Embed Size (px)
Citation preview
522 JOSEPH W. HALLETT AND IRVING H. LEOPOLD
TRAUMATIC INFECTED CORNEAL ULCER
Two cases, each resulting from human fingernail scratches and each positive for nonhemolytic Staph, albus, responded efl^ec-tively in six and eight days respectively.
PROPHYLACTIC TREATMENT
The ointment was applied to 47 eyes following removal of corneal foreign bodies, chalazions, small lid growths, aberrant cilia, or after lacrimal probing. No undue reaction or secondary infection was encountered. Nineteen other patients had the ointment instilled for one to eight days prior to intraocular or strabismus surgery without the occurrence of postoperative infection.
LOCAL REACTIONS
There are described herein a total of seven local reactions out of 147 cases, approximately 4.7 percent. In two cases only transient discomfort was experienced and treat
ment was not stopped. In the other cases reactions developed severe enough to warrant cessation of treatment after 24 hours, two days, two days, seven days, and 10 days respectively. Itching and edema were prominent features of these severe reactions. No effort was made in any of these cases to rule out the possible allergenicity of the ointment base rather than that of the antibiotic.
S U M M A R Y
Erythromycin ointment, one percent, was used in 147 cases of external ocular affections. It appears to be of value in acute infections particularly those due to gram-positive bacteria. It appeared to be of prophylactic value in a small series of traumatic and operative cases. There were seven local reactions of the allergic type ; five were severe enough to require cessation of treatment.
1601 Spring Garden Street (30).
REFERENCE
1. Naib, K., Hallett, J. W., and Leopold, I. H.: Observations on the ocular effects of erythromycin. Am. J. Ophth., 39:395 (Mar.) 1955.
F U N D U S P H O T O G R A P H Y B Y E L E C T R O N I C F L A S H
PART I I I . A NEW FUNDUS-ANTERIOR SEGMKNT CAMERA
ROBERT C. DREWS, M . D . Saint Louis, Missouri
A. INTRODUCTION In Par t I (Am. J. Ophth., Aug., 1957), the
successful adaptation of electronic flash to the Bausch and Lomb-Nordenson fundus camera was described. In Par t I I (Am. J. Ophth., Sept., 1957), it was shown how this new instrument can be used to take high-resolution black and white fundus photographs. In this report I shall describe my own fundus camera. This new camera can also be used to take anterior-segment photographs.
There were several reasons for designing and building an entirely new fundus camera.
Electronic flash fundus cameras are unusually easy to operate and give superior photographs. I felt it was unduly expensive to purchase a camera with a carbon-arc light source, and then discard this source with its complement of clockwork, lenses, prisms, and shutter and install electronic flash.
Exist ing electronic flash fundus cameras^' ^ do not have the electronic flash tube internally mounted and one of these cameras ' uses a separate lamp for focusing. The massive base and castings of present cameras are unnecessary because of the extremely short exposure used with electronic flash (1/3,000th
FUNDUS PHOTOGRAPHY 523
of a second in my un i t ) . Features, such as double exposure prevention, can be built in. And, as will be shown later, the camera can be designed to take anterior segment photographs by removing the ophthalmoscope lens rather than by adding another lens, as in present fundus cameras.
B. C A M E R A D E S I G N
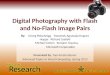
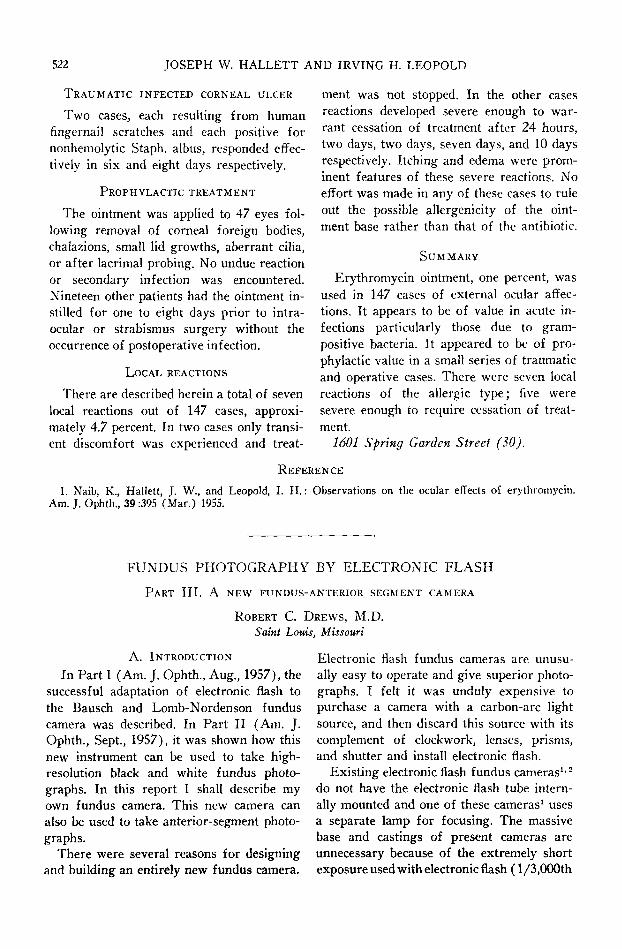
The present unit (fig. 1) is an assemblage of commercially available subunits with a minimum of specially fabricated parts. The ophthalmoscope lens is the Bausch and Lomb aspheric from their binocular ophthalmoscope. The tube and box were made of plastic and painted a flat black on the inside. The electronic flash tube was custom made from quartz. The camera lens is a Kodak enlarging Ektar of four-inch focal length and was chosen for its high correction at short working distances. A single lens reflex camera body is mounted on a bellows attachment, the bellows movement being used for focusing.
