Embed Size (px)
Citation preview

Fluid and Fluid and Electrolytes:Electrolytes:
TUSM III Pediatric TUSM III Pediatric Clerkship Lecture Clerkship Lecture
SeriesSeriesPaul D. Carlan, MDPaul D. Carlan, MDBaystate Medical CenterBaystate Medical Center
Departments of Pediatrics and Departments of Pediatrics and MedicineMedicine
April 16, 2004April 16, 2004

Parenteral Fluid TherapyParenteral Fluid Therapy
IVF is a basic component of the care IVF is a basic component of the care of hospitalized infants and childrenof hospitalized infants and children
Fluid and electrolyte problems can Fluid and electrolyte problems can be challenging, but can be “tamed” be challenging, but can be “tamed” by an organized approach by an organized approach
Useful to consider separately the Useful to consider separately the following questions:following questions: ““How much?” or volume and rateHow much?” or volume and rate ““What kind?” or electrolyte constitution What kind?” or electrolyte constitution

Parenteral Fluid TherapyParenteral Fluid Therapy
IVF therapy is IVF therapy is tailored to address tailored to address differing clinical differing clinical needsneeds MaintenanceMaintenance DeficitDeficit Ongoing lossesOngoing losses

Maintenance: FluidMaintenance: Fluid Metabolism creates two by-products which must be Metabolism creates two by-products which must be
actively eliminated to maintain homeostasisactively eliminated to maintain homeostasis Heat: dissipated by insensible losses from skin and lungHeat: dissipated by insensible losses from skin and lung Solute: waste products of metabolism excreted into the urineSolute: waste products of metabolism excreted into the urine

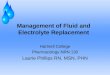
Maintenance: FluidMaintenance: Fluid Basal Metabolic Rate Basal Metabolic Rate
does not does not directly directly relate to body weightrelate to body weight BMR is much higher BMR is much higher
in the neonate than in the neonate than the adult and the the adult and the transition is not lineartransition is not linear
As a result, adults As a result, adults need need less less fluid and fluid and electrolytes than electrolytes than children per kg of children per kg of bodyweightbodyweight

Methods of Estimating Methods of Estimating Maintenance Fluids Maintenance Fluids
Methods of estimating basal or Methods of estimating basal or maintenance fluid requirementsmaintenance fluid requirements Basal Surface AreaBasal Surface Area
Need to know height and weight, requires table, Need to know height and weight, requires table, does not allow for deviations from normal activitydoes not allow for deviations from normal activity
Basal or Calorie Expenditure MethodBasal or Calorie Expenditure Method Requires a table, involves calculations, permits Requires a table, involves calculations, permits
correction for changes in activity or injury, “drier”correction for changes in activity or injury, “drier” Holliday-Segar SystemHolliday-Segar System
Easy to remember, does not require table or difficult Easy to remember, does not require table or difficult calculations, does not allow for deviations from calculations, does not allow for deviations from normal activitynormal activity


Holliday-Segar FormulaHolliday-Segar Formula
How does it work?How does it work? Estimates that 1 kcal of energy requires Estimates that 1 kcal of energy requires
1 cc of fluid to maintain homeostasis1 cc of fluid to maintain homeostasis Derives from fact that for each 100 kcal of Derives from fact that for each 100 kcal of
energy expended, 50 cc of fluid are lost energy expended, 50 cc of fluid are lost through the skin and airways, and 55 to 65 through the skin and airways, and 55 to 65 cc of fluid are required to generate an cc of fluid are required to generate an isosmotic urine (300 mOsm/L)isosmotic urine (300 mOsm/L)
Heat dissipation and solute excretion each Heat dissipation and solute excretion each represent roughly 50% of maintenance needsrepresent roughly 50% of maintenance needs
Anuric patients have one-half maintenance needsAnuric patients have one-half maintenance needs

Maintenance: Maintenance: ElectrolytesElectrolytes
No electrolytes are lost in sweat or No electrolytes are lost in sweat or exhaled water vapor; all electrolyte losses exhaled water vapor; all electrolyte losses are urinaryare urinary Thus, anuric patients have no maintenance Thus, anuric patients have no maintenance
sodium or potassium needssodium or potassium needs Since sodium Since sodium andand fluid requirements are fluid requirements are
based on BMR, the based on BMR, the ratioratio of electrolyte to of electrolyte to water is fixed and maintenance fluid water is fixed and maintenance fluid requirements are the same for requirements are the same for allall patients (regardless of age)patients (regardless of age) DD5 5 0.2 NS + 20 mEq/L of K+.0.2 NS + 20 mEq/L of K+.

