Embed Size (px)
Citation preview

Food and waterborne infections associated with packageholidays
R.Y. CartwrightMicroDiagnostics (UK) Ltd, Merrow, Guildford
1. SUMMARY
The surveillance and prevention of food and waterborne
infections in package holiday tourists relies more on common
sense and experience rather than evidence based scientific
facts. In spite of the major economic value to both sending
and receiving countries it is a problem that is largely ignored
by health departments at both local and national levels.
Package holiday tourism is a growing industry with over
20 million holidays sold every year in the UK. Destinations
are in every continent including countries with poorly
developed, as well as those with an advanced, public health
infrastructure. The incidence of gastrointestinal infection is
not reflected in official surveillance programmes as they
largely fail to capture information on travel associated
infections. Outbreaks of food and waterborne infections in
these resorts are largely not investigated. Major British tour
operators have responded by developing a crude but
effective continuous surveillance system for subjective
travellers’ diarrhoea.
The importance of food and water hygiene is, however,
not ignored and proactive preventative programmes are
being developed and implemented in some resort as well as
by the tourist industry and international agencies. There is a
need for further cooperation and partnership between
workers in different countries, different disciplines and
between the public and private sectors.
2. INTRODUCTION
International tourism is growing rapidly with an estimated
increase in 2000 of 7Æ4% bringing the total number of
international arrivals to 699 million according to the World
Tourism Organisation (2001). Europe accounts for 58% of
international tourism with 403 million arrivals in 2000. In
the UK about 50% of holidays are taken as packages that
include transport and accommodation. The UK package
holiday market has increased with sales increasing from
10Æ66 million package holidays in 1986 to 20Æ03 million in
2000. Over 90% of package holidays sold in Britain are
provided by a few major operators who together comprise
the Federation of Tour Operators (FTO). The number of
destinations increases annually. In 2001, one of the larger
operators provided holidays in 33 different countries using,
in the summer season, over 1400 different units of
accommodation.
A study of infectious intestinal disease (IID) in England
by the Food Standards Agency (2000) estimated that 20% of
the population suffered an IID in a year. Travel abroad
generally was associated with an increase in IID and
although no difference was observed in those travelling to
northern Europe, the risk to those visiting southern Europe,
Mediterranean countries and the Middle East was interme-
diate and, for travel to other countries, was large.
Surveys of illnesses in returning package holiday tourists
were undertaken at airports around 1980. Reid et al. (1980)
reported that for tourists returning to Glasgow, gastroin-
testinal upsets were the most frequent holiday associated
1. Summary, 12S
2. Introduction, 12S
3. Food and waterborne infections, 13S
4. Surveillance and investigation, 14S
4.1 Formal systems, 14S
4.2 Tour operator surveillance using the consumer
satisfaction questionnaire, 15S
4.3 Tour operator surveillance - resort staff records, 16S
4.4 Consumer groups, 17S
5. Investigations, 17S
6. Examples of incidents and situations, 18S
6.1 1984 Albufeira, Portugal, 18S
6.2 1989 Salou, Spain, 19S
6.3 1997 Portinatx, Ibiza, 20S
6.4 1990–2000 Dominican Republic, 20S
6.5 1991 Salmonella in flight meals, 21S
6.6 Emerging pathogens in package tourism, 22S
7. Discussion, 23S
8. References, 24S
Correspondence to: R.Y. Cartwright, MicroDiagnostics (UK) Ltd, 55 Holford
Road, Merrow, Guildford, GU1 2QE (e-mail: [email protected]).
ª 2003 The Society for Applied Microbiology
Journal of Applied Microbiology 2003, 94, 12S–24S

illness and that the incidence was highest in those who had
visited North Africa. Steffen et al. (1983) reported similar
findings in a survey of 16 568 travellers returning on charter
flights to Switzerland and Germany. Neither of these studies
identified the cause of the gastrointestinal upset, only
recording symptoms.
A search of records available from national surveillance
centres produces very little information on travel associated
infections, with the exception of a few specific pathogens
and even then it is a record of the number of cases reported
with no information on the number of travellers. The
Communicable Disease Report from the Public Health
Laboratory Service of England and Wales has a regular
section on common imported diseases but this primarily
relates to a few viruses and parasites. It does not provide any
meaningful information on travel-associated infections.
In spite of this, the majority of travellers and medical
practitioners can easily list a number of countries associated
with travellers’ diarrhoea under one of its many synonyms.
‘Dehli Belly’ and India, ‘Montezuma’s Revenge’ and
Mexico, ‘Tunisian Two Step’ and Tunisia, ‘Pharaoh’s
Curse’ and Egypt to name but a few of the descriptive
terms and the associated countries. Experienced travellers
are well aware that travel to most tropical and subtropical
countries, especially those with a developing public health
infrastructure, requires special care in what food and drink
is consumed. Even with precautions, however, consumer
organization publications such as Holiday which report
high levels of stomach associated illness in travellers visiting
these destinations (Consumers Association 1999).
Travellers’ diarrhoea can be caused by a wide range of
gastrointestinal pathogens and have been the subject of
reviews including those by Farthing (1992), Cartwright
(1993), Castelli and Carosi (1995), and Cartwright and
Chahed (1997). A study by Steffen et al. (1999) in Jamaica
revealed that the most frequently detected pathogens were
enterotoxigenic Escherichia coli, Rotavirus and Salmonella
species.
The source of the pathogens causing travellers’ diarrhoea
has been largely conjecture but it generally assumed that the
predominant route of spread is through contaminated food
or water. In addition to the background of travellers
diarrhoea, ‘classical outbreaks’ of foodborne and waterborne
infections affect package tourists and, although they may
attract considerable media attention, they form a relatively
small part of the overall disease burden.
The control of food and waterborne infections is the
responsibility of public health authorities. Most countries
have legislation regarding food and water hygiene, but the
implementation of the law varies with, very understandably,
public health priorities being focussed on diseases such as
Acquired Immunodeficiency Syndrome and tuberculosis. In
this context it should also be remembered that the majority
of food and waterborne infections in tourists do not impinge
on the health services of holiday countries. The illnesses can
usually be controlled by self-medication, or medical assist-
ance postponed until the tourist returns home. The resort
public health authorities may be unaware of problems and
only hear about them at a later date through international
reporting.
This review considers some aspects of the work under-
taken by major British tour operators over the past 20 years
to reduce the incidence of food and water associated
infections in package tourists. They do not have the
advantage of teams of epidemiologists and microbiologists,
nor do they have the authority to investigate outbreaks.
Cooperation with local public health authorities has been
mixed and frequently it has been more effective to work
through Ministries of Tourism rather than Ministries of
Health. It has become apparent that the control of food and
waterborne infections is best achieved in many countries
through a multidisciplinary approach.
The UK operators have developed a crude but useful
surveillance tool that has, for over 20 years, provided
continuous monitoring of the incidence of stomach related
upsets associated with the majority of resorts used by UK
package tourists. There have been few formal investigations
of outbreaks, incidents or high background illness levels and
consequently most information is descriptive and subjective.
