Embed Size (px)
Citation preview
British Journal of Plastic Surgery (1983) 36, 348-349 0 1983 The Trustees of British Association of Plastic Surgeons
Free flap neo-vascularisation: case report K. 0. ROTHAUS and R. D. ACLAND
Division of Plastic and Reconstructive Surgery, Department of Surgery, University of Louisville, Louisville, Kentucky, USA
Summary-This report records the unusual occurrence of occlusion of the artery of a free flap on the ninth post-operative day. Careful clinical observation strongly suggested that good neo-vascularisation had already occurred at this early date. The pattern of capillary refill suggested that neo-vascularisation originated from the periphery of the recipient site. The decision was made not to re-explore the flap vessel. The flap survived.
Smith (1961) demonstrated clinically that special- the minimum period for survival dependent on ised small flaps might survive if their pedicles were neo-vascularisation alone ranges from 4-7 days divided quite early and partial survival of free flaps (Acland, 1975; Serafin et al., 1977: Tsur et al., with vascular interruption has been reported at 10 1980). days (Serafin et al., 1977). In experimental models, This report presents a case where a free skin flap
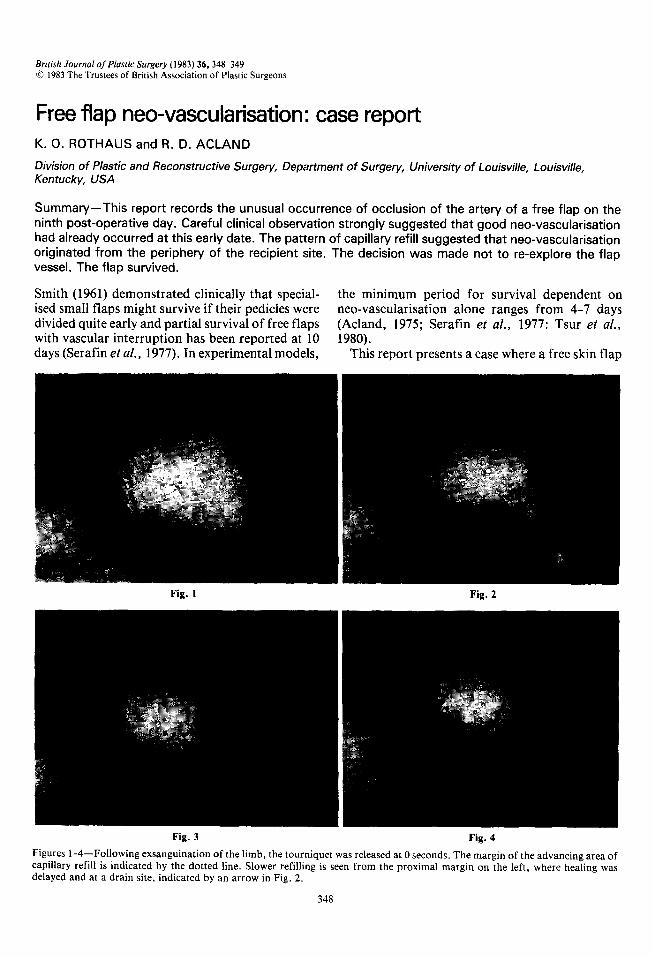
Fig. 1 Fig. 2
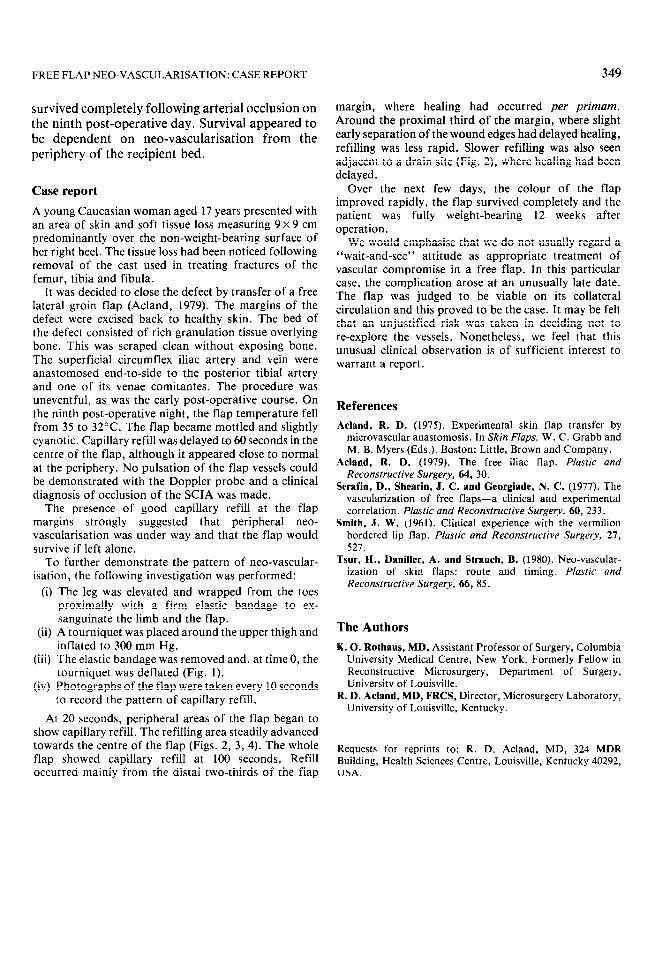
Fig. 3 Fig. 4
Figures 1-4-Following exsanguination of the limb, the tourniquet was released at 0 seconds. The margin of the advancing area of capillary refill is indicated by the dotted line. Slower refilling is seen from the proximal margin on the left, where healing was delayed and at a drain site, indicated by an arrow in Fig. 2.
