ability of this pro- cedure to identify normal disc spaces can be deduced from Column I in Table 1. For the L2-I_3 level, this method selected 16 normal disc spaces of which 13 were also discographically normal. However, coinci- dentally, the discograms showed a total of 16 normal disc spaces. Similarly, at the L5-S1 level, this method produced 10 normal discs of which none was shown as such by the discogram. However, discography showed two other L 5 - S 1 disc spaces as being normal.
When selecting abnormal levels (Table 2) this method gave six abnormal discs at L2-I_3, of which two were also abnormal on the discogram. However, 16 L 2 - L 3 discs were shown as abnormal on the discogram.
The incidence of false positive and false negative findings is shown in Column I of Table 3 for all the disc levels. False negatives may not be considered to be clinically significant but false positives are unacceptable.
Method II i
Tanz (1953) foUowed along the lines of Begg and Falconer but proposed a different pat tern of normal angular changes from flexion to extension and also quoted a range o f angles consistent with normal movement. Our results using Tanz's normals are pre- sented in Column II o f Table 1 for the selection of
Table 1 - Normal disc detection*
Disc Quantification method level
I H 111 IV
Discographically normal
L2-L3 16 (13) 8 (4) 15 (10) 22 (16) 16 L3-L4 16 (11) 15 (11) 17 (11) 25 (19) 19 L4-L5 13 (5) 16 (8) 17 (7) 18 (11) 11 L5-$1 10 (0) 12 (1) 8 (0) 5 (2) 2
* The number in brackets indicates the number of discs which were detected as being normal on both the flexion/extension radiographs and the discogram.

408
Table 2 - Abnormal disc detection*
CLINICAL RADIOLOGY
Disc Quantification method level
I H III I V
Discographically abnormal
L2-L3 6 (2) 14 (4) 6 (0) 0 (0) 6 L3-L4 14 (6) 15 (7) 11 (4) 5 (5) 11 L4-L5 16 (11) 13 (10) 8 (4) 11 (11) 18 L5-Sl 20 (18) 18 (17) 14 (13) 25 (25) 28
* The number in brackets indicates the number of discs which were detected as being abnormal on both the flexion/exten- sion radiographs and the discogram.
Table 3 - Incidence o f false positive and false negative findings
Quantification method
I H II I I V
False negatives 25% 25% 42% 21% False positives 28% 22% 22% Zero
normal disc spaces and in Column II of Table 2 for the selection of abnormal disc spaces. The second column in Table 3 indicates the frequency of our false negative and false positive findings with this method. Again, there is a significant number of false positive findings.
Method III
The method of Pennal et al. (1972) gave results detailed in Columns III of Tables 1, 2 and 3. The much higher incidence of false negative findings may be clinically acceptable but, when considered together with a false positive rate of 22%, makes this pro- cedure of little value. The reduction in the number of discs analysed by this method as against the other three methods results from an intrinsic limitation of Pennal's method. If the range of spinal movement is small, as is frequently the case with patients with low back pain, then Pennal and his colleagues admit that 'insufficient motion has occurred at the vertebral level being studied' and, as a consequence, 'the frame is difficult to read accurately'.
Method IV
The linear antero-posterior displacement method gave results shown in Columns IV of Tables 1,2 and 3. Clearly, that there were no false positives with this method indicates that this method ought to be the method of choice from the four selected for this report.
DISCUSSION
Flexion/extension radiography and discography may not necessarily demonstrate the same features. Flexion/extension radiography assesses dynamic per- formance whereas discography shows the morpho- logical state of the disc. However, we consider that it is not an unreasonable assumption to relate these two features. We support this statement by noting that, since the discogram demonstrates annular integrity, assuming that the annular damage is radial, one would expect a deterioration in the disc's kinetic characteristics (as shown by flexion/extension radio- graphy) to be associated with morphological degeneration (as shown by discography). The in vitro work of van Akkerveeken et al. (1979) supports this argument.
