Embed Size (px)
Citation preview
R e v i e w P a p e r
Gaps in the ARB Knowledge Base: AreARBs Effective Anti–Atrial FibrillationAgents?
Peter Kowey, MD
The impact of atrial fibrillation (AF) on the over-all health of the patient is underestimated bymany health care practitioners. Aging is the mostimportant pathogenetic factor for this diseaseand, with the aging of the population, AF willsoon reach epidemic levels. Although the surfaceelectrocardiograph indicates the presence of thisarrhythmia, there are numerous mechanisms thatcould be causing it. Therefore, the clinician hasto choose which intervention might be best.However, currently available therapeutics, bothpharmacologic and nonpharmacologic, are inade-quate. This paper will discuss the clinical impactof AF, its various treatment options, how inhibi-tors of the renin-angiotensin-aldosterone system(RAAS) can impact atrial electrophysiology, andtherapeutic evidence to support the use of RAASmodulation in AF. J Clin Hypertens (Greenwich).2009;11:S48–S51. ª2009 Wiley Periodicals, Inc.
Lyndon Johnson once told a story about a manwho was interviewing for a job as a switch-
man on a railroad. He was asked the question,‘‘What would you do if you looked to your rightand saw a train coming into the station 100 milesan hour without braking, and you looked to your
left and you saw another train coming into thestation 100 miles an hour without braking? Whatwould you do?’’ And he said, ‘‘I’d go get mybrother, Jeb.’’ ‘‘Why would you get your brother,Jeb?’’ ‘‘Because Jeb ain’t never seen a traincrash.’’
The field of cardiovascular (CV) disease is likethese two trains coming into the station. Theimpact of the disease state is underestimated, andcurrently available therapeutics are inadequate.One of the areas where this is happening is atrialfibrillation (AF), which is at epidemic levels. Atmany hospitals, including Lankanau Hospital inPhiladelphia, AF is the number one reason for inpa-tient CV consultation. And as the population ages,there is a greater incidence of AF, but also type 2diabetes mellitus and hypertension.
CLINICAL IMPACT OF AFAging is by far the most important pathogeneticfactor for AF. For every year a person lives past50, 1% of atrial musculature is replaced withfibrous tissue. Therefore, in a 100-year-old person,almost half the atrium is replaced with fibrous tis-sue. It is this fibrosis that acts as a substrate for AFin the elderly. Prevalence is increased as wellbecause physicians are more aware of the diseaseand spend more time monitoring patients. In addi-tion, better technology has enabled better detectionof the arrhythmia. AF has an important impact onpublic health largely because it is an important riskfactor for stroke due to the formation of bloodclots in the atrium, which can dislodge and blockblood flow in cerebral vessels. Strokes from AFtend to be disabling or fatal. AF is also a risk factor
From the Main Line Health Heart Center, LankenauHospital, Wynnewood, PA. and Jefferson MedicalCollege, Philadelphia, PAAddress for correspondence:Peter R. Kowey, MD, Mainline Health Heart Center,Lankenau Hospital, Wynnewood, PAE-mail: [email protected]
doi: 10.1111/j.1751-7176.2009.00214.x
THE JOURNAL OF CLINICAL HYPERTENSION SUPPL. 1 VOL. 11 NO. 12 DECEMBER 2009S48
for heart failure (HF) due to potentially deleterioushemodynamic and electrophysiologic changes,which could accelerate the progression of leftventricular dysfunction in patients with underlyingHF.
