Embed Size (px)
Citation preview

Brief Clinical Report
Further Delineation ofCerebro-Osteo-Nephrosis Syndrome
Yevgenia Udler,1* Gabrielle J. Halpern,1 Carron Sher,1 Miriam Davidovitz,2 andMordechai Shohat1,3
1Department of Medical Genetics, Rabin Medical Center, Beilinson Campus, Petah Tiqva, Israel2Department of Nephrology, Rabin Medical Center, Beilinson Campus, Petah Tiqva, Israel3Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
We describe an Israeli Jewish child of Ye-menite origin who may be affected with ‘‘ce-rebro-osteo-nephrosis.’’ She is short of stat-ure (height below 3rd centile) due to skel-etal abnormalities. She has minor anomaliesand borderline intelligence. There ismarked proteinuria and she is in kidneyfailure. Opitz et al. [1985: Am J Med Genet22:521–529] described 2 Hutterite sisters inAmerica who were suffering from a condi-tion which greatly resembles that of our pa-tient. We question whether these conditionsin the two families are the same syndromewith pleiotropic expression, as suggested byOpitz et al., or whether they represent twodistinct genetic entities. Am. J. Med. Genet.72:383–385, 1997. © 1997 Wiley-Liss, Inc.
KEY WORDS: short stature; minor anoma-lies; proteinuria
INTRODUCTION
Opitz et al. [1985] described 2 Hutterite sisters withcerebro-osteo-nephrosis, a previously unreported con-dition. We report a possible further case in an IsraeliJewish child of Yemenite origin.
CLINICAL REPORT
D. was born in 1980 to healthy, nonconsanguineousparents who already had one unaffected daughter andwho subsequently gave birth to a healthy son (Fig.1).Both parents are Yemenite Jews.
She was born after an uneventful pregnancy and de-livery. Birth weight was 2,800 g and length was lessthan normal. On examination immediately after birth,
she was found to have a ‘‘large tongue’’ and noisy res-piration.
As she developed, she remained short, always belowthe 3rd centile. She walked at age 11⁄2 years and beganto speak in sentences at age 4 years. She has alwaysattended a remedial class. She is of borderline intelli-gence, but this has been constant from birth and therehas never been any notable deterioration in her level offunctioning or regression to a lower level.
She was discovered to have proteinuria at age 4years, but this was not investigated until age 15 yearswhen she began to complain of general lethargy andtiredness. At this time she was found to have massiveproteinuria and was referred for further evaluation.
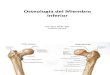
On physical examination her height was 138 cm(<3rd centile) and she had brachycephaly, a flat face, along upper lip, and thick upper and lower vermilionborder. Neurological examination and MRI scan werenormal. Her IQ was found to be 89 with difficulties infine and gross motor function and poor vocabulary. Inaddition, she has problems with day-to-day tasks.
Fundoscopy revealed mild hypertensive retinopathywithout any additional findings. Vision was normal.Audiological examination was also normal. Both ECGand cardiac echocardiography were documented as nor-mal. Blood pressure, however, was elevated (150/90mm Hg). Vertebral X-ray studies documented platy-spondyly and delayed opacification of the vertebralbodies, with mild thoraco-lumbar scoliosis. Pelvic X-rays showed bilateral shortness of the neck of the fe-mura. Joint movements were unlimited. Renal failurewas observed, with a blood creatinine level of 2.5 mg/dl(Glomerular filtration rate (GFR) of ∼25 Ml/min/1.73m2) and hypoalbuminemia of 2.8 g/dl. Renal ultrasoundshowed normal collecting ducts, with intensified paren-chymal echogenicity.
Karyotype was normal (46,XX). There was no rel-evant family history.
DISCUSSION
Opitz et al. [1985] described 2 sisters, members of aLehrerleut Hutterite family from Montana, who weresuffering from a previously unreported condition in-volving primarily the skeletal system, the kidneys, andthe brain. They named this condition cerebro-osteo-
*Correspondence to: Y. Udler, M.D., Department of MedicalGenetics, Rabin Medical Center, Beilinson Campus, Petah Tiqva49 100, Israel.
Received 3 June 1996; Accepted 17 February 1997
American Journal of Medical Genetics 72:383–385 (1997)
© 1997 Wiley-Liss, Inc.

