Embed Size (px)
Citation preview

ARTICLE IN PRESS+ModelEPIRES-4973; No. of Pages 5
Epilepsy Research (2013) xxx, xxx—xxx
jo ur nal ho me p ag e: www.elsev ier .com/ locate /ep i lepsyres
SHORT COMMUNICATION
Focal cortical dysplasia type IIIc associateswith multiple cerebral cavernomas
Pitt Niehusmanna,∗, Albert J. Beckera, Michael P. Malterb,Anna Raabeb, Azize Boströmc, Christian von der Breliec
a Dept. of Neuropathology, University of Bonn Medical Center, Bonn, Germanyb Dept. of Epileptology, University of Bonn Medical Center, Bonn, Germanyc Dept. of Neurosurgery, University of Bonn Medical Center, Bonn, Germany
Received 8 May 2013 ; received in revised form 25 June 2013; accepted 26 July 2013
KEYWORDSEpilepsy;Vascularmalformation;Surgery;Neuropathology
Summary The distinction of isolated malformations and combined lesions constitutes a majornovelty in the 2011 consensus classification of the International League against Epilepsy (ILAE)for focal cortical dysplasias (FCD). Cortical lamination abnormalities together with vascularlesions are subsumed as FCD IIIc. Little is known regarding frequency and etiology of this entity.Here, we systematically evaluated biopsy specimens from 72 drug-refractory epilepsy patientswith cerebral cavernous malformations (CCM) regarding presence of associated FCD. Due to anon-perpendicular orientation of the cortical structures or absence of sufficient cortical tissue
adjacent to the vascular lesion 25 samples were not classifiable. In the remaining 47 cases FCDIIIc was rare (4.3%), but significantly increased in patients with multiple CCM (28.6%; p < 0.05 vs.single CCM). Association of FCD IIIc with multiple CCM may argue against FCD IIIc as an acquiredlesion.© 2013 Elsevier B.V. All rights reserved.cate
Introduction
Recently, a new three tired classification of the InternationalLeague Against Epilepsy (ILAE) for focal cortical dysplasia
Please cite this article in press as: Niehusmann, P., et al., Fcerebral cavernomas. Epilepsy Res. (2013), http://dx.doi.org/
(FCD) was introduced (Blumcke et al., 2011). Type I andtype II FCD of the new classification largely reflect previoussystematics (Palmini et al., 2004). A new third class of FCD
∗ Corresponding author at: Dept. of Neuropathology, University ofBonn Medical Center, Sigmund-Freud-Str. 25, 53105 Bonn, Germany.Tel.: +49 228 287 13492; fax: +49 228 287 14331.
E-mail address: [email protected] (P. Niehusmann).
ieItesF2w
0920-1211/$ — see front matter © 2013 Elsevier B.V. All rights reserved.http://dx.doi.org/10.1016/j.eplepsyres.2013.07.006
omprises combinations of cortical lamination abnormalitiesnd hippocampal sclerosis (FCD IIIa), epilepsy-associatedumors (FCD IIIb), vascular malformations (FCD IIIc) or otherpileptogenic lesions obtained in early life (i.e., traumaticnjury, ischemic injury or encephalitis; FCD IIId). The authorsmphasize that the etiology and pathogenesis of the FCDsII remain enigmatic, but speculate that in these conditionshe FCD is most likely acquired and should not be consid-red as ‘‘dual pathology’’ (Blumcke et al., 2011). Several
ocal cortical dysplasia type IIIc associates with multiple10.1016/j.eplepsyres.2013.07.006
tudies raised the coexistence of hippocampal sclerosis andCD (Garbelli et al., 2006; Thom et al., 2009; Marucci et al.,012). In contrast, occurrence of FCD in epileptic patientsith vascular lesions is mainly described in case reports

IN PRESS+ModelE
2 P. Niehusmann et al.
(ob2
sr
M
P
Owe(wusI
i
Ucvtstiaf
N
SalnfiatsN&mm
S
FPC
Table 1 Number of patients, classifiable cases and diagno-sis of FCD IIIc.
Group Patients Classifiablecases
Diagnosis ofFCD IIIc
Single CCM 59 40 0Multiple CCM 13 7 2
R
Wardufccaw6trb
((F(tv
f8an
D
AprsSbcpEsdffll
ARTICLEPIRES-4973; No. of Pages 5
Giulioni et al., 2007; Maciunas et al., 2010). A recent seriesf 18 patients reported a high association of epilepsy, cere-ral cavernous malformations (CCM) and FCD (Chen et al.,013).
