Embed Size (px)
Citation preview
Florida Medicaid Reform
Rep. Gayle Harrell
Chair, Healthcare General Committee
2
Why Does Florida Need Medicaid Reform? Under traditional fee-for-service Medicaid consumers have few
choices – and few opportunities to participate in health care decisions.
Lack of access to specialists. The traditional program is complex and hard to manage.
– Florida operates 20 different “waiver” programs (examples include: Prepaid Mental Health, Healthy Start; and Prepaid Dental, etc.).
In addition, the state covers over 44 services We need to control the growth of expenditures – left unchecked by
Medicaid will make up 59% of the state’s total budget by the year 2015.
Fraud and abuse in the system We need a system that focuses on improving the health of
recipients, not just paying claims when people are sick.
3
Florida’s Medicaid Reform
Traditional Medicaid Florida’s New Medicaid
Government as consumer Patients as consumers
Complex programs Consistent policies
Government controls More consumer choice
Centralized planning/purchasing
Marketplace decision-making
Blank check Defined investment
Unsustainable growth Predictable growth
Key Elements of Medicaid Reform in Florida
5
Key Elements of Reform
Choice Counseling. Delivery System:
– Coordinated Systems of Care (HMOs and PSNs) New Options / Choice:
– Customized Plans.– Opt-Out.– Enhanced Benefits.
Financing Methodology:– Premium Based.– Risk-Adjusted Premium.– Comprehensive and Catastrophic Risk Models
Low Income Pool (LIP). Outreach Efforts.
Key Elements of Reform
Choice Counseling
7
Choice Counseling
Choice Counseling: A free Service to help beneficiaries understand their plan choices and make a choice that best fits their health care needs.
Certified Choice Counselors:– Florida has the only certification program in the nation.
Choice Counseling available: – In person, group and face-to-face counseling ~ Sessions located near residences of Medicaid
recipients.– In the communities.– Home visits available, if needed by the individual.– Tallahassee Choice Counseling Call Center: Available 8:00 a.m. to 7:00 p.m. Monday-Friday and 9:00
a.m. to 1:00 p.m. Saturdays. “Check It Out” outreach and media campaign:
– Enrollment packets sent to Medicaid beneficiaries.– Packets Contain information regarding covered services; co-payments, if applicable, from each plan;
hospital network contract with each plan; Extra services offered by each plan; 3-ways to enroll in a plan.– Plan information available by Internet (www.flmedicaidreform.com )– Each began July 24, 2006.
Helping Recipient make a choice ~ Provider search:– by PCP or Specialist;– Hospital;– Database Updated weekly.
Delivery System:
Coordinated Systems of Care
1. HMO’s
2. PSN’s
Key Elements of Reform
9
Types of Reform Plans:FFS vs. Capitated
Health Maintenance Organization (HMO) A Health Maintenance Organization (HMO) is an entity licensed under
Chapter 641, Florida Statutes. The Agency contracts with HMOs on prepaid a fixed monthly rate per member (e.g. capitation rate) for which the HMO assumes all risk for providing covered services to their enrollees.
Provider Service Network (PSN) Provider Service Network (PSN) is defined in 409.912, Florida Statutes
as a network established or organized and operated by a health care provider, or group of affiliated health care providers, which provides a substantial proportion of the health care items and services under a contract directly through the provider or group of affiliated providers.
Under Reform, PSN's may be reimbursed on a capitated or fee-for-service basis for up to three years.
The current number of the plans approved are as follows: Broward – 9 HMOs, 4 PSNs. Duval – 3 HMOs, 2 PSNs.
10
Reform Plans Per County as of September 1, 2006 13 Plans in Broward County:
– Access Health Solutions.– AMERIGROUP.– Buena Vista.– Florida NetPass.– HealthEase.– Humana.– Pediatric Associates.– Preferred Medical Plan.– South Florida Community Care Network.– Staywell.– Total Health Choice.– UnitedHealthcare.– Vista Healthplan of South Florida.
5 Plans in Duval County:– Access Health Solutions.– HealthEase.– Shands Jacksonville d/b/a First Coast Advantage.– UnitedHealthcare.– Staywell.

Key Elements of Reform
New Options:
1. Customized Benefits
(One Size Doesn’t Fit ALL!!)
12
Customized Plans
Variety of plan choices for beneficiaries – provides increased access to care – the ability to select a plan that best meets their needs.
All plans are required to cover prescription drugs All plans must meet standards that ensure they’re sufficient to meet
the needs of the population(s) they serve. All medically necessary services for children and pregnant women
will be provided.
13
Customized Benefits Packages
Plan Design Guidelines Flexibility in amount, scope and duration of services:
– Certain services must be provided at or above current coverage levels.