nephrodysplasia. As all patients had nephrosis as acharacteristic renal feature, it seems that cerebro-osteo-nephrosis is a more specific term for this condi-tion. We hereby describe a possible third case occurringin an Israeli Jewish child of Yemenite origin.
Table I shows the comparison between the original 2sisters and our patient. The first of the 2 sisters died atage 3 years. The second was still alive at the time the
report was written, but she had a clinical picture simi-lar to but somewhat less severe than that of her sister.Our patient is already 15 years old and, although theclinical picture is similar to that of the 2 sisters, she isless severely affected; however, she is currently in kid-ney failure and receiving regular dialysis with theeventual intention of performing a kidney transplant.
The older sister in Opitz et al. [1985] apparently diedof nephrotic syndrome. Although at age 11 months uri-nalysis was reported as normal, it was unknown forhow long the child’s kidneys had been affected prior toher death. Our patient was first found to have protein-uria at age 4 years but there is no way of knowing forhow long it had been present.
The older sister in the report of Opitz et al. [1985]apparently had normal cerebral function at birth. How-ever, as she developed, her level of functioning deterio-rated as her seizures became more severe, and she re-gressed. A CT scan documented significant diffuse ce-rebral atrophy with enlargement of the ventricles andsulci. The diagnosis of a degenerative brain diseasewas suggested. The younger sister, at the time of thereport, was only 6 months old, so that it was too earlyto know how she would develop. However, in compari-son with the older sister at the same age, she appearedto be less severely affected.
Our patient was noted from birth to have delayedpsychomotor development and has always been of bor-derline intelligence. However, she has never had anyseizures and her level of cerebral functioning has re-mained constant without any regression. An MRI scanwas normal.
We have been unable to find any subsequent reportsof this condition in the literature. Our patient does not
Fig. 1. Facial appearance. Note brachycephaly, flat face, long upper lip,and upper vermilion border.
TABLE I. Comparison of Patients of Opitz et al. [1985] and Our Patient
Opitz et al. [1985]
Our patientPatient 1 Patient 2
Birth weight 2,138 g 2,817 g 2,800 gShort birth length (<3rd centile) + + +Nephrotic syndrome (focal glomerulosclerosis) + +Facial anomalies + ± +
Flat face + +Brachycephaly + + +Long upper lip + + +Flat philtrum +Upper vermilion border + + +Umbilical hernia + − −Simian crease + − −Large tongue + − +Large anterior fontanelle + − −Small midface compared to calvarial size + − +Very short neck − + +
Skeletal abnormalities + + +Short trunk + + +Short limbs + + ±Platyspondyly + − +Delayed ossification of the vertebral bodies + ? +
Thoraco-lumbar scoliosis, mild − − +CNS
Seizures + ± −CT: diffuse cerebral atrophy +MRI Normal
Karyotype 46,XX ? 46,XX
384 Udler et al.

appear to have any of the other conditions reported inthe literature, which include both neurological and re-nal problems.
Friedreich’s ataxia with nephrotic syndrome andconclusive disorder, described by Watters et al. [1981],includes ataxia and epilepsy with minimal lesion ne-phrotic syndrome. These neurological findings are ab-sent in our patient. Our patient does not have micro-cephaly and, therefore, cannot be classified as havingGalloway-Mowat syndrome [Sano et al., 1995].
The differences between the patients of Opitz et al.[1985] and ours would lead us to question whether weare dealing with a single genetic entity with pleiotropicexpression, or with different conditions involving sepa-rate genes. Further studies of additional cases shouldhelp to elucidate this point.
ACKNOWLEDGMENTS
We thank Bella Eisenstein (Department of Nephrol-ogy, Rabin Medical Center) for her advice in the man-agement of this patient.
REFERENCESOpitz JM, Lowry RB, Holmes TM, Morgan K (1985): Hutterite cerebro-
osteo-nephrodysplasia: Autosomal recessive trait in a Lehrerleut Hut-terite family from Montana. Am J Med Genet 22:521–529.
Sano H, Miyanoshita AK, Watanabe N, Koga Y, Miyazawa Y, YamaguchiY, Fukushima Y, Itami N (1995): Microcephaly and early-onset ne-phrotic syndrome confusion in Galloway-Mowat syndrome. PediatrNephrol 9:711–714.
Watters GV, Zlotkin SH, Kaplan BS, Humphreys P, Drummond KN (1981):Friedrech’s ataxia with nephrotic syndrome and convulsive disorders:Clinical and neurophysiological studies with renal and nerve biopsiesand an autopsy. Neurol 8:55–60.
Cerebro-Osteo-Nephrosis Syndrome 385