Embed Size (px)
Citation preview
Gary L. Bowlin, Ph.D.
Associate ProfessorLouis and Ruth Harris Exceptional Scholar
Professorship Department of Biomedical EngineeringVirginia Commonwealth University
Richmond, Virginia 23284
Co-Founding Inventor
NanoMatrix, Inc.
Co-Founding Inventor and Consultant
TraumaCure, Inc.
Bethesda, MD
June 3, 2008
Development of an Electrospun, Acellular, Bioresorbable, Small Diameter Vascular Prosthetic
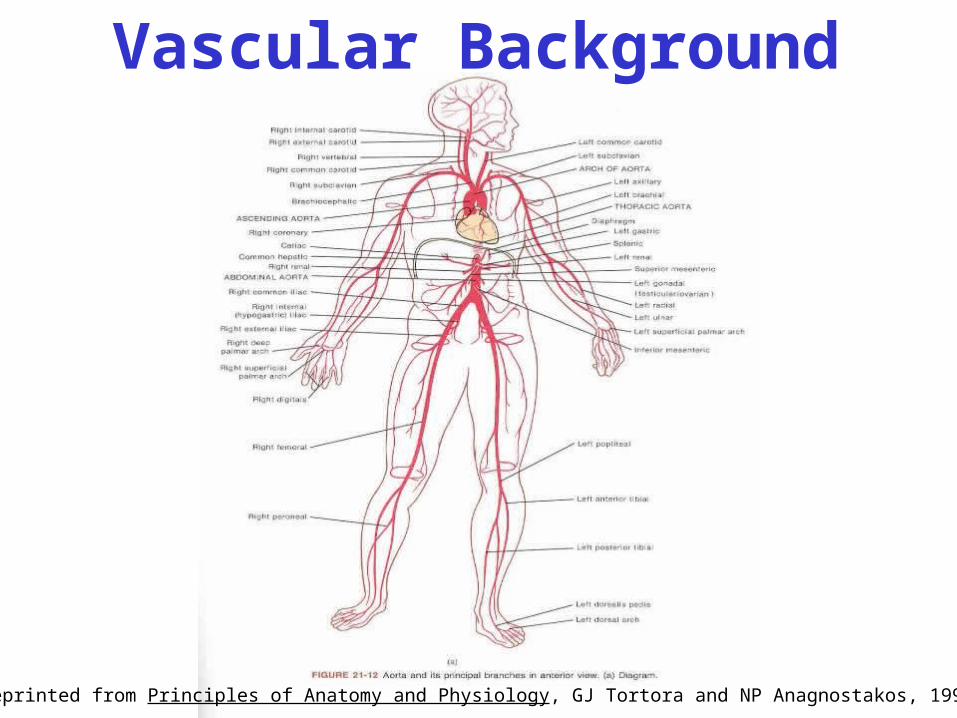
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and NP Anagnostakos, 1993
Vascular Background
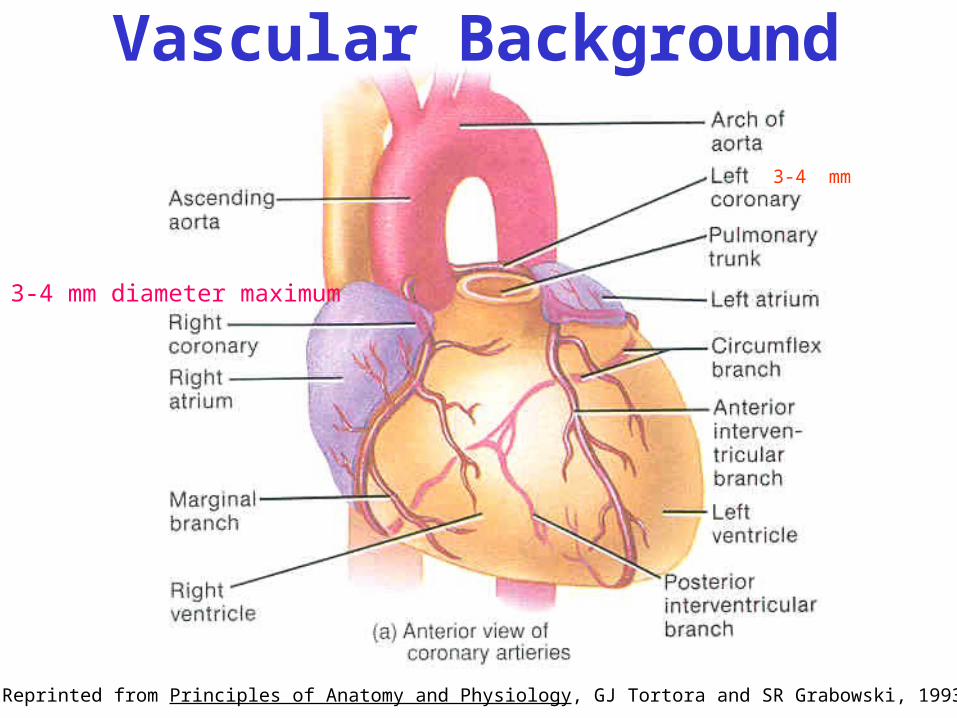
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and SR Grabowski, 1993
3-4 mm
3-4 mm diameter maximum
Vascular Background
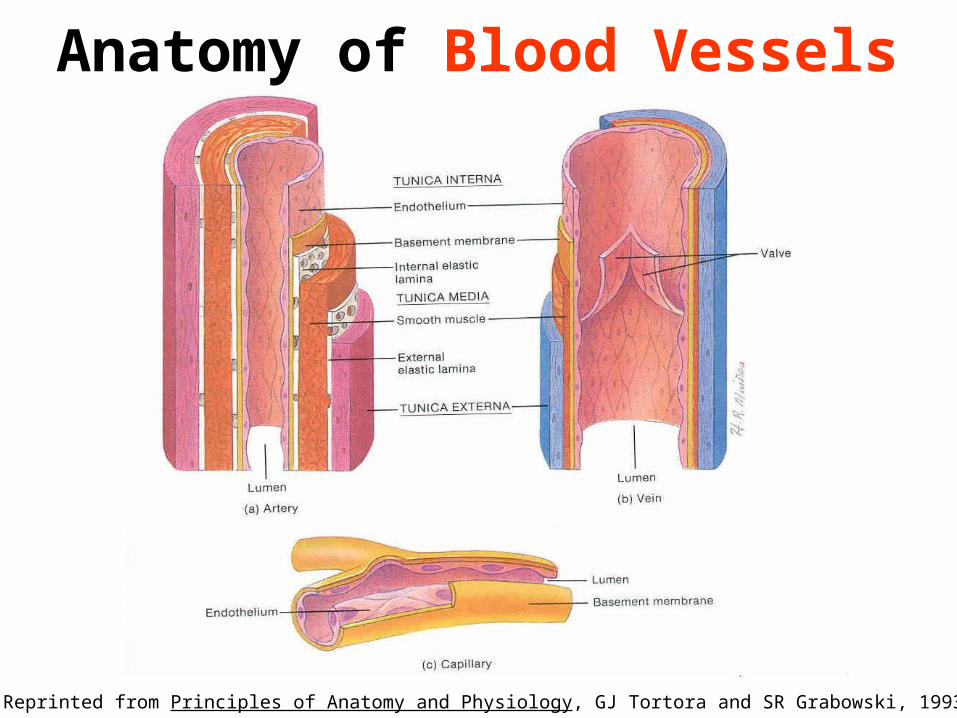
Purpose of Blood VesselsArteries - are the vessels that carry oxygenated blood
from the heart to tissues. They are categorized as large, medium, and small.
Arterioles - Deliver blood from the small arteries to the capillaries.Regulate blood flow!
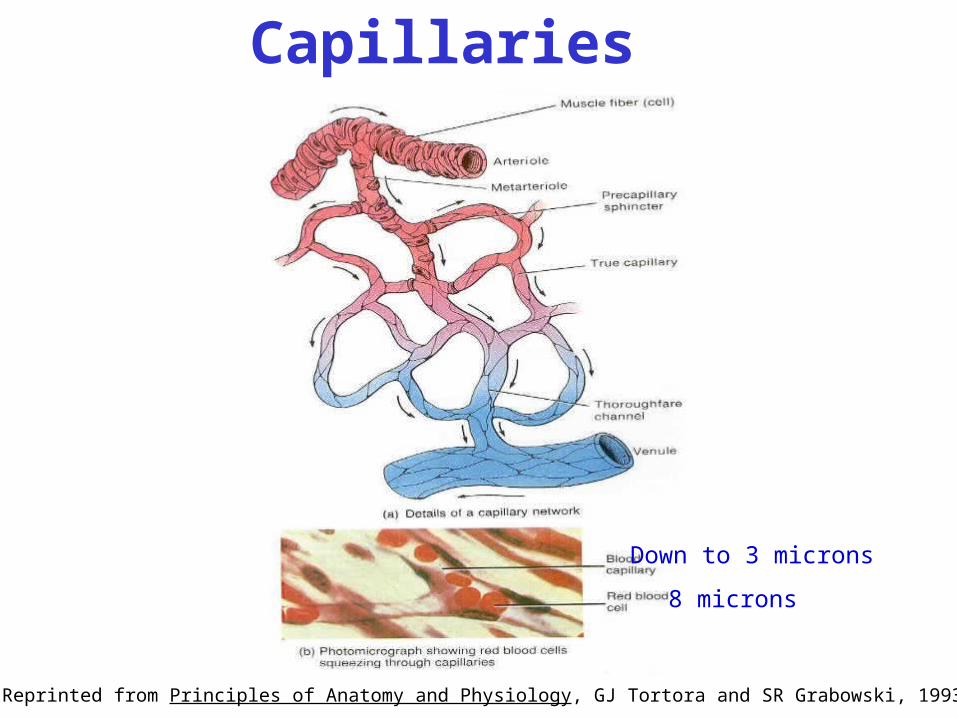
Capillaries - Branch into countless microscopic vessels in the tissue. Substance exchange between the tissue and blood stream occurs through the walls of the capillaries.
Venules - before the capillaries leave the tissue they regroup and dump in to the venules.
Veins - convey the blood back to the heart from the tissue. Run in parallel to the arteries.
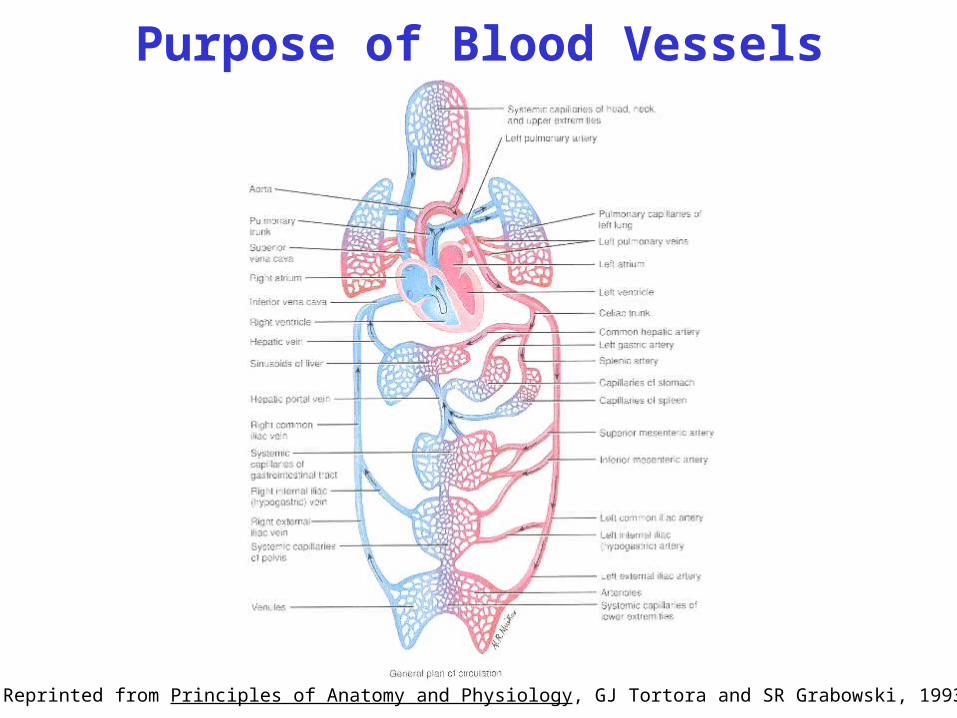
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and SR Grabowski, 1993
Purpose of Blood Vessels
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and SR Grabowski, 1993
Anatomy of Blood Vessels
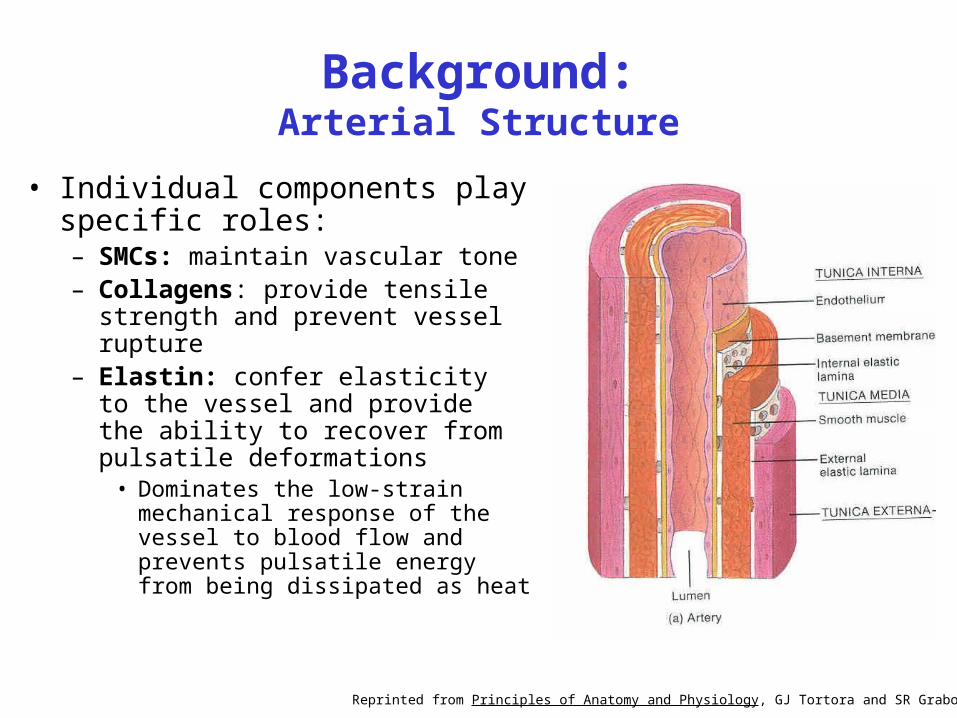
Background:Arterial Structure
• Individual components play specific roles:– SMCs: maintain vascular tone– Collagens: provide tensile strength and
prevent vessel rupture– Elastin: confer elasticity to the vessel
and provide the ability to recover from pulsatile deformations
• Dominates the low-strain mechanical response of the vessel to blood flow and prevents pulsatile energy from being dissipated as heat
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and SR Grabowski, 1993
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and SR Grabowski, 1993
8 microns
Down to 3 microns
Capillaries
Atherosclerosis
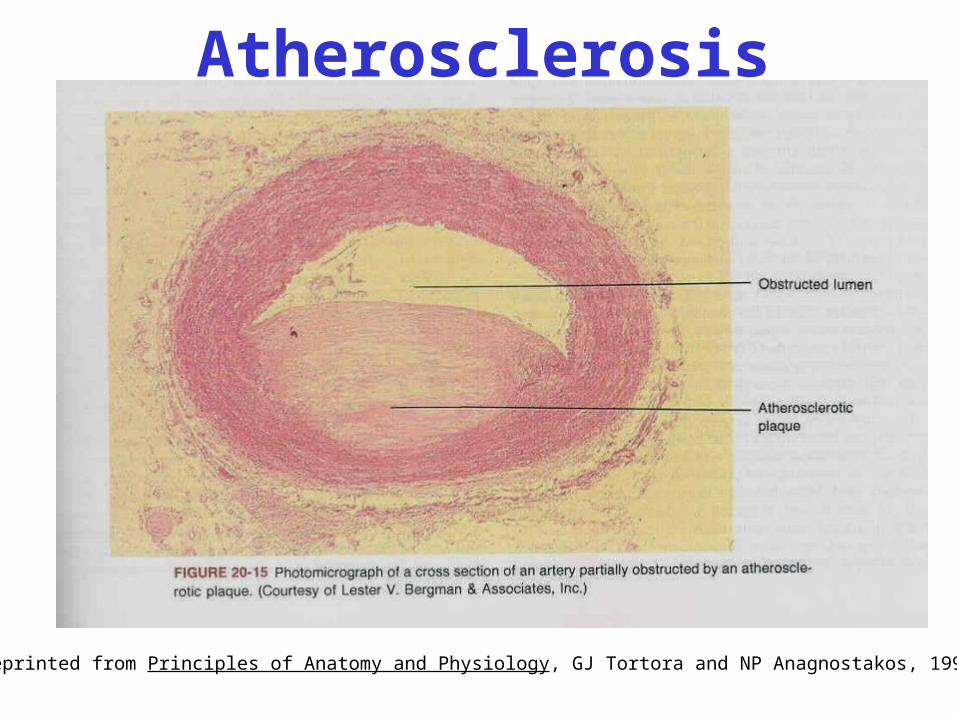
A process in which fatty substances (cholesterol and triglycerides)are deposited in the walls of arteries in response to certain stimuli (hypertension, CO2, dietary cholesterol). Following EC damage,monocytes stick to the tunica interna, develop into macrophages,and take up cholesterol and triglycerides). Smooth muscle cellsin the tunica media ingest cholesterol. This results in the formationof an atherosclerotic plague that decreases the size of the artery lumen.
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and NP Anagnostakos, 1993
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and NP Anagnostakos, 1993
Atherosclerosis
Ischemia - Reduction of blood flow.
Hypoxia - Ischemia leads to hypoxia, reduced oxygen supply. Weakens cells but does not kill them.
Claudication - The act of limping. Numbness of extremities.
Angina Pectoris - Pain in the chest associated with myocardial ischemia.
Myocardial Infarction - Serious myocardial ischemia. Means death of an area of tissue due to lack of blood supply.