Commercially available single lens reflex cameras provide built-in shutter, synchronization, film-advance mechanism, and double-exposure prevention, as well as a viewing and focusing system. A simple camera, such as an Exa, may be used, since only a single slow shutter speed is needed for electronic flash work. However, a more expensive
model, such as the Exakta shown, may be desired because the reflex camera body can be easily detached and used for other types of photography.
With Exakta or E x a cameras one has a choice of focusing screens. I prefer a very fine ground-glass screen over which a drop of immersion oil has been spread for added transmission.
The Bausch and Lomb binocular ophthalmoscope base was chosen because of its relative portability, stability, and ease of adjustment. A Zeiss joystick type instrument table or cross movement base would offer the advantage of eliminating the external high voltage cable to the flash tube, since the camera could be mounted directly on the power supply.
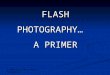
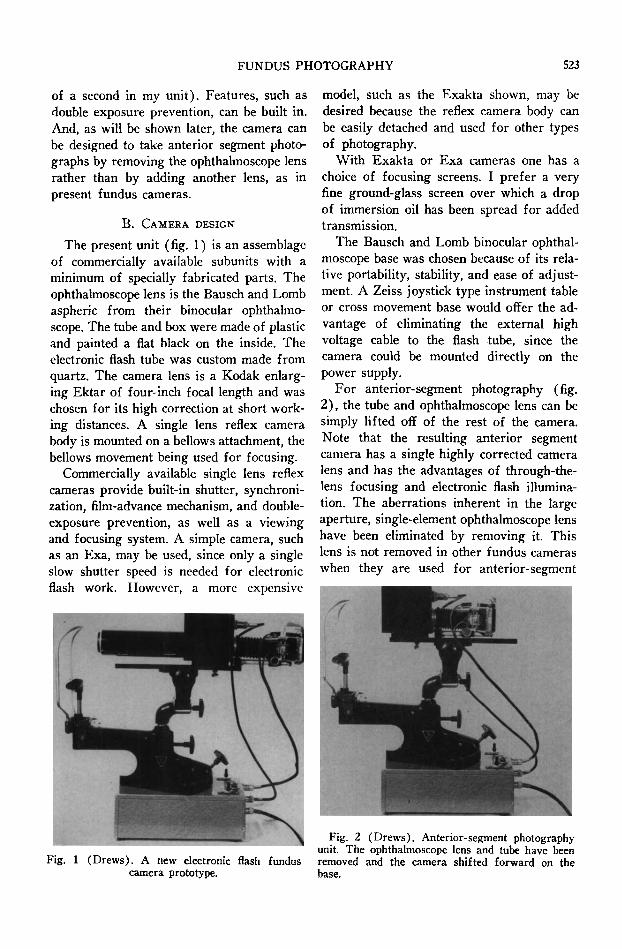
For anterior-segment photography (fig. 2 ) , the tube and ophthalmoscope lens can be simply lifted off of the rest of the camera. Note that the resulting anterior segment camera has a single highly corrected camera lens and has the advantages of through-the-lens focusing and electronic flash illumination. The aberrations inherent in the large aperture, single-element ophthalmoscope lens have been eliminated by removing it. This lens is not removed in other fundus cameras when they are used for anterior-segment
Fig. 1 (Drews). A new electronic flash fundus camera prototype.