AF: TREATMENT OPTIONSTreatment of AF starts with prevention. This iswhere agents that inhibit the renin-angiotensin-aldosterone system (RAAS) may prove most useful.In addition, for patients who have the disease, theseagents may be useful as adjuvant therapy alongwith membrane-active drugs. Once the arrhythmiais established, RAAS inhibitors do not have enoughof an electrophysiologic impact on the atrium to bestand-alone drugs. This is important because it isgood to be in sinus rhythm. A misleading messagefrom trials such as the Atrial Fibrillation Follow-UpInvestigation of Rhythm Management (AFFIRM)and Rate Control versus Electrical Cardioversion(RACE) study was that rate control was as good asrhythm control. This is nonsensical.1,2 Rate controlis a default strategy that is pursued in people whenattempts at sinus rhythm have failed. Patients whohave symptomatic AF need sinus rhythm, and there
is reason to believe that sinus rhythm is associatedwith better outcomes. A post hoc analysis fromAFFIRM that looked at the value of sinus rhythmclearly showed that it is associated with better sur-vival.3 The problem was that patients had to betaking an antiarrhythmic drug to be in sinusrhythm. The drug was usually amiodarone and thebenefits of this drug in this study were offset byserious adverse effects. In the Placebo-Controlled,Double-Blind, Parallel Arm Trial to Assess the Effi-cacy of Dronedarone 400 mg bid for the Preventionof Cardiovascular Hospitalization or Death fromAny Cause in Patients With Atrial Fibrilla-tion ⁄Atrial Flutter (ATHENA) trial, the use of theantiarrhythmic drug, dronedarone, in patients wasassociated with fewer hospitalizations comparedwith patients with AF who were not treated withthat drug.4 The relevant message is that it is goodto be in sinus rhythm.
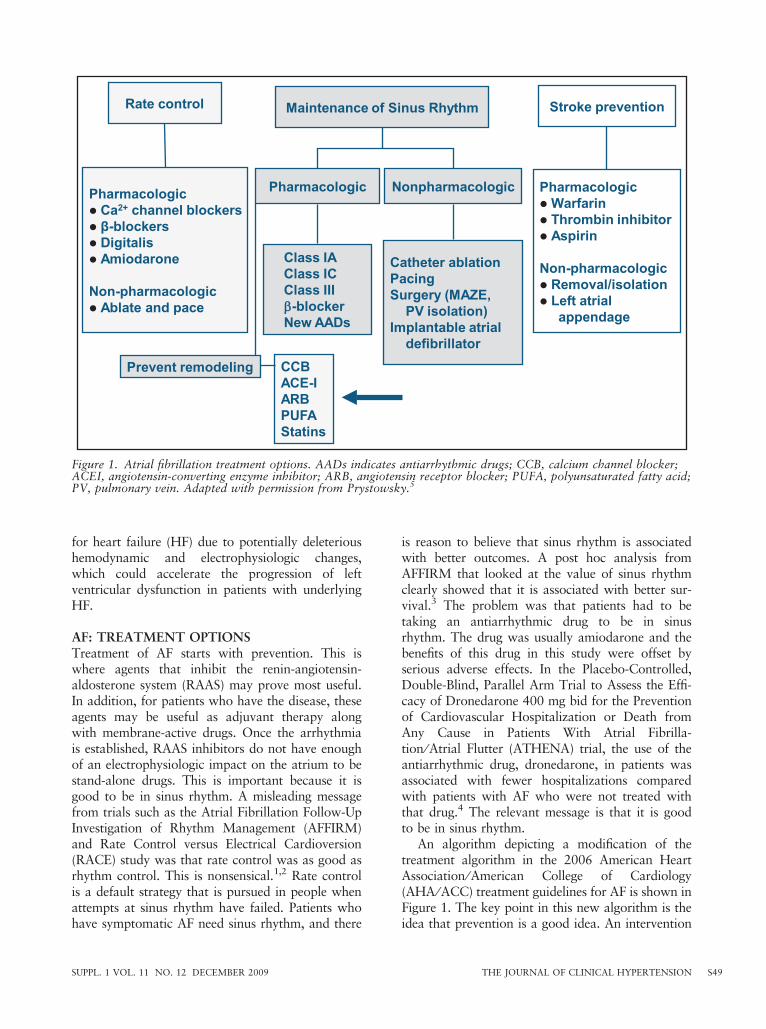
An algorithm depicting a modification of thetreatment algorithm in the 2006 American HeartAssociation ⁄American College of Cardiology(AHA ⁄ACC) treatment guidelines for AF is shown inFigure 1. The key point in this new algorithm is theidea that prevention is a good idea. An intervention
Figure 1. Atrial fibrillation treatment options. AADs indicates antiarrhythmic drugs; CCB, calcium channel blocker;ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; PUFA, polyunsaturated fatty acid;PV, pulmonary vein. Adapted with permission from Prystowsky.5
SUPPL. 1 VOL. 11 NO. 12 DECEMBER 2009 THE JOURNAL OF CLINICAL HYPERTENSION S49
that has relatively low risk and is effective at prevent-ing AF should be contemplated in patients with ahigh risk of developing AF.5
In clinical practice, we already do this. A patientwho has hypertensive heart disease is at high riskfor AF. With ‘‘upstream therapy,’’ the goal is toprevent AF before it starts. Therapeutic candidatesfor upstream therapy include angiotensin-convertingenzyme (ACE) inhibitors, angiotensin receptorblockers (ARB), statins, fish oil, anti-inflammatoryagents, b-blockers, and proliferator-activated recep-tor c modulators.