Deficit: FluidDeficit: Fluid
Definition: Amount of fluid lost before Definition: Amount of fluid lost before treatment is beguntreatment is begun
One-time estimate; additional losses after One-time estimate; additional losses after therapy is begun are considered “on-going therapy is begun are considered “on-going losses”losses”
Methods:Methods: Preillness and current weight changePreillness and current weight change
Fluid deficit (L) = Preillness weight (kg) – current weight Fluid deficit (L) = Preillness weight (kg) – current weight (kg)(kg)
% Dehydration = (Fluid deficit (L)/Preillness weight % Dehydration = (Fluid deficit (L)/Preillness weight (kg))x100(kg))x100
Clinical estimates of weight lossClinical estimates of weight loss


Deficit: ElectrolytesDeficit: Electrolytes Sodium: usually in pediatrics, losses are Sodium: usually in pediatrics, losses are
gastrointestinal or due to a relatively short gastrointestinal or due to a relatively short period of decreased oral intakeperiod of decreased oral intake approximated by 0.45 NSapproximated by 0.45 NS
Potassium: deficit replacement is based on Potassium: deficit replacement is based on rate of safe replacement and not amount rate of safe replacement and not amount since danger of hyperkalemia is greater since danger of hyperkalemia is greater than hypokalemiathan hypokalemia Add 20 mEq potassium/L after UOP is Add 20 mEq potassium/L after UOP is
establishedestablished Potassium infusion rate should not exceed 1 Potassium infusion rate should not exceed 1
mEq/kg/hour unless in monitored settingmEq/kg/hour unless in monitored setting

Ongoing losses: Fluid and Ongoing losses: Fluid and ElectrolytesElectrolytes
Fluid: abnormal losses that occur after Fluid: abnormal losses that occur after the one-time determination of a deficitthe one-time determination of a deficit Diarrhea, vomiting, NG aspirates, polyuriaDiarrhea, vomiting, NG aspirates, polyuria Measured and replaced cc for ccMeasured and replaced cc for cc
Electrolytes:Electrolytes: Consult tables for electrolyte composition Consult tables for electrolyte composition
of on-going lossesof on-going losses GI losses = 0.45 NSGI losses = 0.45 NS Transudates = 0.9 NSTransudates = 0.9 NS Radiant losses = sodium freeRadiant losses = sodium free

Overview of Parenteral Overview of Parenteral Rehydration StrategyRehydration Strategy
Phase I (emergency): If the patient is Phase I (emergency): If the patient is hemodynamically unstable or in shock, “one or hemodynamically unstable or in shock, “one or more” boluses of 20 cc/kg isotonic fluid should more” boluses of 20 cc/kg isotonic fluid should be given in the first 30 minutesbe given in the first 30 minutes
Phase II (deficit, maintenance, ongoing fluid Phase II (deficit, maintenance, ongoing fluid replacement):replacement):
1.1. Calculate fluid deficitCalculate fluid deficit2.2. Calculate maintenance fluidCalculate maintenance fluid3.3. Give ½ of deficit therapy + maintenance over Give ½ of deficit therapy + maintenance over
first 8 hours and remainder of deficit + first 8 hours and remainder of deficit + maintenance over next 16 hoursmaintenance over next 16 hours
4.4. Adjust above based on consideration of Adjust above based on consideration of ongoing losses likely to be encounteredongoing losses likely to be encountered