For flexion/extension radiography, there is a prob- lem of what constitutes normal movement. Ethical considerations preclude the taking of two lateral radiographs of the lumbar spine in normal, asympto- matic patients. We found it necessary, therefore, when analysing Method IV, to assume normal move- ment patterns and to assess abnormality against these assumptions. We postulated that normal movement was given by regular trends of motion along the spine, this principle having been previously described by Jirout (1957).
We must accept that it is not possible, either uniquely or precisely, to define any individual's movement in terms of its deviation from normal Also, it is not possible to be aware of the movement pattern of any individual prior to the onset of spinal discomfort.
Diagnostic procedures which produce a high incidence of false positive findings are, generally, of little value to the referring clinician. In our opinion, the first three methods of quantifying flexion and extension films fall into this category and will not be further considered. However, the fourth method, while generating false negatives, gave no false posi-

F L E X I O N AND E X T E N S I O N R A D I O G R A P H Y OF THE L U M B A R SPINE 4 0 9
tires in our series. Consequently, we consider that, of our four selected methods, this final method ought to be the method of choice.
Looking further into the results generated by Method 1V has revealed the following interesting points.
(1) The ability of the flexion/extension analysis to detect abnormalities is reduced as the number of discographically degenerate discs increases in any individual. Of those subjects whose discogram indi- cated a single level abnormality, all had this level singled out by the fiexion/extension analysis. (One ought to comment on the rather unlikely situation where a normal disc space has abnormal spaces immediately above and below it. We would be rather doubtful about any flexion and extension procedure being able to distinguish normal from abnormal in such cases. We did not have such an example in our series.)
(2) Increasing degeneracy on Erlacher's scale was associated with increasing agreement between the discographic appearances and this flexion/extension quantification procedure.
(3) The lower discs, generally, were more reliably assessed by the flexion/extension films. Of the disco- graphically degenerate discs, none (out of six) of the L2-L3 discs was also abnormal on the flexion/ extension analysis, whereas 25 (out of 28) of the LS-S1 discs were so identified. The extremely variable behaviour of the L1-L2 disc space in exten- sion accounts for some of the difficulty in diagnosing L2-L3 (and L1-L2) abnormalities from flexion/ extension radiography.
Turning away from the analysis of the results of Method IV, it is worth discussing the real value of flexion and extension radiography in clinical practice.
The use of a diagnostic procedure to select the level (or levels) showing a deviation from either normal morphology or normal behaviour does not necessarily imply that the origin of back pain will be identified. However, by definition, some form of abnormality must exist to account for the presence of pain.
The value of flexion/extension radiography in the management of orthopaedic patients needs to be con- sidered for two separate situations. Firstly, will a single set of flexion/extension radiographs aid the diagnosis of any particular patient? All discographic- ally single level abnormalities were correctly diagnosed by flexion/extension radiography using the principle of antero.posterior displacement assessment (Method IV). Nevertheless, the finding of a single level abnor- mality on flexion/extension radiography does not exclude the presence of another discographically abnormal level. Indeed, it might be that such a second
28
unsuspected level of abnormality is, in fact, the symptomatic level in such a patient. Observing the extremes of spinal movement of those patients whose flexion and extension characteristics are investigated on a single occasion can, thus, be confusing. Excep- tions to this are (1) that group of patients who show a grossly increased movement at a single level and (2) those patients whose dynamic characteristics of the lumbo-sacral spine are entirely normal. On certain occasions flexion/extension radiographs may demon- strate the presence of an otherwise unsuspected early spondylolisthesis (Troup, 1978).
Secondly, can one reasonably detect changes in disc performance in individuals from flexion/exten- sion radiographs on a serial basis? If, on the first visit of a patient with low back pain, the flexion/ extension radiographs are normal (and, in our experience, it is possible that a Group 3 disc lesion (Erlacher, 1952) may be missed), subsequent radio- graphs in flexion/extension some months later may demonstrate the abnormal level with the annular damage more advanced. Such supportive evidence might be most helpful.