RAAS INHIBITORS AND THEIR EFFECTSON ATRIAL ELECTROPHYSIOLOGYThere is no way to dissociate the antihypertensiveeffects, antifibrotic effects, and anti-inflammatoryeffects of a drug from its direct electrophysio-logic effects. In a canine right ventricle pacingmodel, AF duration was increased relative to con-trols due to pacing-induced atrial electrical remod-eling caused by the formation of fibrous tissue.Tissue fibrosis creates a substrate that causes persis-tent arrhythmias independent of action potentialduration. Although enalapril attenuates the devel-opment of interstitial fibrosis, it has no impact onthe atrial effective refractory period, conductionvelocity, or wavelength of conduction. Thus, angio-tensin II may contribute to the development ofatrial fibrosis but may do so even with minimaldirect electrophysiologic effects.6,7
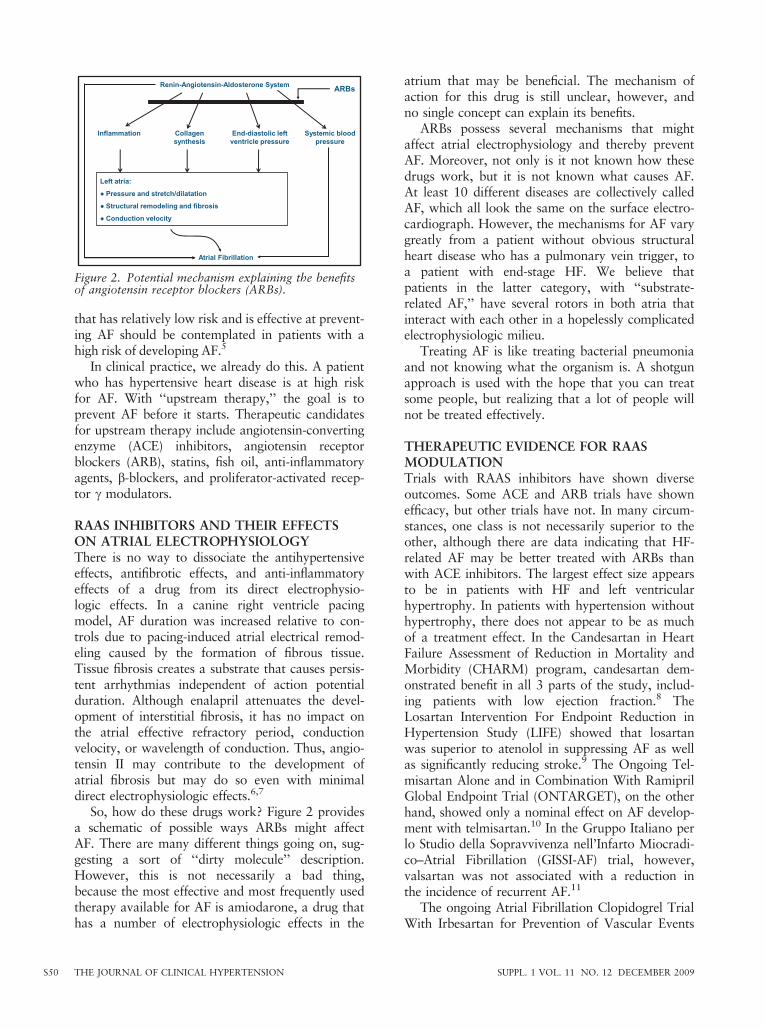
So, how do these drugs work? Figure 2 providesa schematic of possible ways ARBs might affectAF. There are many different things going on, sug-gesting a sort of ‘‘dirty molecule’’ description.However, this is not necessarily a bad thing,because the most effective and most frequently usedtherapy available for AF is amiodarone, a drug thathas a number of electrophysiologic effects in the
atrium that may be beneficial. The mechanism ofaction for this drug is still unclear, however, andno single concept can explain its benefits.