Case 1Case 1 A 5 month male old infant is brought to A 5 month male old infant is brought to
your ER with 4 day history of vomiting, your ER with 4 day history of vomiting, diarrhea, and reduced oral intake. UOP is diarrhea, and reduced oral intake. UOP is markedly reduced. On exam, the infant is markedly reduced. On exam, the infant is fussy but consolable. He pushes you away fussy but consolable. He pushes you away when you try to examine him. Weight is 6.3 when you try to examine him. Weight is 6.3 kg (5-25kg (5-25thth %ile), BP is 90/55 (50 %ile), BP is 90/55 (50thth %ile), HR %ile), HR is 190 (>95is 190 (>95thth %ile). The fontanelle is slightly %ile). The fontanelle is slightly sunken and his skin turgor is diminished. sunken and his skin turgor is diminished. The cardiopulmonary, abdominal, and The cardiopulmonary, abdominal, and neurologic exams are normal. He has neurologic exams are normal. He has stopped vomiting but refuses to drink.stopped vomiting but refuses to drink.

Case 1: Solution ACase 1: Solution ACombined Deficit/MaintenanceCombined Deficit/Maintenance
Bolus: 140 cc (20 cc/kg) of NS given for Bolus: 140 cc (20 cc/kg) of NS given for hemodynamic instabilityhemodynamic instability
Deficit Fluid:Deficit Fluid: No preillness weight, so must estimateNo preillness weight, so must estimate
Oliguria, tachycardia, no shock Oliguria, tachycardia, no shock 10% dehydrated 10% dehydrated Deficit = 10% or 100 cc/kg x 7kg*= 700 ccDeficit = 10% or 100 cc/kg x 7kg*= 700 cc
Maintenance Fluid:Maintenance Fluid: Holliday-Segar: 4 cc/kg for first 10 kg = 7 kg x Holliday-Segar: 4 cc/kg for first 10 kg = 7 kg x
4 cc/kg = 28 cc/hr4 cc/kg = 28 cc/hr
*Note: Should use preillness weight to calculate deficit = (6.3 *Note: Should use preillness weight to calculate deficit = (6.3 kg x 100)/(100-10%) = 7 kgkg x 100)/(100-10%) = 7 kg

Case 1: Solution ACase 1: Solution A Combined Deficit/MaintenanceCombined Deficit/Maintenance
First 8 hours: First 8 hours: Maintenance:Maintenance:
28 cc/hr x 8 hours = 224 cc of D28 cc/hr x 8 hours = 224 cc of D5 5 0.2 NS + 20 0.2 NS + 20 mEq KCl/LmEq KCl/L
Half Deficit = 700/2 = 350 cc of 0.45 NSHalf Deficit = 700/2 = 350 cc of 0.45 NS Total Fluid = 574 cc/ 8 hour = 71.8 cc/hrTotal Fluid = 574 cc/ 8 hour = 71.8 cc/hr IVF: 75 cc/hr of DIVF: 75 cc/hr of D5 5 0.3 NS + 20 mEq 0.3 NS + 20 mEq
KCl/LKCl/L

Case 1: Solution ACase 1: Solution A Combined Deficit/MaintenanceCombined Deficit/Maintenance
Next 16 hours: Next 16 hours: Maintenance:Maintenance:
28 cc/hr x 16 hours = 448 cc of D28 cc/hr x 16 hours = 448 cc of D5 5 0.2 NS + 0.2 NS + 20 mEq KCl/L20 mEq KCl/L
Half Deficit = 700/2 = 350 cc of 0.45 NSHalf Deficit = 700/2 = 350 cc of 0.45 NS Total Fluid = 798 cc/ 16 hour = 49.9 Total Fluid = 798 cc/ 16 hour = 49.9
cc/hrcc/hr IVF: 50 cc/hr of DIVF: 50 cc/hr of D5 5 0.2 NS + 20 mEq 0.2 NS + 20 mEq
KCl/LKCl/L

