Embed Size (px)
Citation preview

Foveal cone optical density in retinitis pigmentosa
Ann E. Elsner, Stephen A. Burns, and Louis A. Lobes, Jr.
We have used a color matching technique to estimate the optical density of the foveal cone photopigments in a
group of patients with retinitis pigmentosa. We find that foveal cone optical density is reduced in patients
with retinitis pigmentosa. This reduction of density can occur early in the disease process and is found in
patients with minimal visual field loss or 20/20 visual acuity. Foveal cone optical density is highly correlated
with visual acuity and correlated with visual field area. Full-field ERG measurements are severely reducedearly in the disease before significant foveal changes occur.
1. Introduction
Retinitis pigmentosa (RP) is a group of degenerativediseases of the retina known to cause night blindness, aprogressive loss of visual field, narrowing of the retinalvasculature, and alteration of the retinal pigment epi-thelium throughout the retina.' However, despite thevitreous changes' and opacifications in the posteriorsubcapsular portion of the lens2 associated with retini-tis pigmentosa, visual acuity of 20/20 to 20/40 is oftenretained until later stages of the disease. Although itis possible to estimate the rate of progression of fieldloss once begun,3 4 it is not yet possible to determinethe long-range prognosis for macular function, e.g.,visual acuity. It has been shown that the disease af-fects both the fovea and periphery.5 The progressionof retinitis pigmentosa in the fovea is not yet wellunderstood. One substrate shown to be severely dam-aged in at least one type of retinitis pigmentosa is thephotopigment/retinal pigment epithelial complex.6
To investigate early outer retinal damage affecting thecentral area of vision, we have used noninvasive tech-niques to measure (a) the effective optical density ofphotopigment in the central 40 of vision, (b) theamount of light that bleaches one-half of the photopig-ment, and (c) the rate at which the photopigmentregenerates following a bleach.
Previously the optical density of the photopigmentin the foveal cones of patients with retinitis pigmen-tosa has been investigated with both retinal densitom-
The authors are with University of Pittsburgh, Eye and Ear Insti-tute, Ophthalmology Department, 230 Lothrop Street, Pittsburgh,Pennsylvania 15213.
Received 8 July 1986.
0003-6935/87/081378-07$02.00/0.© 1987 Optical Society of America.
etry7 8 and color matching.9 These techniques mea-sure only outer retinal function. Neither technique isaffected by later neural processing.10 For normal ob-servers the two techniques give similar estimates of thehalf-bleach illuminance and of the optical density ofthe human cone photopigments.11-16 For patientswith retinitis pigmentosa, recent studies using retinaldensitometry indicate that the cones in the central 20of the retina have optical densities less than those ofnormal observers. In retinal densitometry, the opticaldensity measurements of photopigments depend onthe difference between the amount of light reflectedfrom the retina in the bleached and unbleached states.The assumption is that the change in reflectance is dueto light absorbed by the photopigment. Stray lightthat reflects back to the detector from the lens orvitreous, without reaching the retina, results in artifac-tually low difference measurements. Since lens andvitreous changes in patients can be extensive, theseeffects could be large. To minimize these artifacts,only patients with good visual acuity were tested.7 8
Also, in contrast to retinal densitometry, color match-ing measurements are determined only by the lightabsorbed by functioning cones. A loss in the totalnumber of cones will not be detected. The color matchdepends on the spectral sensitivities of the photore-ceptors, which in turn depend on the concentration ofphotopigment and the path length of light through thephotopigment.1"12 To measure the optical density ofthe photopigments, the difference between the colormatches at low illuminance and high illuminance isobtained. By assuming the extinction spectra of thecone photopigments to be those of the average observ-er,17 the optical density is calculated.'2 At low illu-minances, a shift in the color match toward that usual-ly found at higher illuminances, e.g., thepseudoprotanomalous shift, can imply reduced opticaldensity.9 However, a change in the spectral sensitivitydue to abnormal extinction spectra or the effects of
1378 APPLIED OPTICS / Vol. 26, No. 8 / 15 April 1987

preretinal filtering can also cause a shift in colormatches. Without measuring both the low illumi-nance and high illuminance color matches, quantita-tive measurements of the optical density of cone pho-topigments cannot be obtained.1"18
We have developed two noninvasive color matchingtechniques: (1) steady-state color matching," whichmeasures the optical density of cone photopigments asa function of the steady-state retinal illuminance, and(2) dynamic color matching,13"19 which measures thechange with time of the optical density of photopig-ments following a known change in illuminance. Wecompare the results of these color matching techniqueswith those obtained by other researchers using retinaldensitometry.78 In addition, we compare the opticaldensities obtained in all three studies with results fromthree common clinical techniques used in assessingretinitis pigmentosa: visual acuity; visual fields; andthe full-field electroretinogram (ERG).