348
FREE FLAP NEO-VASCULARISATION: CASE REPORT
survived completely following arterial occlusion on the ninth post-operative day. Survival appeared to be dependent on neo-vascularisation from the periphery of the recipient bed.
Case report
A young Caucasian woman aged 17 years presented with an area of skin and soft tissue loss measuring 9 x 9 cm predominantly over the non-weight-bearing surface of her right heel. The tissue loss had been noticed following removal of the cast used in treating fractures of the femur, tibia and fibula.
It was decided to close the defect by transfer of a free lateral groin flap (Acland, 1979). The margins of the defect were excised back to healthy skin. The bed of the defect consisted of rich granulation tissue overlying bone. This was scraped clean without exposing bone. The superficial circumflex iliac artery and vein were anastomosed end-to-side to the posterior tibia1 artery and one of its venae comitantes. The procedure was uneventful, as was the early post-operative course. On the ninth post-operative night, the flap temperature fell from 35 to 32°C. The flap became mottled and slightly cyanotic. Capillary refill was delayed to 60 seconds in the centre of the flap, although it appeared close to normal at the periphery. No pulsation of the flap vessels could be demonstrated with the Doppler probe and a clinical diagnosis of occlusion of the SCIA was made.
The presence of good capillary refill at the flap margins strongly suggested that peripheral neo- vascularisation was under way and that the flap would survive if left alone.
To further demonstrate the pattern of neo-vascular- isation, the following investigation was performed:
(i) The leg was elevated and wrapped from the toes
(ii)
(iii)
(iv)
proximally with a firm elastic bandage to ex- sanguinate the limb and the flap. A tourniquet was placed around the upper thigh and inflated to 300 mm Hg. The elastic bandage was removed and, at time 0, the tourniquet was deflated (Fig. 1). Photographs of the flap were taken every 10 seconds to record the pattern of capillary refill.
At 20 seconds, peripheral areas of the flap began to show capillary refill. The refilling area steadily advanced towards the centre of the flap (Figs. 2, 3, 4). The whole flap showed capillary refill at 100 seconds. Refill occurred mainly from the distal two-thirds of the flap
349
margin, where healing had occurred per primam. Around the proximal third of the margin, where slight early separation of the wound edges had delayed healing, refilling was less rapid. Slower refilling was also seen adjacent to a drain site (Fig. 2), where healing had been delayed.
Over the next few days, the colour of the flap improved rapidly, the flap survived completely and the patient was fully weight-bearing 12 weeks after operation.
We would emphasise that we do not usually regard a “wait-and-see” attitude as appropriate treatment of vascular compromise in a free flap. In this particular case, the complication arose at an unusually late date. The flap was judged to be viable on its collateral circulation and this proved to be the case. It may be felt that an unjustified risk was taken in deciding not to re-explore the vessels. Nonetheless, we feel that this unusual clinical observation is of sufficient interest to warrant a report.
References
Acland, R. D. (1975). Experimental skin flap transfer by microvascular anastomosis. In Skin Flaps. W. C. Grabb and M. B. Myers (Eds.). Boston: Little, Brown and Company.
Acland, R. D. (1979). The free iliac flap. Phstic and Reconstructive Surgery, 64, 30.
Serafin, D., Shearin, J. C. and Georgiade, N. C. (1977). The vascularization of free flaps-a clinical and experimental correlation. Plastic and Reconstructive Surgery, 60, 233.
Smith, J. W. (1961). Clinical experience with the vermilion bordered lip flap. Plastic and Reconstructive Surgery, 27, 527.
Tsur, H., Daniller, A. and Strauch, B. (1980). Neo-vascular- ization of skin flaps: route and timing. Plastic and Reconstructive Surgery, 66, 85.
The Authors
K. 0. Rothaus, MD, Assistant Professor of Surgery, Columbia University Medical Centre, New York. Formerly Fellow in Reconstructive Microsurgery, Department of Surgery, University of Louisville.
R. D. Acland, MD, FRCS, Director, Microsurgery Laboratory, University of Louisville, Kentucky.
Requests for reprints to: R. D. Acland, MD, 324 MDR Building, Health Sciences Centre, Louisville, Kentucky 40292, USA.





