On a serial basis, patients who have undergone spinal fusions can be followed for evidence of failure of the fusion or the premature failure of the disc immediately adjacent to the fusion.
The question of the radiation dosage to the patient is one which is always relevant to radio- diagnostic procedures. The decision to perform flexion/extension radiographs must be based on clinical judgement but we feel that the relatively high radiation dose associated with the taking of two lumbosacral radiographs is unacceptable unless there is a reasonable expectation of achieving an improvement in patient management. We suggest that this needs careful thought.
CONCLUSIONS
1. Flexion/extension radiography is likely to be con- fusing if only performed on a single occasion.
2. On a serial basis, this procedure may be more rewarding in ce/tain areas of patient management, such as the assessment of the stability of a spinal fusion.
3. If performed on a serial basis and if a quantifica- tion procedure is adopted, the actual construction technique used needs careful scrutiny. Our survey shows that the measurement of linear antero- posterior displacement may be the method of choice.
4. The radiation dose to the patient cannot be over- looked. We advise careful consideration of this matter by our clinical and radiological colleagues.

410 CLINICAL RADIOLOGY
Acknowledgements. We would like to thank the Back Research Unit, Harlow Wood Orthopaedic Hospital (Director: Mr R. C. Mulholland, FRCS), the X-ray Department, Harlow Wood Orthopaedic Hospital and the Medical Physics Depart- ment, Nottingham City Hospital (Head: Dr J. H. Todd). Dr P. Davies, Consultant Radiologist, Nottingham City Hospital gave helpful advice on the manuscript. Secretarial assistance was given by Mrs S. Jones, Mrs S. Blythe, Mrs J. Lawrenson and Mrs D. S. Willis.
REFERENCES
Bakke, S. N. (1931). RSntgenologische Beobachtungen fiber die Bewegungen der Wirbelsaule. Acta Radiologica Supple- mentum, 13, 1-75.
Begg, A. C. & Falconer, M. A. (1949). Plain radiography in intraspinal protrusion of lumbar intervertebral disks: a correlation with operative findings. British Journal of Surgery, 36, 225-239.
Erlacher, P. R. (1952). Nucleography. Journal o f Bone and Joint Surgery, 34B, 204-210.
Gianturco, C. (1944). A roentgen analysis of the motion of the lower lumbar vertebrae in normal individuals and in patients with low back pain. American Journal o f Roent- genology and Radium Therapy, 52, 261-268.
Ho, R. W. H. (1962). Testing intervertebral joint movement. Journal of the American Osteopathic Association, 61, 635-639.
Hoag, J. M., Kosok, M. & Moser, J. R. (1960). Kinematic analysis and classification of vertebral motion. Journal o f the American Osteopathic Association, 59, 899-908.
Israel, M. (1959). A quantitative method of estimating flexion and extension of the spine. Military Medicine, 124,181-186.
Jirout, J. (1957). The normal mobility of the lumbo-sacral spine. Acta Radiologica, 47, 345-348.
Knutsson, F. (1944). The instability associated with disk degeneration in the lumbar spine. Acta Radiologica, 25, 593-609.
Lindahl, D. (1966). Determination of the sagittal mobility of the lumbar spine. Acta Orthopaedica Scandinavica, 37, 241-254.
Melamed, A. & Ansfield, D. J. (1947). Posterior displacement of lumbar vertebrae. American Journal o f Roentgenology and Radium Therapy, 58, 307-328.
Morgan, F. P. & King, T. (1957). Primary instability of lumbar vertebrae as a common cause of low back pain. Journal o f Bone and Joint Surgery, 39B, 6-22 .
Park, W. M., McCall, I. W., O'Brien, J. P. & Webb, J. K. (1979). Fissuring of the posterior annulus fibrosus in the lumbar spine. British Journal o f Radiology, 52, 382-387.
Pennal, G. F., Corm, G. S., McDonald, G., Dale, G. & Garside, H. (1972). Motion studies of the lumbar spine. Journal o f Bone and Joint Surgery, 54B, 442-452.