II. Method
A. Apparatus and Stimulus
The patient makes color matches using the four-channel high-illuminance Maxwellian view apparatusdescribed previously.1"12 To ensure that most pa-tients make accurate color matches we use a 40 bipar-tite field. The patient matches the color and bright-ness of a 590-nm standard light with a mixture of agreen (546-nm) and red (650-nm) primary. By turn-ing the color knob, the patient adjusts the ratio of thered vs green primaries at approximate constant lumi-nance. By turning the brightness knob, he adjusts theluminance of the red and green mixture. A computercontinuously monitors these adjustments. A dim 480-nm light minimizes the contribution of the short-wave-length sensitive cones at high retinal illuminances.Additional field sizes from 1 to 8 are available toinvestigate changes in optical density with retinal ec-centricity.'2 '2 0
The patient is aligned with the optical axis of theapparatus using infrared LEDs, a TV camera, a videomonitor, and a bite bar positioner. The patient's pupilsize and position are monitored throughout the experi-ment so that all the light from the stimulus enters thepupil. The patient's fixation is monitored throughoutthe experiment to ensure that the same central regionof vision is tested at all illuminances.
B. Steady-State Color Matching Technique
To obtain estimates of optical density as a functionof retinal illuminance, we vary the retinal illuminanceof the field in eight steps, from 260 to 130,000 trolands(Td), for patients and in nine steps, from 260 to260,000 Td, for normal control observers. Followingdiscussion of instructions and informed consent, thepatient is aligned to the apparatus. At each illumi-nance he reaches a steady state of adaptation, thenmakes ten color matches. At the end of the session,the matches are calibrated, and the log ratio of the redto green primaries, log (R/G), is computed. We fit a
cumulative normal distribution to these data" to ob-tain (a) the base line (moderate illuminance) colormatch, (b) the optical density (the difference betweenthe base line and high illuminance color match),2 ' and(c) the retinal illuminance required to bleach half ofthe photopigment, the half-bleach illuminance Io. Forone patient we measured optical densities for both eyesand additional field sizes in one eye.
C. Dynamic Color Matching Technique
To obtain the rate of change of the optical densityfollowing a change in retinal illuminance, we measurethe timing of the shift in the color match following aluminance increment or decrement. First, the patientmakes a color match at low retinal illuminance, thendark adapts for 15 min. Next the patient continuouslybrackets the color match, first too red, then too green,then too red, for 3 min (the base line period). Follow-ing this, the illuminance is abruptly increased (thebleaching period); the patient brackets the high illumi-nance color match for 6 min. The retinal illuminanceis then decreased (the regeneration period), and thepatients bracket the color match for 6 min. Typically,the highest illuminance used in the bleaching period is89,000 Td. From these data we obtain measurementsof the time required to regenerate one-half of the pho-topigment (half-time). We compute the half-time asthe time after the end of the bleaching period requiredto regenerate one-half of the difference between thebase line and bleaching period color matches. Pa-tients with greatly reduced optical density are notrecruited for this test. Those patients recruited aretested a minimum of 2 weeks following the steady-state measurements for the eye tested. Thus far, onlythree return patients have sufficient optical densityand color discrimination to obtain meaningful half-time estimates.