Here we re-evaluated the biopsy specimens from a largeeries of 72 drug-refractory epilepsy patients with CCM withespect to the presence of FCD IIIc.
aterial and methods
atients
n the basis of a recently published series of 1721 patientsith resective epilepsy surgery for drug-refractory focalpilepsy at Bonn Epilepsy Center between 1988 and 2009Bien et al., 2013), we re-evaluated all operated casesith histopathological diagnosis of CCM (n = 84). All patientsnderwent detailed epileptological evaluation assessingeizure semiology, MRI findings and video-EEG monitoring.nvasive monitoring was carried out in two constellations:
i. If clinical or imaging findings and electrophysiologicalmonitoring revealed incongruent results
i. If the lesion was located in or close to eloquent brainareas so that functional mapping should distinguishbetween lesional epileptogenic zone and functional area
sing neuroradiological and, if available, histopathologi-al data patients were subdivided for presence of singleersus multiple CCM. Twelve patients were excluded fromhe study due to insufficient MR-images. Ascertainment ofeizure outcome was performed at standardized postopera-ive checkups within the Bonn Neuro-Center and telephonenterviews. Patients with absence of all seizures includinguras within the last two years were considered as seizureree (i.e. Engel Class 1A; Engel et al., 1993).
europathology
urgical specimens were fixed in formaldehyde overnightnd embedded into paraffin. Macroscopic and histopatho-ogical examinations were performed by experiencedeuropathologists at the University of Bonn (AB, PN). Classi-ability and classification of histopathological specimen wasssessed independently by both neuropathologists. Estima-ion differed only in single cases regarding classifiability. Inuch cases the specimens were categorized as unclassifiable.europathological stainings comprised at least hematoxilin
eosin, Prussian blue and Elastica-van-Gieson for assess-ent of CCM and NeuN-immunohistochemistry (monoclonalouse, Millipore, USA) for evaluation of FCD.
tatistical analyses
Please cite this article in press as: Niehusmann, P., et al., Fcerebral cavernomas. Epilepsy Res. (2013), http://dx.doi.org/
isher 2-sided exact test was performed using GraphPadrism version 6.01 for Windows, GraphPad Software, La Jollaalifornia USA. P < 0.05 was considered significant.
mcti
Overall 72 47 2
esults
e identified 72 patients with concordant radiologicalnd neuropathological diagnosis of CCM who underwentesective epilepsy surgery between 1988 and 2009 forrug-refractory epilepsy (see Table 1). 19 Patients (26.4%)nderwent invasive monitoring. 13 Patients (18.1%) sufferedrom multiple CCM. Overall 25 samples (34.7%) were notlassifiable due to a non-perpendicular orientation of theortical structures or absence of sufficient cortical tissuedjacent to the vascular lesion. This includes 19 samplesith single CCM (32.2% of all patients with single CCM) and
cases with multiple CCM (46.1% of all cases with mul-iple CCM). However, no statistically significant differenceegarding the number of classifiable cases was observedetween both groups (p > 0.05).
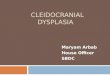
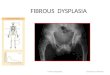
Only in two cases we identified unequivocal FCD IIIcFig. 1). Both patients showed multiple CCM on MR-imagesFig. 2). Thus in the overall cohort of 47 classifiable patientsCD IIIc is a rare finding (4.3%). However, 2 out of 7 patients28.6%) with multiple CCM and sufficient adjacent corticalissue for classification were diagnosed with FCD IIIc (p < 0.05s. single CCM).
Sufficient data regarding seizure outcome were availablerom 70 patients (97%). Seizure freedom was achieved in4.7% and did not significantly differ between classifiablend unclassifiable cases (p > 0.05). Both patients with diag-osis of FCD IIIc are seizure free since surgery.
iscussion
ssessment of cortical lamination adjacent to the CCM wasossible in 65.3% of specimens. In the remaining cases noeliable classification could be established, due to smallpecimen size or tangential gaiting of the cortical structures.everal reasons may be responsible for the relative low num-er of classifiable cases. The applied surgical technique washosen according to the preoperative clinical and electro-hysiological data which delineated the epileptogenic zone.xtent of resection at least included the CCM itself and theurrounding hemosiderotic rim (lesionectomy). Patients withrug-refractory epilepsy associated with CCM might profitrom extended lesionectomy to reach postoperative seizurereedom (Raabe et al., 2012). Nevertheless, performingesionectomy results in smaller biopsy specimens, oftenacking cortical tissue. The different extent of resection
ocal cortical dysplasia type IIIc associates with multiple10.1016/j.eplepsyres.2013.07.006
ight contribute to the relative high percentage (34.7%) ofases, which are not histopathologically classifiable. Addi-ionally, en bloc resection was not routinely performedn epilepsy surgery for CCM over the last two decades.

