Embed Size (px)
Citation preview
Future ART options for HIV-infected children exposed to maternal HAART
Lee Kleynhans
Experts Roundtable
23-24 June 2008
Overview
• Current WHO recommendations• Problems• Solutions
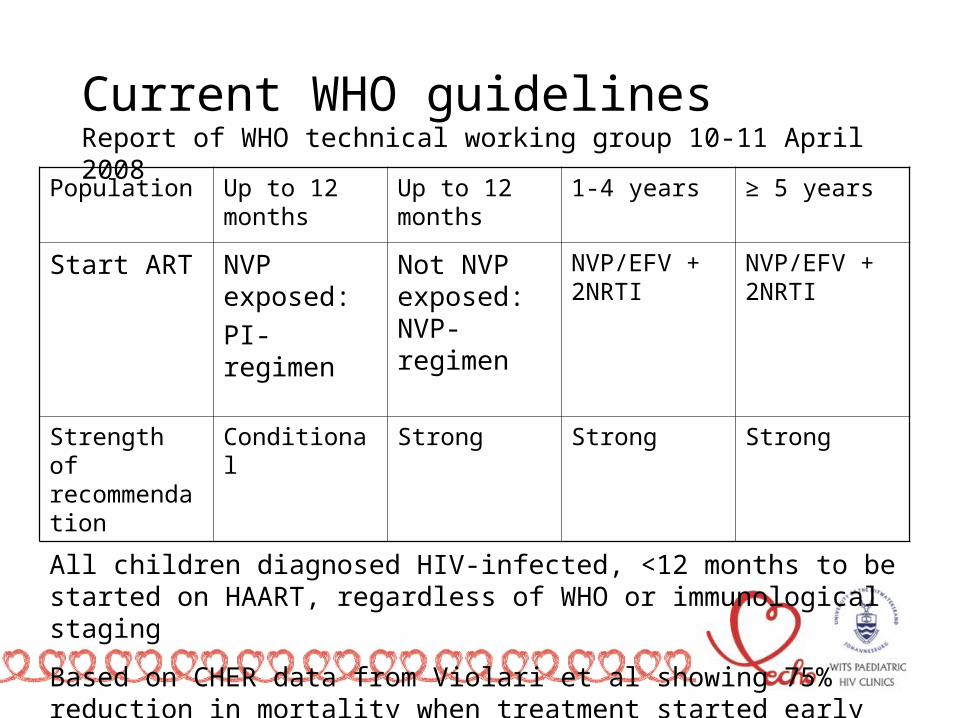
Current WHO guidelinesReport of WHO technical working group 10-11 April 2008
Population Up to 12 months
Up to 12 months
1-4 years ≥ 5 years
Start ART NVP exposed:
PI- regimen
Not NVP exposed: NVP-regimen
NVP/EFV + 2NRTI
NVP/EFV + 2NRTI
Strength of recommendation
Conditional Strong Strong Strong
All children diagnosed HIV-infected, <12 months to be started on HAART, regardless of WHO or immunological staging
Based on CHER data from Violari et al showing 75% reduction in mortality when treatment started early
Arrivé et al, Int Journ Epid 2007 Oct 36(5):1009-21Prevalence of resistance to nevirapine in mothers and children after single-dose exposure to prevent vertical transmission of HIV 1: A meta-analysis
• NVP resistance detected after single dose NVP for PMTCT – 35.7% resistance in women – Over half of infants 52.6% (studies range between
40-90% babies)
• In adults started on NVP-based regimen after 12 months 70% HIV RNA suppression (Weidle P et al CROI 2008)
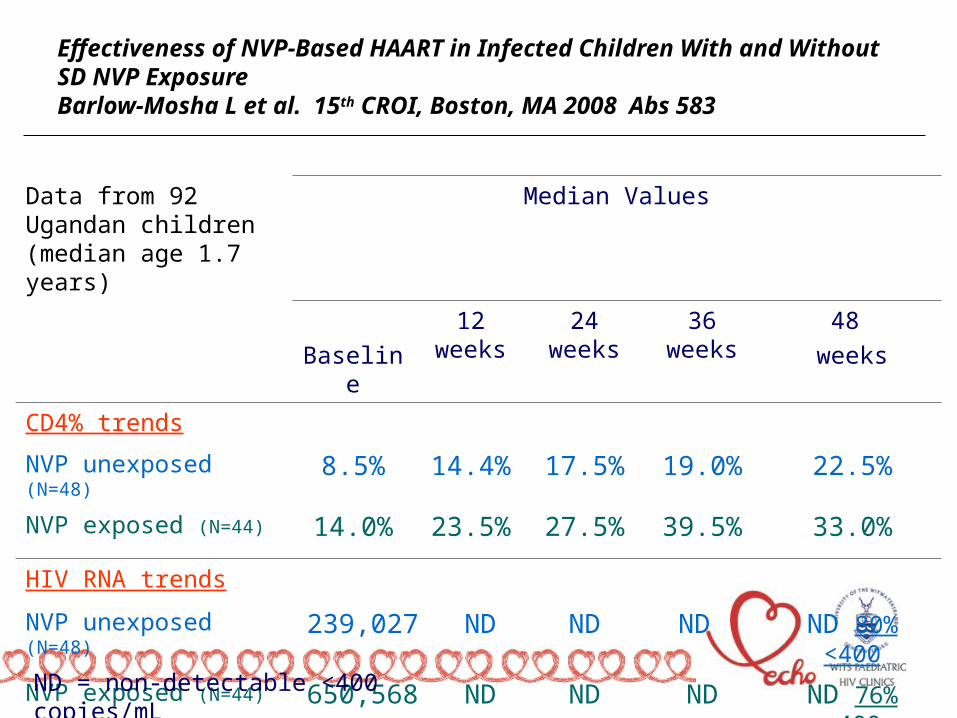
Effectiveness of NVP-Based HAART in Infected Children With and Without SD NVP ExposureBarlow-Mosha L et al. 15th CROI, Boston, MA 2008 Abs 583
Data from 92 Ugandan children (median age 1.7 years)
Median Values
Baseline
12 weeks
24 weeks
36 weeks 48
weeks
CD4% trends
NVP unexposed (N=48) 8.5% 14.4% 17.5% 19.0% 22.5%
NVP exposed (N=44) 14.0% 23.5% 27.5% 39.5% 33.0%
HIV RNA trends
NVP unexposed (N=48) 239,027 ND ND ND ND 80% <400
NVP exposed (N=44) 650,568 ND ND ND ND 76% <400
ND = non-detectable <400 copies/mL
• But no study results yet on a head to head comparison between NVP-based and OI-based regimens in infants in low-income settings.
• Awaiting data from NEVEREST study- Coronation Hospital South Africa
• PACTG 1060 underway
Zidovudine with Nevirapine for PMTCT reduces Nevirapine resistance in mothers from the Western Cape, South Africa GU Van Zyl et al; Journal of medical Virology 80:942-946
• Recently reported from Western Cape • 17.1 % NNRTI resistance if dual therapy
given as PMTCT• Reduction compared to single dose NvP• Confirmed by Arrivé et al• Reduced to 4% (mother) and 16% (infant)
respectively
Antiretroviral Drug Penetration into Breast Milk and Infant Plasma: BAN StudyCorbett A et al. 15th CROI Boston, MA, 2008 Abs 648