Case 1: Solution BCase 1: Solution B Sequential Deficit/MaintenanceSequential Deficit/Maintenance
Bolus: 140 cc (20 cc/kg) of 0.9 NS Bolus: 140 cc (20 cc/kg) of 0.9 NS First 8 hours:First 8 hours:
Remainder of Deficit: 20 cc/kg bolus Remainder of Deficit: 20 cc/kg bolus represents 2% of body weight. Since infant represents 2% of body weight. Since infant was 10% dehydrated, the remainder of was 10% dehydrated, the remainder of deficit after the bolus is 8% (or 80 cc/kg). deficit after the bolus is 8% (or 80 cc/kg). This can be replaced over next 8 hours at This can be replaced over next 8 hours at 1%/hr.1%/hr.
1%/hr = 10 cc/kg/hr = 70 cc/hr 1%/hr = 10 cc/kg/hr = 70 cc/hr IVF (Deficit): DIVF (Deficit): D5 5 0.45 NS + 20 mEq/L KCl0.45 NS + 20 mEq/L KCl

Case 1: Solution BCase 1: Solution B Sequential Deficit/MaintenanceSequential Deficit/Maintenance
Next 16 hoursNext 16 hours Day’s worth of maintenance fluid is Day’s worth of maintenance fluid is
then provided in next 16 hoursthen provided in next 16 hours 4 cc/kg/hr x 7 kg x 24 hours = 672 cc 4 cc/kg/hr x 7 kg x 24 hours = 672 cc
FluidFluid 672 cc/16 hours = 42 cc/hr672 cc/16 hours = 42 cc/hr IVF (Maintenance): DIVF (Maintenance): D5 5 0.2 NS + 20 0.2 NS + 20
mEq/L KClmEq/L KCl


Monitoring Effectiveness of Monitoring Effectiveness of Parenteral TherapyParenteral Therapy

Oral Rehydration Oral Rehydration TherapyTherapy
Indications: mild to moderate dehydrationIndications: mild to moderate dehydration Contraindications: shock, severe Contraindications: shock, severe
dehydration, intractable vomiting, coma, dehydration, intractable vomiting, coma, gastric distensiongastric distension
Method: give 5-10 cc or ORT q 5-10 minutesMethod: give 5-10 cc or ORT q 5-10 minutes Fluids: Cerealyte, Pedialyte, Naturalyte, Fluids: Cerealyte, Pedialyte, Naturalyte,
Rehydralyte, WHO/UNICEF ORSRehydralyte, WHO/UNICEF ORS Avoid soda, juice, gatorade, jelloAvoid soda, juice, gatorade, jello
Lack sufficient sodium and potassium, are often Lack sufficient sodium and potassium, are often hyperosmolar, can perpetuate diarrheahyperosmolar, can perpetuate diarrhea

Disorders of SodiumDisorders of Sodium
Serum Sodium = Osmolality = WaterSerum Sodium = Osmolality = Water Regulated by thirst , ADH, & renal water Regulated by thirst , ADH, & renal water
handlinghandling A disruption in A disruption in water balancewater balance is manifested as is manifested as
an abnormality in an abnormality in serum sodiumserum sodium Sodium is a functionally impermeable solute, Sodium is a functionally impermeable solute,
so it contributes to tonicity and induces water so it contributes to tonicity and induces water movement across membranesmovement across membranes Hypernatremia = hyperosmolar (hypertonic) Hypernatremia = hyperosmolar (hypertonic)
dehydrationdehydration Hyponatremia = hyposmolar (hypotonic) Hyponatremia = hyposmolar (hypotonic)
dehydrationdehydration

Hypernatremia = Hypernatremia = Serum Sodium > Serum Sodium > 145 mmol/L145 mmol/L
Hypernatremia Hypernatremia represents a deficit represents a deficit of water in relation of water in relation to the body’s sodium to the body’s sodium storesstores Net water loss Net water loss
CommonCommon Hypertonic sodium Hypertonic sodium
gaingain UncommonUncommon Usually iatrogenicUsually iatrogenic