D. Visual Acuity, Visual Fields, and ERG
Clinical measurements of visual acuity, visual fields,and ERGs are collected by trained ophthalmic techni-cians. Visual acuity is determined using a projectedchart. Visual fields are obtained on a Goldmann pe-rimeter for several targets. We then digitize the visualfields on the PAR Microsystems IS-2000 image proces-sor. From the digitized images we compute the area(in arbitrary units) contained within each isopter, sub-tracting out scotomata and the blind spot as needed.For comparison with previous studies, we report areasfor the II 4 and I 2 isopters. For three patients inwhich there was no II 4 isopter collected because theadjacent isopters were close together, an area measure-ment was obtained by interpolation. ERGs were mea-sured using Burian-Allen electrodes and Ganzfield,white light stimulation following 35 min of dark adap-tation. The amplitude of the a wave was measured for100-,us flashes with the patient in a dark-adapted state(scotopic ERG) and with the patient in a light-adaptedstate (photopic ERG).
15 April 1987 / Vol. 26, No. 8 / APPLIED OPTICS 1379

Table 1. Patient Statistics
Optical Io FamilyP/S/age density VA (Td) II 4 area I 2 area S. ERG P. ERG history
1 4.3 18,5871 4.5 16,9821 4.5 16,0331 4.6 11,5660.80.670.670.50.50.50.4
4.65.74.4
4.74.04.0
10,1458960
13,60916,74915,061
274 0.25 0.53356 0 03356 0.1 0251 0.2 0
0 074 0 0
24997
2082688
000.330.20
00.410.670.50
The areas of the visual field isopters are in arbitrary units. The photopic ERG (P. ERG) andscotopic (S. ERG) data are the proportion of the normal a-wave amplitude. The family history iscoded as D for dominantly inherited RP, F for other members of the family affected, and S for a singlefamily member affected. The normal population means and standard deviation were: optical density= 0.27 + 0.037; Io = 4.40 ± 0.09 log Td (n = 27).
E. Patient Population
Ten patients, aged 11 to 46, were recruited (average26.6 yr); most were recently diagnosed as having retini-tis pigmentosa. All had night blindness, reduced orextinguished full-field ERGs, and fundus abnormali-ties consistent with RP. Visual acuities ranged from20/20 to 20/50; no patient had visually significant cata-racts or media opacities (see Table I). Visual fieldabnormalities ranged from a subtle constriction ofisopters to large island scotomata in the midperiphery.None of the patients has x-linked RP. Patient 6, afemale, has Usher's syndrome and a brother with RP,but no other family members have been diagnosedwith RP. Patients 7 and 8 are brother and sister withtwo brothers without RP. Patient 10 has a brotherwith RP and a sister without RP; both his parents haveseverely reduced ERG amplitudes. We compare ourresults to a population of twenty-seven normal observ-ers, aged 18-47 yr (average 30 yr)."
Ill. Results
A. Optical Density
For every retinitis pigmentosa patient the opticaldensity of the photopigments in the central 4° of visionis less than the average optical density for normalobservers, which is 0.27 with a standard deviation of0.037. This is shown in Figs. 1-4. At moderate retinalilluminances retinitis pigmentosa patients requiremore of the red primary in the mixture to match thestandard than do normals. This shift in the colormatch has been called a pseudoprotanomalous shift.The optical densities2 ' range from 0.244 (about 1 stan-dard deviation below average) to dilute (see Table I).Nine of ten patients had significantly less optical den-sity than the average of normal observers [seven with p<0.01 and two with p <0.05 (Ref. 22)].
To test whether a patient with a decreased opticaldensity still had the highest optical density at thefovea, we measured the change in the color match with
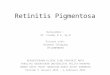
field size'2'20 in a patient with 20/20 visual acuity andno family history of RP. Additional field sizes of 8, 2,and 1 (Fig. 1) were tested. The difference betweenfield sizes was similar to that of normal observers with-all field sizes yielding somewhat lower optical densitiesthan measurements on normal observers.12 Thus inthis patient there appears to be a generalized loss ofphotopigment over at least the central 80 rather than aloss localized to the central fovea.8
The optical density was reduced even for patientswith only mild constriction of visual fields (Figs. 1 and2) or 20/20 visual acuity (Figs. 1, 3, and 4). Thus thechange in optical density in the central 40 of visionoccurs early in the disease progression.