It has, however, been sufficient to stimulate improvement
programmes resulting in major reductions in the incidence
of gastrointestinal upsets among package tourists. These
programmes have also been considered as beneficial to the
health of the local indigenous population. It has been a
salutary reminder that many of the major improvements in
public health hygiene in the UK occurred before there was
any knowledge of the microbes responsible for the cause of
gastrointestinal diseases.
Although the situation is far from satisfactory, especially
for the package holiday tourist, it should be recognized that
many tourists do not use a package and they are potentially
at greater risk as they may use accommodation and eating
establishments whose standards are not influenced by tour
operators.
3. FOOD AND WATERBORNE INFECTIONS
The spectrum of food and waterborne infections is wide
including cholera, campylobacteriosis, cryptosporidiosis,
E. coli infections, salmonellosis, shigellosis, enteric fevers,
brucellosis, hepatitis A, amoebiasis and trematode infections.
Legionellosis is also waterborne. This review concentrates on
those infections that result in a gastrointestinal upset and as
such also fit the diagnosis of travellers’ diarrhoea.
A causative pathogen is isolated from very few package
tourists and then it is only as a result of the tourists visiting
HOLIDAY FOOD AND WATER INFECTIONS 13S
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

their own general practitioner who arranges for a faecal
examination. In a few resorts if a tourist is admitted to a
local clinic, a laboratory confirmed diagnosis might be made.
It is extremely rare for any food or water microbiology
aimed at identifying a pathogen to be undertaken. Similarly
epidemiological investigations in resorts are uncommon.
The result is that, although food or water may be considered
the probable source of some infections, the proof that would
be normally expected in the UK is lacking (CDSC 1991).
The tourist industry has recognized this problem and,
rather than relying solely on definitive diagnoses and source
identification before taking any action, respond to sympto-
matic reports from tourists. As a rule of thumb, a stomach
upset lasting more than 24 h in a tourist is termed subjective
travellers’ diarrhoea (STD) and is used as an indicator of
possible food or waterborne disease.
Within the overall category of gastrointestinal illness in
tourists a number of distinct different illness categories are
recognized. The commonest is characterized by diarrhoea
with nausea and some vomiting that commences during the
first few days after arrival in a resort and generally lasts
2–3 days. This is classical travellers’ diarrhoea, with entero-
toxigenic E. coli the most frequently identified pathogen. If the
illness lasts 18–36 h and is characterized by vomiting with
some diarrhoea with the onset at any time during the holiday,
the causative agent is commonly the Norovirus. Although
Norovirus infections may be associated with the consumption
of contaminated water or shellfish, the virus may be readily
spread through the air and the environment. Less frequently,
but nevertheless with significant frequency, cases and some-
times outbreaks of the classical forms of gastroenteritis are
reported. The signs and symptoms of salmonellosis, shigel-
losis, giardiasis, E. coli O157 infection, campylobacteriosis and
cryptosporidiosis are the same whether the infection occurs at
home or on holiday.
4. SURVEILLANCE AND INVESTIGATION
The surveillance of food and waterborne infections in
package tourists has not only relied on the formal systems,
but alternative and complimentary systems have also been
developed. These have assisted in recognizing both out-
breaks and deficiencies in the public health infrastructure of
some destinations.
The investigation of outbreaks and high background levels
of gastrointestinal illness in tourists is variable with little
formal action being taken in most resorts.
4.1 Formal systems
In many countries the surveillance systems for the detection
and reporting of infections, including water and foodborne
diseases, are weak or non-existent. Resources for investigation
purposes are meagre and public health priorities are targeted
at disease that impact more directly on the health and economy
of the country. This situation is compounded by the lack
of accredited laboratories that are adequately funded and
staffed to undertake relevant microbiological investigations.
Even in countries with a well-developed surveillance and
health infrastructure data collection on travel-associated
infections is inadequate. Illnesses in package tourists that are
contained within the holiday country are very rarely notified
to the authorities in that country. Even when significantly
large outbreaks have occurred there may be considerable
pressure from hoteliers to prevent any formal notification as
‘this may be bad for business’. Even if notification does occur
local political pressures may prevent any further action being
taken.
The surveillance of communicable diseases in the UK is
well developed and, although information on travel-associ-
ated illnesses is very deficient, it has enabled outbreaks
caused by specific pathogens to be identified. It should be
remembered, however, that the system depends on tourists
consulting their general practitioner, a faecal specimen being
submitted to a laboratory, a pathogen being isolated or
identified and the result being reported to the Public Health
Laboratory Service (PHLS), Communicable Disease Sur-
veillance Centre (CDSC), or in Scotland to the Scottish
Centre for Infection and Environmental Health, together
with the travel information. The number of cases being
reported compared with the number of those infected is
likely to be low and the lack of information on the number of
tourists visiting a suspect source destination means that the
incidence of disease cannot be determined.
Information from CDSC is, however, shared with Enter-
net, the international surveillance network for Salmonellae
and E. coli, and also transmitted, as appropriate, to the
regional office of the World Health Organisation and the
Ministry of Health of the holiday country. This whole
procedure may take weeks, or even months, so that local
investigations, even if possible, may no longer be relevant.
No information is available on the incidence of package travel
associated illness from established surveillance systems.
Formal systems do, however, identify cases of specific
infections that may be of great public health importance, not
only for tourists but also the indigenous population of the
country concerned. The enteric fevers because of Salmonella
typhi and Salmonella paratyphi are recognized as important,
although infrequent, causes of food and water associated
infections in package tourists. The potential seriousness of
these infections has led to formal investigations in the
countries concerned. More recently reported cases of E. coli
O157 have received particular attention.
The transfer of information from holiday countries of
illness outbreaks in tourists to the governments of sending
countries and to the tour operators is lacking.
14S R.Y. CARTWRIGHT
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

4.2 Tour operator surveillance using theconsumer satisfaction questionnaire
In the 1980s it was generally recognized in the tourist
industry that certain destinations were associated with an
above average incidence of gastrointestinal illnesses in
package holiday tourists. There was, however, no measure
of the levels of illness in resorts, reliance being placed on the
impressions of staff in resort and the number of complaints
from returning tourists. Representations to government
officials in high incidence areas were usually countered with
the comment that there was no proof and it was just the
English who complained.
Major tour operators collected a considerable amount of
information for marketing purposes from returning tourists
by means of a client satisfaction questionnaire (CSQ)
completed by adult tourists during the return charter flights
to the UK. The CSQs primarily collected information that
would be of use to the operators in designing their
programmes for future seasons. As CSQs were issued on
every flight it gave a continuous stream of information
enabling trends over time to be observed as well as
differences between resorts.
A suggestion that a health questionnaire be included was
met with opposition from the tour operator’s legal advisers
who feared that attention might be drawn to illnesses with a
subsequent increase in demand for compensation. Eventu-
ally it was agreed to insert a question asking if the tourists
had been ill during their holiday and if so with what illness.