Hypernatremia: Clinical Hypernatremia: Clinical ManifestationsManifestations
Related to CNS dysfunction; sequelae Related to CNS dysfunction; sequelae are prominent when the increase in are prominent when the increase in serum sodium is rapid or largeserum sodium is rapid or large
Affects the very young or very oldAffects the very young or very old Infants: hyperpnea, muscle weakness, Infants: hyperpnea, muscle weakness,
restlessness, high-pitched cry, restlessness, high-pitched cry, insomnia, lethargy, or coma. Seizures insomnia, lethargy, or coma. Seizures are uncommon.are uncommon.
Elderly: often asymptomatic until Na > Elderly: often asymptomatic until Na > 160160


Hypernatremia: Hypernatremia: ManagementManagement
ApproachApproach Identify CauseIdentify Cause Correct HypertonicityCorrect Hypertonicity
Rapid CorrectionRapid Correction Improves prognosis in patients in whom Improves prognosis in patients in whom
hypernatremia developed acutely hypernatremia developed acutely (sodium loading)(sodium loading)
Correct serum sodium by up to 1 Correct serum sodium by up to 1 mmol/L/hrmmol/L/hr

Hypernatremia: Hypernatremia: ManagementManagement
Slow CorrectionSlow Correction Prudent in patients with hypernatremia of longer or Prudent in patients with hypernatremia of longer or
unknown durationunknown duration Correct sodium by 0.5 mmol/L/hr or 10 mmol/d with Correct sodium by 0.5 mmol/L/hr or 10 mmol/d with
goal of 145 mmol/Lgoal of 145 mmol/L Others suggest adding the calculated fluidOthers suggest adding the calculated fluid deficit to deficit to
maintenance fluid requirements and giving over 48 hoursmaintenance fluid requirements and giving over 48 hours IVFIVF
Only hypotonic fluids are appropriate unless frank Only hypotonic fluids are appropriate unless frank circulatory collapse existscirculatory collapse exists
The more hypotonic the infusate, the lower the The more hypotonic the infusate, the lower the required volume to correct the hypertonicity, and required volume to correct the hypertonicity, and the lower the risk of cerebral edemathe lower the risk of cerebral edema

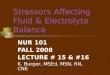
Hypernatremia: Hypernatremia: ManagementManagement
Rate of infusion is Rate of infusion is calculated using the calculated using the Madias FormulaMadias Formula which which estimates the change in estimates the change in serum sodium caused by serum sodium caused by 1 liter of any infusate. 1 liter of any infusate. The required volume, The required volume, and thus rate, is and thus rate, is determined by dividing determined by dividing the change in serum the change in serum sodium desired for a sodium desired for a given period of time by given period of time by the value obtained from the value obtained from Madias formula.Madias formula.

Case 2Case 2
A 1 week old female neonate is admitted to A 1 week old female neonate is admitted to the PICU after increasing lethargy and the PICU after increasing lethargy and difficulty with breastfeeding. Her difficulty with breastfeeding. Her birthweight was 3.8 kg. Her admission birthweight was 3.8 kg. Her admission weight is 3.3 kg. On exam, the infant is weight is 3.3 kg. On exam, the infant is difficult to arouse. BP is 72/62 (75difficult to arouse. BP is 72/62 (75thth %ile), %ile), HR is 120 (50HR is 120 (50thth %ile), RR is increased at 60. %ile), RR is increased at 60. The PE is unrevealing except for hypotonia The PE is unrevealing except for hypotonia and decreased level of consciousness. The and decreased level of consciousness. The nurse informs you the sodium is 165 nurse informs you the sodium is 165 mmol/liter.mmol/liter.

Case 2: Solution ACase 2: Solution A Bolus?: noBolus?: no Deficit Fluid:Deficit Fluid:
Deficit = 3.8 kg – 3.3 kg = 0.5 kg or 500 ccDeficit = 3.8 kg – 3.3 kg = 0.5 kg or 500 cc Maintenance Fluid:Maintenance Fluid:
Holliday-Segar: 4 cc/kg for first 10 kg: 3.8 kg x 4 cc/kg Holliday-Segar: 4 cc/kg for first 10 kg: 3.8 kg x 4 cc/kg = 15.2 cc/hr = 15.2 cc/hr
48 hours needs: 48 hours needs: Deficit = 500 cc of 0.45 NSDeficit = 500 cc of 0.45 NS Maintenance = 15 cc/hr x 48 hr = 720 cc of DMaintenance = 15 cc/hr x 48 hr = 720 cc of D5 5 0.2 NS + 0.2 NS +
20 mEq KCl/L20 mEq KCl/L Total Fluid = 500 cc + 720 CC = 1200 cc/ 48 hour = 25 Total Fluid = 500 cc + 720 CC = 1200 cc/ 48 hour = 25
cc/hcc/h IVF: 25 cc/hr of DIVF: 25 cc/hr of D5 5 0.3 NS + 20 mEq KCl/L0.3 NS + 20 mEq KCl/L