– Other services must be provided to meet state established sufficiency standards for the population.
– Remaining services must be offered, but amount, scope and duration are flexible.
14
Additional Servicesat Plan Option
Reform plans can enhance any service above current levels and can add services not currently covered.
New services the plans will offer include the following:– Over-the-counter medications (from $10-$25 per household,
per month).– Adult preventive dental.– Additional Adult Vision (up to $125 per year for upgrades).– Respite Care.– Home delivered meals (post surgical care).– Circumcisions for newborns.
Key Elements of Reform
New Options:
2. Opt Out
16
The Opt Out Program
Employed Medicaid recipients will be offered the choice to opt-out of Medicaid and direct the premium paid by Medicaid on their behalf to an employer-sponsored plan, towards payment for the employee’s share of that plans premium.
The Opt Out program will help bridge the gap to independence as Medicaid recipients who work now have a new option for health insurance.
The Opt Out Program is a completely voluntary program. The individual may opt out of Medicaid at any time to participate in their
employer sponsored program. An enrollee will have the option to reenroll in Medicaid at the time of their
Medicaid open enrollment period, their employer’s open enrollment period, or due to loss of their job.
The Agency has contracted with a vendor to administer the opt out program who will communicate directly with Medicaid recipients and employers to establish a process by which premium payments will be made.
17
Employers in the Opt Out Program
Major employers of Medicaid recipients have been identified.
The Agency worked with these employers requesting they partner with the Agency to help ensure a successful Opt Out Program.
Employers asked to accept premium payments on behalf of Opt Out enrolled individuals.
Employers asked to work with Medicaid recipients who are interested in Opt Out in answering questions regarding available insurance.
The Opt Out program has the potential to build stronger employer/employee relationships.
Key Elements of Reform
New Options:
3. Enhanced Benefits

19
Enhanced Benefits The goal of the Enhanced Benefits program is to promote self
involvement in one’s health care needs. Participation in healthy behaviors that have positive outcomes and
can improve one’s health status will be rewarded in the form of “credit dollars” that may be used to purchase health related products and supplies.
Beneficiaries may earn up to a maximum of $125 per year in “credit dollars.”
All recipients enrolled in a Medicaid Reform Health plan are eligible for the Enhanced Benefit program.