The illness descriptions were categorized, according to laid
down criteria, by the clerks entering data from the CSQs
into a computer. The term STD was coined for illnesses
described as a stomach upset, diarrhoea or vomiting.
In the first few years, only a sample of the CSQs were
analysed according to the commercial requirements of the
operator, the proportions varying between resorts. Never-
theless, the total number of CSQs analysed each year
exceeded 200 000. The data was analysed monthly using the
statistical analysis system SPSS. The standard output
chosen gave the monthly incidence of STD for each holiday
region and resort. Further analysis could be undertaken to
hotel level but the numbers were often too small to enable
any meaningful statistics to be obtained.
In 1995, the health question was refined initially to ask
specifically if during their holiday they had suffered from a
stomach upset and data entry using optical mark readers was
introduced. In the same year the annual number of
questionnaires analysed exceeded 1Æ5 million.
In summer 2000, the question was further refined to ask if
any stomach upset lasted for more than 24 h. The purpose
of this refinement was to reduce the number of reported
stomach upsets following an episode of excessive alcohol
intake.
As of 2002, further tour operators have included the latest
question in their CSQs and it is expected that upwards of
3–4 million sets of data will become available for analysis.
The analysis results are produced monthly and as such are
retrospective.
Although the change in the questions prevents a com-
parative longitudinal analysis to be undertaken, over the
years the pattern of illness between geographical areas for
each year is remarkably similar.
It was recognized from the outset that such information
was very crude in formal surveillance terms and was in no
way controlled or substantiated. The data was also restricted
to tourists over 16 years of age. The question was whether
the information provided would be sufficient for the purpose
for which it was required. The requirements were to identify
problem areas, to work with local authorities and hoteliers in
identifying causes, to take remedial actions and to assess the
effectiveness of such actions.
It rapidly became apparent that suspect problem areas
were indeed those with a higher level of travellers’ diarrhoea
and that some resorts previously not suspected warranted
closer inspection.
The number and location of resorts and hotels is variable
both between summer and winter seasons and from year to
year as the operators develop their programmes. Popular
destinations have, however, remained relatively constant
over the 20 years that this surveillance method has been in
operation. Southern European and Mediterranean destina-
tions take the majority of package holidaymakers, but there
has been a growing number of long haul destinations in
Africa, Asia, America and the Caribbean. In summer 2001, a
total of over 1 million CSQs were analysed with tourists
visiting over 500 resorts in 33 countries and staying in over
2000 different hotels.
As the make up of destinations is very different between
winter and summer seasons, with family holiday seaside
resorts predominating in the summer, and ski and long haul
sunspots in the winter seasons, the seasons are analysed
separately.
A major drawback of this form of surveillance is that it
provides no information, either microbiological or epidemi-
ological, as to the cause of the illnesses. It does, however,
provide an indicator as to where further studies may be of
value and also, because of the ongoing nature of the study,
does provide a measure to assess the effectiveness of any
remedial measures.
Geographical variations The overall geographical pattern
of STD has altered little over the past 13 years. Compared
with southern European destinations, the north African,
Caribbean and Central American destinations were associ-
ated with an appreciably higher level of stomach upsets.
(Table 1).
HOLIDAY FOOD AND WATER INFECTIONS 15S
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

This information compares well with the anecdotal
information and the results of the airport passenger surveys
and demonstrates that between 1989 and 2001 the areas of
higher risk remain unaltered.
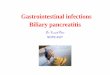
In summer 2001, of 709 579 UK tourists completing
CSQs 6% recorded a stomach upset lasting more than 24 h.
In those returning from Switzerland the incidence was 2Æ5%
while those returning from Egypt it was 30Æ8% (Fig. 1).
This higher rate has been relatively unaltered for many
years.
When the regional results are further examined by resort
it is possible to ascertain whether any problems are restricted
to a smaller geographical area or whether there is a larger
problem that may reflect the state of the public health
infrastructure. Resort data similarly can be examined to
hotel level providing information that may suggest a food
hygiene problem within one hotel or a community wide
situation that may indicate, for example, a water supply
problem.
An example of this examination of regional results for
Tunisia is given in Table 2. In 1989 here was an overall
STD incidence of 17% in 3949 tourists. In 2001, the overall
incidence was 21% in 11 149 tourists.
There is an overall similarity in the levels and patterns of
illness for each resort, and in both 1989 and 2001. The actual
questions asked varied, as in 1989 the tourists stated their
illness whereas in 2001 they were asked if they had a
stomach upset lasting more than 24 h. The hotels used in
the 2 years also were different as some were dropped from
the programme and others added but with little overall
effect on the incidence. The breakdown for the resort of
Monastir (Table 3) shows an overall similarity between
hotels in 1989 with no single hotel being responsible for the
overall level of illness. The incident values for some hotels
have no significance due the small denominator. In 2001,
hotel 5 from 1989 was the only one remaining in the
programme. The seasonal incidence of STD was 21% in
1989 and 22% in 2001. Similar findings have been observed
in other years and can be interpreted as reflecting the overall
state of hygiene and environmental control in the country,
coupled with the level of the public health infrastructure.
This is supported by little observed change in illness levels
in spite of the introduction of intensive food hygiene
programmes in hotels by the Tunisian government.
In 1997, there was a Salmonella outbreak associated with a
hotel in Ibiza. In Table 4 the monthly CSQ incidence
pattern of resort 3 differs from the other two resorts with an
increase in June. Analysis of the hotel associated illness for
this resort indicated that the problem was associated with
hotel 3. The pattern of illness coincided with an outbreak of
Salmonella food poisoning in this hotel. The CSQ results
also indicate that the outbreak was successfully controlled.
4.3 Tour operator surveillance – resort staffrecords
Neither formal surveillance nor the tour operator CSQs
provide immediate information on a situation of food or
waterborne illness as it occurs. If immediate action is to be
taken to control an outbreak, prompt notification is neces-
sary. When a tourist in a package becomes unwell the usual
response is to try self-medication then, if that is not
effective, to inform the tour operator representative. There
is a general reluctance by tourists to seek medical assistance
in another country unless absolutely necessary. It has proved
very difficult to arrange with tour operators for the
representatives to keep records of reported illnesses, but a
system is being introduced to record basic information. The
provision of early information on outbreaks together with
clinical information, even if very basic, is of great value in
EgyptDominican Republic
MexicoTunisia
CubaTurkey
St LuciaJamaicaAntigua
BarbadosZakynthos
Costa DoradaMalta
MajorcaCyprus
Costa BravaGran Canaria
TenerifeNeopolitan Riviera
Greek MainlandCorfu
AlgarveRhodes
CreteMinorcaFloridaAustria
Switzerland
0 10 20 30
Incidence (%) of subjective travellers' diarrhoea
Fig. 1 Incidence of subjective travellers’ diarrhoea in British package
holiday tourists summer 2001
Table 1 Comparative incidence of subjective travellers’ diarrhoea of
different destinations compared with Majorca
Region 1989 1993 1998 2001
Spain – Majorca 1 1 1 1
Spain – Costa Brava 1 1Æ1 1Æ2 1
Spain – Costa Dorada 1Æ7 1Æ3 1Æ1 1Æ1Portugal – Algarve 1Æ6 1Æ2 1Æ1 0Æ8Greece – Zakynthos 1Æ2 1Æ8 1Æ7 1Æ2Malta 1Æ2 1Æ3 0Æ8 1Æ2Turkey 5Æ5 5 3 3
Tunisia 4Æ4 5Æ2 3 4Æ2Egypt Not used 8Æ4 3Æ7 6Æ2Dominican Republic Not used 9Æ1 3Æ2 6
Mexico 7Æ4 5Æ2 4Æ1 4
Florida 0Æ4 0Æ6 0Æ8 0Æ6
16S R.Y. CARTWRIGHT
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

assessing whether they are likely to be because of bacterial
food poisoning or because of the Norovirus. The distinction
is important, as it will affect the subsequent actions that
need to be taken.