B. Comparison of Optical Density to Visual Acuity, VisualFields, and ERG
Visual acuity and optical density were highly corre-lated with the patients with the best visual acuitytending to have the highest optical density: r = 0.713(p <0.01).23 The area of visual field for the I 2 isopterwas also significantly correlated with optical density, r= 0.621 (p <0.05). While optical density was alsopositively correlated with the II 4 isopter area, thiscorrelation did not reach significance. In the eightpatients who had recent visual fields, all had visualfield defects, ranging from subtle isopter constrictionin patients 1 and 6 to obvious field defects in six otherpatients. Only patient 9 had a partial central fielddefect.
No other correlations were significant. All the pa-tients in our study had ERG amplitudes that wereextinguished or severely reduced with respect to ourclinical norms. Thus we did not find a positive corre-lation of optical density with the a-wave amplitude ofeither the photopic ERG or the scotopic ERG. Sincethe waveforms of most patients were essentially flat,the use of other measurements such as the b-waveamplitude would not increase the correlations.
1380 APPLIED OPTICS / Vol. 26, No. 8 / 15 April 1987
1/F/402/F/222/F/233/F/124/M/215/M/466/F/227/M/258/F/209/M/44
10/M/14
0.1510.2440.2190.1880.1860.0780.09600.0510.0880.131
DSSSSDFFFFF

I I I
LE)
3 .10.1
01f n
-0.3 _
2.0 3.0 4.3 5.3
Log TdFig. 1. Average color match as a function of retinal illuminance inTrolands for the left eye, I and right eye, * of patient 2. Log (R/G)is the log ratio of the red to green primaries in the mixture required tomatch a 590-nm standard light. Dashed lines indicate +2 standarddeviations of the average of normal observers. Additional symbols
indicate color matches for 1°, O, 20, a and 80 0.
0.
3.1
LD
3.1010
-0.I
2.0 3.0
Log Td4.0 5.0
a.
-e~~~ X17 1 1
2.3 3.3 4.3 5.0
Log TdFig. 3. Average color match (squares) as a function of retinal illu-
minance for patient 1. Scale and dashes as in Fig. 1.
010-
2.3 3.8 4.0 5.3
Log TdFig. 4. Average color match (squares) as a function of retinal illu-
minance for patient 3. Scale and dashes as in Fig. 1.
Fig. 2. Average color match, *, as a function of retinal illuminancefor patient 6. Scale and dashes as in Fig. 1.
C. Half-Bleach Illuminance
Most patients had half-bleach illuminances that didnot differ from those of the normal observers, whichaveraged 4.4 log Td with a standard deviation of 0.088.Two patients had half-bleach illuminances less thannormal (p <0.01), and three had half-bleach illumin-ances greater than normal (p <0.01 for two patientsand p <0.05 for one patient). Patients 1, 3, 4, and 6had significantly lower than normal optical densitiesbut normal values for Io (see Figs. 2-4). The opticaldensity was so low in patient 7 that an estimate of thehalf-bleach illuminance could not be computed.
D. Dynamic Color Matching Results
The time required to regenerate one-half of the pho-topigment (half time) is 144 s for the right eye ofpatient 2 and 139 s for patient 3, who has lower opticaldensity. Note that both these patients have normal Iovalues. These measurements are somewhat longerthan our typical measurements but fall within therange of our normal observers for these conditions.'4Patient 5, who has a significantly higher than normalIo, has a half-time of 68 s.
If the regeneration of the RP patients were extreme-ly slow, it would be possible to attribute the lowerdensity measurements to partial bleaching at our low-
0. 1
a: 0.0
0I0
-0..
0 1 2
TIME (min)
0.1 r
E 0.0
0
-0.