ARTICLE IN PRESS+ModelEPIRES-4973; No. of Pages 5
FCD IIIc in CCM 3
Figure 1 Histopathologic findings in vascular malformations associated with focal cortical dysplasia type IIIc. (A) H&E stainingshows a right temporo-polar cavernous malformation characterized by dilated, endothelium-lined blood vessels without arterialfeatures. Strong hyalinization of the vessel walls can be observed. Multiple cavernous malformations were found in this patient(see Fig. 2). (B) Labeling of neuronal cell bodies using antibodies against NeuN reveals abnormal radial cortical lamination adjacentto the vascular malformation. High magnification (inset in B) shows formation of microcolumns (black arrowhead) and cellular
yer
eetpiscwaiobm
pbwh(tha
abnormalities such as hypertrophic pyramidal neurons outside lain B = 50 �m.
Correct orientation of such biopsy samples is challenging andmay complicate assessment of FCD IIIc. These findings indi-cate the need to optimize intraoperative and postoperativehandling of biopsy specimens in surgery due to CCM asso-ciated epilepsy. In addition, abundant hemosiderin depositsare often observed in CCM and further complicate the eval-uation of the cortical lamination.
A recently published series from the Cleveland Clinic sup-ports this aspect (Chen et al., 2013). Chen and co-workersidentified in a collective of 146 patients, which were diag-nosed with CCM on biopsy specimens from 1989 to 2011 only18 cases with epilepsy and ample tissue for assessment ofFCD. However, the number of patients with epilepsy withinthe whole cohort of patients with neuropathological diagno-sis of CCM is not given in this publication.
Overall, coexistence of focal cortical dysplasia and CCMwas rare in our series with only two cases out of 47 clas-sifiable specimens (4.3%). Unclassifiable cases were notassociated with a poor seizure outcome, arguing against thepresence of epileptogenic foci missed by surgery. Intrigu-ingly, both patients with diagnosis of FCD IIIc suffered frommultiple CCMs, whereas no patient with single CCM showed
Please cite this article in press as: Niehusmann, P., et al., Fcerebral cavernomas. Epilepsy Res. (2013), http://dx.doi.org/
an associated FCD. Thus, within the collective of patientswith multiple CCMs FCD IIIc was diagnosed in more than28% of the classifiable cases. Presence of multiple CCMsstrongly indicates a genetic origin of the disease (Batra
enr
5 (white arrowhead). Scale bars: A = 500 �m, B = 200 �m, insert
t al., 2009). In addition, associated lesions of the CNS andxtracranial anomalies are frequent in patients with mul-iple CCMs (Ardeshiri et al., 2008). Regarding etiology andathogenesis of FCD IIIc, the exclusive observation of per-lesional dyslamination in patients with multiple CCM in ourtudy may therefore argue against FCD as an acquired pro-ess. However, particularly the number of classifiable casesith multiple CCM in our study is small and larger seriesre necessary to further analyze this aspect. In addition,t has to be emphasized that FCD Type IIIc is not referrednly to cortical lamination abnormalities adjacent to CCMut also to other vascular abnormalities, e.g. arteriovenousalformations and telangiectasias.However, an association of FCD IIIc with more complex
resentation than ‘only’ single CCM has also been reportedy others. In a recently published series Maciunas and co-orkers identified in two out of seven epilepsy patients withistopathological confirmation of a CCM coexistence of a FCDMaciunas et al., 2010). Interestingly, both patients had ahird cerebral lesion. One patient suffered from additionalippocampal sclerosis, the other had an additional venousngioma.