4.4 Consumer groups
Increasingly tourists consumer groups are collecting infor-
mation from disgruntled tourists who have been affected by a
gastrointestinal upset on holiday. The information will
frequently include the results of any laboratory tests arranged
by the tourist’s general practitioner. The consumer groups
tend to contact the relevant tour operator demanding that
action be taken. This system has on occasions provided the
earliest notification of a problem, as formal reporting of
laboratory results may take a week or more. The first
indication of a major swimming pool associated outbreak of
cryptosporidiosis in 2000 in Majorca was by this means. At
present a drawback of consumer group notification is that it is
usually not possible to obtain confirmation of the results or to
obtain further details of the travel. Reporting by this route is
also frequently followed by litigation with the provision of
further information being moderated by lawyers.
5. INVESTIGATIONS
Formal investigations are rarely undertaken or, if they have
been, the reports are not generally available. Such investi-
gations would normally be the responsibility of the local
public health departments who do not usually receive any
substantiated information on an outbreak at an early time
enough to undertake a meaningful investigation. The
resources available are also frequently minimal, with the
investigation of outbreaks in tourists being low in their
priority order. Staff from CDSC have given advice on
outbreak investigation but they have no authority to
Table 2 Incidence of subjective travellers’ diarrhoea in British package tourist visiting Tunisia in summers 1989 and 2001
May June July August Sept Oct Total season
Resort 1989 2001 1989 2001 1989 2001 1989 2001 1989 2001 1989 2001 1989 2001
Hammamet 11 9 13 10 19 16 30 24 28 27 15 24 18 18
Monastir 18 12 17 16 16 36 20 29 20 22 23 15 18 23
Port El Kantaoui 16 7 15 12 18 22 14 27 24 25 6 26 15 21
Sousse 10 11 19 17 17 28 18 27 23 27 9 27 16 23
Tunisia – all resorts 13 9 16 14 18 24 23 27 25 25 15 25 17 21
Table 3 Subjective travellers’ diarrhoea associated with hotels in Monastir, Tunisia in summer 1989
May June July Aug Sept Oct Total season
Hotel % n % n % n % n % n % n % n
1 18 45 7 14 14 14 24 17 31 13 20 10 18 119
2 25 16 21 19 7 15 17 36 21 28 60 5 20 119
3 17 6 0 0 0 4 19 26 14 36 11 19 13 104
4 14 22 22 27 23 22 29 17 11 36 11 9 18 134
5 18 39 18 17 21 14 28 18 31 32 28 18 21 171
Monastir all hotels 18 128 17 83 16 69 20 130 20 145 23 62 18 670
%, Incidence; n, number of CSQs in analysis.
Table 4 Incidence of subjective travellers’
diarrhoea associated with Ibiza, three resorts
on the island and three hotels in resort 2, 1997
May June July Aug Sep Oct Season
Ibiza 11 12 15 14 13 12 13
Resort 1 12 11 16 12 15 13 13
Resort 2 10 11 16 14 13 14 13
Resort 3 10 17 20 16 13 10 15
Hotel 1 10 16 13 19 16 9 14
Hotel 2 2 8 2 15 3 0 5
Hotel 3 7 23 36 12 8 7 19
HOLIDAY FOOD AND WATER INFECTIONS 17S
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

undertake investigations in another country unless formally
invited by the government of that country.
The Catalan Public Health Department investigated an
outbreak of typhoid fever in Salou, Spain in 1989 with
invited support from the PHLS and, in 1999, a suspected
outbreak of paratyphoid B in Antalya, Turkey was inves-
tigated by a joint European team coordinated by staff from
CDSC but facilitated by the FTO.
An outbreak of gastroenteritis on a cruise ship in the
Mediterranean was investigated by a team from CDSC at
the request of, and financed by, the tourist industry
(McEvoy 1996). This ship outbreak could be investigated
as the vessel was in international waters.
A questionnaire study into Norovirus-like illness in
Andorra in February 2002 was undertaken in Eire and
Northern Ireland as substantial illness in passengers of
returning flight to Dublin and Belfast was reported to the
port health authorities (Feely and McKeown 2002).
The major UK tour operators are not in a position to
undertake outbreak investigations, yet they have a legal
responsibility to ensure that their clients are not unneces-
sarily put at risk. In the event of a suspected outbreak of
foodborne infection they usually send an independent
consultant to the hotel or hotels concerned to undertake a
risk assessment and to make any necessary recommenda-
tions. The consultants have trained as environmental health
officers, many reaching senior positions in local authorities,
before joining a consultative company. These consultants
can only work within the hotels with the agreement of the
manager. An inspection of the kitchen and food hygiene
practices is undertaken, and the quality of the water in the
hotel checked. Increasingly it is the policy to liase with the
resort public health department to share information. As
such a consultant’s inspection is not an outbreak investiga-
tion but may identify possible causative factors that can be
remedied. This is a reflection on the practical problems in
dealing with possible food and waterborne infections in
package holiday tourists. Local authorities will not usually
consider an investigation as a matter or priority, whereas the
tour operator will be mindful that at all times there will be
aircraft in the air bringing new tourists to a destination.
Every effort must be taken to ensure their safety.
6. EXAMPLES OF INCIDENTS ANDSITUATIONS
This section provides examples of some outbreaks and
situations of possible food or waterborne infections that have
occurred between 1984 and 2000.
6.1 1984 Albufeira, Portugal
In August, an increasing number of tourists reported
gastroenteritis characterized by diarrhoea, abdominal
cramps and nausea to their tour operator. Guests in hotels
in different parts of the town were affected with attack rates
of up to 85%.
The results of a questionnaire survey of returning tourists
from this and an adjacent resort confirmed that in late
August over 65% of tourists to Albufeira had gastroenteritis
compared with 39% in a neighbouring resort. Samples of
water from the public water supply revealed the presence of
coliforms.