Case 2: Solution BCase 2: Solution B Deficit (Madias Formula)Deficit (Madias Formula)
TBW: (0.8 x 3.8kg) = 3 LTBW: (0.8 x 3.8kg) = 3 L Retention of 1 L of 0.2 NS will reduce the serum sodium Retention of 1 L of 0.2 NS will reduce the serum sodium
by 40 ([34-195]/[3+1])by 40 ([34-195]/[3+1]) The goal of therapy is to reduce the serum sodium by The goal of therapy is to reduce the serum sodium by
20 mmol/L in 48 hours. Therefore, 20/40 is 0.5 L or 500 20 mmol/L in 48 hours. Therefore, 20/40 is 0.5 L or 500 cc of fluid is required.cc of fluid is required.
48 hour needs:48 hour needs: Deficit = 500 cc of DDeficit = 500 cc of D55 0.2 NS 0.2 NS Maintenance = 3.8 kg x 4 cc/kg = 15.2 cc/hr x 48 hr = Maintenance = 3.8 kg x 4 cc/kg = 15.2 cc/hr x 48 hr =
720 cc of D720 cc of D5 5 0.2 NS + 20 mEq KCl/L0.2 NS + 20 mEq KCl/L Total Fluid = 500 cc + 720 CC = 1200 cc/ 48 hour = 25 Total Fluid = 500 cc + 720 CC = 1200 cc/ 48 hour = 25
cc/hcc/h IVF: 25 cc/hr of DIVF: 25 cc/hr of D5 5 0.2 NS + 20 mEq KCl/L0.2 NS + 20 mEq KCl/L


HyponatremiaHyponatremia
Serum Sodium < 136 mmol/LSerum Sodium < 136 mmol/L Hypotonic hyponatremia results Hypotonic hyponatremia results
from an excess of water in relation from an excess of water in relation to existing sodium stores, which can to existing sodium stores, which can be decreased, normal, or increased.be decreased, normal, or increased. Impaired renal water excretionImpaired renal water excretion
commoncommon Excess water intakeExcess water intake
uncommonuncommon

Adults: thiazide Adults: thiazide diuretics, SIADH, diuretics, SIADH, polydipsia, and polydipsia, and TURPTURP
Children: GI fluid Children: GI fluid loss, ingestion of loss, ingestion of dilute formula, dilute formula, accidental accidental ingestion of water, ingestion of water, and multiple tap and multiple tap water enemas.water enemas.

Hyponatremia: Clinical Hyponatremia: Clinical ManifestationsManifestations
Related to CNS dysfunction; sequelae Related to CNS dysfunction; sequelae are prominent when the decrease in are prominent when the decrease in serum sodium is rapid or largeserum sodium is rapid or large
Symptoms: Headache, nausea, Symptoms: Headache, nausea, vomiting, muscle cramps, lethargy, vomiting, muscle cramps, lethargy, restlessness, disorientation, and restlessness, disorientation, and depressed reflexesdepressed reflexes
If Na < 125 mmol/L: seizure, coma, If Na < 125 mmol/L: seizure, coma, brain damage, herniation, and deathbrain damage, herniation, and death