Symptoms/Problems with Atherosclerosis
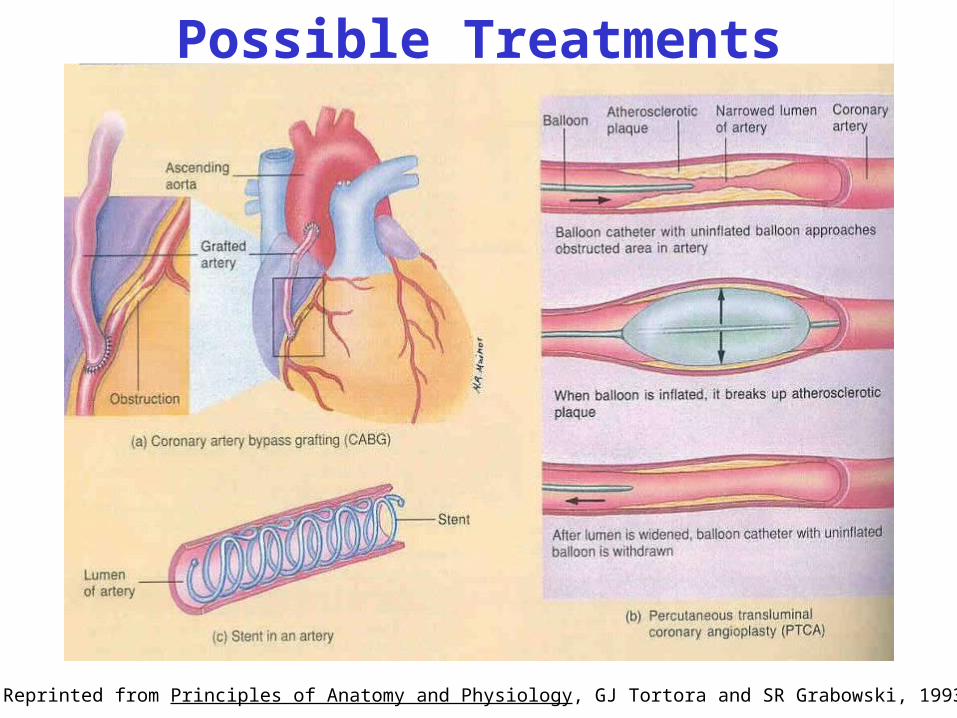
Reprinted from Principles of Anatomy and Physiology, GJ Tortora and SR Grabowski, 1993
Possible Treatments
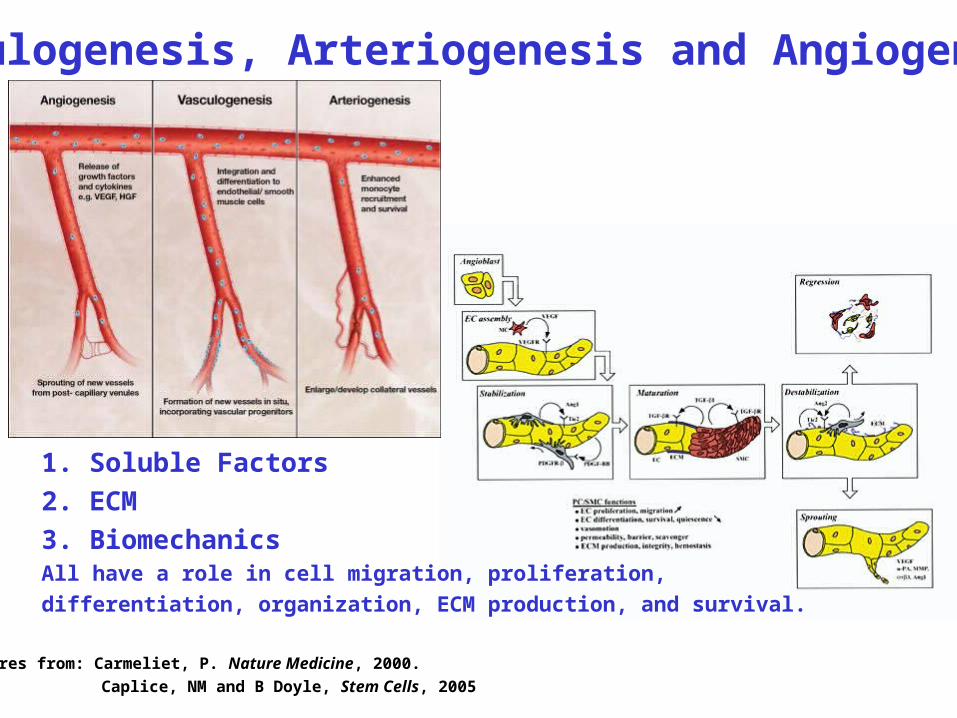
Vasculogenesis, Arteriogenesis and Angiogenesis
1. Soluble Factors
2. ECM
3. BiomechanicsAll have a role in cell migration, proliferation,
differentiation, organization, ECM production, and survival.
Figures from: Carmeliet, P. Nature Medicine, 2000.
Caplice, NM and B Doyle, Stem Cells, 2005
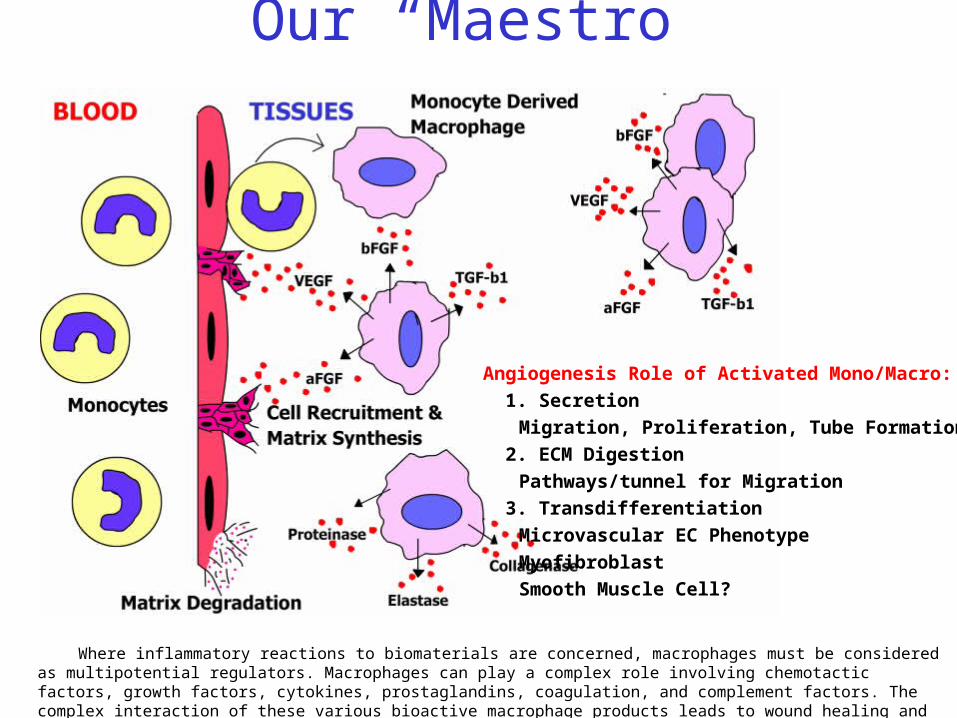
Our “Maestro”
Where inflammatory reactions to biomaterials are concerned, macrophages must be considered as multipotential regulators. Macrophages can play a complex role involving chemotactic factors, growth factors, cytokines, prostaglandins, coagulation, and complement factors. The complex interaction of these various bioactive macrophage products leads to wound healing and cellular ingrowth.
Angiogenesis Role of Activated Mono/Macro:
1. Secretion
Migration, Proliferation, Tube Formation
2. ECM Digestion
Pathways/tunnel for Migration
3. Transdifferentiation
Microvascular EC Phenotype
Myofibroblast
Smooth Muscle Cell?
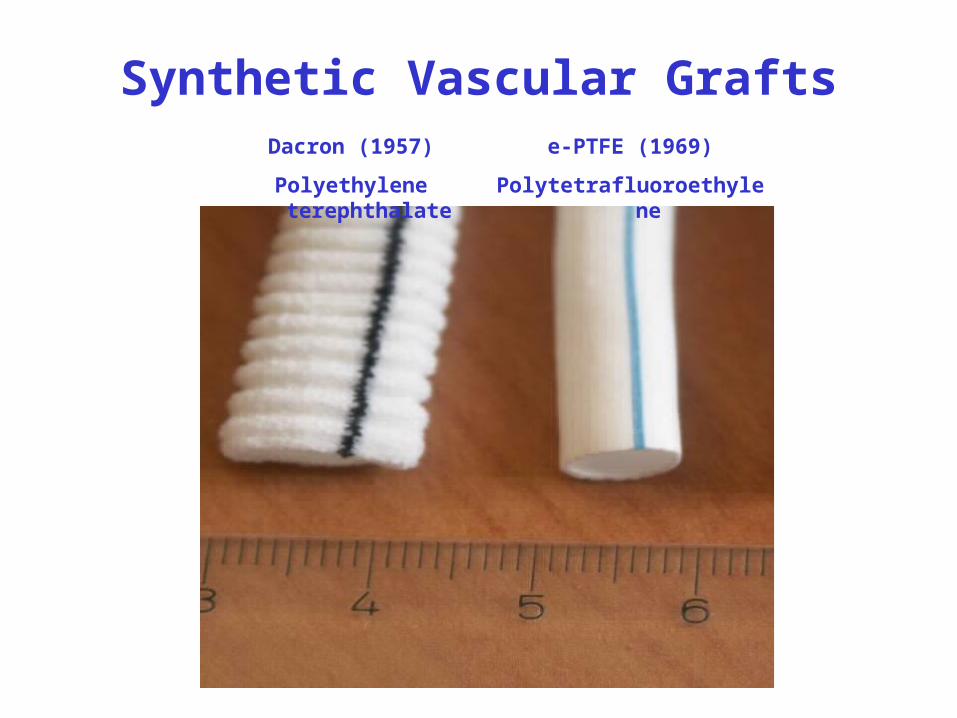
Synthetic Vascular GraftsDacron (1957)
Polyethylene terephthalate
e-PTFE (1969)
Polytetrafluoroethylene
Tissue Engineering Components
1. Scaffolding (a.k.a. extracellular matrix)GelsFibrous ScaffoldsPorous Structures
2. CellsAutologous CellsAllogenic CellsXenogenic CellsStem CellsUniversal Donor Cells
3. Signaling SystemsChemical (i.e. growth factors)Mechanical (Bioreactors)
4. Time/Physiologic Integration
5. Ethical/Moral/Social Issues

Biodegradable Scaffold and Tissue Engineered Vessel
Scaffold9 MonthsStatic Culture
Tissue Engineering Cell Source
Autologous Cells
Autologous – one’s own.
If one was to use autologous cells for the production of a tissue engineered product,the process would require starting with a biopsy of the tissue/organ which contains the cells required to replicate the desired product.
Advantage: Immune acceptable
Downsides: Limited availability not “off-the shelf” Variability between individuals Expansion in many cases limited or not possible.
Alternative Method: Implantation of an appropriate acellular matrix that has the capacity to recruit and develop the proper cell lines.
Types of Cells in BodyBased on the Proliferative Potential
1. Renewing or Liable (e.g. skin)
Continuous turnover, balances losses
2. Expanding or Stable (e.g. liver)
Capable of proliferation if needed
3. Permanent or Static (e.g. heart)
No proliferative capacity
Tissue Engineering Cell SourceAllogenic Cells – Source same species.
This type of cell source is or could be readily available through tissue/cell banks.
Limitations:1. Tissue donations2. Proliferative capacity in vitro3. Potential for genetic engineering to be immune acceptable
Benefits:1. Can grow and preserve large quantity of cells, thus “off-the-shelf”2. Potentially a reproducible source3. Cost effective
Xenogenic Cells – source different species
Tissue Engineering Cell Source
This type of cell source is or could be readily available through tissue/cell banks.
Limitations:1. Rejection2. Cost – harvest and maintain3. Proliferative capacity in vitro
Genetic engineering could eliminate or reduce these limitations.
Benefits:1. Can grow and preserve large quantity of cells2. Potentially a reproducible source
Main concern with this source is the potential for animal virus transmission.
Tissue Engineering Cell SourceStem Cells – Pluripotent cells
Types of Stem Cells:1. Embryonic stem cells
derived from embryos 2. Adult stem cells
undifferentiated cells in tissues and organs Examples of adult stem cells:
Hematopoietic stem cellsMesenchymal stem cellsNeural stem cellsEpithelial stem cellsBrain stem cells
Limitations:1. In vitro culture capacity2. Differentiation
Big question then is there a single stem cell that exists in the bonemarrow, blood stream, tissues, or organs that can be universally used.
Tissue Engineering Cell SourceUniversal Donor Cells – U.S. Patent 5,705,732
The concept here is to genetically engineer a cell to provide it with protection form hyperacute rejection brought about by complementsystem-based lysis.
At the same time, the genetic engineering causes the cells not to present proteins produced by the class I and II major histocompatibility complex genes on the cell surface. This eliminates attack from the T-cells.
What is created are immunologically neutral cells.
Finally, the cells can be genetically altered with a self-destruction mechanism so that they can be removed from the host when and if desired.
Ethical/Moral/Social Issues
Should we be altering, re-engineering Mother Nature?Who defines “Quality of Life”? Research (academia) vs. Industry – Funding of research/development and control
of Intellectual Property.Does academia need to further develop the field?Will Industry/Venture Capitalists Invest?Minimizing conflicts of interest.Should life saving technology be patented and controlled exclusively?
Are animal models justified?How should human research be performed? Informed consent?
Regulatory IssuesWho determines testing protocols?Who determines what is enough testing?Who and What determines safety and efficacy?
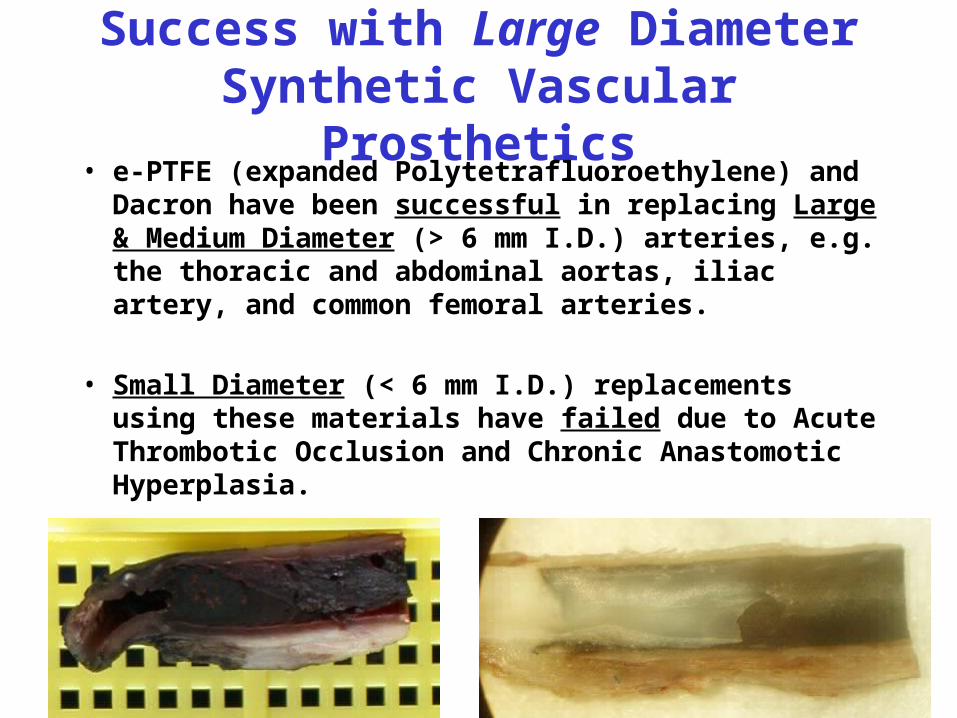
Success with Large Diameter Synthetic Vascular Prosthetics
• e-PTFE (expanded Polytetrafluoroethylene) and Dacron have been successful in replacing Large & Medium Diameter (> 6 mm I.D.) arteries, e.g. the thoracic and abdominal aortas, iliac artery, and common femoral arteries.
• Small Diameter (< 6 mm I.D.) replacements using these materials have failed due to Acute Thrombotic Occlusion and Chronic Anastomotic Hyperplasia.
“Ideal” Vascular Prosthetic “Search for the Holy Grail” – M.S. Conte 1998
Ease of Handling Durable
Suture Retention Packaging and Handling
Ease of Suture Placement After Tissue Ingrowth
Flexible with Kink Resistance Appropriate Remodeling Response
Biocompatible Porous
Non-toxic Leak Resistant but Promote Healing/Regeneration
Non-thrombogenic Compliance Matching Native Artery
Resist Aneurysm Formation
Infection Resistant
Characteristics:
Other Concerns:Easily Manufactured Available in a Variety of Sizes
Easily Stored Lengths, Diameters, and Tapers
Economical
Basically, clinicians are demanding off-the-shelf availability (especially for emergency cases) as provided by current polymeric vascular prosthetics without the short and long-term complications. All these requirements create a daunting challenge.
Bioresorbable Vascular Prosthetic History
The origin of the concept for a bioresorbable graft is credited to Claude Guthrie who in 1919 wrote “To restore and maintain mechanical function an implanted segment only temporarily restores mechanical continuity and serves as a scaffolding or bridge for the laying down of an ingrowth of tissue derived from the host.”
The actual application of a bioresorbable material for use as a vascular prosthetic was first reported by Wesolowski et al. in the early 1960’s utilizing fabrics composed of a variety of Dacron yarns, collagen coatings, and collagen fibers.
Bioresorbable Vascular Prosthetic History (1970’s)
Dr. Ingvar Eriksson and associates in the late 1970’s pioneered the use of PLGA (Vicryl (polyglactin 910)) as a suture mesh graft where the mesh had a fiber diameter of 140 microns with a pore size of 400x400 microns. This large pore size required pre-clotting, but after pre-clotting hemostasis was achieved in minutes after implantation.
The PLGA mesh structure upon implantation in a pig aorta model (4 cm diameter graft) allowed early in-growth of smooth muscle cells (SMCs) from the native aorta to form a neo-media which was completely endothelialized within 20 days. The PLGA mesh almost completely degraded within 40 days, however the neo-artery wall retained sufficient strength through the observed time with very little dispersed elastin deposition.
Bioresorbable Vascular Prosthetic History (1980’s)
In the early 1980’s, Dr. Howard Greisler and associates utilized a similar PGA mesh tube (250 micron fiber diameter and 400 micron pore size; length = 2.5 cm) in a rabbit aortic model of regeneration. The results after 7.5 months were that a significant number of animals exhibited mild graft/aorta dilation and hyperplasia with the regenerated graft wall composed of myofibroblasts and dense collagen matrix.
Overall, they concluded that the PGA bioresorbable structure permitted some degree of arterial regeneration. However, at 6 months the histological evaluation revealed lipid laden macrophages and histiocytes, suggesting the early development of arteriosclerosis.
Bioresorbable Vascular Prosthetic History (1980’s)
In 1987, Howard Greisler and associates published results utilizing PDS absorbable vascular prosthetics made by the same technique utilized for the PGA scaffolds just discussed (Rabbit model).
Implanted grafts (length = 2.5 cm) were evaluated at 2 weeks up to 12 months with one out of all the 28 evaluated having a small aneurysm and no perigraft hematomas. The myofibroblast migration paralleled the macrophage-mediated degradation of the PDS structure, which was delayed relative to the PGA structures.
A confluent endothelial cell (EC) lining was present within two weeks with the mechanical properties of the explants at 1 year resembling artery elasticity (compliance). Finally, the regenerated aorta segments at 1 year withstood 1200 mm Hg of systolic pressure.
All these implant studies elicit more tissue in-growth of smooth muscle cell- like myofibroblasts and more rapid EC lining development when compared to Dacron or e-PTFE in the animal models.
Speculation by the authors is that the enhanced EC lining is due to transinterstitial migration of capillaries and the overall healing is initiated largely by the macrophages being activated by the polymer interaction.
A 1988 study by this group, verified transinterstitial migration of capillaries to form the neo-intima. Additionally, the PDS based grafts (4 mm diameter) had patency rates significantly higher than Dacron and e-PTFE controls.