QuinneU, R. C. & Stockdale, H. R. (1982). The significance of osteophytes on lumbar vertebral bodies in relation to discographic findings. Clinical Radiology, 33, 197-203.
Quinnell, R. C., Stockdale, H. R. & Harmon, B. (1980). Pressure standardized lumbar discography. British Journal o f Radiology, 53, 1031-1036.
Rosenberg, P. (1955). The R-Center method. A new method of analysing vertebral motion by X-rays. Journal o f the American Osteopathic Association, 55,103-111.
Tanz, S. S. (1953). Motion of the lumbar spine. American Journal o f Roentgenology, Radium Therapy and Nuclear Medicine, 69, 399-412.
Troup, J. D. G. (1978). Personal communication. van Akkerveeken, P. F., O'Brien, J. P. & Park, W. M. (1979).
Experimentally induced hypermobility in the lumbar spine. Spine, 4,236-241.
Wiles, P. (1935). Movements of the lumbar vertebrae during flexion and extension. Proceedings o f the Royal Society o f Meclicine, 28,647-651.
APPENDIX: MATHEMATICAL DESCRIPTION OF METHOD IV
FLEXION EXTENSION
1/2 L -Ve r teb ra l w~dth A= (x12+x2 2) Xl = Loos(@2)+d
d = Horlzonlal B = (X32 + X42 ~ X 2 = A 4- Lstn(e/2) d ~splacement
x 3 = A+ LsJn(e/2) A - Postenor disc
height ~ = Lcos(~/2)- d
. ' .A = [( Lcos(°/2)+d)2+iA+Lsln(@2))2] ~'2
. ' .B = [{ Lcosi°/2)-d)2+iA+LslniJa/2))2] 1/2
Fig. 3 - Mathematical description of relative vertebral movements during flexion and extension.

F L E X I O N AND E X T E N S I O N R A D I O G R A P H Y OF THE L U M B A R SPINE 411
¢ Measured D,sp~acemenl, D (cm) ( = 1 / 2 (A - Bl)
+o- D = d;~/~ A=lcm = 0 ° "/~'2"/ & ~ 2 c m
08- Z///~~ 06- 04-
02-
o d2 o'4 o'6 o'8 15 True Displacement , d ccml ..,,.
04-
¢ D (cm)
;o- D.=d~. / ~ = 1 0 ° / j A = l c m
08- / / ~ j A=2cm
06- / / ~ ~
/ / /
02-
o o'2 o'4 o'6 o'8 ;~ d (cm)
Fig. 4 Typical relationships between the calculated value of ½(A - B) and the true horizontal displacement, d. In both cases, L is taken to be 3.8 cm.
In general, each disc space can be represented as shown in Fig. 3. The normal erect position is given by the thin lines while the thick lines indicate the vertebral position in either complete flexion or extension.
Assuming a symmetrical layout of the vertebrae in the normal erect position and also considering only the horizontal component o f the vertebral displace- ment, then A and B can be calculated from the true displacement, d, by using the Pythagorean relation- ship for the lengths of the sides o f a right angled triangle. That is:
A 2 = [L cos (0/2) + d] 2 + [L sin (0/2) + A] 2
B 2 = [L cos (0/2) - d] 2 + [L sin (0/2) + A] 2
Therefore, ½ ( A - B) can be calculated. In the situation where the disc space is parallel-sided (i.e. 0 -+ 0°), then the equations reduce to:
A 2 = (L + d) 2 + A 2
B 2 = (L - d) 2 + A 2
In Fig. 4, we plot the value of ½ ( A - B) against the true horizontal displacement, d, for 0 = 0 ° and 0 = 10 °. The vertebral width, L, is taken as 3.8 cm in both cases.
½(A - B) is not exactly proportional to d but the extent o f departure is insignificant for our purposes.
The vertebral width, L, was defined by two parallel lines WX and YZ (Fig. 1) and was set at 3.8 cm for convenience, since this is the width of a commonly available transparent ruler.