ARBs possess several mechanisms that mightaffect atrial electrophysiology and thereby preventAF. Moreover, not only is it not known how thesedrugs work, but it is not known what causes AF.At least 10 different diseases are collectively calledAF, which all look the same on the surface electro-cardiograph. However, the mechanisms for AF varygreatly from a patient without obvious structuralheart disease who has a pulmonary vein trigger, toa patient with end-stage HF. We believe thatpatients in the latter category, with ‘‘substrate-related AF,’’ have several rotors in both atria thatinteract with each other in a hopelessly complicatedelectrophysiologic milieu.
Treating AF is like treating bacterial pneumoniaand not knowing what the organism is. A shotgunapproach is used with the hope that you can treatsome people, but realizing that a lot of people willnot be treated effectively.
THERAPEUTIC EVIDENCE FOR RAASMODULATIONTrials with RAAS inhibitors have shown diverseoutcomes. Some ACE and ARB trials have shownefficacy, but other trials have not. In many circum-stances, one class is not necessarily superior to theother, although there are data indicating that HF-related AF may be better treated with ARBs thanwith ACE inhibitors. The largest effect size appearsto be in patients with HF and left ventricularhypertrophy. In patients with hypertension withouthypertrophy, there does not appear to be as muchof a treatment effect. In the Candesartan in HeartFailure Assessment of Reduction in Mortality andMorbidity (CHARM) program, candesartan dem-onstrated benefit in all 3 parts of the study, includ-ing patients with low ejection fraction.8 TheLosartan Intervention For Endpoint Reduction inHypertension Study (LIFE) showed that losartanwas superior to atenolol in suppressing AF as wellas significantly reducing stroke.9 The Ongoing Tel-misartan Alone and in Combination With RamiprilGlobal Endpoint Trial (ONTARGET), on the otherhand, showed only a nominal effect on AF develop-ment with telmisartan.10 In the Gruppo Italiano perlo Studio della Sopravvivenza nell’Infarto Miocradi-co–Atrial Fibrillation (GISSI-AF) trial, however,valsartan was not associated with a reduction inthe incidence of recurrent AF.11
The ongoing Atrial Fibrillation Clopidogrel TrialWith Irbesartan for Prevention of Vascular Events
Figure 2. Potential mechanism explaining the benefitsof angiotensin receptor blockers (ARBs).
THE JOURNAL OF CLINICAL HYPERTENSION SUPPL. 1 VOL. 11 NO. 12 DECEMBER 2009S50

(ACTIVE I) study uses irbesartan in one of its treat-ment arms. In the factorial design of this study,9000 patients are being evaluated for their responseto irbesartan vs placebo for the prevention of vas-cular events including stroke, myocardial infarction,vascular death, and HF hospitalizations. This is thelargest trial ever conducted studying the effect ofblood pressure lowering in patients with AF. Base-line parameters show that more than 60% ofpatients were already taking ACE inhibitors andmore than 65% of patients had permanent AF.12
RAAS INHIBITION AS ADJUNCTIVETHERAPYThe goal of adjunctive therapy is to improve theefficacy of a membrane-active drug such as amioda-rone by adding an ACE inhibitor or ARB. A studyby Madrid and colleagues13 demonstrated that irbe-sartan augmented the effect of amiodarone whileYin and colleagues14 showed a similar responsewith both losartan and perindopril in a patientpopulation with lone AF or AF in the absence ofstructural heart disease.
CONCLUSIONSThere is likely added benefit of using RAAS modu-lators and perhaps drugs from other classes forpatients with AF, but the mechanism by which thisoccurs is unclear. Another unexplored area is dos-age. It may not be accurate to presume that dosesthat lower blood pressure or are used for treatingHF will be the same doses to cause anti-fibrillatoryeffects. Getting answers is not easy since large num-bers of patients are needed to study multiple dosesin multiple arms to determine efficacy in preventionstudies. Adequately powered, better prospectivestudies are needed to study RAAS inhibitors aloneand in combination with membrane-active agents,perhaps even in combination with other therapeuticprocedures, such as catheter ablation.