Bioresorbable Vascular Prosthetic History (1980’s)
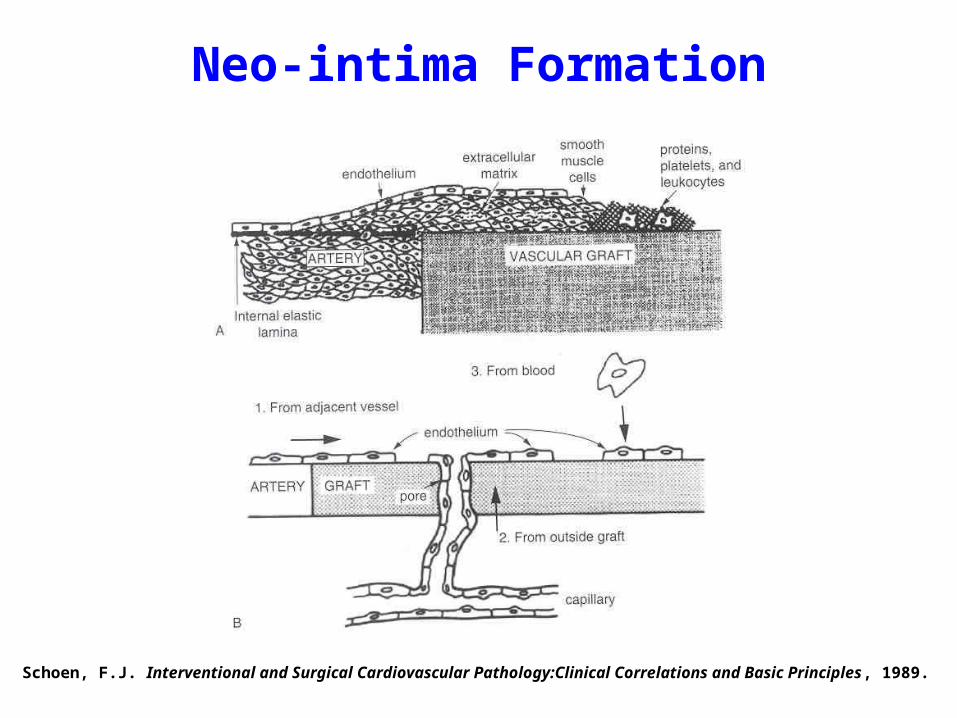
Schoen, F.J. Interventional and Surgical Cardiovascular Pathology:Clinical Correlations and Basic Principles , 1989.
Neo-intima Formation
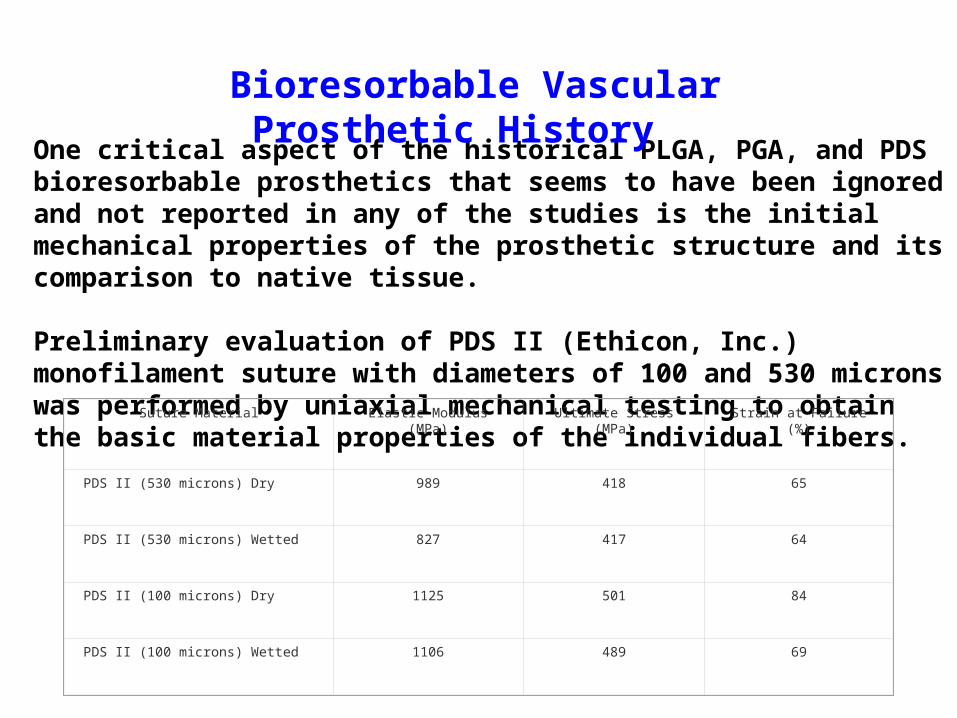
One critical aspect of the historical PLGA, PGA, and PDS bioresorbable prosthetics that seems to have been ignored and not reported in any of the studies is the initial mechanical properties of the prosthetic structure and its comparison to native tissue.
Preliminary evaluation of PDS II (Ethicon, Inc.) monofilament suture with diameters of 100 and 530 microns was performed by uniaxial mechanical testing to obtain the basic material properties of the individual fibers.
Bioresorbable Vascular Prosthetic History
Suture Material Elastic Modulus (MPa) Ultimate Stress (MPa) Strain at Failure (%)
PDS II (530 microns) Dry 989 418 65
PDS II (530 microns) Wetted 827 417 64
PDS II (100 microns) Dry 1125 501 84
PDS II (100 microns) Wetted 1106 489 69
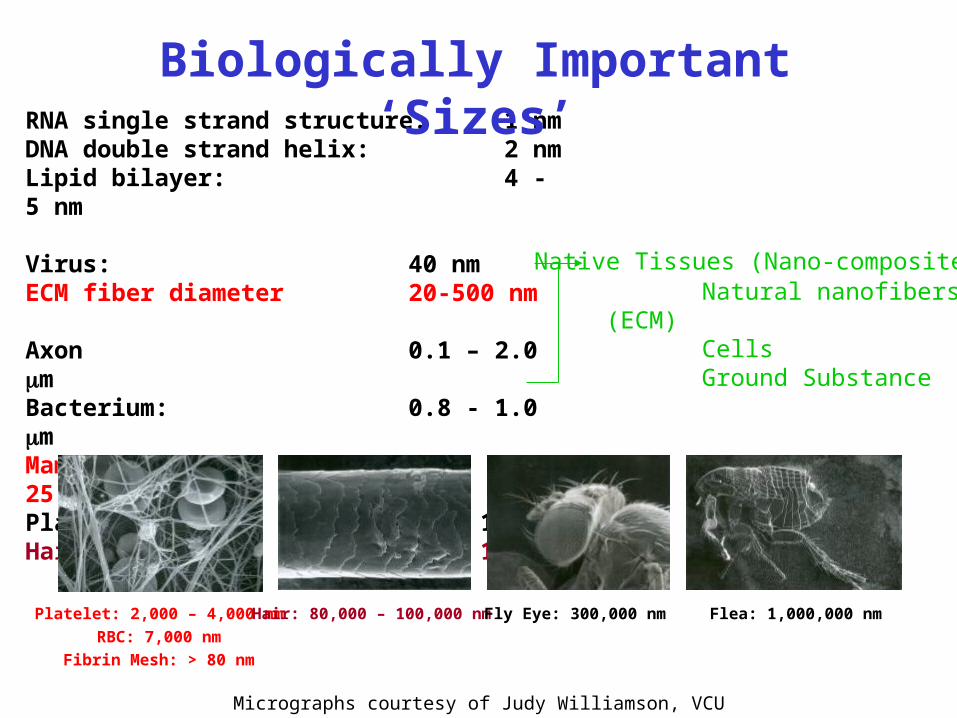
RNA single strand structure: 1 nm DNA double strand helix: 2 nmLipid bilayer: 4 - 5 nm
Virus: 40 nmECM fiber diameter 20-500 nm
Axon 0.1 – 2.0 mBacterium: 0.8 - 1.0 mMammalian cell: 5 - 25 mPlant cell: 70 - 100 mHair Shaft 80 - 100 m
Biologically Important ‘Sizes’
Micrographs courtesy of Judy Williamson, VCU
Platelet: 2,000 – 4,000 nm
RBC: 7,000 nm
Fibrin Mesh: > 80 nm
Hair: 80,000 – 100,000 nm Fly Eye: 300,000 nm Flea: 1,000,000 nm
Native Tissues (Nano-composites):Natural nanofibers (ECM)CellsGround Substance
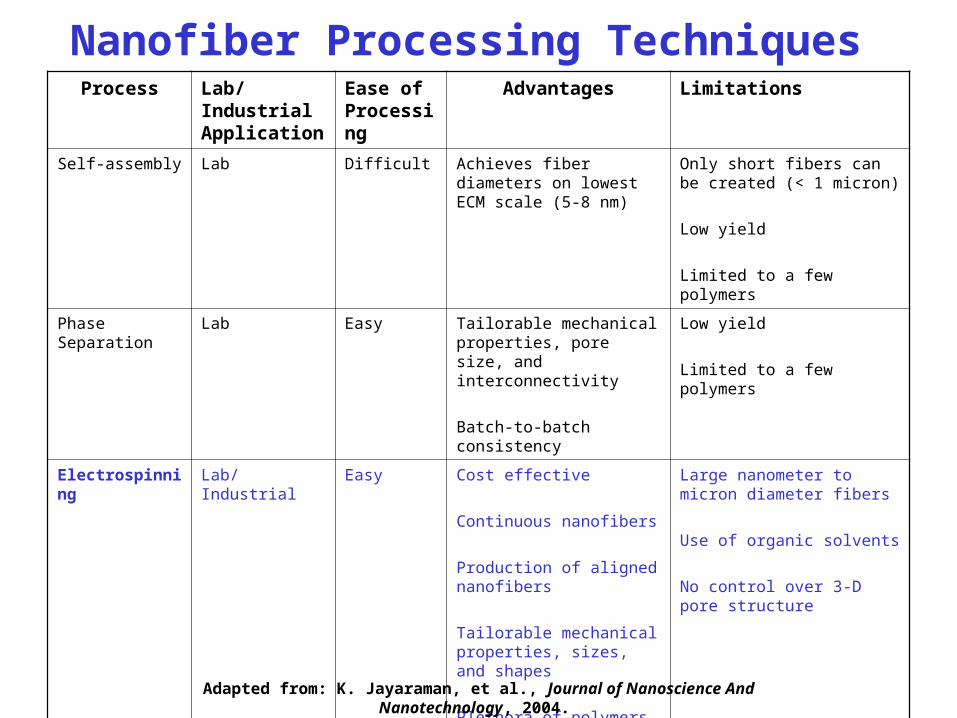
Process Lab/Industrial Application
Ease of Processing
Advantages Limitations
Self-assembly Lab Difficult Achieves fiber diameters on lowest ECM scale (5-8 nm)
Only short fibers can be created (< 1 micron)
Low yield
Limited to a few polymers
Phase Separation Lab Easy Tailorable mechanical properties, pore size, and interconnectivity
Batch-to-batch consistency
Low yield
Limited to a few polymers
Electrospinning Lab/Industrial Easy Cost effective
Continuous nanofibers
Production of aligned nanofibers
Tailorable mechanical properties, sizes, and shapes
Plethora of polymers may be used
Large nanometer to micron diameter fibers
Use of organic solvents
No control over 3-D pore structure
Nanofiber Processing Techniques
Adapted from: K. Jayaraman, et al., Journal of Nanoscience And Nanotechnology, 2004.
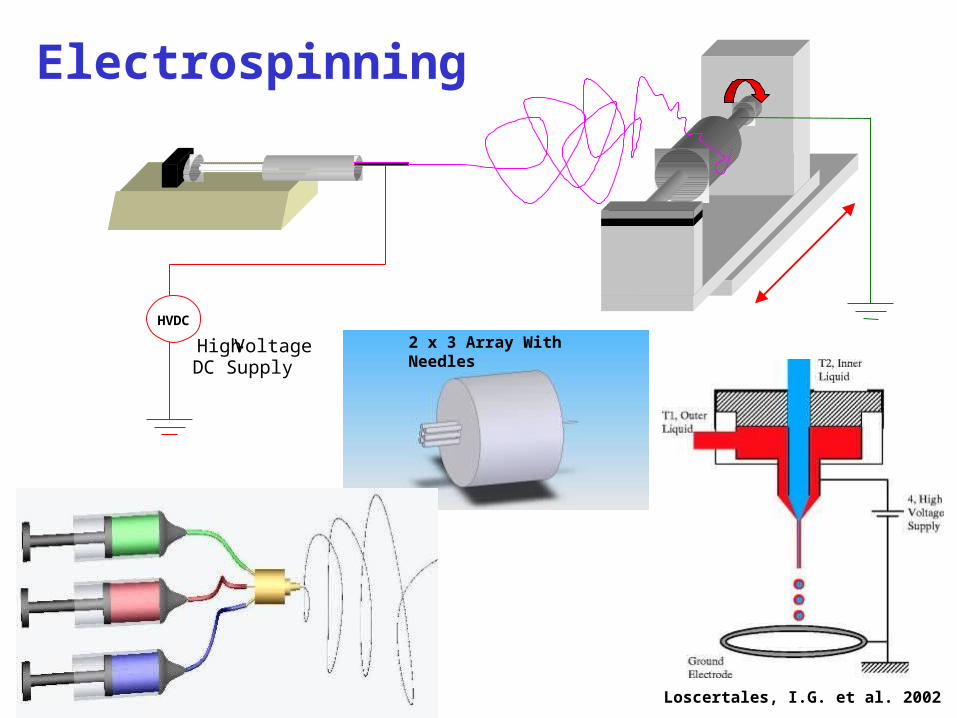
Electrospinning
HVDC
High-VoltageDC Supply
Loscertales, I.G. et al. 2002
2 x 3 Array With Needles
Specific Aim 1: To electrospin bioresorbable polymers to form nano- to micro-fibrous, seamless vascular prosthetic constructs for potential use as an acellular vascular prosthetic.
Specific Aim 2: To perform mechanical characterization of the electrospun nano- to micro-fiber structures. The mechanical evaluations will include stress-strain, burst strength, permeability, and suture retention.
Specific Aim 3: To perform in vivo evaluation of the vascular constructs using a rat subcutaneous model to evaluate biocompatibility and regeneration potential.
Specific Aim 4: To perform in situ evaluation of the vascular constructs using a large animal femoral artery model to evaluate long-term in vivo mechanical performance as well as the thromboresistance and regeneration capacities of the prosthetic.
The hypothesis of this study is that an electrospun composite composed of natural and synthetic polymers will be comparable mechanically (e.g., burst strength and suture retention) to current clinically used prosthetics and/or a native small caliber artery. The corollary is that the in vivo performance of the electrospun composites is capable of promoting the full regeneration of a functional arterial segment. The hypothesis and corollary will be tested using in vitro and in vivo experimental validation.
Overall Research Aims
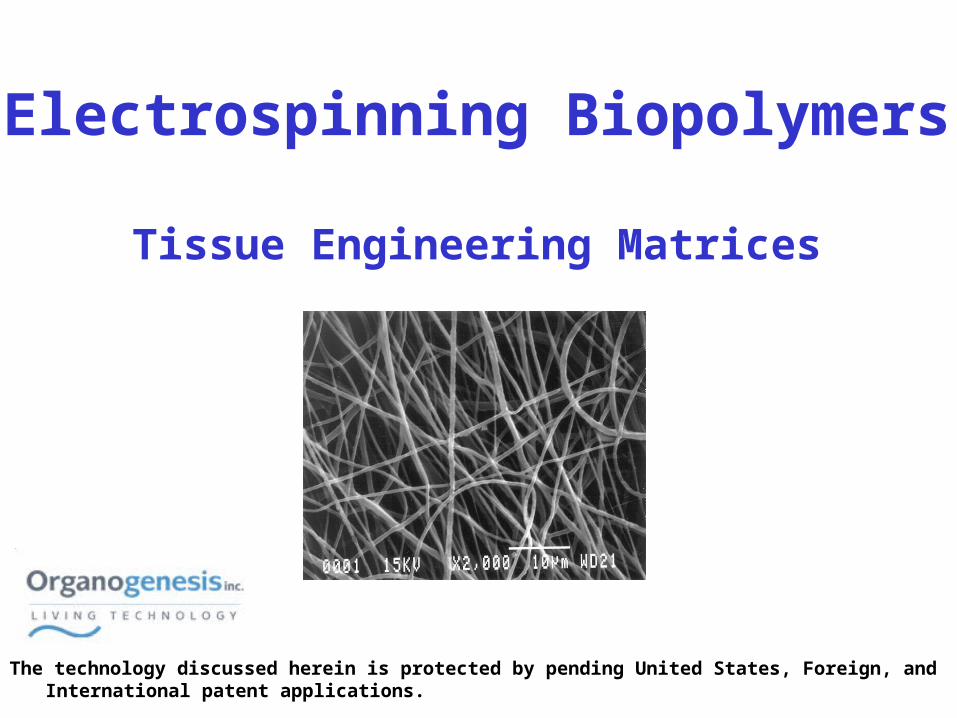
Electrospinning Biopolymers
Tissue Engineering Matrices
The technology discussed herein is protected by pending United States, Foreign, and International patent applications.