• While 3TC concentrations in breast milk was 2.6-fold higher than maternal plasma, infant plasma exposure was relatively low (1% of breast milk).
• NVP concentrations in breast milk were 70% of maternal plasma, with infant exposure 20% of breast milk.
• NFV concentration in breast milk is very low, 8%, with no drug found in the infant.
• Conclusion: Risk for toxicity in the infant appears low but low drug levels in infant from drug passage from breast milk for NVP (possibly 3TC) may suggest risk of resistance if infant becomes infected.
KIBS Maternal HAART Prophylaxis study Zeh C et al. 15th CROI, Boston, MA, 2008 Abs 84LB
• Women receiving lamivudine, zidovudine and either nevirapine or nelfinavir
• 5.8% transmission rate• Genotypic resistance in infants:• 43% of women taking NVP• 100% of women taking nelfinavir• No PI resistance but 100% NRTI resistance in
nelfinavir group and 100% NNRTI resistance in NVP group
KIBS Maternal HAART Prophylaxis study Zeh C et al. 15th CROI, Boston, MA, 2008 Abs 84LB
• Resistance mutations included:
– NRTI: M184V in 13, K65R in 4, D67N in 2 and T215Y in 2
– NNRTI: Y181C in 3, K103N in 2, G190A in 2, K101E in 1
• Among NVP-exposed infants:
– 4/6 had NRTI and 6/6 NNRTI resistance
• Among NFV-exposed infants:
– 10/10 had NRTI and 0/10 had PI resistance
Cont….
• Cumulative risk of resistance…not detected initially
• Emerged week 14-24• Most of resistance risk during breastfeeding• 69% babies tested PCR + by 6 weeks• Unknown maternal VL
Potential problems in infant
• High viral load if HIV-infected in face of low drug levels
• 3TC and NVP have highest plasma levels• These are the drugs with low genetic barrier for
resistance• Atripla: FTC presumably similar to 3TC but no data.• No data found on EFV levels in infants
• Resistance testing prohibitively expensive therefore not possible in low income settings
• Many countries still using NVP as 1st line due to cost compared with kaletra®
• 3TC excellent drug…cheap and minimal side effects
Solutions
• EARLY INFANT TESTING
• At 6 week EPI visit, results at week 10
• EARLY INFANT DIAGNOSIS
• EARLY INFANT TREATMENT
Solutions
• Use WHO treatment guidelines BUT need to be aware of possible resistance and virological failure
• ? Motivate for at least 1 viral load within 6 months to assess HIV RNA supression as may miss failure if only using clinical and immunological criteria-> Risk TAMs and other NRTI resistance mutations and decrease future options
• Stop interventional HAART as soon as child diagnosed HIV-infected (given for 1st 24 weeks not for maternal health)





