Hyponatremia: Hyponatremia: ManagementManagement
Symptomatic: Hypertonic saline Symptomatic: Hypertonic saline therapy (can be combined with therapy (can be combined with furosemide to limit expansion of ECF)furosemide to limit expansion of ECF) Correct 1-2 mmol/L/hour x several hours Correct 1-2 mmol/L/hour x several hours
if severly symptomaticif severly symptomatic Target for increase in serum sodium of Target for increase in serum sodium of
no more than 8 mmol/d to prevent no more than 8 mmol/d to prevent osmotic demyelinationosmotic demyelination
Asymptomatic: Fluid therapy is Asymptomatic: Fluid therapy is guided by Madias Formula guided by Madias Formula

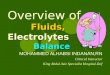
Hyponatremia: Hyponatremia: ManagementManagement
Rate of infusion is Rate of infusion is calculated using the calculated using the Madias FormulaMadias Formula which which estimates the change in estimates the change in serum sodium caused by serum sodium caused by 1 liter of any infusate. 1 liter of any infusate. The required volume, The required volume, and thus rate, is and thus rate, is determined by dividing determined by dividing the change in serum the change in serum sodium desired for a sodium desired for a given period of time by given period of time by the value obtained from the value obtained from Madias formula.Madias formula.

Case 3Case 3
A 12 year old male is found unresponsive at A 12 year old male is found unresponsive at the bottom of a swimming pool. He is the bottom of a swimming pool. He is resuscitated in the field and on arrival to the resuscitated in the field and on arrival to the ER is intubated and ventilated but has a ER is intubated and ventilated but has a spontaneous pulse. In the trauma room, he spontaneous pulse. In the trauma room, he develops generalized tonic-clonic seizures. develops generalized tonic-clonic seizures. He is loaded with phenytoin. His stat sodium He is loaded with phenytoin. His stat sodium then returns at 110 mmol/L. His weight is then returns at 110 mmol/L. His weight is 45 kg, BP is 100/70 (normal), HR is 100 45 kg, BP is 100/70 (normal), HR is 100 (normal). On exam, he is unresponsive and (normal). On exam, he is unresponsive and his right pupil is sluggish. his right pupil is sluggish.

Case 1: SolutionCase 1: Solution
Initial management is to prevent cerebral Initial management is to prevent cerebral edema and herniation; TBW: 0.6 x 45 kg = 27 edema and herniation; TBW: 0.6 x 45 kg = 27 LL
Madias Formula: Retention of 1 L of 3% NS Madias Formula: Retention of 1 L of 3% NS will increase the serum sodium by 14.4 mmol will increase the serum sodium by 14.4 mmol ([513-110])/([27+1])([513-110])/([27+1])
The goal of therapy is to increase the serum The goal of therapy is to increase the serum sodium by 5 mmol/L in 3 hours. Therefore, sodium by 5 mmol/L in 3 hours. Therefore, 5/14 = 350 cc of fluid is required.5/14 = 350 cc of fluid is required.
IVF: 350 cc/3 hr = 120 cc/hr of 3% NS x 3 IVF: 350 cc/3 hr = 120 cc/hr of 3% NS x 3 hours. hours.

ReferencesReferences
Adrogue, HJ and NE Madias. Hypernatremia. New England Adrogue, HJ and NE Madias. Hypernatremia. New England Journal of Medicine. 2000; 342(20): 1493-1499.Journal of Medicine. 2000; 342(20): 1493-1499.
Adrogue, HJ and NE Madias. Hyponatremia. New England Adrogue, HJ and NE Madias. Hyponatremia. New England Journal of Medicine. 2000; 342(21): 1581-1589.Journal of Medicine. 2000; 342(21): 1581-1589.
Choukair, MK. Fluids and Electrolytes. In: Siberry GK and R. Choukair, MK. Fluids and Electrolytes. In: Siberry GK and R. Iannone, ed. The Harriet Lane Handbook. 15Iannone, ed. The Harriet Lane Handbook. 15thth ed. St. ed. St. Louis, MO: Mosby; 2000: 229-240.Louis, MO: Mosby; 2000: 229-240.
Roberts, KB. Fluid and Electrolytes: Parenteral Fluid Roberts, KB. Fluid and Electrolytes: Parenteral Fluid
Therapy. Pediatrics in Review. 2001; 22(11): 380-387Therapy. Pediatrics in Review. 2001; 22(11): 380-387..