Reports were being received by CDSC and Scandinavian
surveillance centres of an increase in the number of
gastrointestinal pathogens from tourists returning from
Albufeira. The predominant isolate was Shigella sonnei,although Salmonella spp, Campylobacter and Giardia lamblia
were also reported.
The attendance record at the local health clinic showed
that in early August there was a distinct rise in the number
of cases presenting with diarrhoea (Fig. 2). Those affected
were the indigenous population, Portuguese tourists and
foreign tourists.
The pattern of illness throughout the community sugges-
ted the possibility of contaminated water. The water supply
system was investigated by the Algarve Public Health
Department together with invited assistance from the
PHLS. Major deficiencies were identified with totally
inadequate chlorination of the water supply. Inadequacies
1 11 21 31 10 20 30 9 19 29 9 19 29 0
20
40
60
80
100
Pat
ient
s w
ith d
iarr
hoea
August September OctoberJulyFig. 2 Patients with diarrhoea attending the
clinic in Albufeira 1984
18S R.Y. CARTWRIGHT
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

in the sewage disposal system were also identified with raw
sewage passing over the beaches used by tourists.
In view of the severity of the situation emergency
chlorination of the water supply was undertaken by adding
bleach to all the service reservoirs. Over the subsequent
months major works were instituted to ensure the safety of
the drinking water supply and to bring the sewage system
and treatment works up to an acceptable standard. The level
of gastrointestinal illness fell after chlorination of the water
supply, and the level of STD fell from a peak of 50% in
1984 to under 20% in subsequent years.
Although not proven, there is strong suggestive evidence
that the gastroenteritis was associated with both drinking
and recreational waters. The outbreak was investigated by a
joint Portuguese British team led by the Medical Officer for
Health of the Algarve. Major expenditure was necessary to
improve the public health infrastructure but was beneficial
to the indigenous population as well as the tourists.
6.2 1989 Salou, Spain
In mid-July, a tour operator became aware of an unexpected
increase in reports of diarrhoea and vomiting among their
clients. Eleven tourists had been admitted to the local clinic
requiring rehydration. The local authority was aware of the
problem and had tested foods and water samples although
the results were not known. Shortly afterwards three cases of
typhoid fever in tourists recently returned from Salou were
received by CDSC. A resort visit was made by a medical
consultant on behalf of the tour operator to investigate the
high level of gastroenteritis. It was observed that the tap
water had a very high saline content and was undrinkable.
Hotels were obtaining water from lorries, the source of the
water not being known.
Following the typhoid reports an investigation was
undertaken by the Catalan Public Health Department with
invited assistance from the PHLS.
A total of 15 cases of typhoid fever were reported from
returning tourists from Salou and the neighbouring Cam-
brils; seven from England and Wales, two from Switzerland,
one from each of Sweden, Eire and Spain, in addition to
three local inhabitants. Twelve of the isolates were typed at
the PHLS Central Public Health Laboratory in London.
Three different phage types were recognized. Nine were
type A, two were type C1 and one was type E1. The cases
had stayed at different hotels or lived in different parts of
the municipalities and no common feature such as eating at a
restaurant or bathing from the same beach could be
identified.
Hotel kitchens were inspected and food handlers screened
for Salm. typhi. No carriers were identified.
Most hotels were obtaining water from lorries that had
been filled from various inland wells and rivers, some of
which were unlicensed. The inadequacy of the public water
supply had been recognized as a result of the wells becoming
exhausted and the saline content of the water rising. A new
public water supply had been constructed with a river source
and fortuitously was due to become operational within a few
weeks.
It was considered that contaminated lorry water was the
most probable source of the infections. The multiple phage
types indicated sewage contamination of the water from a
community or communities containing a number of typhoid
excretors. Hoteliers were given advice on the importance of
only purchasing water from approved suppliers and on the
management of the water within their buildings. The new
public water supply became operational within a few weeks
of the outbreak and this was accompanied by a sharp drop in
the number of cases of gastroenteritis and no further cases of
typhoid fever.
The CSQ results revealed that there had been a high
incidence of STD the previous year but this had not been
accompanied by any reported typhoid fever cases. The
following years, after the new water supply became opera-
tional, the incidence of STD was greatly reduced (Fig. 3).
Although there was a general improvement in hygiene
standards, it is most probable that the reduction in
gastrointestinal illness was associated with the introduction
of the new water supply. The typhoid outbreak, while not
proven, was also most probably waterborne.
This outbreak underlies the importance of adequate
drinking water supplies and the problems that can be
associated with unofficial supplies. Although the presence
of S. typhi was not demonstrated in lorry water supplies
the circumstantial evidence is very suggestive. It was
fortunate that the new public water supply became
operational within such a short time. The publicity
surrounding this outbreak severely affected the number
of tourists visiting the resort in the subsequent years
m j j a s o m j j a s o m j j a s o m j j a s o0
5
10
15
20
25
30
Sub
ject
ive
trav
elle
rs' d
iarr
hoea
(%
) New water supply
1988 1989 1990 1991
Fig. 3 Subjective travellers’ diarrhoea in British tourists visiting
Salou, Spain 1988–1991
HOLIDAY FOOD AND WATER INFECTIONS 19S
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

underlying the fact that food and waterborne infections can
have major economic consequences.
6.3 1997 Portinatx, Ibiza
In mid-June, there was a sudden increase in the number of
guests in one hotel reporting with diarrhoea and vomiting. In
the following week, cases of Salmonella enteritidis phage type 8
infections were reported to CDSC. In the period 20–29 June,
92 illness reports were recorded by the representative of the
tour operator in the hotel, from 17 of these S. enteritidis phage
type 8 was isolated. In mid-July a further 73 illness cases were
recorded, with S. enteritidis phage type 8 being isolated from
17 of these cases.
The local health department was notified of the findings
but no formal investigation was undertaken. The tour
operator arranged for hygiene consultants to visit the hotel
and inspect the kitchens and food handling practices. Major
deficits were observed with no adequate separation of raw
and prepared foods, slicing machines being used for raw and
cooked foods with insufficient cleaning, poor refrigeration
facilities and a lack of understanding of food hygiene
principles by the senior kitchen staff. It was not possible to
arrange any bacteriological examination of foods or the
environment. It was observed that the only poultry used in
the kitchen was turkey. This was on the menu twice every
week. It was purchased as frozen 5 kg rolls that were
thawed, but the inner temperatures not checked, before
cooking. The turkey originated in France being driven to
Barcelona then shipped to Ibiza. The local public health
department had no information on the bacteriological
quality of this product and were unwilling to undertake
any testing.
A thorough cleaning programme was introduced and a
trainer chef installed to take over the food preparation and
train the staff in the kitchen. All turkey rolls were cut in half
for thawing and cooking not commenced until the core
temperature was above 4�C. The core cooking temperature
reached at least 80�C. Medium- and long-term plans to
improve the kitchen facilities were drawn up. It was decided
not to withdraw guests from the hotel as the new chef was of
the opinion that safe food could be produced from the
kitchen with proper supervision. No further cases of
Salmonella infection were reported after mid-July.