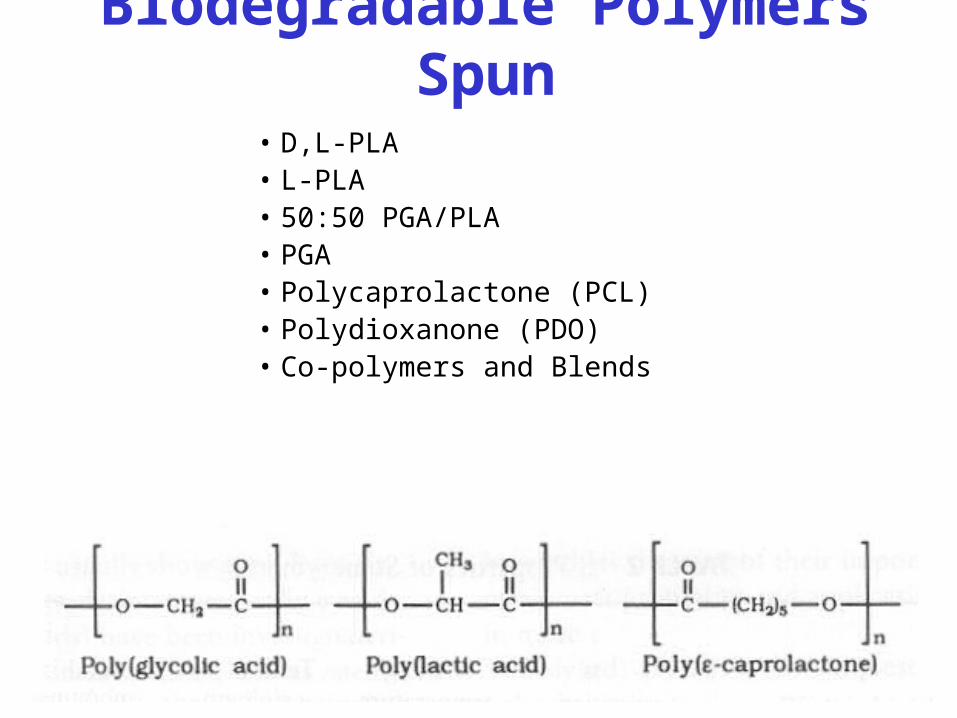
Biodegradable Polymers Spun• D,L-PLA • L-PLA • 50:50 PGA/PLA • PGA• Polycaprolactone (PCL)• Polydioxanone (PDO)• Co-polymers and Blends
y = 0.0101x - 0.2875
R2 = 0.969
0
0.5
1
1.5
2
2.5
25 75 125 175
Concentration (mg/ml)
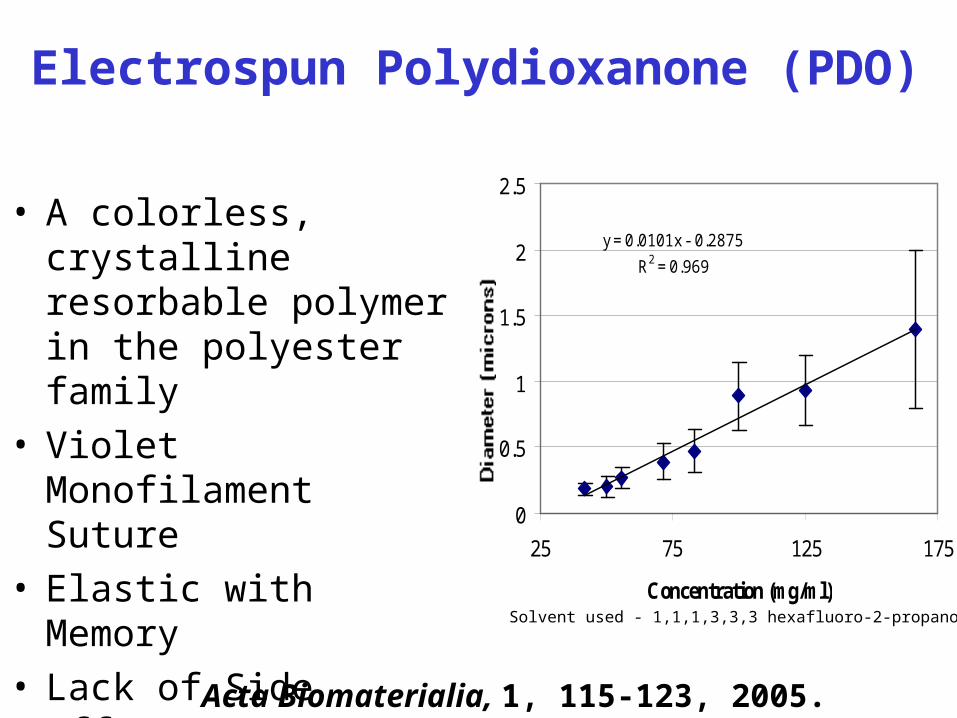
• A colorless, crystalline resorbable polymer in the polyester family
• Violet Monofilament Suture• Elastic with Memory• Lack of Side Effects
Inflammation
Electrospun Polydioxanone (PDO)
Solvent used - 1,1,1,3,3,3 hexafluoro-2-propanol
Acta Biomaterialia, 1, 115-123, 2005.
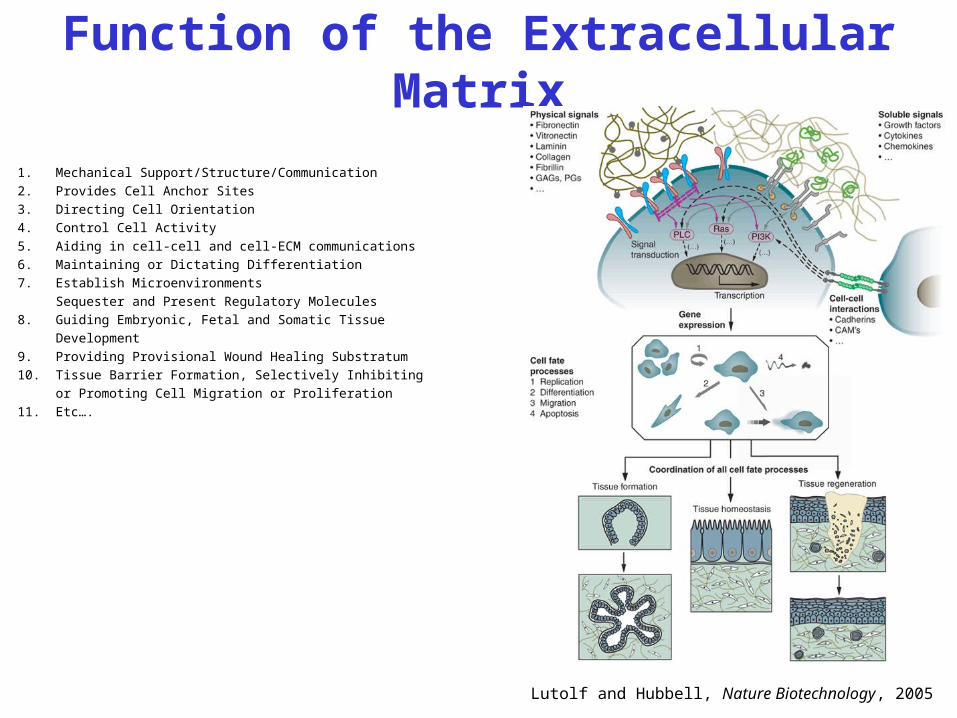
Function of the Extracellular Matrix
1. Mechanical Support/Structure/Communication
2. Provides Cell Anchor Sites
3. Directing Cell Orientation
4. Control Cell Activity
5. Aiding in cell-cell and cell-ECM communications
6. Maintaining or Dictating Differentiation
7. Establish Microenvironments
Sequester and Present Regulatory Molecules
8. Guiding Embryonic, Fetal and Somatic Tissue
Development
9. Providing Provisional Wound Healing Substratum
10. Tissue Barrier Formation, Selectively Inhibiting
or Promoting Cell Migration or Proliferation
11. Etc….
Lutolf and Hubbell, Nature Biotechnology, 2005
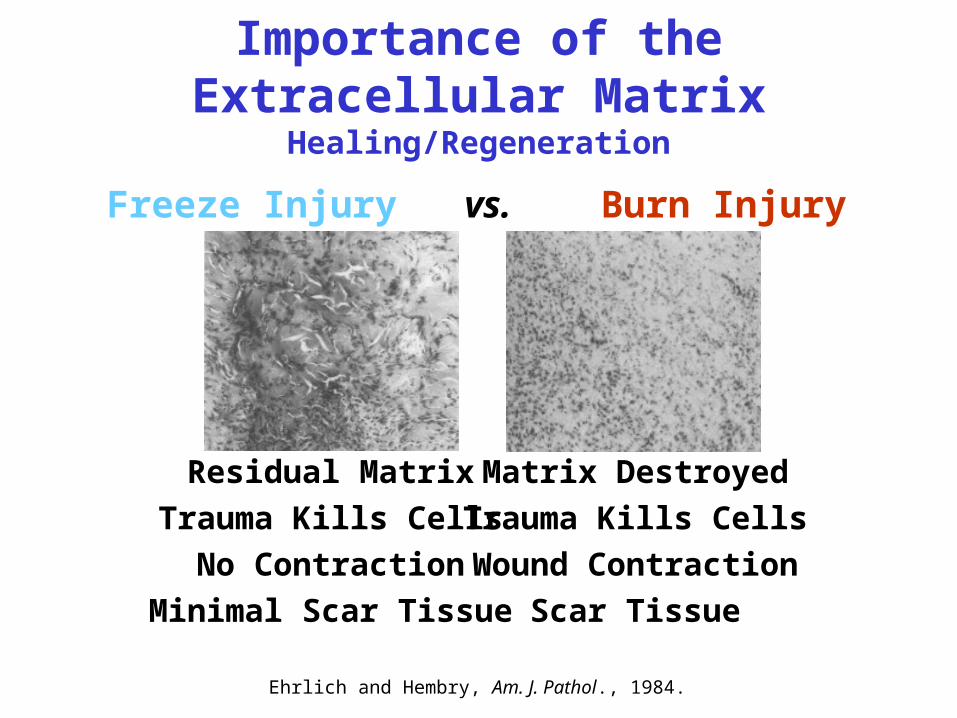
Importance of the Extracellular Matrix Healing/Regeneration
Freeze Injury vs. Burn Injury
Ehrlich and Hembry, Am. J. Pathol., 1984.
Residual Matrix
Trauma Kills Cells
No Contraction
Minimal Scar Tissue
Matrix Destroyed
Trauma Kills Cells
Wound Contraction
Scar Tissue
Natural Polymers (Proteins) Electrospun• Collagen Type I
Calf Skin, Human Placenta, Rat Tail
• Collagen Type II
Chicken Sternal Cartilage
• Collagen Type III
Human Placenta
• Collagen Type IVHuman Placenta
• Elastin
• FibrinogenHuman and Bovine, Fraction 1 from Plasma
• Hemoglobin
• Myoglobin
• Blends {Globular
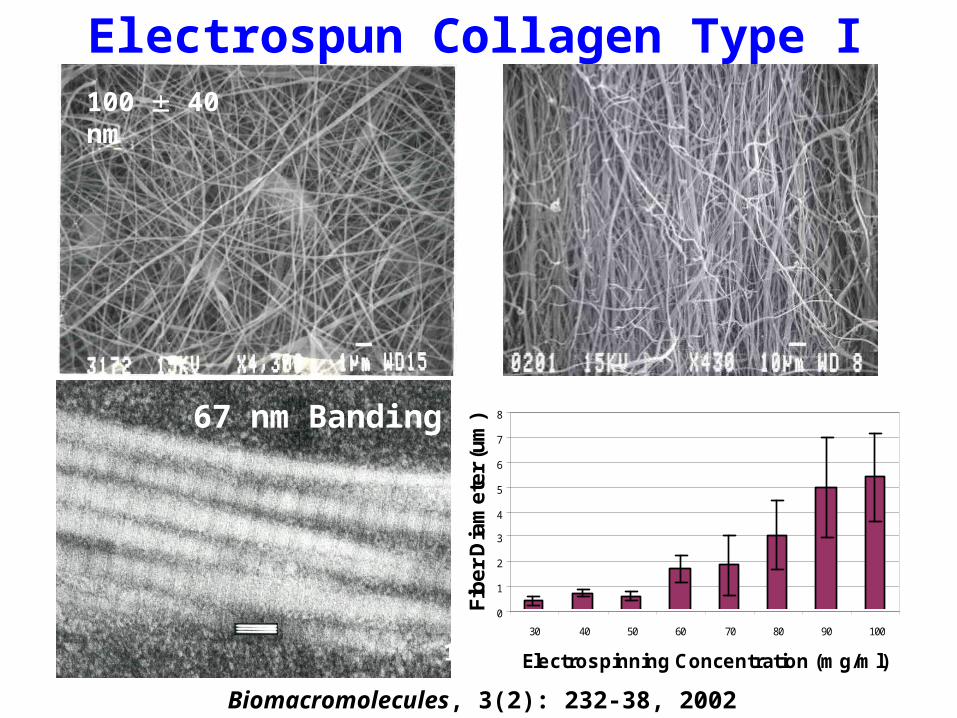
Electrospun Collagen Type I
110 40 nm
100 40 nm
Biomacromolecules, 3(2): 232-38, 2002
67 nm Banding
100 nm
0
1
2
3
4
5
6
7
8
30 40 50 60 70 80 90 100
Electrospinning Concentration (mg/ml)
Fib
er
Dia
met
er
(um
)
Electrospun Biopolymer Scaffold
Immune Response
The technology discussed herein is protected by pending United States, Foreign, and International patent applications.
• Dose-response
• Time-course effects
Electrospun Biopolymer ScaffoldMonocyte & Macrophage Interactions
Transforming Growth Factor β ELISA
• Macrophages were seeded on 10 mm circular discs of electrospun Polydioxanone, collagen and blends (50:50, 70:30, 90:10) at a density of 400,000 cells/well in a 48 well plate.
• Cell culture Supernatants were tested for the presence of TGF-β on day 7, 14, 21, 28.
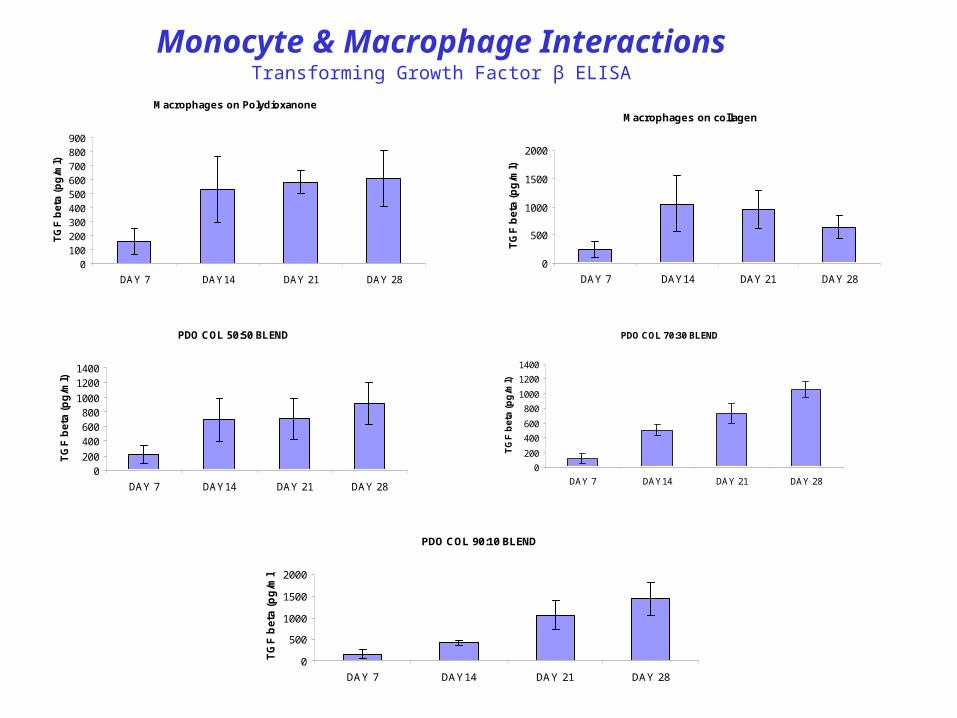
Macrophages on Polydioxanone
0100200300400500600700800900
DAY 7 DAY14 DAY 21 DAY 28
TG
F b
eta
(pg
/ml)
Macrophages on collagen
0
500
1000
1500
2000
DAY 7 DAY14 DAY 21 DAY 28
TG
F b
eta
(pg
/ml)
PDO COL 50:50 BLEND
0200
400600800
1000
12001400
DAY 7 DAY14 DAY 21 DAY 28
TG
F b
eta
(pg
/ml)
PDO COL 70:30 BLEND
0
200
400
600
800
1000
1200
1400
DAY 7 DAY14 DAY 21 DAY 28
TG
F b
eta
(pg
/ml)
PDO COL 90:10 BLEND
0
500
1000
1500
2000
DAY 7 DAY14 DAY 21 DAY 28
TG
F b
eta
(p
g/m
l)
Monocyte & Macrophage InteractionsTransforming Growth Factor β ELISA
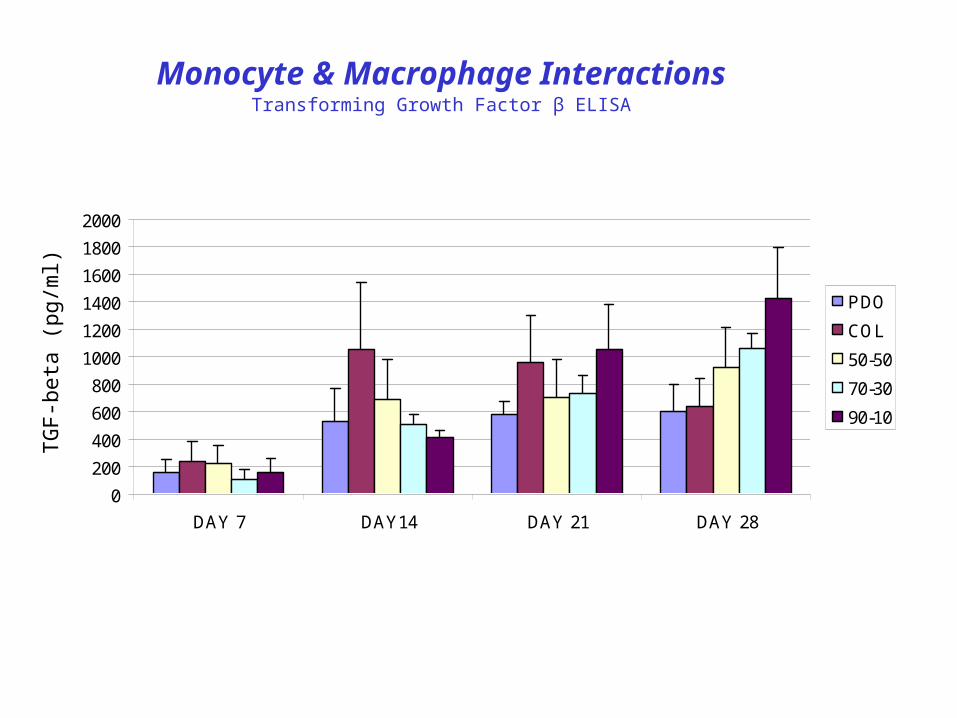
Monocyte & Macrophage InteractionsTransforming Growth Factor β ELISA
0
200
400
600
800
1000
1200
1400
1600
1800
2000
DAY 7 DAY14 DAY 21 DAY 28
PDO
COL
50-50
70-30
90-10TG
F-b
eta
(pg/
ml)
Electrospun Biopolymer ScaffoldIn Vitro Immune Testing
The technology discussed herein is protected by pending United States, Foreign, and International patent applications.
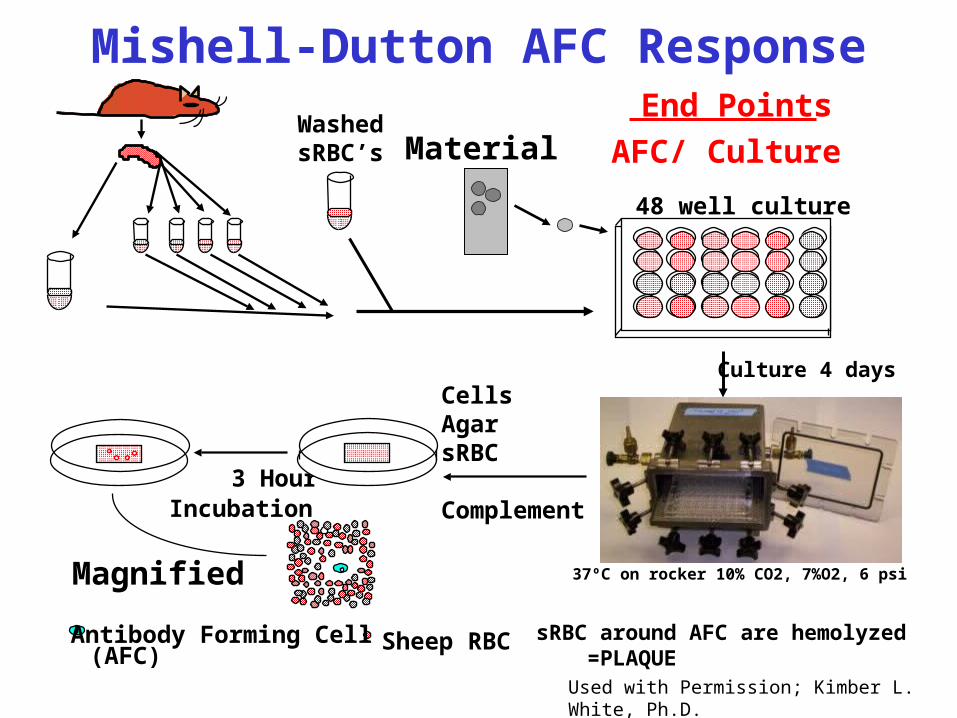
Material
3 Hour Incubation
WashedsRBC’s
48 well culture
End Points
AFC/ Culture
CellsAgarsRBC
Complement
Culture 4 days
37ºC on rocker 10% CO2, 7%O2, 6 psiMagnified
sRBC around AFC are hemolyzed =PLAQUE
Sheep RBC(AFC)Antibody Forming Cell
Used with Permission; Kimber L. White, Ph.D.