3 0 1 2
TIME (mIn)3
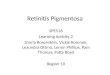
Fig. 5. Color match as a function of time for a 5500-Td lightfollowing 15 min of dark adaptation for patient 5 (top curve, left), anormal observer (bottom curve, left), and a patient with central
serous retinopathy (right).
est retinal illuminances. In central serous retinopathywe have measured a low optical density that we attri-bute to very slow regeneration; consequently there isbleaching of the cone photopigments at abnormallylow retinal illuminances. None of the three RP pa-tients tested with the dynamic color matching tech-nique showed evidence of bleaching at abnormally lowretinal illuminances. However, to test for this possi-bility we performed an additional experiment. Pa-tient 5 and a central serous patient of similar age andvisual acuity were each dark adapted for 15 min priorto test. Figure 5 shows the results for each patient
15 April 1987 / Vol. 26, No. 8 / APPLIED OPTICS 1381
-//
//
l
/X/
/ - --- --
/
- - - -_ - - - /
I I _
I I
4. . ,
0.4 0.4 J I I
.

together with a normal control. During the period ofdark adaptation the central serous patient was able toregenerate additional photopigment, while the RP pa-tient was not. Once the 5500-Td field was presented,the optical density decreased for the central serouspatient but not for the RP patient. Similar to the RPpatient, a normal observer shows no evidence ofbleaching at 5500 Td, even for a 15-min presentation.This experiment was repeated for both patients, butwith the central serous patient tested at a lower retinalilluminance (260 Td) to control for the higher Io in theRP patient. Again the central serous patient bleachedat a low retinal illuminance (260 Td), but the RPpatient did not bleach at 5500 Td. This experimentsupports the hypothesis that the RP patients havelower optical densities due to factors other than therate of regeneration of the cone photopigments.
IV. Discussion
A. Optical Density and Half-Bleach Illuminance
The optical density of RP patients, in agreementwith previous studies,7-9 was less than that of normalobservers. According to Beer's law, F(X) = 110-a(X)c(see Ref. 11), where F(X) is the absorption spectrum,a(X) is the extinction spectrum of the pigment, c is theconcentration of pigment, and is the path length oflight through the pigment. Thus, with a color match-ing technique, changes in optical density depend ononly the concentration of the photopigment and thepath length of light through the photopigment. Recallthat the low illuminance color matches are shiftedupward from those of normal observers for all of ourRP patients. In contrast, the high-illuminance colormatches, which are made with dilute concentrations ofphotopigments for both normal observers and pa-tients, do not differ. Thus a change in optical densitydoes not reflect changes in a(X) between patients andnormal observers. Recall also that a reduction in thenumber of photoreceptors will not change the colormatch, since only functioning cones contribute to thematch.
In our testing conditions a reduction in the mea-sured optical density could be caused by at least threedifferent factors": shortened or otherwise damagedcones; cones oriented obliquely to the path of the inci-dent light; and abnormal photopigment regeneration.We will now discuss data that support the first twofactors and indicate for which data the third may alsobe a possibility.
The first two factors are types of structural change inthe cones. Cones that are shortened or damaged sothat they contain either a lowered concentration ofphotopigment or shortened outer segments must havelower than normal optical density. The second struc-tural factor that may contribute to the decreased opti-cal density measured at low retinal illuminances is thealignment of the cones. If the cones are alignedobliquely to the optical path of the incident light, adecreased optical path length results as well as sensi-tivity changes due to the Stiles-Crawford effect.24
Thus less light is absorbed, and the effective opticaldensity is decreased. Also, since less light is absorbed,more light is required to bleach the photopigmentsresulting in higher Io values. As can be seen in Table I,three RP patients have higher than normal values of Io.These patients should show a generalized loss of sensi-tivity to light. A foveal sensitivity loss (more lightrequired to detect a target) has been demonstrated inRP patients7 2 5 ; since there is less effective opticaldensity, there is a decreased ability of the photorecep-tors to catch quanta. It should be noted that otherstructural factors could cause a sensitivity loss withoutnecessarily decreasing the path length and thus theoptical density.26 Our technique cannot distinguishbetween changes in path length and changes in concen-tration.