Fig. 2 (Drews). Anterior-segment photography unit. The ophthalmoscope lens and tube have been removed and the camera shifted forward on the base.
524 ROBERT C. DREWS
photography, and their photographs are, therefore, inferior to those made with cameras designed specifically for such work. One of the features of the camera presented in this paper is the fact that it can be used for both fundus and anterior-segment photography without compromising the quality of either.
C . T H E ELECTRONIC F L A S H U N I T
The same basic electronic flash circuit is used as was described in Par t I. The block diagram (Pa r t I, fig. 3 ) is correct for this unit also. However, the power supply has been simplified and made much more compact, enabling one to mount it below the camera base. Thus camera and power supply are an integral unit.
D . O P E R A T I O N
Operation for fundus photography is the same as before (see Par t I, E ) . Briefly: With the camera loaded and the patient positioned before it, one turns on the power supply, turns on the focusing light, focuses, and then pulls back a lever switch to take the picture.
For anterior-segment photography, the ophthalmoscope lens is removed with its mounting tube. The camera is then moved closer or farther from the patient depending on how large an area is to be photographed. The flash unit is operated in the same manner as for fundus photography. Note that, be-
Fig. 4 (Drews). Anterior-segment photograph of both eyes. The left eye had been homatropinized for fundus photography.
cause the same light source is used both for focusing and taking the picture, one can sec exactly where the reflection of the light source will be on the patient's cornea. This allows adjustments to be made so that the reflection of the light source does not overlie the pathology that one desires to photograph.
E. R E S U L T S
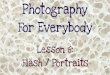
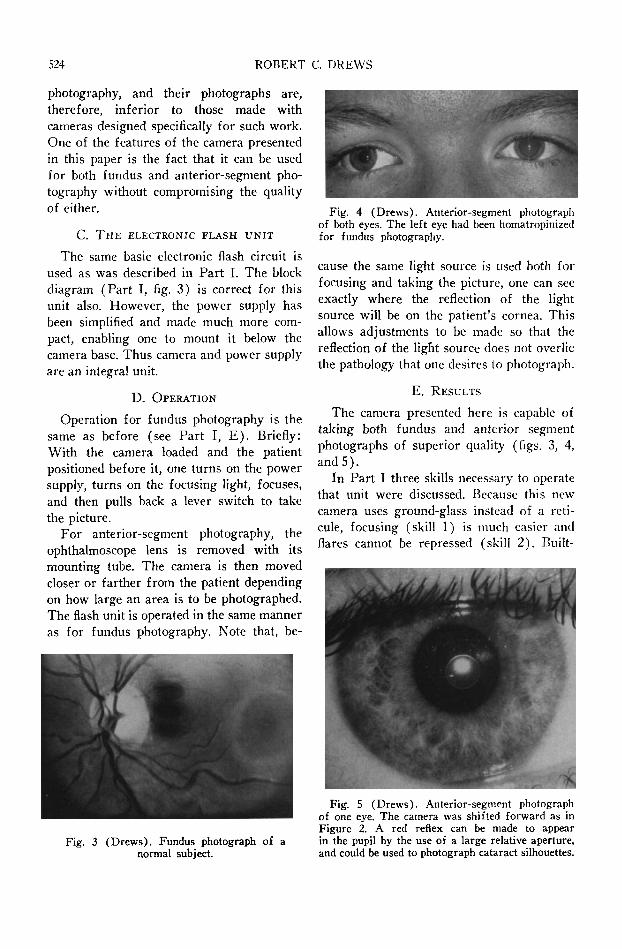
The camera presented here is capable of taking both fundus and anterior segment photographs of superior quality (figs. 3, 4, and 5 ) .
In Par t I three skills necessary to operate that unit were discussed. Because this new camera uses ground-glass instead of a reticule, focusing (skill 1) is much easier and flares cannot be repressed (skill 2 ) . Built-
Fig. 3 (Drews). Fundus photograph of a normal subject.