There is no definitive proof as the source of the
Salmonella infections but it was accepted that the deficien-
cies in the kitchen hygiene were a major factor in the
outbreak. Whether or not the turkey rolls were the source of
infection is a matter of conjecture although in other places
frozen poultry rolls that have been insufficiently thawed or
cooked have been associated with Salmonella outbreaks. It
was unfortunate that the local public health authority was
unable to mount an investigation. The tour operator has no
power to close a hotel although they can withdraw their
clients. The owners of the hotel were very cooperative and
had not appreciated the level of poor hygiene in the kitchen.
The incidence of STD in hotel guests rose above the resort
average in June and July. The hotel affected was hotel 3 in
Table 4.
6.4 1990–2000 Dominican Republic
The major tour operators introduced the Dominican
Republic as a destination in the late 1980s. In 1990, the
incidence of STD was 40% for summer season, rising to
46% in August. This is compared with a seasonal level of
2% for Florida, another new destination.
In the Dominican Republic there was very little difference
between resorts or individual hotels suggesting possible
inadequacies in the public health infrastructure, especially
the water and sewage systems. A visit was made by a tour
operator consultant in 1991 to gain an understanding of the
general public health infrastructure and hotel hygiene
standards. Discussions were held with the Secretary of
State for Tourism, senior officials within the Ministry of
Health, the Pan American Health Organisation representa-
tive, the Hotel Owners Organisation, the national water
authority and the tour operators. Major inadequacies were
identified, not least of which was the intermittent electricity
supply with no reliable back-up system. This affected
pumps for water and sewage as well as the functioning of
cold storage facilities.
Some of the hotel kitchens had very poor standards, with
no understanding of food hygiene principles by the staff. It
was concluded that there was a very real possibility of both
food and waterborne infections occurring. The housing and
facilities for hotel staff were such that levels of personal
hygiene accepted as normal in Europe could not be achieved.
There was some official acceptance by government repre-
sentatives of the situation and an indication that action
would be taken.
Over the next few years, little improvement was observed
in spite of numerous consultant visits and discussion with a
succession of Ministers of Health and of Tourism. Tour
operators identified those hotels that posed the greatest risk
and removed them from their programme. The destination
remained popular with tourists, but the incidence of STD
was unacceptably high and evenly spread amongst the
hotels. The reason for this high incidence was not identified
and there were no facilities or resources for a thorough
investigation. Various hypotheses were, however, consid-
ered. These included inadequacies in the public health
infrastructure. In particular, the water and sewage systems
and the level of kitchen hygiene and food hygiene practices
in the hotels were deficient. In some of the tourist areas a
new public water supply was constructed supplying both the
20S R.Y. CARTWRIGHT
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

hotels and the indigenous population, but there was no
measurable impact on the STD levels. The water supplies in
other areas were variable with many hotels relying on their
own shallow wells. Chlorination within hotels and ultraviolet
light treatment was frequently used, but was uncontrolled.
On-site testing, with a portable laboratory, usually indicated
the presence of coliforms, and occasionally E. coli, in hotel
water systems. Tour operators recommended that guests
should only use bottled water. Ice remained a problem, as
many hotels had their own ice making machines using their
own uncontrolled water. The water supplies to some of the
villages where the hotel staff lived was intermittent or by
water lorry. The quality of the supply was unknown, but on
general grounds regarded with suspicion. A few sewage
disposal systems serving groups of hotels were in existence
although many hotels had their own treatment plants.
The public health departments had insufficient resources
or trained inspectors to visit hotels and advise on food
hygiene. Inspections by hygiene consultants employed by
tour operators revealed that in most hotels there were major
deficiencies in the kitchen facilities and the food hygiene
practices in most, but not all, hotels.
In 1998, members of the Federation of Tour Operators
decided that, if they were to continue to offer holidays to
this destination, a comprehensive food hygiene-training
programme was necessary. They all adopted a common
policy that they would only use hotels that contracted with
Cristal International, a commercial food hygiene training
and auditing company. Hotels that did not agree were
removed from all the operators’ programmes. Initial
inspections by Cristal International revealed that many
hotels would require major refurbishment of kitchen areas to
enable basic food hygiene practices to be achieved and to
progress to a HACCP (Hazard Analysis Critical Control
Point) approach (WHO 1997). In the first 4 months of the
programme 13 500 food handlers were given basic food
hygiene training, the majority receiving such training for the
first time. It was discovered that the training needed to be
repeated regularly because of a large staff turnover. Training
was also provided for government health inspectors. This
initiative has been maintained, although alternative consult-
ants are now acceptable. Many hoteliers who were initially
hostile to this approach, particularly as capital expenditure
was necessary to upgrade kitchens, have found that parti-
cipation in the programme has proved to be a marketing
advantage. Ministers in the Dominican Republic govern-
ment have expressed their support for the programme. As a
result of this action a reduction in the incidence of STD was
observed and the number of ‘food poisoning’ complaints
received by tour operators declined (Table 5).
The introduction of a food hygiene programme is
universally recommended but there is little evidence to
show that, at least in the short-term, such programmes affect
the level of foodborne infection. To draw conclusions from
the experience in the Dominican Republic is largely
circumstantial in the absence of either any formal epidemi-
ological studies or any microbiological studies. The differ-
ences in STD rates are, however, at the least coincidental
with improvements in food preparation hygiene and
conform to what would have been expected on theoretical
grounds.
6.5 1991 Salmonella in flight meals
In early August 1991, reports of gastroenteritis because of
S. enteritidis phage type 6 in passengers who had flown with
two charter airlines from Corfu on 2 August were received
by CDSC (CDSC 1991). There had been 10 flights from
Corfu on that day carrying a total of 1373 passengers. The
airlines were notified by the Department of Health. Reports
were also received from other countries of similar Salmonella
illness in passengers who had flown from Corfu on that day.
All the flights involved had uploaded their flight meals from
the same supplier in Corfu. The meal served comprised: a
cold starter of fish and potato salad with mayonnaise, a main
course of stewed meat, potato, sweet corn and peas followed
by a desert of a gateau. No starters or deserts were available
for examination but a main course dish that had been deep-
frozen was examined at Guildford Public Health Laborat-
ory. A Salmonella was isolated from the meal but was a
different serotype to the outbreak strain.
Questionnaires were sent from CDSC to 1200 passengers
and there was a 57% response rate. The overall attack rate
was just over 50%. The relative risks associated with foods
consumed were fish 3Æ9%, potato salad 2Æ5%, meat 6Æ7%,
vegetables 3Æ9% and gateaux 2Æ4%. The flight meal kitchen
was visited and found to be of a high standard. At this stage
the mayonnaise used in the potato salad was considered to be
the most likely source of infection and this hypothesis was
strengthened when the chef admitted that in the week of
the outbreak he had changed from a commercial mayonnaise
to mayonnaise prepared in the kitchen from shell eggs.