The third factor, a photopigment kinetic defect, isnot necessarily related to cone structure. If the photo-pigment is regenerated more slowly in the RP patientthan in normal observers, less light is required tobleach photopigment. This may be the cause of theabnormally low values of Io found in two patients.Slowed photopigment regeneration could mask a sen-sitivity defect in some conditions. In patients with akinetic defect, a dim light could bleach appreciableamounts of photopigment. This would not be the casefor patients with only structural defects in their cones.As discussed in the results, we have seen evidence ofthis in central serous patients but not in RP patients.We will further investigate this possibility by perform-ing dynamic color matching on patients with low val-ues of Io. Thus it is possible to begin to determine thefactors underlying the decreased optical density foundearly in the central 40 of patients with RP.
B. Comparisons with Previous Studies
As stated in Sec. I, we are examining the relation ofoptical density in the central region of vision withclinical measures, such as visual acuity, visual fields,and full-field ERG. We want to determine whetherthe visual acuity loss, so detrimental to patients, isrelated to mechanisms underlying decreased opticaldensity. Also, if the degeneration is operating over theentire retina early in the disease, we should see evi-dence of this. Although the visual field and full-fieldERG measurements depend on sensitivity to light anda sensitivity loss can be due to factors other thandecreased optical density, these measurements arereadily available in most centers.
We compared our results to results of two recentstudies7 8 to investigate the relation between opticaldensity and visual acuity, visual field area, and full-field ERG responses. The similarities across studiesincluded (a) lower than average optical density formany RP patients, (b) visual acuity better than 0.5 formost patients, (c) a similar range of visual field areasobtained with Goldmann perimeters at specifiedisopters, and (d) ERG amplitudes reported with re-spect to established norms. The main differences are(a) the pattern of inheritance, (b) the method of ob-taining measures of cone photopigment concentration,
1382 APPLIED OPTICS / Vol. 26, No. 8 / 15 April 1987

and (c) the visual field isopters tested. In our study,there were only two cases of dominant inheritance, onecase of Usher's syndrome, and no confirmed cases of x-linked inheritance. Similarly, in the study of van Meeland van Norren7 there was only one case of dominantinheritance, although there were some potential casesof x-linked inheritance. In contrast, the Kilbride etal. 8 study had several cases of dominant inheritance.Our method of obtaining cone photopigment concen-tration is color matching."" 2 In contrast, cone photo-pigment concentration is measured by imaging densi-tometry by Kilbride et al. 8 and by nonimagingdensitometry by van Meel and van Norren. Visualfield areas were reported for both the II 4 and I 2isopters in our study, the II 4 only in the Kilbridestudy, and mainly the I 2 in the van Meel and vanNorren study. Thus differences among studies maybe due to both differences in method and/or differ-ences in patient populations.
1. Cone Optical DensityAll studies report lower optical densities for most
retinitis pigmentosa patients than for normal observ-ers. Kilbride et al., but not van Meel and van Norren,examined the effect of retinal locus on optical density.With our method and normal observers, we previouslyreported an increase of optical density with decreasingfield size for normal observers.'2 In this study, wefound a similar increase in optical density with fieldsize for a patient with no family history of RP, patient 2(see Fig. 1). In contrast, Kilbride et al. found a smallerthan normal change with field size for recessive RP andUsher's syndrome patients.
2. Visual AcuityIn agreement with our findings, visual acuity was
significantly correlated with the estimate of opticaldensity in the van Meel and van Norren study as wellas the Kilbride et al. study (p <0.01 for the van Meeland van Norren studies and the 2-3° annulus data ofKilbride et al. and p <0.05 for the central 2 and 1-2°annulus data of Kilbride et al.23 ).
3. Visual FieldsIn agreement with our study, Kilbride et al. found a
significant correlation with visual field area and opti-cal density for their central 2° data [p <0.01 (Ref. 23)].While the visual field area vs optical density correla-tion coefficients was positive for the two other condi-tions in the Kilbride et al. study as well as in the vanMeel and van Norren study, none was statisticallysignificant. It should be noted that in both studies novisual field data were reported for some patients,thereby reducing the sample size and the chance toreach statistical significance.