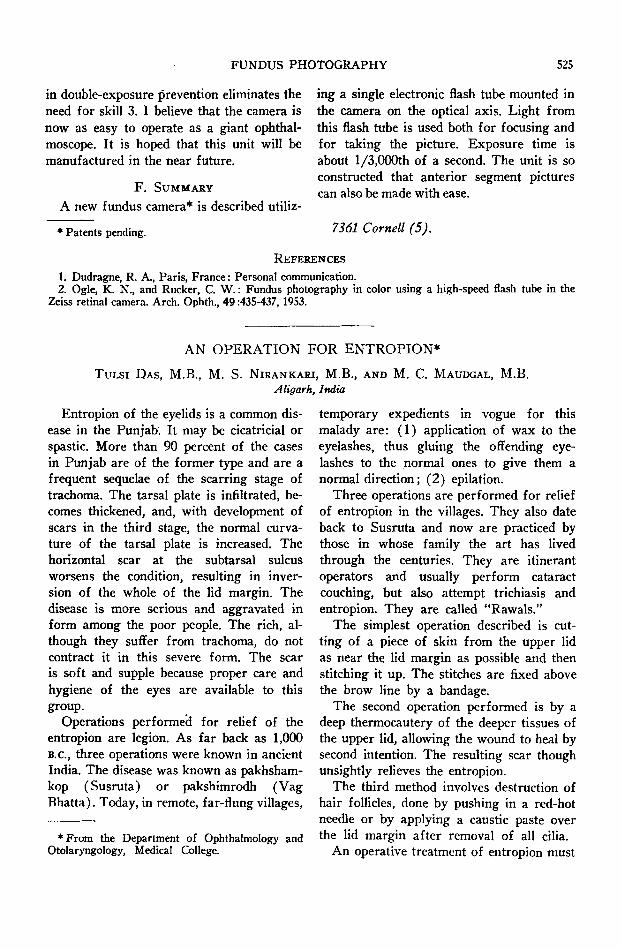
Fig. 5 (Drews). Anterior-segment photograph of one eye. The camera was shifted forward as in Figure 2. A red reflex can be made to appear in the pupil by the use of a large relative aperture, and could be used to photograph cataract silhouettes.
FUNDUS PHOTOGRAPHY 525
in double-exposure prevention eliminates the need for skill 3. I believe that the camera is now as easy to operate as a giant ophthalmoscope. I t is hoped that this unit will be manufactured in the near future.
F . S U M M A R Y
A new fundus camera* is described utiliz-
* Patents pending.
ing a single electronic flash tube mounted in the camera on the optical axis. Light from this flash tube is used both for focusing and for taking the picture. Exposure time is about l /3,000th of a second. The unit is so constructed that anterior segment pictures can also be made with ease.
7361 Cornell (5).
R E F E R E N C E S
1. Dudragne, R. Α., Paris, France: Personal communication. 2. Ogle, K. N., and Rucker, C. W.: Fundus photography in color using a high-speed flash tube in the
Zeiss retinal camera. Arch. Ophth., 49:435-437, 1953.
A N O P E R A T I O N F O R E N T R O P I O N *
TuLsi D A S , M . B . , M . S . N I R A N K A R I , M . B . , A N D M . C . M A U D G A L , M . B .
Aligarh, India
Entropion of the eyelids is a common disease in the Punjab. I t may be cicatricial or spastic. More than 90 percent of the cases in Ptmjab are of the former type and are a frequent sequelae of the scarring stage of trachoma. The tarsal plate is infiltrated, becomes thickened, and, with development of scars in the third stage, the normal curvature of the tarsal plate is increased. The horizontal scar at the subtarsal sulcus worsens the condition, resulting in inversion of the whole of the lid margin. The disease is more serious and aggravated in form among the poor people. The rich, although they suffer from trachoma, do not contract it in this severe form. The scar is soft and supple because proper care and hygiene of the eyes are available to this group.
Operations performed for relief of the entropion are legion. As far back as 1,000 B.c., three operations were known in ancient India. The disease was known as pakhsham-kop (Susru ta) or pakshimrodh (Vag Bhat ta) . Today, in remote, far-flung villages.
•From the Department of Ophthalmology and Otolaryngology, Medical College.
temporary expedients in vogue for this malady a re : ( 1 ) application of wax to the eyelashes, thus gluing the oflFending eyelashes to the normal ones to give them a normal direction; ( 2 ) epilation.
Three operations are performed for reHef of entropion in the villages. They also date back to Susruta and now are practiced by those in whose family the art has lived through the centuries. They are itinerant operators and usually perform cataract couching, but also attempt trichiasis and entropion. They are called "Rawals ."
The simplest operation described is cutting of a piece of skin from the upper lid as near the lid margin as possible and then stitching it up. The stitches are fixed above the brow line by a bandage.
The second operation performed is by a deep thermocautery of the deeper tissues of the upper lid, allowing the wound to heal by second intention. The resulting scar though unsightly relieves the entropion.
The third method involves destruction of hair follicles, done by pushing in a red-hot needle or by applying a caustic paste over the lid margin after removal of all cilia.
An operative treatment of entropion must