ocal cortical dysplasia type IIIc associates with multiple10.1016/j.eplepsyres.2013.07.006
A recently published study focused on the four param-ters cortical thickness, neuronal cell density, shortesteuronal diameter and diameter of neuronal nucleuseported significant alterations among the FCD III types

ARTICLE IN PRESS+ModelEPIRES-4973; No. of Pages 5
4 P. Niehusmann et al.
Figure 2 MRI findings in a patient with multiple cerebral cavernous malformations and FCD IIIc. This patient suffered from complexpartial seizures with secondary generalization for 6 years. Axial MRI T2 image shows a CCM in the right temporopolar region withmixed intense core signal and typical hypointense hemosiderotic rim (A). Preoperative workup revealed this CCM as to be potentiallyepileptogenic. Cranial MR imaging showed three other CCM, two of which were located supratentorial in the right frontal lobe asdepicted in the axial T2 weighted MR imaging (B) and (C). Another CCM was located in the right cerebellar hemisphere (not shown).F
o(ccla
icisTTIalgssnispaont
bCiio
D
Mrfatew
A
O(f
CD IIIc was not identifiable on MR imaging
nly in the group associated with vascular malformationsMuhlebner et al., 2012). This also may indicate a spe-ial position of FCD associated with vascular lesions inomparison to the other FCD III types. However, only aimited number of FCD III cases were included in thenalysis.
Our findings of only rare coexistence of CCM and FCD aren contrast to the above mentioned study from Chen andolleagues (Chen et al., 2013). They report adjacent FCDn 13 out of 18 epilepsy-patients with diagnosis of CCM andufficient tissue for evaluation of the cortical architecture.his indicates a major problem in classification for FCD.he interobserver agreement in the evaluation of the new
LAE classification for FCD has been analyzed recently amongn international group of neuropathologists with differentevels of experience (Coras et al., 2012). The neuropatholo-ists were invited to evaluate 25 samples, including a broadpectrum of FCD and negative controls, using the ILAE clas-ification for FCD. In a first and second evaluation roundine expert reviewers, which were mostly also involvedn the ILAE classification proposal reached a good interob-erver agreement. However, only a moderate agreement wasresent in an international group of 21 neuropathologists
Please cite this article in press as: Niehusmann, P., et al., Fcerebral cavernomas. Epilepsy Res. (2013), http://dx.doi.org/
t a third evaluation round. The lowest agreements werebserved in pooled ratings for FCD I/III and particularly in theegative controls (Coras et al., 2012). This may explainhe differences regarding association of FCD with CCMs
nEFo
etween our series and the results from others. However,hen and co-workers did not report if they also observed an
ncreased association of FCD IIIc with multiple CCMs. Furthernvestigations are necessary to elucidate the natural historyf FCD IIIc.
isclosure
PM received payments for lecture and manuscript prepa-ation from EISAI, UCB and Desitin and travel expensesor scientific meetings from Medtronic. None of the otheruthors has any conflict of interest to disclose. We confirmhat we have read the Journal’s position on issues involved inthical publication and affirm that this report is consistentith those guidelines
cknowledgment
ur work is supported by Deutsche ForschungsgemeinschaftKForG ‘‘Innate Immunity’’ TP2, AJB), Bundesministeriumür Bildung und Forschung (NGFNplus; AJB), Euroepi-
ocal cortical dysplasia type IIIc associates with multiple10.1016/j.eplepsyres.2013.07.006
omics Network of the European Science Foundation (AJB),lse-Kröner Fresenius Foundation (AJB), German Israelioundation (AJB) & the BONFOR Program of the Universityf Bonn Medical Center (PN, AJB).

IN+Model
G
G
M
M
M
P
R
T
ARTICLEEPIRES-4973; No. of Pages 5
FCD IIIc in CCM
References
Ardeshiri, A., Beiras-Fernandez, A., Steinlein, O.K., Winkler,P.A., 2008. Multiple cerebral cavernous malformations associ-ated with extracranial mesenchymal anomalies. NeurosurgicalReview 31, 11—17, discussion 17-18.
Batra, S., Lin, D., Recinos, P.F., Zhang, J., Rigamonti, D., 2009. Cav-ernous malformations: natural history, diagnosis and treatment.Nature Reviews Neurology 5, 659—670.
Bien, C.G., Raabe, A.L., Schramm, J., Becker, A., Urbach, H.,Elger, C.E., 2013. Trends in presurgical evaluation and surgicaltreatment of epilepsy at one centre from 1988-2009. Journal ofNeurology, Neurosurgery, and Psychiatry 84, 54—61.
Blumcke, I., Thom, M., Aronica, E., Armstrong, D.D., Vinters,H.V., Palmini, A., Jacques, T.S., Avanzini, G., Barkovich, A.J.,Battaglia, G., Becker, A., Cepeda, C., Cendes, F., Colombo, N.,Crino, P., Cross, J.H., Delalande, O., Dubeau, F., Duncan, J.,Guerrini, R., Kahane, P., Mathern, G., Najm, I., Ozkara, C.,Raybaud, C., Represa, A., Roper, S.N., Salamon, N., Schulze-Bonhage, A., Tassi, L., Vezzani, A., Spreafico, R., 2011. Theclinicopathologic spectrum of focal cortical dysplasias: a con-sensus classification proposed by an ad hoc Task Force of theILAE Diagnostic Methods Commission. Epilepsia 52, 158—174.