4. Full-Field ERGMost of the patients in our study had severely re-
duced or extinguished scotopic and photopic ERGs.Similarly, the patients in the van Meel and van Norrenstudy had severely reduced or extinguished scotopic
ERG b-wave amplitudes. The correlation betweenmeasures of the ERG amplitude and optical densitywas not statistically significant in either study. Incontrast, some patients in the Kilbride study had nor-mal scotopic or photopic ERGs. The correlation be-tween scotopic ERG amplitude and optical densitywas statistically significant only in a 1-2° annuluscondition in the Kilbride et al. study (p <0.01). Thecorrelation between photopic ERG amplitude and op-tical density was statistically significant only in the 2-30 annulus condition (p <0.05). The other four corre-lation coefficients were not statistically significant.Clearly the correlation between optical density andclinical ERG does not hold under all methods andpatient populations. Thus it is difficult to determinewhether ERG amplitudes are well-correlated with op-tical density in the central region of vision. Morequantitative ERG techniques may yield better infor-mation in understanding disease mechanisms.
V. Conclusion
Photopigment optical density is reduced early in thecourse of RP. The mechanisms underlying this reduc-tion can be investigated using steady-state and dy-namic color matching. We have shown that somepatients have significantly reduced optical densitywithout having significant changes in photopigmentkinetics; structural changes in the fovea seem a morelikely explanation for the reduced optical density forthese early foveal changes. While visual acuity andvisual field changes3 may be of predictive value formacular function, the full-field ERG, as used clinical-ly, may not because it is severely reduced early in thecourse of the disease.
We thank Joseph Warnicki for his assistance in digi-tizing the visual, fields. This research was supportedby NIH NEI EYO-4395 and by Research to PreventBlindness.
References1. D. Finklestein and R. W. Massof, "Status of the Wilmer Insti-
tute Retinitis Pigmentosa Center," in Management of Retinaland Vascular Disorders, S. L. Fine and S. L. Owens, Eds. (Wil-liams and Wilkins, Baltimore, 1983).
2. S. Merin, "Cataract Formation in Retinitis Pigmentosa," BirthDefects 18, 187 (1982).
3. R. Massof, J. Sunness, R. Palmer, T. Emmel, and D. Finklestein,"Unilateral and Asymmetric Retinitis Pigmentosa: Character-istics and Natural History," Invest. Ophthalmol. Vision Sci.Suppl. 26, 128 (1985).
4. E. L. Berson, M. A. Sandberg, B. Rosner, D. G. Birch, and A. H.Hanson, "Natural Course of Retinitis Pigmentosa over a Three-Year Interval," Am. J. Ophthalmol. 99, 240 (1985).
5. R. W. Massof, D. Finklestein, S. J. Starr, K. R. Kenyon, J. A.Fleischman, and I. H. Maumenee, "Bilateral Symmetry of Vi-sion Disorders in Typical Retinitis Pigmentosa," Br. J. Ophthal-mol. 63, 90 (1979).
15 April 1987 / Vol. 26, No. 8 / APPLIED OPTICS 1383

6. R. B. Szamier, E. L. Berson, R. Klein, and S. Meyers, "Sex-Linked Retinitis Pigmentosa: Ultrastructure of Photorecep-tors in Pigment Epithelium," Invest. Ophthalmol. Vision Sci.18, 145 (1979).
7. G. J. van Meel and D. van Norren, "Foveal Densitometry inRetinitis Pigmentosa," Invest. Ophthalmol. Vision Sci. 24, 1123(1983).
8. P. E. Kilbride, M. Fishman, G. A. Fishman, and L. P. Hutman,"Foveal Cone Pigment Density Difference and Reflectance inRetinitis Pigmentosa," Arch. Ophthalmol. 104, 220 (1986).
9. R. S. L. Young and G. Fishman, "Color Matches of Patients withRetinitis Pigmentosa," Invest. Ophthalmol. Vision Sci. 19, 967(1980).
10. Color matching could be influenced by later neural processing inthat color discrimination becomes worse, but discrimination isusually good in patients with good visual acuity. Retinal densi-tometry could be influenced by later neural damage if the dam-aged neurons scattered light. Again this is unlikely in patientswith good visual acuity.
11. S. A. Burns, A. E. Elsner, L. A. Lobes, Jr., and B. H. Doft, "APsychophysical Technique for Measuring Cone PhotopigmentBleaching," Invest. Ophthalmol. Vision Sci. (in press).