An account will be established for each recipient at the time of the first credit deposit in the account and account statements will be mailed to the recipient anytime activity occurs on the account (credits and debits).
Beneficiaries use their Medicaid card as a “debit card” at participating pharmacies to access funds.
20
Enhanced Benefits
The Enhanced Benefits program will be administered by the Agency, with cooperation with the health plans.
The health plans are required to submit a monthly report to the Agency identifying all members of the plan that met the criteria for a healthy behavior for the reporting period.
The reporting period is based on paid claims with corresponding procedure codes.
Once the report is received by the Agency, the process to credit the account begins.
Recipients will be able to contact the health plans and the State for detailed information on the program and accounts.
21
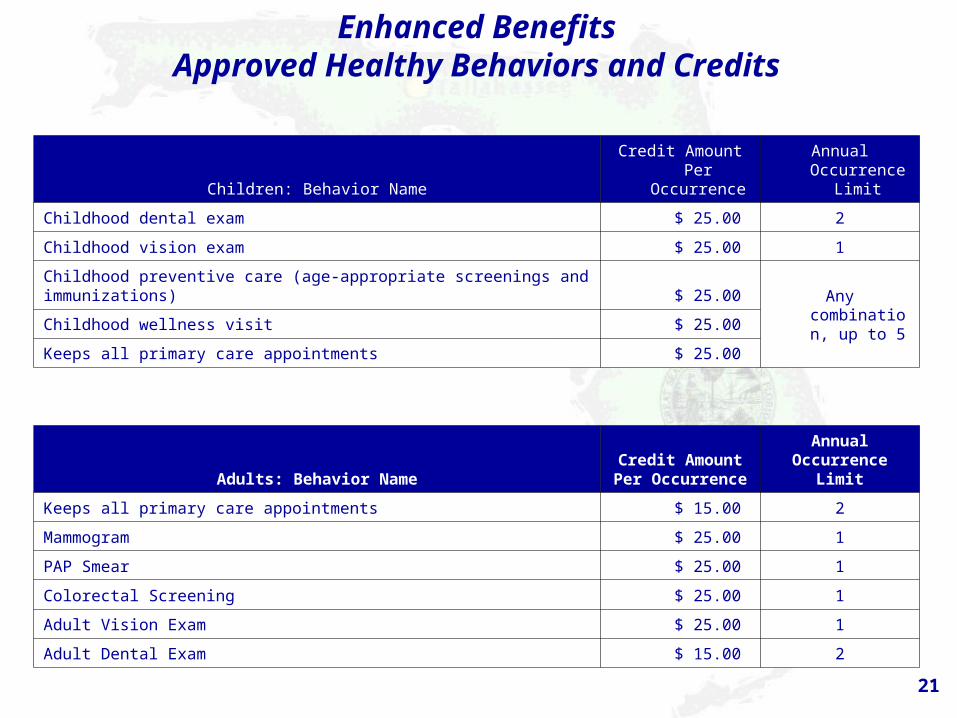
Enhanced BenefitsApproved Healthy Behaviors and Credits
Children: Behavior NameCredit Amount Per
OccurrenceAnnual Occurrence
Limit
Childhood dental exam $ 25.00 2
Childhood vision exam $ 25.00 1
Childhood preventive care (age-appropriate screenings and immunizations) $ 25.00 Any combination,
up to 5Childhood wellness visit $ 25.00
Keeps all primary care appointments $ 25.00
Adults: Behavior NameCredit Amount Per Occurrence
Annual Occurrence Limit
Keeps all primary care appointments $ 15.00 2
Mammogram $ 25.00 1
PAP Smear $ 25.00 1
Colorectal Screening $ 25.00 1
Adult Vision Exam $ 25.00 1
Adult Dental Exam $ 15.00 2
22
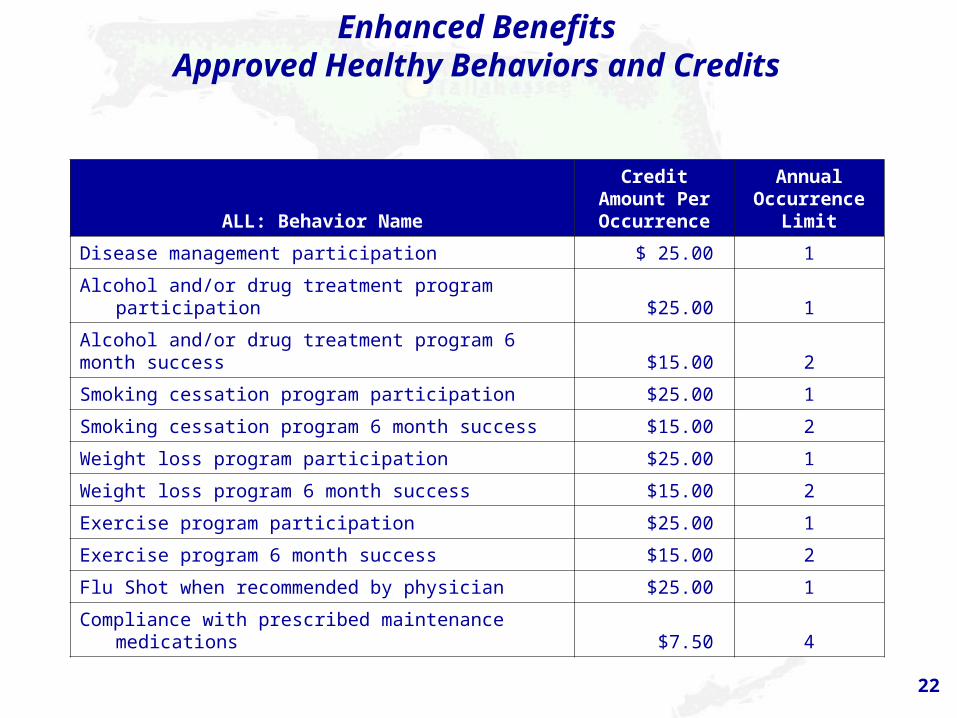
Enhanced BenefitsApproved Healthy Behaviors and Credits
ALL: Behavior NameCredit Amount Per Occurrence
Annual Occurrence
Limit
Disease management participation $ 25.00 1
Alcohol and/or drug treatment program participation $25.00 1
Alcohol and/or drug treatment program 6 month success $15.00 2
Smoking cessation program participation $25.00 1
Smoking cessation program 6 month success $15.00 2
Weight loss program participation $25.00 1
Weight loss program 6 month success $15.00 2
Exercise program participation $25.00 1
Exercise program 6 month success $15.00 2
Flu Shot when recommended by physician $25.00 1
Compliance with prescribed maintenance medications $7.50 4
Financing Methodology:
1. Premium Based Financing
2. Risk Adjusted Premiums
3. Comprehensive and Catastrophic Risk Models
Key Elements of Reform
24
1. Premium Based
Changes to the premium calculation along with the risk adjustment process allow for more accurate allocation of funds.
Plans that are paid fee-for-service (PSNs) will be monitored against the capitated premium as a benchmark.