Chen, D.J., Severson, E., Prayson, R.A., 2013. Cavernous angiomasin chronic epilepsy associated with focal cortical dysplasia. Clin-ical Neuropathology 32, 31—36.
Coras, R., de Boer, O.J., Armstrong, D., Becker, A., Jacques, T.S.,Miyata, H., Thom, M., Vinters, H.V., Spreafico, R., Oz, B.,Marucci, G., Pimentel, J., Muhlebner, A., Zamecnik, J., Buccol-iero, A.M., Rogerio, F., Streichenberger, N., Arai, N., Bugiani,M., Vogelgesang, S., Macaulay, R., Salon, C., Hans, V., Polivka,M., Giangaspero, F., Fauziah, D., Kim, J.H., Liu, L., Dandan, W.,Gao, J., Lindeboom, B., Blumcke, I., Aronica, E., 2012. Goodinterobserver and intraobserver agreement in the evaluation of
Please cite this article in press as: Niehusmann, P., et al., Fcerebral cavernomas. Epilepsy Res. (2013), http://dx.doi.org/
the new ILAE classification of focal cortical dysplasias. Epilepsia53, 1341—1348.
Engel Jr., J., Van Ness, P.C., Rasmussen, T.B., Ojemann, L.M.,1993. Outcome with respect to epileptic seizures. In: Engel Jr.,
PRESS5
J. (Ed.), Surgical Treatment of the Epilepsies. Raven Press, NewYork, pp. 609—621.
arbelli, R., Meroni, A., Magnaghi, G., Beolchi, M.S., Ferrario, A.,Tassi, L., Bramerio, M., Spreafico, R., 2006. Architectural (TypeIA) focal cortical dysplasia and parvalbumin immunostaining intemporal lobe epilepsy. Epilepsia 47, 1074—1078.
iulioni, M., Zucchelli, M., Riguzzi, P., Marucci, G., Tassinari, C.A.,Calbucci, F., 2007. Co-existence of cavernoma and cortical dys-plasia in temporal lobe epilepsy. Journal of Clinical Neuroscience14, 1122—1124.
aciunas, J.A., Syed, T.U., Cohen, M.L., Werz, M.A., Maciunas, R.J.,Koubeissi, M.Z., 2010. Triple pathology in epilepsy: coexistenceof cavernous angiomas and cortical dysplasias with other lesions.Epilepsy Research 91, 106—110.
arucci, G., Farnedi, A., Giulioni, M., 2012. Reelin: a possiblelink between hippocampal sclerosis and cortical dyslamina-tion in the setting of FCD type IIIa. Neurological Sciences 33,1479—1481.
uhlebner, A., Coras, R., Kobow, K., Feucht, M., Czech, T., Ste-fan, H., Weigel, D., Buchfelder, M., Holthausen, H., Pieper, T.,Kudernatsch, M., Blumcke, I., 2012. Neuropathologic measure-ments in focal cortical dysplasias: validation of the ILAE 2011classification system and diagnostic implications for MRI. ActaNeuropathologica 123, 259—272.
almini, A., Najm, I., Avanzini, G., Babb, T., Guerrini, R., Foldvary-Schaefer, N., Jackson, G., Luders, H.O., Prayson, R., Spreafico,R., Vinters, H.V., 2004. Terminology and classification of thecortical dysplasias. Neurology 62, S2—S8.
aabe, A., Schmitz, A.K., Pernhorst, K., Grote, A., Von der Bre-lie, C., Urbach, H., Friedman, A., Becker, A.J., Elger, C.E.,Niehusmann, P., 2012. Cliniconeuropathologic correlations showastroglial albumin storage as a common factor in epileptogenicvascular lesions. Epilepsia 53, 539—548.
hom, M., Eriksson, S., Martinian, L., Caboclo, L.O., McEvoy, A.W.,
ocal cortical dysplasia type IIIc associates with multiple10.1016/j.eplepsyres.2013.07.006
Duncan, J.S., Sisodiya, S.M., 2009. Temporal lobe sclerosis asso-ciated with hippocampal sclerosis in temporal lobe epilepsy:neuropathological features. Journal of Neuropathology & Exper-imental Neurology 68, 928—938.