Diapositiva 1
Closed fracture middle right claviclePRESENTED BY : Nur Raisah
UlfahC111 09 382ADVISOR : dr. M. Arief Faisal dr. Padlan
SUPERVISOR :dr. Zulfan Oktasatria Siregar,
Sp.OTIDENTITYName:H.S.C.Age:56 years old / MaleAdmission:March
16th, 2015 at 17.59Registration:71 60
32Status:JKDAUTOANAMNESISChief Complain : Pain at right
shoulderSuffered since 12 hours before admitted to Wahidin General
Hospital due to motor vehicle accident.Patient was riding
motorcycle, then hit a cow in front of him and fell down to the
right side. The exact mechanism of injury was unclear.History of
loss of conciousness (-), vomiting (-).Prior treatment at Bulukumba
Hospital.Patient is tailor and right handed .PRIMARY
SURVEYA:ClearB:RR 18 x/min, spontaneous, thoracoabdominal typeC:BP
130/80 mmHg, HR 78 x/min strong, regularD:GCS 15 (E4M6V5), pupil
isochoric, diameter 3 mm/3mm, light reflex +/+E:T: 36,8 oCSECONDARY
SURVEYRight Shoulder RegionLook:Deformity (+), Swelling (+),
Hematome (+), Wound (-)Feel:Tenderness (+)NVD : Sensibility is
good, pulsation of radial artery is palpable, CRT < 2Move
:
Active and passive motions of shoulder joint can not be
evaluated due to painCLINICAL FINDINGS
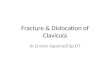
RADIOLOGY FINDINGS
LABORATORY FINDINGSItemResultNormal
RangeWBC9,64,00-10,0RBC4,34,00-6,00HGB13,112,0-16,0HCT3937,0-48,0PLT201150-400CT7004-10BT2301-7HBsAgNon
ReactiveNon ReactiveDIAGNOSISClosed Fracture Middle Right
ClavicleMANAGEMENTIVFDAnalgesicApply arm sling at right upper
extremityConservative Treatment10
DiscussionINTRODUCTIONSolomon L, et all. Apleys System of
Orthopaedics and Fractures. Ninth Edition. London : Hodder Arnold.
2010; p.687, 772-5.
EpidemiologyClavicle fractures account for approximately 4% of
all fractures and 35% to 43% of shoulder girdle injuriesMiddle
third fractures account for 80% of all clavicle fractures, whereas
fractures of the lateral and medial third of the clavicle account
for 15% and 5%, respectively.Finkemeier, CG. Fracture and
Dislocation of the Shoulder Girdle and Humerus. In: Chapman M,
Szabo RM, Marder R, Vince KG, et al. Ed. Chapmans Orthopedic
Surgery Third Edition. New York: Lippincott Williams &
Wilkins.2001. P432-80Egol KA, Koval KJ, Zuckerman JD. Clavicle
Fracture. In Handbook of Fracture. Philadelphia:Wolters Kluwer.
2010. P143-9
Anatomy
Netter, F. Atlas of Human Anatomy 6th edition18
Mechanism of TraumaEgol KA, Koval KJ, Zuckerman JD. Clavicle
Fracture. In Handbook of Fracture. Philadelphia:Wolters Kluwer.
2010. P143-919CLINICAL FINDINGSPatients usually present with
splinting of the affected extremity, the arm adducted across the
chest and supported by the contralateral hand to unload the injured
shoulder.The proximal fracture end is usually prominent and may
tent the skin. Assessment of skin integrity is essential to rule
out open fracture.Up to 9% of patients with clavicle fractures have
additional fractures,most commonly rib fractures.Most brachial
plexus injuries are associated with proximal third clavicle
fractures (traction injury).
20CLASSIFICATION (ALLMAN)Group l: fracture of the middle third
(80%). This is the most common fracture in both children and
adults; proximal and distal segments are secured by ligamentous and
muscular attachments.
Group ll: fracture of the distal third (I5%). This is
subclassified according to the location of the coracoclavicular
ligaments relative to the fracture
Group lll: fracture of the proximal third(5%). Minimal
displacement results if the costoclavicular ligaments remain
intact. It may represent epiphyseal injury in children and
teenagers.Finkemeier, CG. Fracture and Dislocation of the Shoulder
Girdle and Humerus. In: Chapman M, Szabo RM, Marder R, Vince KG, et
al. Ed. Chapmans Orthopedic Surgery Third Edition. New York:
Lippincott Williams & Wilkins.2001. P432-80Egol KA, Koval KJ,
Zuckerman JD. Clavicle Fracture. In Handbook of Fracture.