Mishell-Dutton AFC Response
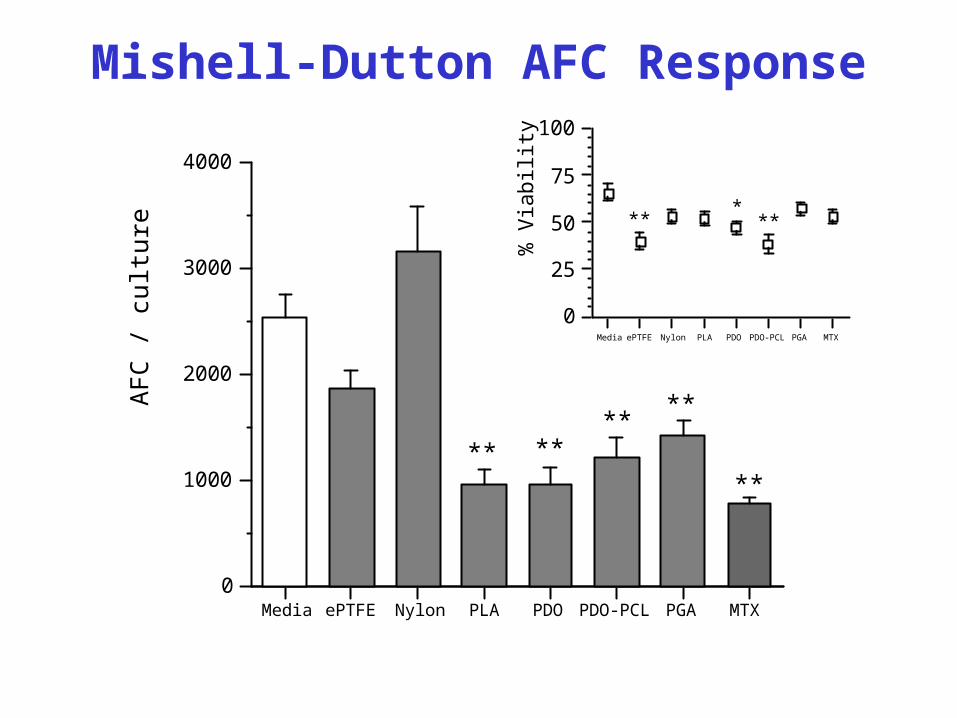
Mishell-Dutton AFC Response
0
1000
2000
3000
4000A
FC
/ c
ultu
re
Media ePTFE Nylon PLA PDO PDO-PCL PGA MTX
****
****
**
0
25
50
75
100
% V
iabi
lity
Media ePTFE Nylon PLA PDO PDO-PCL PGA MTX
** ***
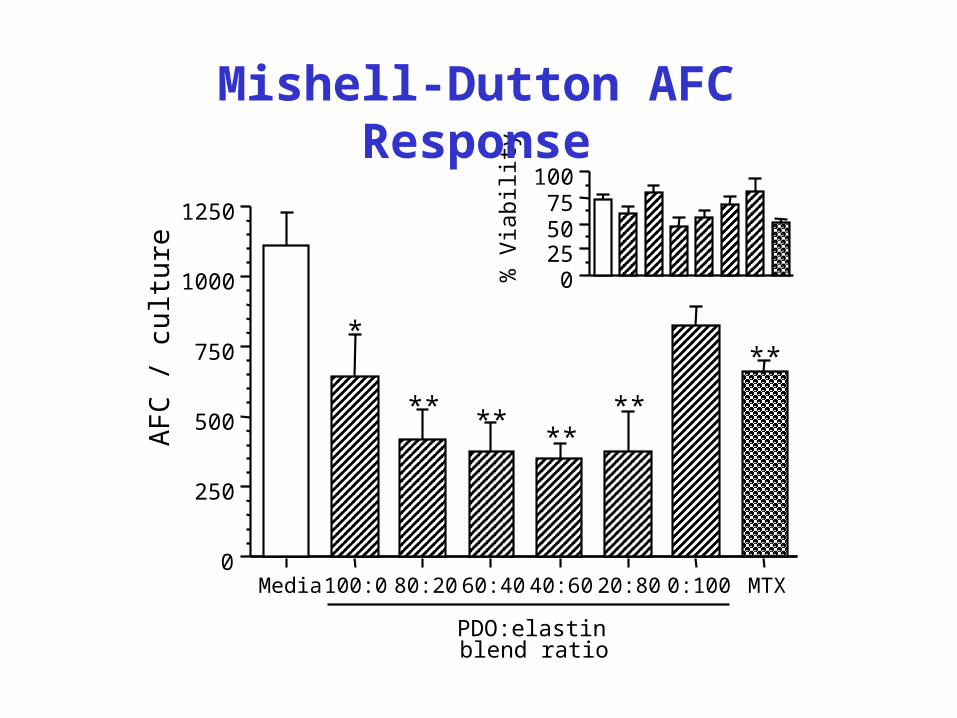
0
250
500
750
1000
1250
AF
C /
cul
ture
Media 100:0 80:20 60:40 40:60 20:80 0:100 MTX
PDO:elastin blend ratio
0255075
100
% V
iabi
lity
*
** ****
**
**
Mishell-Dutton AFC Response
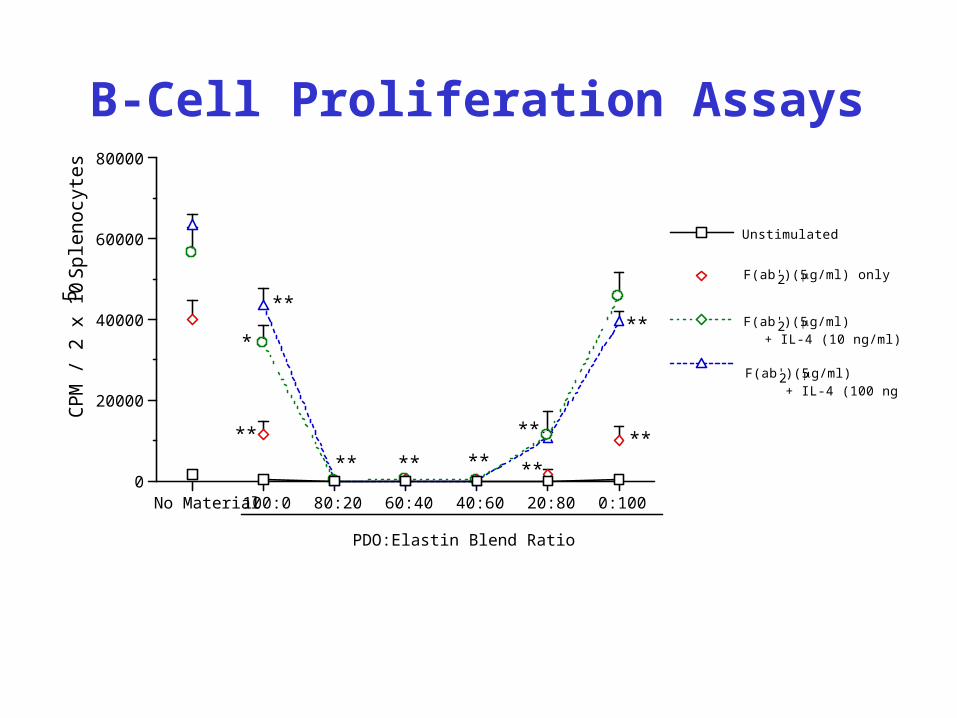
*
CP
M /
2 x
10
5 S
ple
no
cyte
s
0
20000
40000
60000
80000
No Material 100:0 80:20 60:40 40:60 20:80 0:100
PDO:Elastin Blend Ratio
**
**
** ** **
**
**
**
** F(ab')2 (5 g/ml) + IL-4 (10 ng/ml)
F(ab')2 (5 g/ml) + IL-4 (100 ng/ml)
F(ab')2 (5 g/ml) only
Unstimulated
B-Cell Proliferation Assays
The technology discussed herein is protected by pending United States, Foreign, and International patent applications.
Electrospun Collagen/Elastin and Polydioxanone:
Vascular Tissue Engineering
Collagen/Elastin for “bioactivity”
PDO for “strength” and macrophage activation
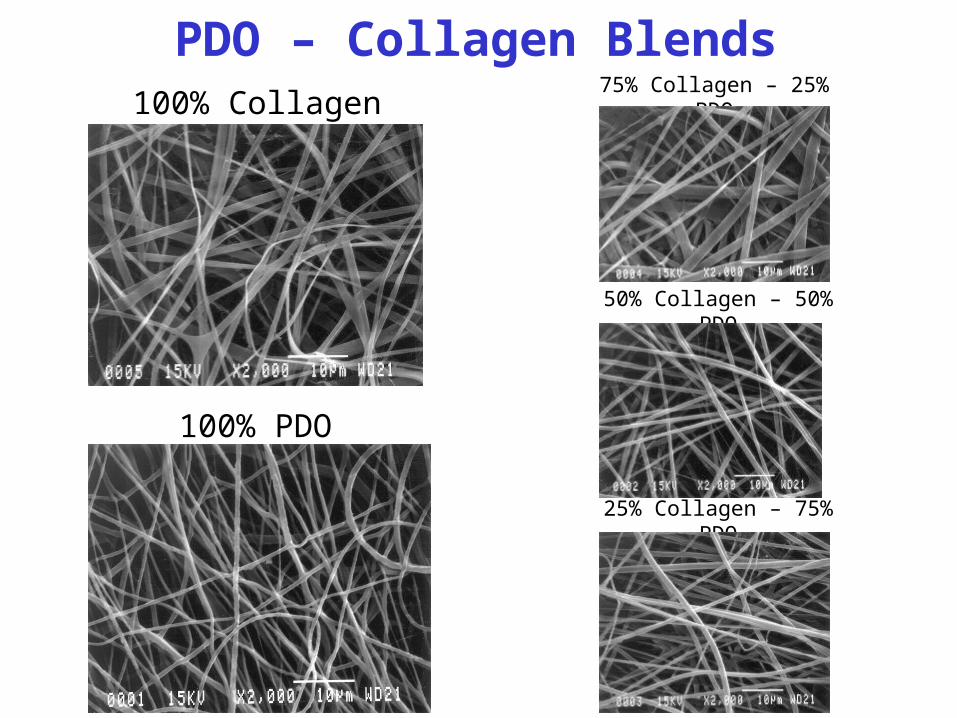
100% Collagen 75% Collagen – 25% PDO
50% Collagen – 50% PDO
25% Collagen – 75% PDO
100% PDO
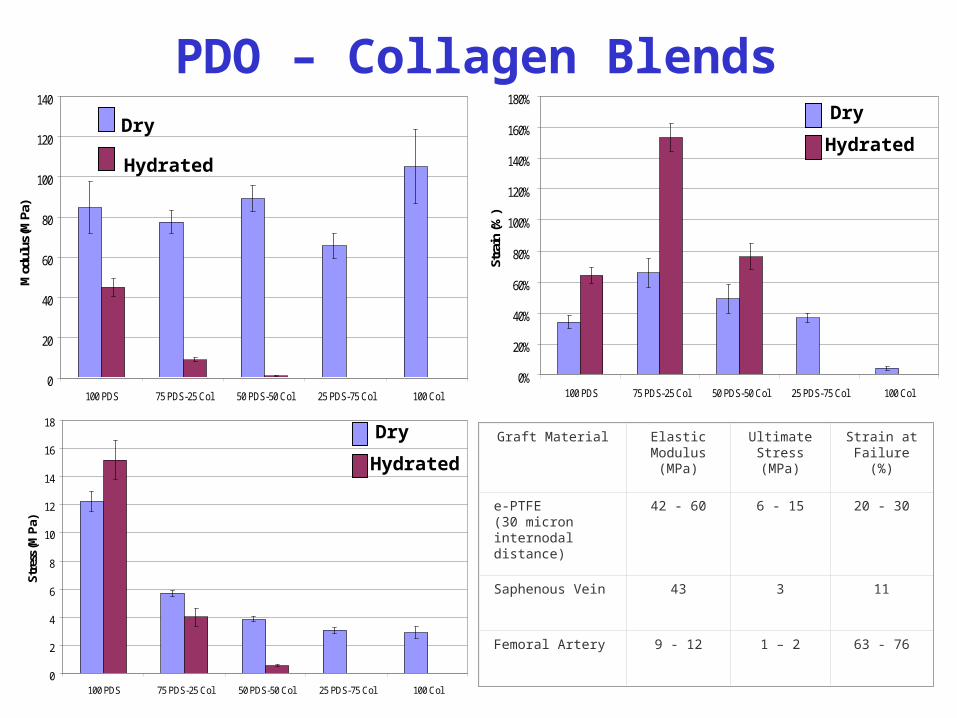
PDO – Collagen Blends
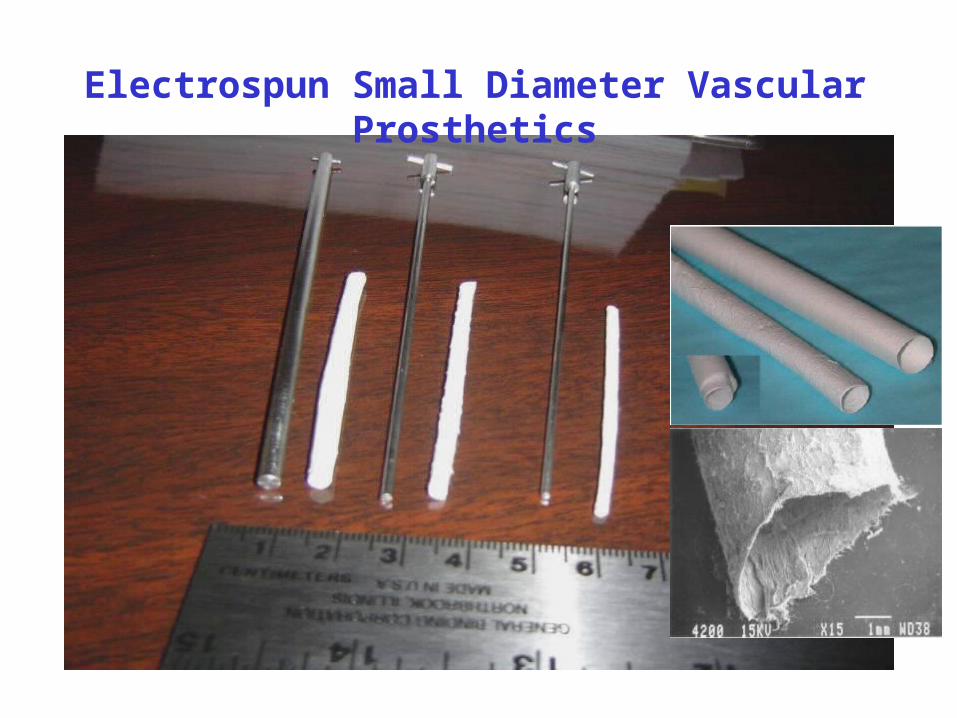
Electrospun Small Diameter Vascular Prosthetics
0
20
40
60
80
100
120
140
100 PDS 75 PDS-25 Col 50 PDS-50 Col 25 PDS-75 Col 100 Col
Mod
ulus
(MPa
)
0
2
4
6
8
10
12
14
16
18
100 PDS 75 PDS-25 Col 50 PDS-50 Col 25 PDS-75 Col 100 Col
Stre
ss (M
Pa)
0%
20%
40%
60%
80%
100%
120%
140%
160%
180%
100 PDS 75 PDS-25 Col 50 PDS-50 Col 25 PDS-75 Col 100 Col
Stra
in (%
)
Graft Material Elastic Modulus (MPa)
Ultimate Stress (MPa)
Strain at Failure (%)
e-PTFE(30 micron internodal distance)
42 - 60 6 - 15 20 - 30
Saphenous Vein 43 3 11
Femoral Artery 9 - 12 1 – 2 63 - 76
PDO – Collagen BlendsDry
Hydrated
Dry
Hydrated
Dry
Hydrated
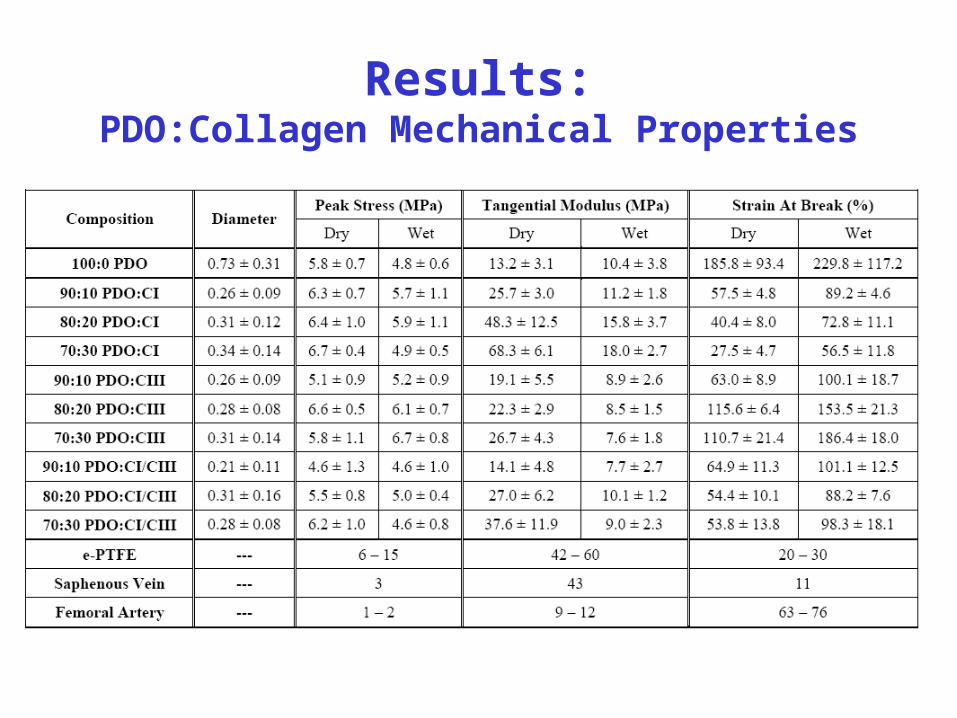
Results:PDO:Collagen Mechanical Properties
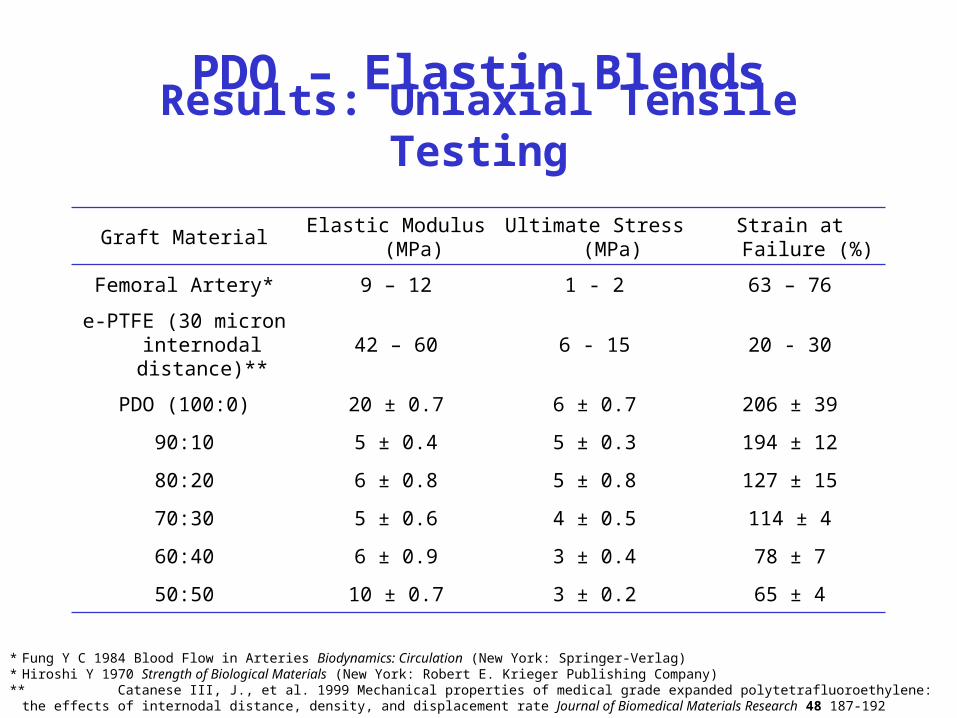
Results: Uniaxial Tensile Testing
Graft MaterialElastic Modulus
(MPa)Ultimate Stress (MPa) Strain at Failure (%)
Femoral Artery* 9 – 12 1 - 2 63 – 76
e-PTFE (30 micron internodal
distance)**42 – 60 6 - 15 20 - 30
PDO (100:0) 20 ± 0.7 6 ± 0.7 206 ± 39
90:10 5 ± 0.4 5 ± 0.3 194 ± 12
80:20 6 ± 0.8 5 ± 0.8 127 ± 15
70:30 5 ± 0.6 4 ± 0.5 114 ± 4
60:40 6 ± 0.9 3 ± 0.4 78 ± 7
50:50 10 ± 0.7 3 ± 0.2 65 ± 4