Table 5 Incidence of subjective travellers’ diarrhoea (STD) in British package holiday tourists visiting the Dominican Republic during the summer
season
1992 1993 1994 1995 1996 1997 1998 1999 2000
STD (%) 43 46 48 43 57 57 38 34 29
HOLIDAY FOOD AND WATER INFECTIONS 21S
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

A sample of the mayonnaise had been examined in a local
laboratory after the outbreak and Salmonella was reported to
have been isolated. A visit was made to the laboratory, which
was a small private clinical laboratory, to obtain a sub-
culture of the isolate for phage typing. The isolate had not
been retained, but it was readily apparent that the report was
meaningless as the identification relied on colonial appear-
ance on a blood agar plate. It transpired that the laboratory
staff were aware that the mayonnaise was the suspect food
and they duly obliged!
The main courses had been prepared as a large batch in
the flight meal kitchen and there were a large number of
ready to serve portions in a deep freeze. Ten meals were
examined in the UK and from two the outbreak strain was
isolated. On both occasions the Salmonella was present in
the sweet corn and peas section of the dish. This section also
contained large numbers of coliforms. The vegetables had
been prepared by cooking in bulk, the water drained off then
they were rinsed with cold water to ensure rapid cooling and
refreshing. This process took place in containers that may
have previously contained raw vegetables and salads. The
water used was from the municipality supply and had
residual chlorine of 0Æ6–0Æ8 mg l)1.
The final conclusion was that the vegetables were
contaminated during the cooling and refreshing stage. The
source of contamination was not identified although it could
have been from a previously contaminated container or from
a food operative. The initial hypothesis of the mayonnaise
was not substantiated. It was interesting and disturbing to
note that the chef and the local environmental health
inspectors had little understanding of the potential dangers
of fresh eggs. The findings of the local laboratory underlined
the dangers of using non-accredited laboratories. The
investigations in this incident were possible as the illnesses
commenced after the tourists had returned to the UK. The
investigations in Corfu were arranged by the principal
airline involved but there was good support from the local
public health department. As a result of the outbreak the
flight meal kitchen ceased trading.
6.6 Emerging pathogens in package tourism
Over the past few years two pathogens have been
associated with package tourism, and each has brought
their own particular problems.
Cryptosporidium parvum has been reported from isolated
cases of returning tourists for many years but in 2000 major
outbreaks were recorded. The diagnosis was made on return
to the UK and the information reported to CDSC at
variable rates. A relatively new feature was that in one
instance a consumer group was the first to notify the tour
operator that there was a problem but were unwilling to
assist in obtaining further information. The tour operator
was in the situation of being expected by consumers to take
action to prevent further cases of an unsubstantiated disease.
When further information was forthcoming from the
affected tourists and CDSC, it was apparent that the
outbreak was associated with only one hotel in the resort.
This indicated that the drinking water supply was unlikely
to be the source of infection. The hotel swimming pool
became the suspect source and cooperation with the local
health department sought. They stated that the pool was
satisfactory and indicated no real interest in the outbreak
although there were over 150 confirmed cases. It was not
possible for the tour operators to mount an epidemiological
study for legal reasons. Examination of hotel pool water by
Thames Water laboratories in the UK revealed the presence
of low levels of oocysts. The tour operator withdrew from
the hotel, although it continued to be used by operators from
other European countries.
In the year 2000, returning tourists reported 219 cases of
confirmed cases of cryptosporidiosis, including 106 from the
above outbreak, to FTO members from seven different
countries or major holiday regions. The majority were
associated with one of the Balearic Islands (CDSC 2000).
Hotel swimming pool water treatment processes varied but
it was recognized that spread from a faecal accident in the
pool to other bathers would occur before the water was
processed. Examination of the reported cases indicated that
in some instances the index case developed symptoms
shortly after arrival in the hotel and had travelled from a part
of the UK where cases of cryptosporidiosis were occurring.
It is possible, that in some instances, Cryptosporidium may
have been taken to the hotels by tourists.
The other ‘new’ pathogen is the Norovirus that is, at the
present time, the most problematic cause of gastrointestinal
infection in package holiday tourist. Although the spread
once introduced into a hotel or ship may be through the air,
the initial source may be food, water or an infected guest or
member of staff. Investigation of the outbreak in Andorra by
the Irish epidemiology service (Feely and McKeown 2002)
and consultants commissioned by tour operators raised the
possibility that the drinking water may have been the source
of infection. The diagnosis is generally from the clinical
presentation. Once established in a hotel it generally persists
for a few weeks with a recrudescence in the number of cases
each week as new susceptible hosts or tourists arrive. It is
not clear what the indications are for closing a hotel to break
the chain of infection, or indeed whether such a move would
be supported by resort public health authorities.
There is an urgent need for further investigation into
outbreaks of Norovirus in holiday resorts, both to identify
sources of infection and to control the outbreaks. The health
and safety committee of the FTO has produced pilot
guidelines on the management of Norovirus outbreaks in
hotels that will be tested in summer 2002.
22S R.Y. CARTWRIGHT
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

7. DISCUSSION
Gastrointestinal infections are regarded as the commonest
travel associated illnesses. The term travellers’ diarrhoea is
used to cover the majority of these infections and has been
the subject of many reviews (Farthing 1992; Cartwright
1993; Castelli and Carosi 1995; Cartwright and Chahed
1997) but little sustained epidemiological and microbiologi-
cal study. Studies such as that by Steffen et al. (1999) have
primarily concentrated on the presentation of the illnesses,
their duration and severity, the causative agents and the
effect of various medications. There is a lack of information
on the source of the infections and the effect of public health
measures to reduce the illness of the infections.
National communicable disease surveillance programmes
do not identify the majority of water and foodborne disease
in travellers. This is mainly because the illness is usually
self-treated, or if medical assistance is sought, laboratory
tests were not undertaken or even available. The incentive to
improve the situation has a low priority in national health
service programmes as the illnesses have a minimal effect on
the health services of a country and those affected return to
their home country within a short time. Imported infections
in returning tourists may be identified, but any investigation
is regarded as the responsibility of the local health author-
ities in the holiday destination. Travel associated gastroin-
testinal infections that are primarily food and waterborne
are, therefore, largely ignored by the Ministries or Depart-
ments of Health of most countries. Ministries of Tourism
may have a concern but, as it is a health issue, may be
powerless to take action. This has resulted in the UK tourist
industry, and in particular the major tour operators,
developing a crude surveillance system and in promoting
health and safety programmes.
Academic epidemiologists ridiculed the development of
the CSQ approach to collect basic health data 20 years ago
as being too simplistic to be of any value. Its limitations
were, however, recognized from the beginning and inap-
propriate conclusions not drawn from the results. It has
proved to be adequate for the purpose for which it was
required. The results have been used to great advantage in
identifying high-risk resorts, and in separating problems
because of deficient public health infrastructure from those
of poor kitchen hygiene in hotels. It has been possible to
monitor the health effects of remedial actions.