Philadelphia:Wolters Kluwer. 2010. P143-9Subtype Group IIType l:
Minimal displacement: interligamentous fracture between the conoid
and trapezoid or between the coracoclavicular and AC ligaments;
ligaments still intact Type ll: Displaced secondary to a fracture
medial to the coracoclavicular ligaments: higher incidence of
nonunionllA: Conoid and trapezoid attached to the distal
segmentllB: Conoid torn, trapezoid attached to the distal segment
Type lll: Fracture of the articular surface of the AC joint with no
ligamentous injury: may be confused with first-degree AC joint
separation Finkemeier, CG. Fracture and Dislocation of the Shoulder
Girdle and Humerus. In: Chapman M, Szabo RM, Marder R, Vince KG, et
al. Ed. Chapmans Orthopedic Surgery Third Edition. New York:
Lippincott Williams & Wilkins.2001. P432-80Egol KA, Koval KJ,
Zuckerman JD. Clavicle Fracture. In Handbook of Fracture.
Philadelphia:Wolters Kluwer. 2010. P143-9
Tipe I: pergeseran minimal. Fraktur antara ligamen conoid dan
trapezoid atau diantara coracoclaviculer dengan ligamen
acromioclavicular. Ligamen tetap intak. (gambar 6A)Tipe II.
Pergeseran sekunder medial dari ligamen coracoclaviculer. Insidens
dari nonunion tinggi.IIA. Conoid dan trapezoid masih terhubung pada
segmen distal (Gambar 7A)IIB: Conoid ruptur, trapezoid masih
terhubung dengan segmen distal (gambar 7B)Tipe III. Fraktur pada
permukaan sendi dari acromioclavicular dan tidak ada kerusakan
ligamen. Dapat sulit dibedakan dengan terputusnya ligamen
acromioclavicular. (gambar 6B)Tipe IV. Ligamen tetap terhubung pada
periosteum, (anak-anak) dengan pergeseran dari fragmen proximalTipe
V . Fraktur Cominutif, ligamen tidak terhubung pada fragmen
proximal maupun distal, namun pada fragmen ketiga.
22Subtype Group IIIType l: Minimal displacementType ll:
DisplacedType lll: IntraarticularType lV: Epiphyseal separationType
V: Comminuted
TREATMENT (OPERATIVE)Indication for Operative treatment:Open
FractureFracture that threaten the overlying skin (rare)Fracture
that widely displaced (>2cm)Fracture associated in neurovascular
compromiseFracture in multiply injured patientsIpsilateral upper
extremity injuries needing early mobilizationLower Extremity
injuries requiring crutch walkingFracture in patients with
neuromuscular diseaseSymptomatic bump at union site, hyperthrophic
callusFinkemeier, CG. Fracture and Dislocation of the Shoulder
Girdle and Humerus. In: Chapman M, Szabo RM, Marder R, Vince KG, et
al. Ed. Chapmans Orthopedic Surgery Third Edition. New York:
Lippincott Williams & Wilkins.2001. P432-80Egol KA, Koval KJ,
Zuckerman JD. Clavicle Fracture. In Handbook of Fracture.
Philadelphia:Wolters Kluwer. 2010. P143-9Indication of surgical
treatment:
Fracture SpecificDisplacement >2 cmShortening >2
cmIncreasing comminution (>3 fragments)Segmental fracturesOpen
fracturesImpending open fractures with soft tissue
compromiseObvious clinical deformity (usually associated with items
1 and 2)Scapular malposition and winging on initial examination
TREATMENT Non operatif Most minimally displaced clavicle
fractures can be successfully treated non operatively with some
form of immobilization.In general, immobilization is used for 4 to
6 weeks.ConservativeOperative
Immobilization (Mitella/ arm sling)
Open Reduction Internal fixation-plate fixation-intramedullary
fixation
MANAGEMENTSolomon. L. et al. Injurys of the Knee and Leg in
Apleys System of Orthopaedics and Fractures 9th Edition. UK:
Arnold. 2010.COMPLICATIONEarly:Neurovascular
CompromisePneumothoraxLate:MalunionNonunionPosttraumatic
arthritisCole A, Pavlou P, Warwick, D. Injuries of the Shoulder,
Upper arm, and Elbow In:Solomon L, Wawick D, Nayagam, S Ed.Apleys
System of Orthopaedic and Fractures. London:Hodder Arnold. 2010.
733-66.Neurovascular compromise: This is uncommon and can result
from either the initial injury or secondary to compression of
adjacentstructures by callus andor residual deformity. Subclavian
vessels are at risk with superior plating.Malunion: This may cause
a bony prominence and may be associated with poorer DASH scores at
one year.Nonunion: The incidence of nonunion following clavicle
fractures ranges from 0.1% to I3.0Vo, with 85% of all nonunions
occurring inthe middle third. tr Factors implicated in the
development of nonunions of the clavicle include (l) severify of
initial trauma (open wound), (2) ex-tent of displacement of
fracture fragments, (3) soft tissue interposition, (4) refracture,
(5) inadequate period of immobihzation, and (6) primary open
reduction and internal fixation.Posttraumatic arthritis: This may
occur after intraarticular injuries to the sternoclavicular or AC
joint.28