* Fung Y C 1984 Blood Flow in Arteries Biodynamics: Circulation (New York: Springer-Verlag)* Hiroshi Y 1970 Strength of Biological Materials (New York: Robert E. Krieger Publishing Company)** Catanese III, J., et al. 1999 Mechanical properties of medical grade expanded polytetrafluoroethylene: the effects of internodal distance, density, and
displacement rate Journal of Biomedical Materials Research 48 187-192
PDO – Elastin Blends
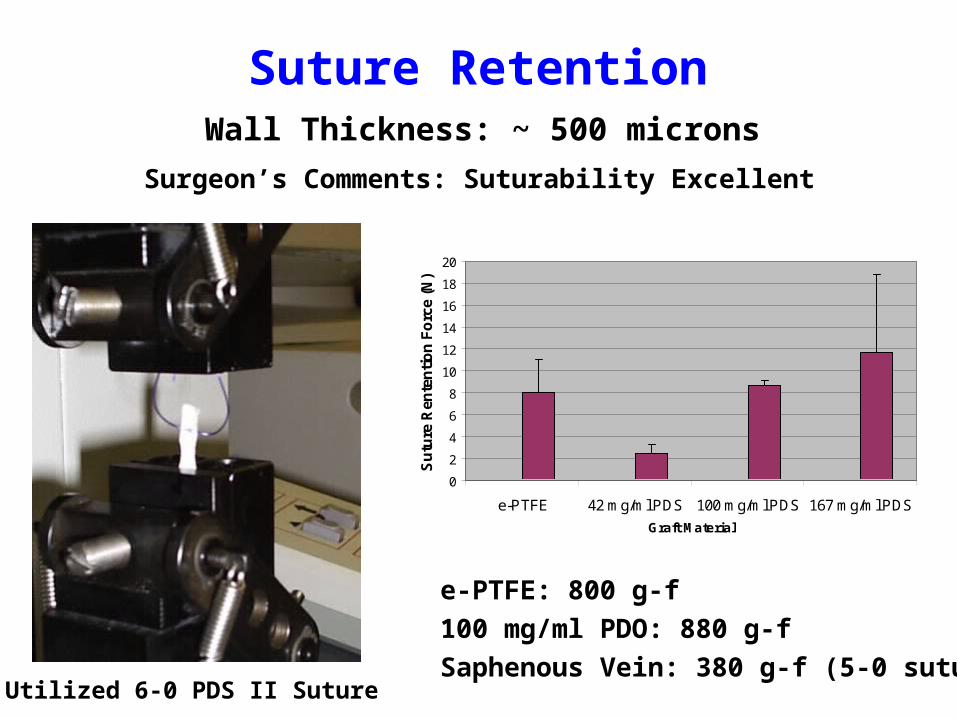
Suture Retention
Utilized 6-0 PDS II Suture
0
2
4
6
8
10
12
14
16
18
20
e-PTFE 42 mg/ml PDS 100 mg/ml PDS 167 mg/ml PDS
Graft Material
Su
ture
Ren
ten
tio
n F
orc
e (N
)
e-PTFE: 800 g-f
100 mg/ml PDO: 880 g-f
Saphenous Vein: 380 g-f (5-0 suture)
Surgeon’s Comments: Suturability Excellent
Wall Thickness: ~ 500 microns
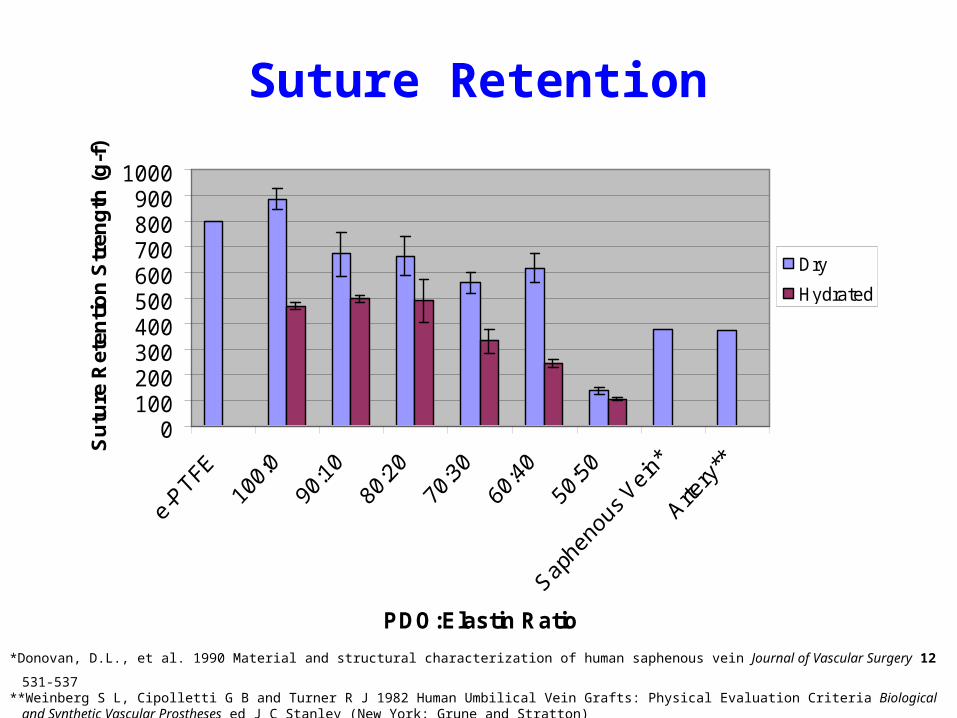
0100200300400500600700800900
1000
PDO:Elastin Ratio
Su
ture
Ret
enti
on
Str
eng
th (
g-f
)
Dry
Hydrated
*Donovan, D.L., et al. 1990 Material and structural characterization of human saphenous vein Journal of Vascular Surgery 12 531-537**Weinberg S L, Cipolletti G B and Turner R J 1982 Human Umbilical Vein Grafts: Physical Evaluation Criteria Biological and Synthetic Vascular Prostheses ed
J C Stanley (New York: Grune and Stratton)
Suture Retention
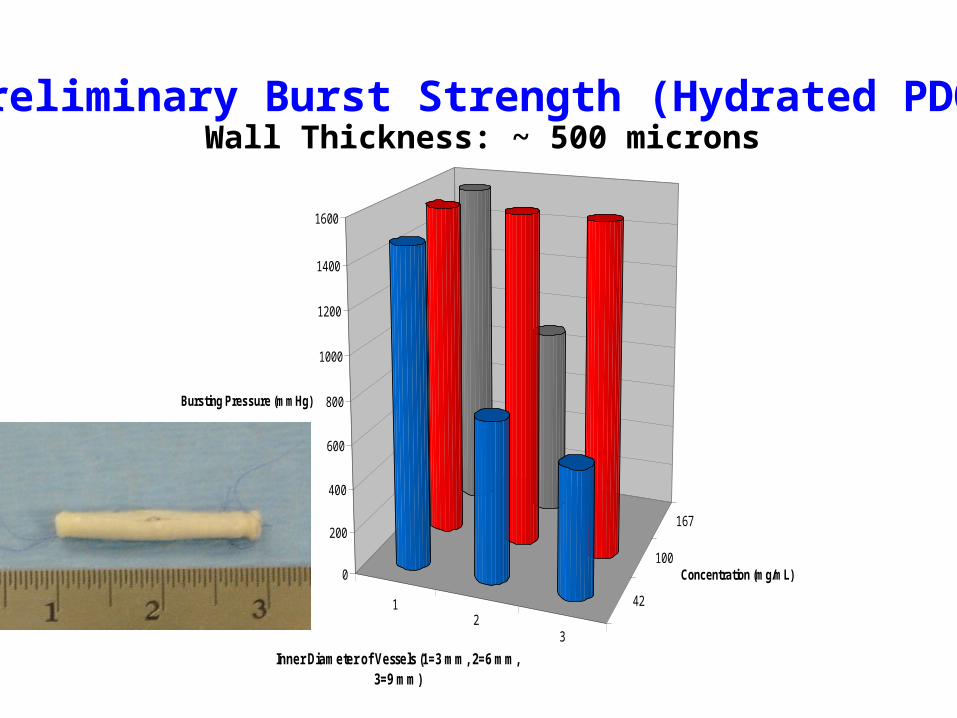
12
3
42
100
167
0
200
400
600
800
1000
1200
1400
1600
Bursting Pressure (mmHg)
Inner Diameter of Vessels (1=3 mm, 2=6 mm, 3=9 mm)
Concentration (mg/mL)
Preliminary Burst Strength (Hydrated PDO)Wall Thickness: ~ 500 microns
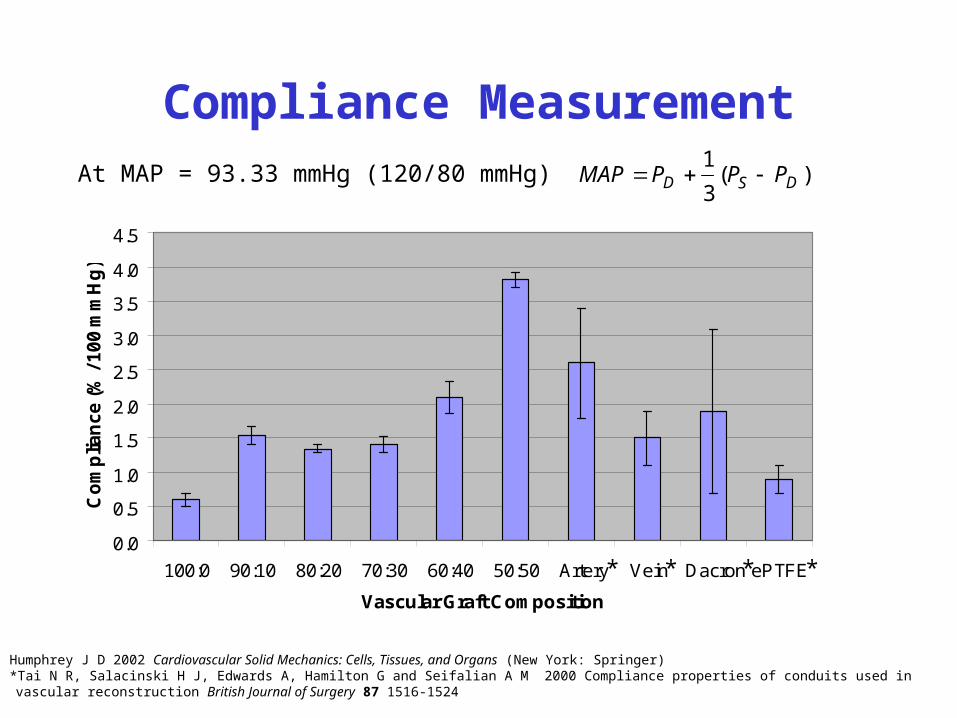
Compliance Measurement
Humphrey J D 2002 Cardiovascular Solid Mechanics: Cells, Tissues, and Organs (New York: Springer) *Tai N R, Salacinski H J, Edwards A, Hamilton G and Seifalian A M 2000 Compliance properties of conduits used in vascular reconstruction British Journal of Surgery 87 1516-1524
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
100:0 90:10 80:20 70:30 60:40 50:50 Artery Vein Dacron ePTFE
Vascular Graft Composition
Co
mp
lian
ce (%
/ 100 m
mH
g)
* ***
)(3
1DSD PPPMAP At MAP = 93.33 mmHg (120/80 mmHg)
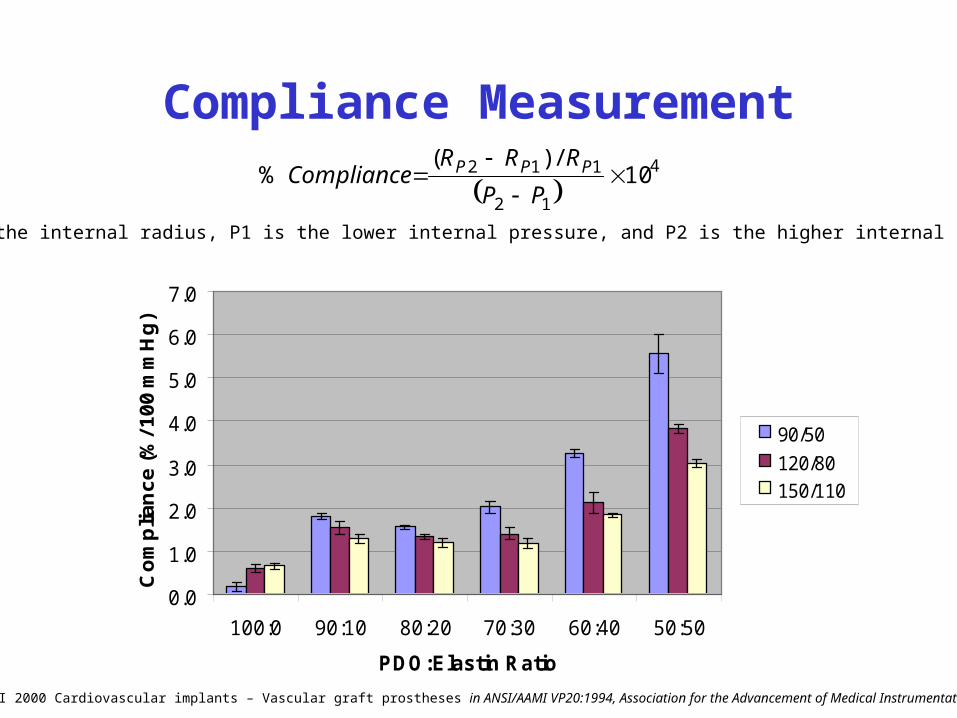
Compliance Measurement
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
100:0 90:10 80:20 70:30 60:40 50:50
PDO:Elastin Ratio
Co
mp
lian
ce
(%
/ 10
0 m
mH
g)
90/50
120/80
150/110
4
12
112 10/)(
%
PP
RRRCompliance PPP
ANSI 2000 Cardiovascular implants – Vascular graft prostheses in ANSI/AAMI VP20:1994, Association for the Advancement of Medical Instrumentation
R is the internal radius, P1 is the lower internal pressure, and P2 is the higher internal pressure