The use of encounter data and full risk adjustment for premium calculation will be phased in over the next two to three years.
This transition will allow the state to more appropriately allocate funding to the plans.
25
2. Risk Adjustment
The Agency will risk adjust plan premiums in accordance with Florida Statute.
Risk Adjusted Rates:– Distributes capitation payments across health plans based on
the health risk of the members enrolled in each health plan. Risk Adjustment Process:
– Better matches payment to risk.– Pay for the risk enrolled.
The Agency will initially use Medicaid Rx model to risk adjust rates and will move to Chronic Illness and Disability Payment Systems (CDPS), diagnostic based risk adjustment model.
26
3. Comprehensive and Catastrophic Risk Models
HMO’s and PSN’s may limit risk under certain circumstances– All capitated PSNs and HMOs in areas where there has
been no managed care (rural counties) may limit their financial risk by electing to take financial responsibility only for the Comprehensive component.
• they get less premium, • the state acts as reinsurer for the Catastrophic
component. Why Introduce the Catastrophic Risk Model?
– To encourage new managed care entities to enter the market:
– To encourage managed care entities to participate in rural and medically underserved areas.

Key Elements of Reform
Low Income Pool
28
Low Income Pool (LIP)
Under Medicaid Reform, Upper Payment Limit (UPL) becomes the Low Income Pool.
Statute mandated the Low Income Pool be established to ensure continued government support for the provision of health care services to Medicaid, underinsured and uninsured populations. The low income pool consists of a capped annual allotment of $1 billion total computable for each year of the 5-year demonstration period. Roll over provision allows to exceed $1billion in a given year.
A Low Income Pool Council was created, per statute, to advise the Agency, the Governor and the Legislature on funding methodology and allocation of the LIP funds.
Low Income Pool funds will be allocated to hospitals serving a significant portion of Florida’s Medicaid, uninsured and underinsured populations.
Additional categories for distribution of LIP funds determined.
Key Elements of Reform
Outreach Efforts Prior to Implementation of Reform Pilot

30
Outreach to Beneficiaries,Advocates, Agencies, Local Officials, Community
Leaders
62 Meetings / Trainings held. Collaborative effort with advocacy groups to
provide materials/information to beneficiaries. One-on-one telephone and face-to-face assistance. Check It Out Campaign including the development and testing of
reform materials by beneficiaries, and distribution of reform brochure to 121,933 households.
Local Marketing/Outreach campaign activities conducted by Area Office staff and local marketing firm with brochures distributed at health fairs, public events, public transit sites, local businesses and local churches.
Advertisements placed on buses, in local newspapers and with local radio spots.
Reform Hotline and Medicaid Reform Website provided additional public access to information about Reform.
31
Outreach to Plans and Providers
Targeted outreach to potential health care plans, Medicaid providers, beneficiaries, advocates, agencies and elected officials/community leaders.
Announcements of public meetings broadcast in the Florida Administrative Weekly and to an interested parties list.
Technical Assistance Meetings held with focused topics to guide the plans through the Reform process.
Training sessions held, specific to provider audiences such as MediPass Providers; Pharmacy Providers, Behavioral Health Providers, and other Specialty Providers..
Articles Published in The Florida Medicaid Provider Bulletin.
32
Reform Timeline April – November 2004: Stakeholder meetings and Provider workshops held
seeking input from providers, beneficiaries, and advocates; evaluating potential options available to the state; identifying barriers to implementation, and proposing solutions.
May 6, 2005: Reform authorized by Florida Legislature in SB 838. August 31, 2005: Draft waiver request posted on AHCA website.
– Agency for Health Care Administration (Agency), the state Medicaid Agency, received comments on the draft.
– Agency reached agreement on Upper Payment Limit (UPL) program with Centers for Medicare and Medicaid Services (CMS).
October 3, 2005: Waiver request submitted to CMS, after 30-day posting. October 19, 2005: Waiver request approved by CMS. December 8, 2005: Approved by the Legislature. July 1, 2006: Choice counseling hotline available for recipients. September 1, 2006: Enrollment began for Duval and Broward Counties.
33
Reform Plan EnrollmentJuly 24 – September 26, 2006
Transition of existing 210,000 beneficiaries over 7 months.
Broward County Voluntary Enrollments and Plan Changes:– 15,403
Duval County Voluntary Enrollments and Plan Changes:– 9,638
Total Broward and Duval County : 25,041
34
Questions?















![Vol 63 - [Tom Harrell].pdf](https://img.pdfslide.net/doc/110x75/55cf8f6f550346703b9c5157/vol-63-tom-harrellpdf.jpg)