There have been, and still are, deficiencies in the
investigation of suspected outbreaks. What is often not
obvious is the background political manoeuvring to prevent
any investigation in some destinations. The fear of publicity,
the need for capital expenditure or the risk of senior
personnel losing their job are but some of the reasons for
these obstructions. Diplomacy becomes an essential require-
ment in the encouragement of investigations. Although tour
operators have no authority to undertake investigations in
resorts, they can arrange for consultants to inspect hotels
that have been involved in an incident. If a problem involves
more than one hotel, or is thought to have a wider
community involvement, the local health authority is
contacted and in some resorts there has been an excellent
response.
The prevention of travel-associated infections is largely
concentrated on pre-travel advice. Travel clinics and advice
from government departments (Department of Health 2000)
encourages tourists to alter their behaviour with immuniza-
tion for a few selected diseases. Dietary advice such as ‘boil it,
cook it, peel it or forget it’ as advised by Kozicki et al. (1985),
has been promulgated for many years but there is little
evidence to show that it has been effective. Indeed, it is
advice that may be very difficult to follow on package
holidays with all the food provided by a hotel. The
presentation of food dishes are often like works of art but
may contain a mixture of cooked foods and salads, the safety
of the dish relying on the preparation of the salad component.
In countries with active programmes for the prevention of
foodborne infections, the emphasis is on education and the
implementation of good food hygiene programmes based on
the HACCP principles. This in turn requires the food
preparation premises to meet required standards and a
certain level of basic education of the food handlers. The
FTO has encouraged the governments of destination
countries to develop and implement food hygiene pro-
grammes, but with limited and variable success. As a result,
part of their overall proactive health and safety programme
has been the development of a food hygiene code of practice
and auditing programme for use by their members. This is
being introduced in 2002 and will become part of the
contract between tour operators and hoteliers. It will be
complimentary to any national legislation. In the Caribbean,
a joint venture by the Caribbean Alliance for Sustainable
Tourism and the Caribbean Epidemiology Centre has
developed the Quality Tourism for the Caribbean project
that includes guidelines for food safety and sanitation (QTC
2002). They are also developing local surveillance of tourists
illnesses based on a hotel reporting system.
The World Tourism Organisation is developing an
International Food Safety Standard for the Tourism Sector
with inputs from the food section of WHO, FAO, the
hospitality industry, private consultants and tour operators.
The prevention of waterborne disease primarily depends
on the provision of a safe drinking water supply. In many
tourist areas, especially those in developing areas, this
cannot be guaranteed. Private water supplies may have little
or no control and even municipal supplies may have a level
of control that does not meet either European or American
requirements. This may be in spite of the country’s own
legislation stipulating the standards for drinking water. The
HOLIDAY FOOD AND WATER INFECTIONS 23S
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S

ambassador of a major tourist destination informed about a
meeting at which gastrointestinal illnesses were being
discussed, that his government could pass any laws that
were required and the solution was being implemented.
The surveillance, investigation and prevention of food and
waterborne infections associated with package holiday travel
raises many questions as to who is responsible legally,
morally and practically. The information available is by no
means clear and can vary rapidly with time. The tourists
expect that their health will be safeguarded, yet continue to
book holidays to destinations with a known high incidence of
food and waterborne infections. Those who work to improve
the situation do so with tools reminiscent of those available
to John Snow in the control of a cholera outbreak associated
with the Broad Street pump. Improvements have been made
and will continue to be made but require active public
private partnership and cross discipline cooperation at both
professional and political levels. The numbers of package
holiday tourists will continue to increase, as will the number
of destinations. Appropriate surveillance methods, investi-
gation facilities and preventative programmes need to be
developed in order to keep the levels of food and waterborne
infections to a minimum.
8. REFERENCES
Cartwright, R.Y. (1993) Travellers’ diarrhoea. British Medical Bulletin
49, 348–362.
Cartwright, R.Y. and Chahed, M. (1997) Foodborne diseases in
travellers. World Health Statistics Quarterly 50, 102–110.
Castelli, F. and Carosi, G. (1995) Epidemiology of traveler’s diarrhea.
Chemotherapy 41(Suppl 1), 20–32.
CDSC (1991) Communicable Disease Report 1, 149.
CDSC (2000) Communicable Disease Report 10, 285.
Consumers Association (1999) Sick leave Holiday Which, Autumn
1999, 184–197.
Department of Health (2000) Health advice for travellers. T6, London.
Farthing, M.J. (1992) Travellers’ diarrhoea. British Journal of Hospital
Medicine 48, 82–92.
Feely, E. and McKeown, P. (2002) Gastroenteritis in holidaymakers
returning from Andorra, January–February 2002. EuroSurveillance
Weekly 10, 1–2.
Food Standards Agency (2000) A Report of the Study of Infectious
Intestinal Disease in England, London.
Kozicki, M., Steffen, R. and Schar, M. (1985) ‘Boil it, cook it, peel it or
forget it’: does this rule prevent travellers’ diarrhoea? International
Journal of Epidemiology 14, 169–172.
McEvoy, M., Blake, W., Brown, D., Green, J. and Cartwright, R.
(1996) An outbreak of viral gastroenteritis on a cruise ship.
Communicable Disease Report CDR Review 6, R188–192.
Quality Tourism for the Caribbean (2002) Food safety and sanitation,
Port of Spain Trinidad.
Reid, D., Dewar, R., Fallon, R.J., Cossar, J.H. and Grist, N.R. (1980)
Infection and travel: the experience of package tourists and other
travellers. Journal of Infection 2, 365–370.
Steffen, R., Van der Linde, F., Gyr, K. and Schar, M. (1983)
Epidemiology of diarrhea in travelers. Journal of the American
Medical Association 249, 1176–1180.
Steffen, R., Collard, F., Tornieporth, N., Campbell-Forrester, S.,
Ashley, D., Thompson, S., Mathewson, J.J., Maes, E., Stephenson,
B., DuPont, H.L. and von Sonnenburg, F. (1999) Epidemiology,
etiology, and impact of traveler’s diarrhea in Jamaica. Journal of the
American Medical Association 281, 811–817.
World Health Organisation (1997) HACCP Introducing the Hazard
Analysis and Critical Control Point System. WHO/FSF/FOS/97.2.
World Tourism Organisation (2001) Tourism Highlights 2001, Madrid.
24S R.Y. CARTWRIGHT
ª 2003 The Society for Applied Microbiology, Journal of Applied Microbiology Symposium Supplement, 94, 12S–24S























![Waterborne Disease [FINAL]](https://img.pdfslide.net/doc/110x75/55a6e1d11a28ab9a558b4647/waterborne-disease-final.jpg)