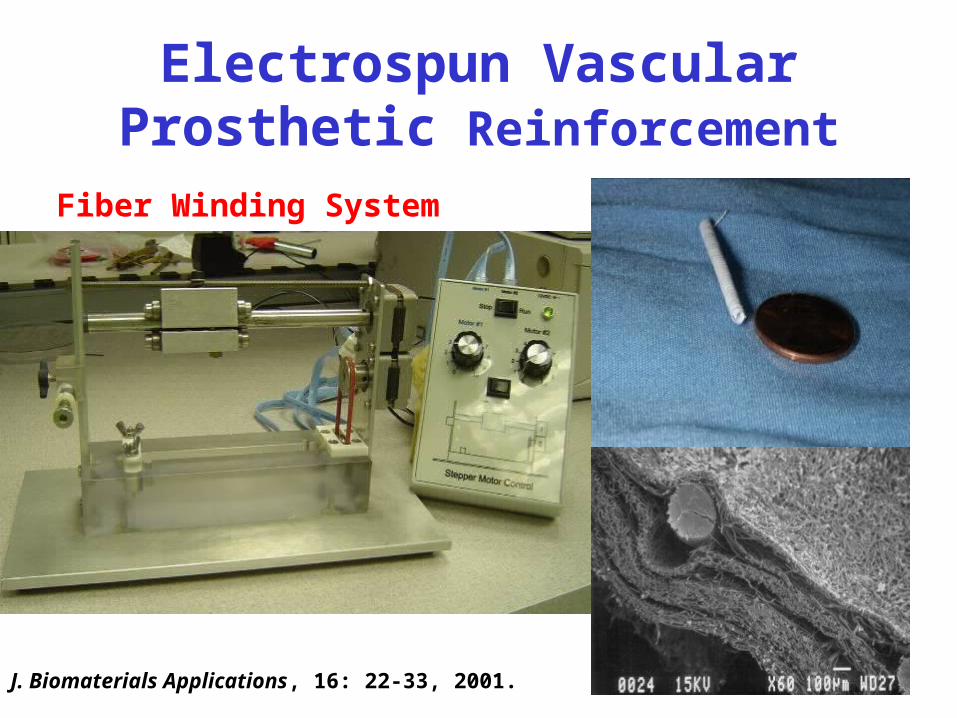
Electrospun Vascular Prosthetic Reinforcement
J. Biomaterials Applications, 16: 22-33, 2001.
Fiber Winding System
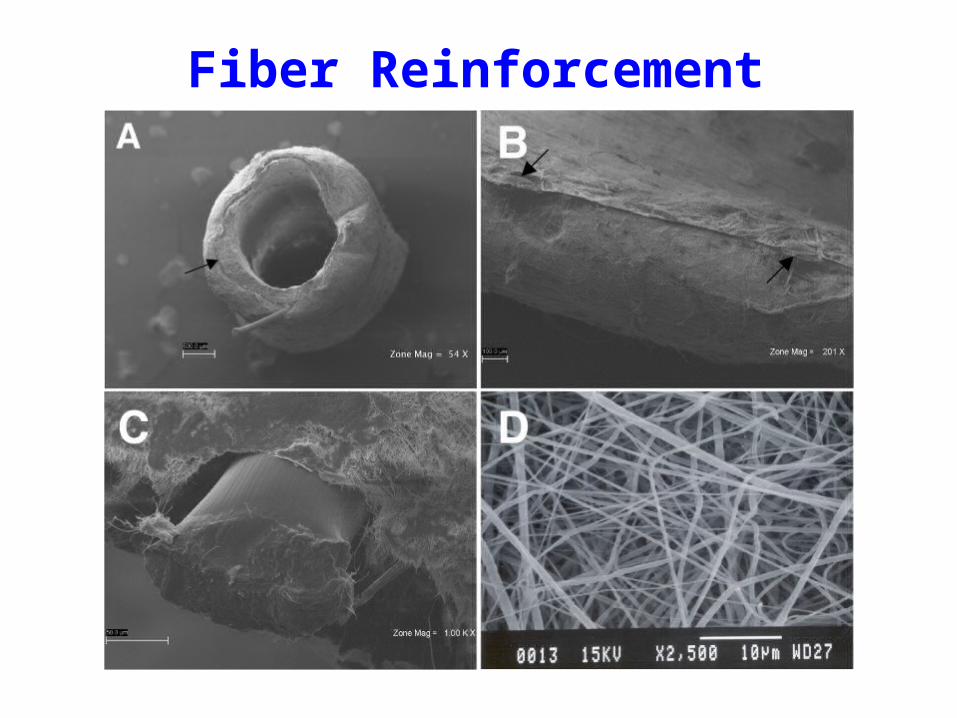
Fiber Reinforcement
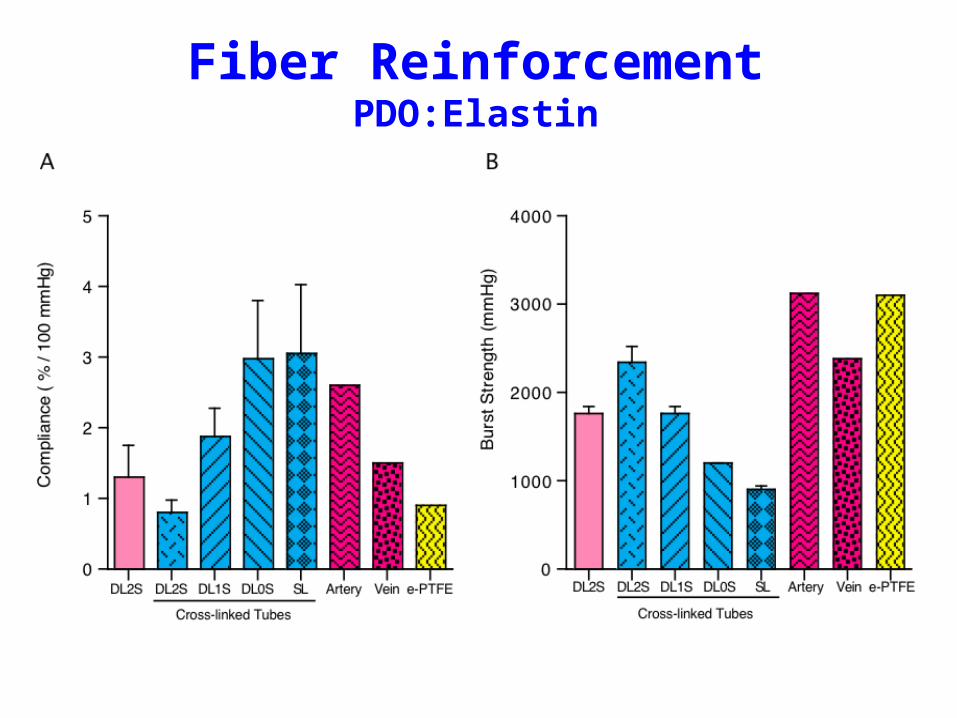
Fiber ReinforcementPDO:Elastin
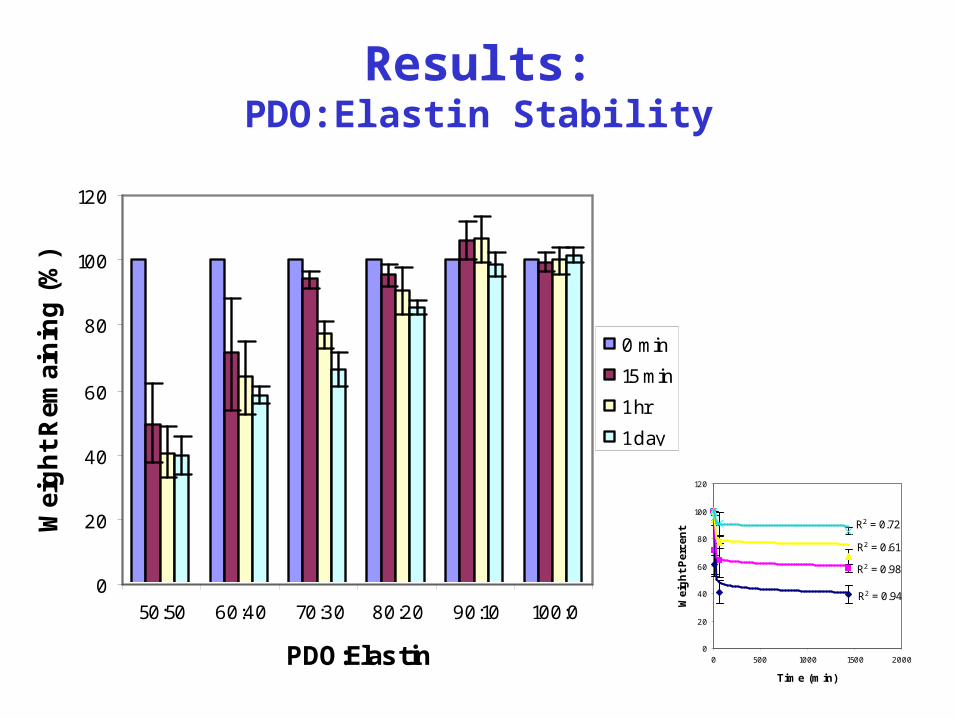
Results:PDO:Elastin Stability
0
20
40
60
80
100
120
50:50 60:40 70:30 80:20 90:10 100:0
PDO:Elastin
Wei
gh
t R
emai
nin
g (
%)
0 min
15 min
1 hr
1 day
R2 = 0.94
R2 = 0.98
R2 = 0.61
R2 = 0.72
0
20
40
60
80
100
120
0 500 1000 1500 2000
Time (min)W
eig
ht
Per
cen
t
50:50
60:40
70:30
80:20
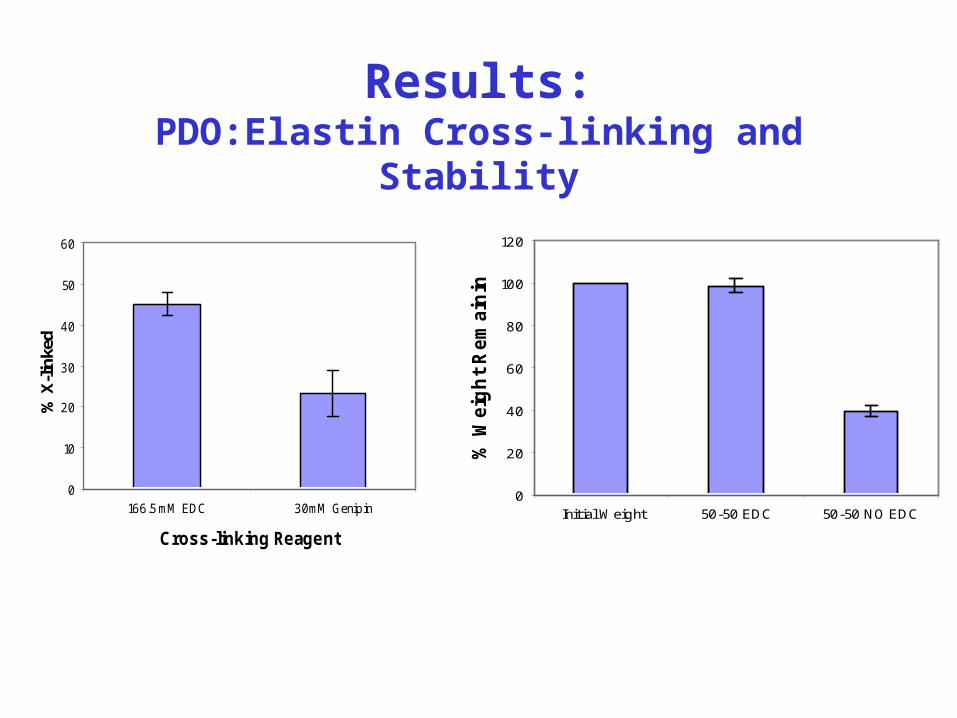
Results:PDO:Elastin Cross-linking and Stability
0
10
20
30
40
50
60
166.5 mM EDC 30mM Genipin
Cross-linking Reagent
% X
-lin
ked
0
20
40
60
80
100
120
Initial Weight 50-50 EDC 50-50 NO EDC
% W
eig
ht
Rem
ain
ing
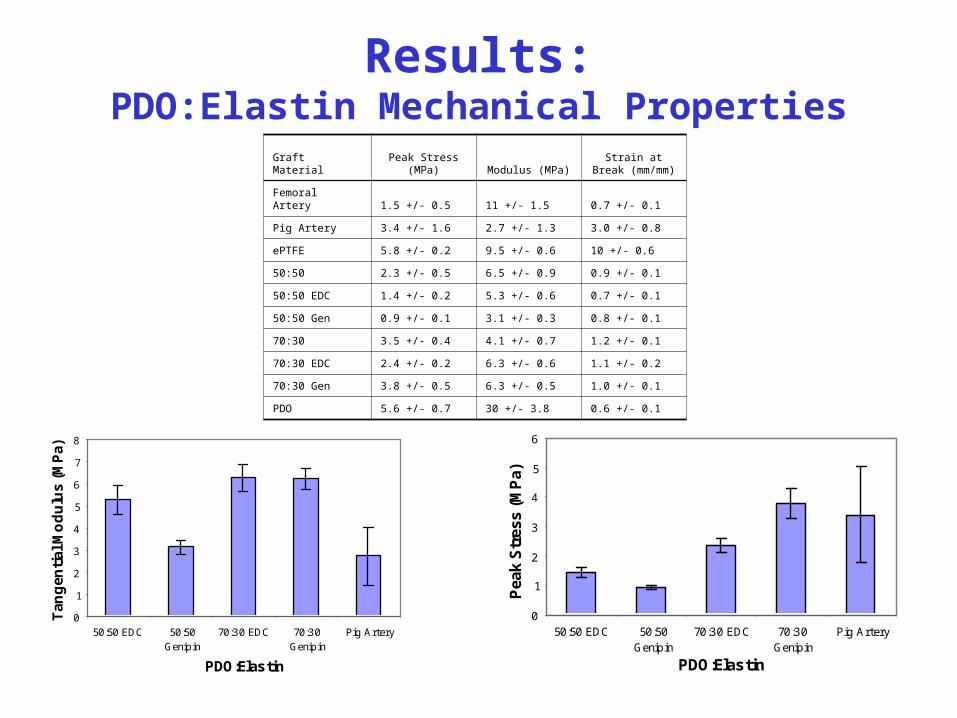
Graft Material Peak Stress (MPa) Modulus (MPa)Strain at Break
(mm/mm)
Femoral Artery 1.5 +/- 0.5 11 +/- 1.5 0.7 +/- 0.1
Pig Artery 3.4 +/- 1.6 2.7 +/- 1.3 3.0 +/- 0.8
ePTFE 5.8 +/- 0.2 9.5 +/- 0.6 10 +/- 0.6
50:50 2.3 +/- 0.5 6.5 +/- 0.9 0.9 +/- 0.1
50:50 EDC 1.4 +/- 0.2 5.3 +/- 0.6 0.7 +/- 0.1
50:50 Gen 0.9 +/- 0.1 3.1 +/- 0.3 0.8 +/- 0.1
70:30 3.5 +/- 0.4 4.1 +/- 0.7 1.2 +/- 0.1
70:30 EDC 2.4 +/- 0.2 6.3 +/- 0.6 1.1 +/- 0.2
70:30 Gen 3.8 +/- 0.5 6.3 +/- 0.5 1.0 +/- 0.1
PDO 5.6 +/- 0.7 30 +/- 3.8 0.6 +/- 0.1
0
1
2
3
4
5
6
7
8
50:50 EDC 50:50Genipin
70:30 EDC 70:30Genipin
Pig Artery
PDO:Elastin
Tan
gen
tial
Mo
du
lus
(MP
a)
0
1
2
3
4
5
6
50:50 EDC 50:50Genipin
70:30 EDC 70:30Genipin
Pig Artery
PDO:Elastin
Pea
k S
tres
s (M
Pa)
Results:PDO:Elastin Mechanical Properties
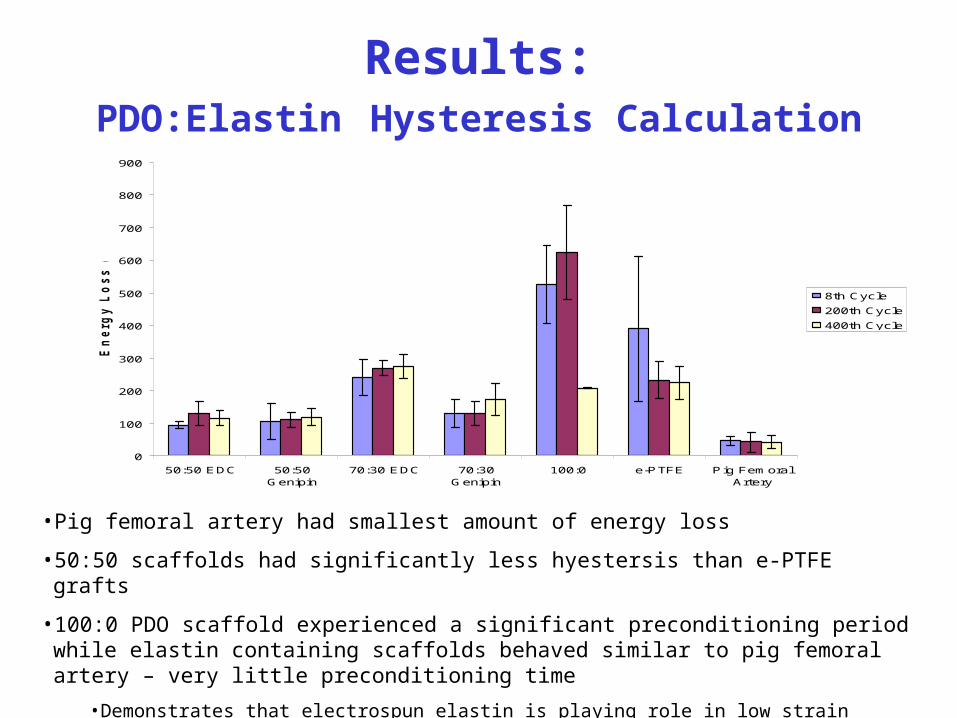
Results:PDO:Elastin Hysteresis Calculation
0
100
200
300
400
500
600
700
800
900
50:50 EDC 50:50Genipin
70:30 EDC 70:30Genipin
100:0 e-PTFE Pig FemoralArtery
En
erg
y L
os
s (
J/m
^3
)
8th Cycle
200th Cycle
400th Cycle
• Pig femoral artery had smallest amount of energy loss
• 50:50 scaffolds had significantly less hyestersis than e-PTFE grafts