12. S. A. Burns and A. E. Elsner, "Color Matching at High Illumin-ances: the Color-Match-Area Effect and Photopigment Blea-ching," J. Opt. Soc. Am. A 2, 698 (1985).
13. A. E. Elsner and S. A. Burns, "Factors Influencing Photopig-ment Kinetics," Invest. Ophthalmol. Vision Sci. Suppl. 27, 74(1986).
14. M. Alpern, "Lack of Uniformity in Colour Matching," J. Physiol.288, 85 (1979).
15. G. Wyszecki and W. S. Stiles, "High-Level Trichromatic ColorMatching and the Pigment-Bleaching Hypothesis," Vision Res.20, 23 (1980).
16. V. C. Smith, J. Pokorny, and D. V. Norren, "DensitometricMeasurements of Human Cone Photopigment Kinetics," VisionRes. 23, 517-524 (1983).
17. V. C. Smith, J. Pokorny, and S. J. Starr, "Variability of ColorMatching Data. I. Interobserver Variability in the Unit Coor-dinates," Vision Res. 16, 1087 (1976).
18. In contrast, measurements at both high and low retinal illumin-ances are still preferable but not essential in following a patientwho is improving over time or who has one eye that can serve as agood control for the other eye.
19. S. A. Burns, A. E. Elsner, L. A. Lobes, Jr., and B. H. Doft,"Psychophysical Techniques for Investigating Cone Kinetics,"in Technical Digest, Noninvasive Assessment of Visual Func-tion (Optical Society of America, Washington, DC, 1985), paperTuAl.
20. J. Pokorny and V. C. Smith, "The Effect of Field Size on Red-Green Color Mixture Equations," J. Opt. Soc. Am. 66, 705(1976).
21. The optical density is actually computed from the differencebetween high and low illuminance color matches according to aset of nonlinear equations. However, since over the range ofoptical densities obtained experimentally, this equation is wellapproximated by a linear dependence. We use the linear ap-proximation in this paper. References 11 and 12 provide fur-ther details.
22. Using a t distribution, we formed confidence limits based on ournormal population."1 We determined the extent to which eachpatient's parameters differed from normal. We expected theoptical density of RP patients to be less than normal (one-tailedtest). However, we expected that the half-bleach illuminance Iocould be either higher or lower than that of normal observers(two-tailed test).
23. We determined the significance of the Pearson product momentcorrelation coefficient by the formula t = [r (n - 2)1/2]/(I - r2)1/2,with n degrees of freedom, where n = the number of observationsin the correlation. W. Mendenhall and M. Ramsey, Statisticsfor Psychology (Duxbury, North Scituate, MA, 1973).
24. D. G. Birch, M. A. Sandberg, and E. L. Berson, "The Stiles-Crawford Effect in RP," Invest. Ophthalmol. Vision Sci. 22,157(1982).
25. K. R. Alexander, L. P. Hutman, and G. A. Fishman, "Dark-Adapted Foveal Thresholds and Visual Acuity in Retinitis Pig-mentosa," Arch. Ophthalmol. 104, 390 (1986).
26. A. E. Elsner, S. A. Burns, L. A. Lobes, Jr., and B. H. Doft, "ConePhotopigment Bleaching Abnormalities in Diabetes," Invest.Ophthalmol. Vision Sci. (in press).
SHORT COURSE OFFERED ON LASER MEASUREMENTSNBS is sponsoring a 3-day course (May 12-14) in the concepts,techniques, and apparatus used in measuring laser parameters,emphasizing the measurement of power, energy, and pulsecharacteristics. The course, offered in Colorado Springs,Colo., will be taught by laser experts from academia,industry, and NBS and other government agencies. Students areexpected to have a degree in physics or electricalengineering, preferably with some experience in using lasers.The fee for the course is $595. For registration (deadline
April 3) contact: Kent Zimmerman, Office of ConferenceServices, Campus Box 153, University of Colorado, Boulder,Colo. 80310-0153, telephone: 303/492-5151.
1384 APPLIED OPTICS / Vol. 26, No. 8 / 15 April 1987