Disclosures: Dr Kowey has indicated that he owns stock, stockoptions, or bonds from CardioNet. He has received grants foreducational activities from Medtronic, Inc, Boston Scientific,and St. Jude Medical. He also served as an advisor orconsultant for sanofi-aventis, GlaxoSmithKline, AstraZenecaPharmaceuticals LP, Johnson & Johnson PharmaceuticalResearch & Development, LLC, Solvay Pharmaceuticals, Inc,and Boehringer Ingelheim Pharmaceuticals, Inc. The authoracknowledges the assistance of Practicum Educational Services
in preparing this article and styling the paper for journalsubmission. Editorial support was provided by Ronald K. Miller,PhD, and funded by Daiichi Sankyo, Inc. The author received anhonorarium from Daiichi Sankyo, Inc, for time and effort spentpreparing this article.
REFERENCES
1 Cooper HA, Bloomfield DA, Bush DE, et al. Relationbetween achieved heart rate and outcomes in patients withatrial fibrillation (from the Atrial Fibrillation Follow-upInvestigation of Rhythm Management [AFFIRM] Study).Am J Cardiol. 2004;93:1247–1253.
2 Van Gelder IC, Hagens VE, Bosker HA, et al. A comparisonof rate control and rhythm control in patients with recurrentpersistent atrial fibrillation. N Engl J Med. 2002;347:1834–1840.
3 The AFFIRM Investigators. Relationships between sinusrhythm, treatment, and survival in the Atrial Fibrillation Fol-low-Up Investigation of Rhythm Management (AFFIRM)study. Circulation. 2004;109:1509–1513.
4 Hohnloser SH, Crijns HJGM, van Eickels M, et al. Effectof dronedarone on cardiovascular events in atrial fibrilla-tion. N Engl J Med. 2009;360:668–678.
5 Prystowsky E. Management of atrial fibrillation: therapeu-tic options and clinical decisions. Am J Cardiol. 2000;85:3D–11D.
6 Shi Y, Ducharme A, Li D, et al. Enalapril effects on atrialremodeling and atrial fibrillation in experimental conges-tive heart failure. Cardiovasc Res. 2002;54:456–461.
7 Ram R, Van Wagoner D. Aldosterone antagonism as anantiarrhythmic approach for atrial arrhythmias in heartfailure. J Cardiovasc Electrophysiol. 2006;17:542–543.
8 Ducharme A, Swedberg K, Pfeffer MA, et al. CHARMInvestigators. Prevention of atrial fibrillation in patientswith symptomatic chronic heart failure by candesartan inthe Candesartan in Heart failure: Assessment of Reductionin Mortality and morbidity (CHARM) program. AmHeart J. 2006;152:86–92.
9 Wachtell K, Lehto M, Gerdts E, et al. Angiotensin IIreceptor blockade reduces new-onset atrial fibrillation andsubsequent stroke compared to atenolol: the LosartanIntervention For End point reduction in hypertension(LIFE) study. J Am Coll Cardiol. 2005;45:712–719.
10 Yusuf S, Diener HC, Sacco RL, et al. Telmisartan to pre-vent recurrent stroke and cardiovascular events. N Engl JMed. 2008;359:1225–1237.
11 GISSI-AF Investigators, Disertori M, Latini R, et al.Valsartan for prevention of recurrent atrial fibrillation.N Engl J Med. 2009;360:1606–1617.
12 The Active Steering Committee; ACTIVE Investigators.Rationale and design of ACTIVE: the atrial fibrillationclopidogrel trial with irbesartan for prevention of vascularevents. Am Heart J. 2006;151:1187–1193.
13 Madrid AH, Bueno MG, Rebollo JM, et al. Use of irbe-sartan to maintain sinus rhythm in patients with long-standing persistant atrial fibrillation: a prospective andrandomized study. Circulation. 2002;106:331–336.
14 Yin Y, Dalal D, Liu Z, et al. Prospective randomizedstudy comparing amiodarone vs. amiodarone plus losar-tan vs. amiodarone plus perindopril for the prevention ofatrial fibrillation recurrence in patients with lone paroxys-mal atrial fibrillation. Eur Heart J. 2006;27:1841–1846.
SUPPL. 1 VOL. 11 NO. 12 DECEMBER 2009 THE JOURNAL OF CLINICAL HYPERTENSION S51