• 100:0 PDO scaffold experienced a significant preconditioning period while elastin containing scaffolds behaved similar to pig femoral artery – very little preconditioning time
•Demonstrates that electrospun elastin is playing role in low strain response of scaffold
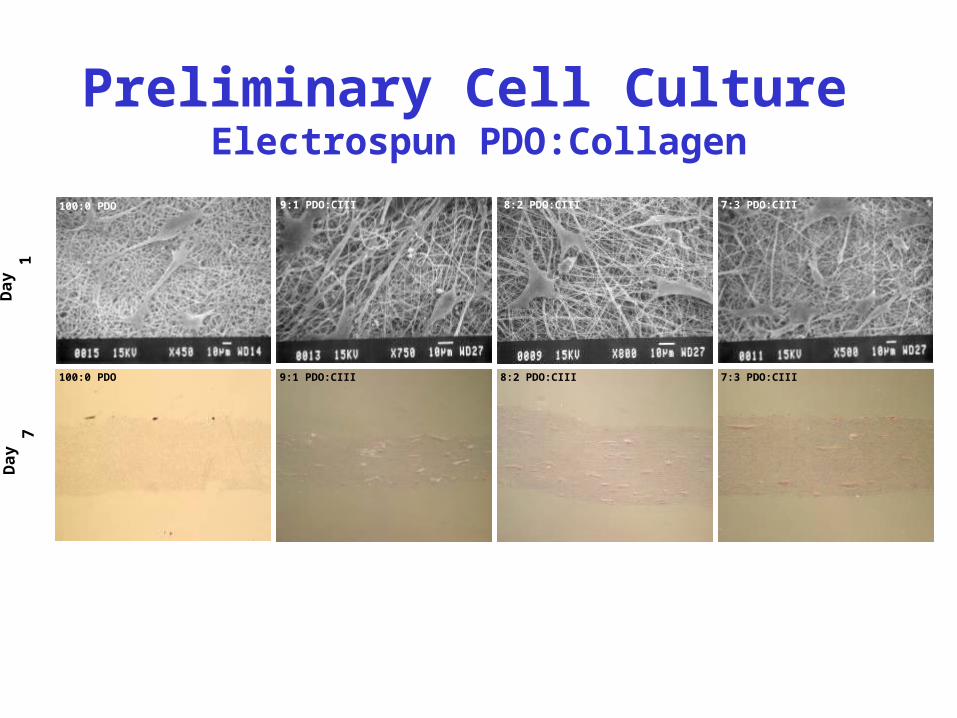
Preliminary Cell Culture Electrospun PDO:Collagen
9:1 PDO:CIII 8:2 PDO:CIII 7:3 PDO:CIII100:0 PDO
100:0 PDO 9:1 PDO:CIII 8:2 PDO:CIII 7:3 PDO:CIII
Day
7D
ay 1
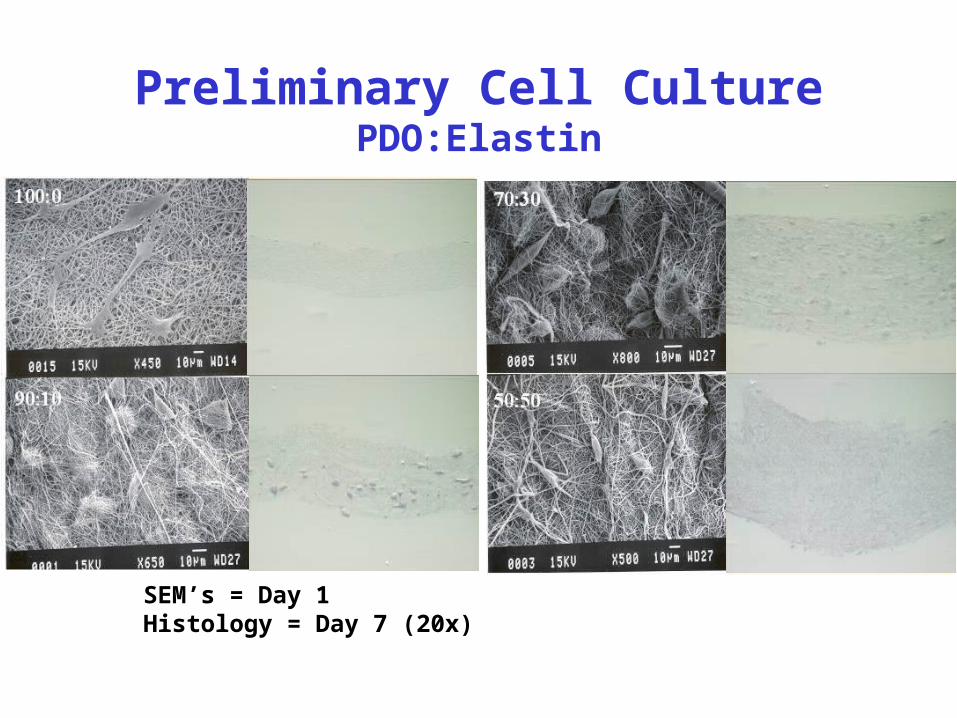
Preliminary Cell CulturePDO:Elastin
SEM’s = Day 1Histology = Day 7 (20x)
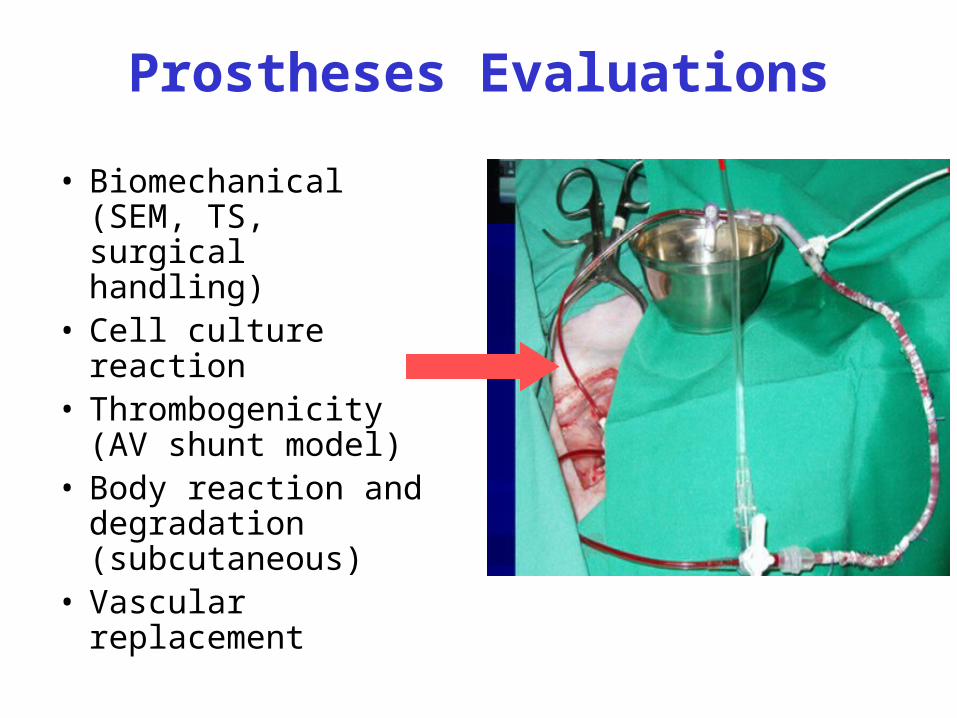
Prostheses Evaluations
• Biomechanical (SEM, TS, surgical handling)
• Cell culture reaction• Thrombogenicity (AV
shunt model)• Body reaction and
degradation (subcutaneous)
• Vascular replacement
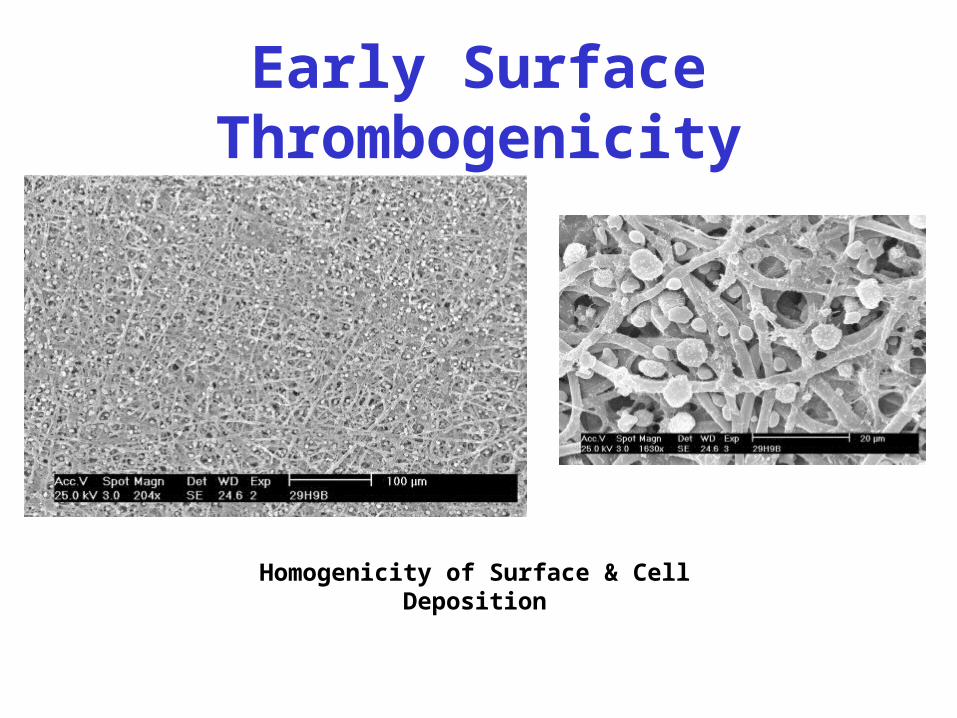
Early Surface Thrombogenicity
Homogenicity of Surface & Cell Deposition
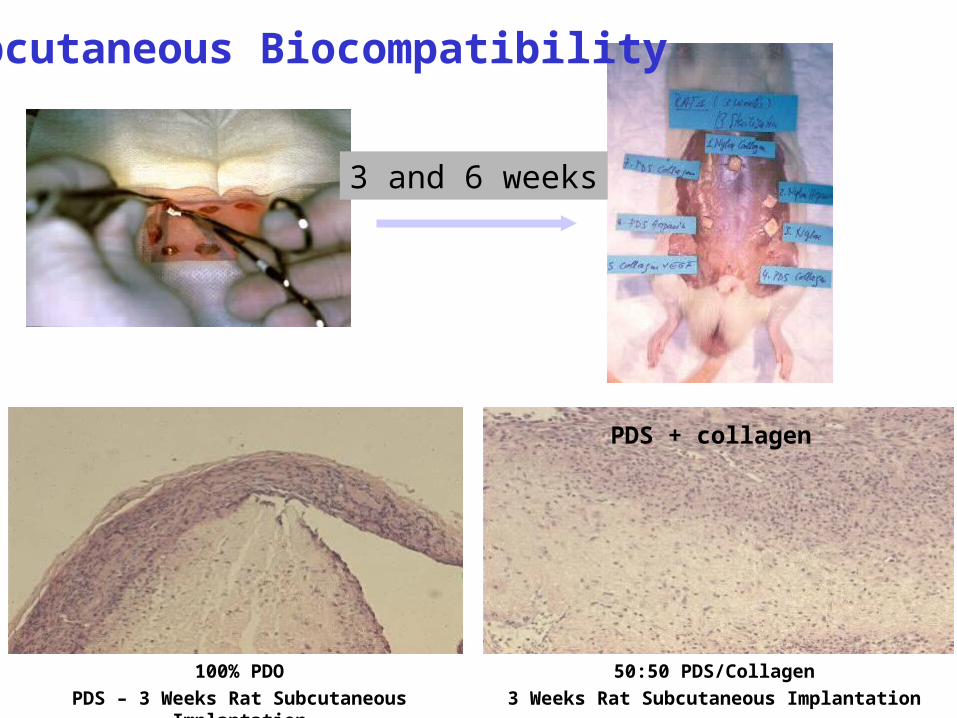
3 and 6 weeks
Subcutaneous Biocompatibility
100% PDO
PDS – 3 Weeks Rat Subcutaneous Implantation
PDS + collagen
50:50 PDS/Collagen
3 Weeks Rat Subcutaneous Implantation
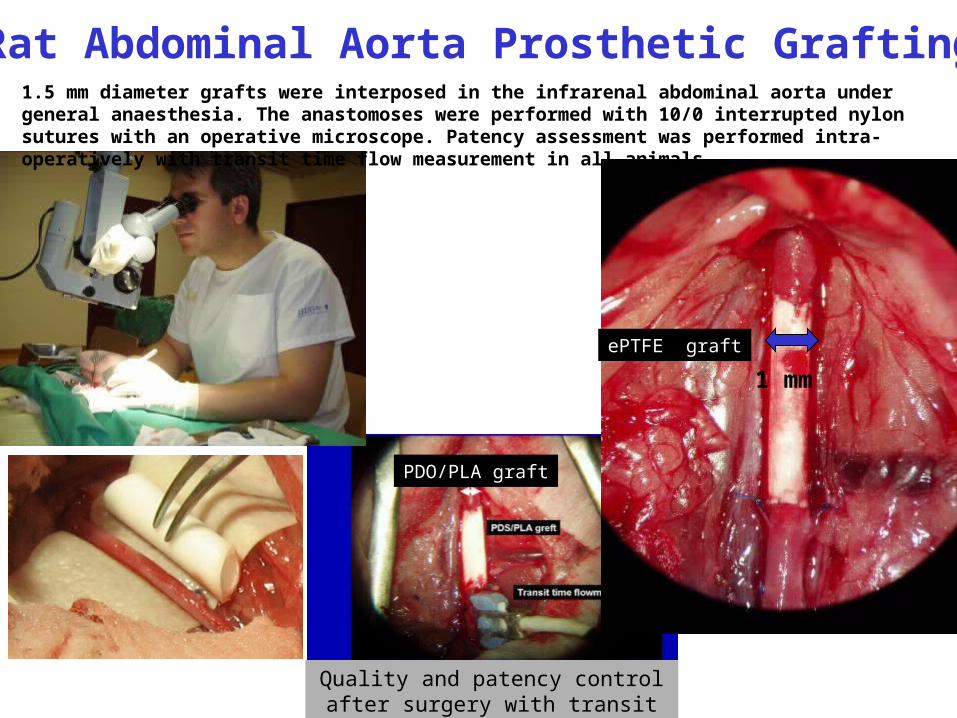
PDO/PLA graft
Quality and patency control after surgery with transit time
flowmeter
1 mm
ePTFE graft
1.5 mm diameter grafts were interposed in the infrarenal abdominal aorta under general anaesthesia. The anastomoses were performed with 10/0 interrupted nylon sutures with an operative microscope. Patency assessment was performed intra-operatively with transit time flow measurement in all animals.
Rat Abdominal Aorta Prosthetic Grafting
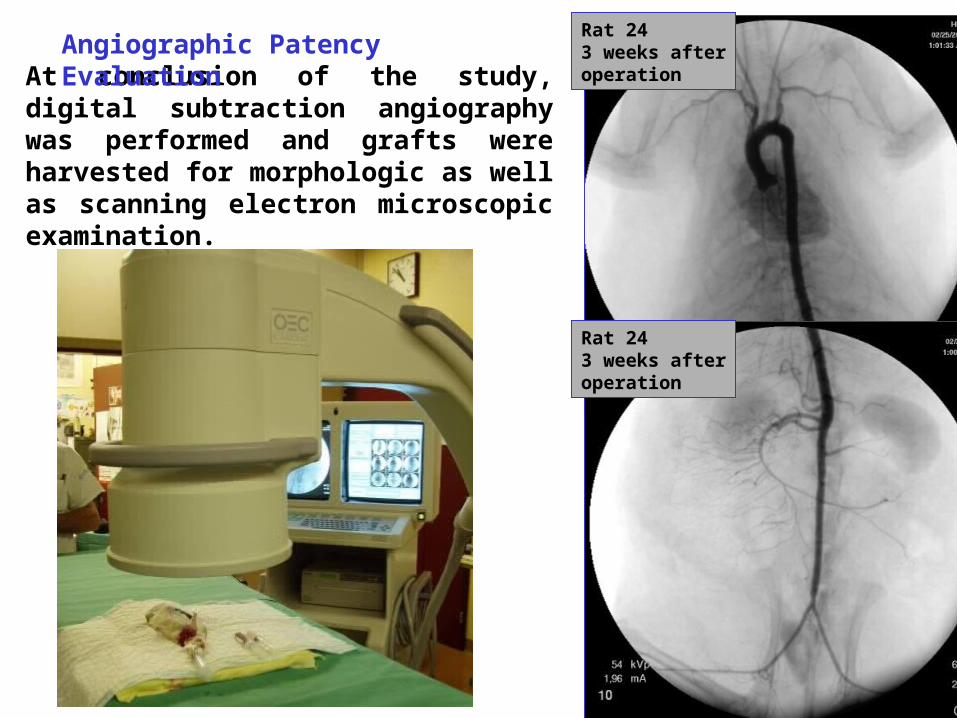
Rat 24 3 weeks afteroperation
Rat 24 3 weeks afteroperation
At conclusion of the study, digital subtraction angiography was performed and grafts were harvested for morphologic as well as scanning electron microscopic examination.
Angiographic Patency Evaluation
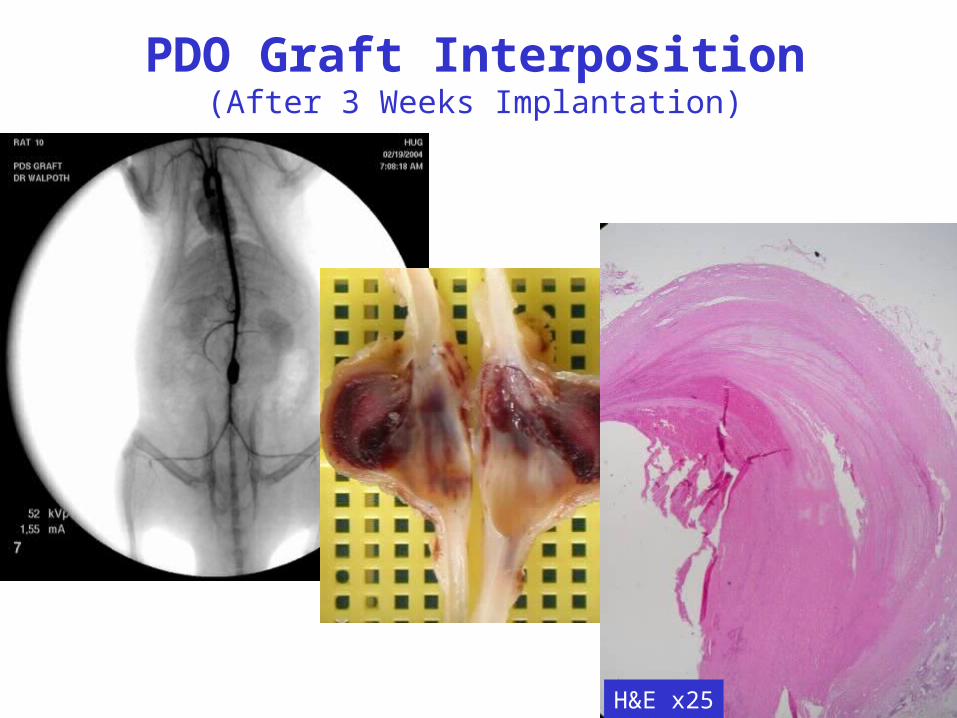
PDO Graft Interposition(After 3 Weeks Implantation)
ePTFE greft
H&E x25
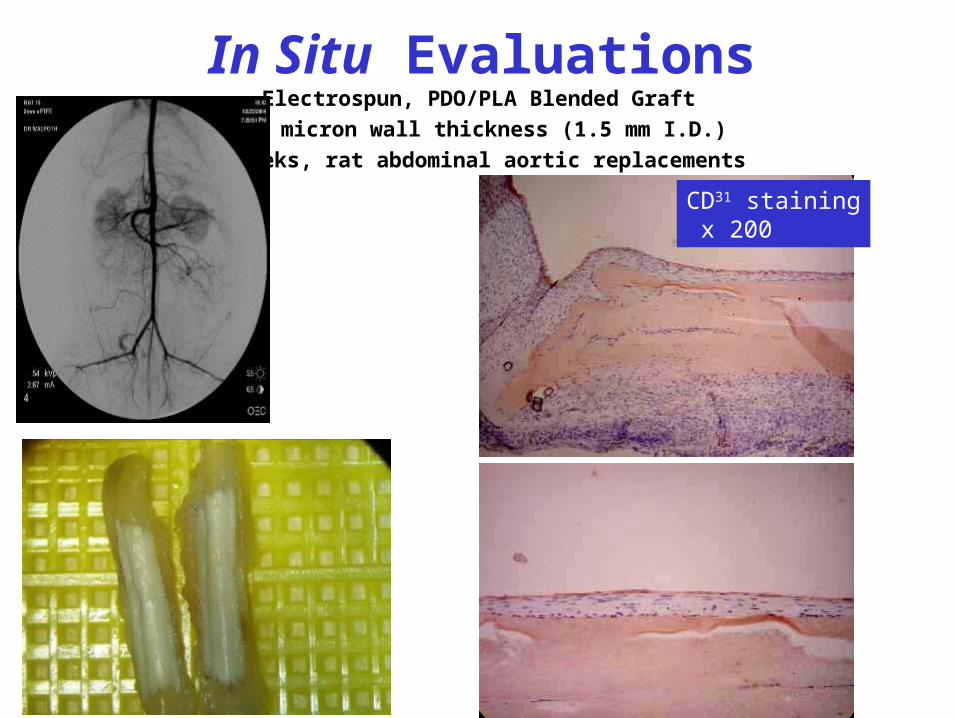
In Situ EvaluationsElectrospun, PDO/PLA Blended Graft
500 micron wall thickness (1.5 mm I.D.)
3 weeks, rat abdominal aortic replacements
CD31 staining x 200
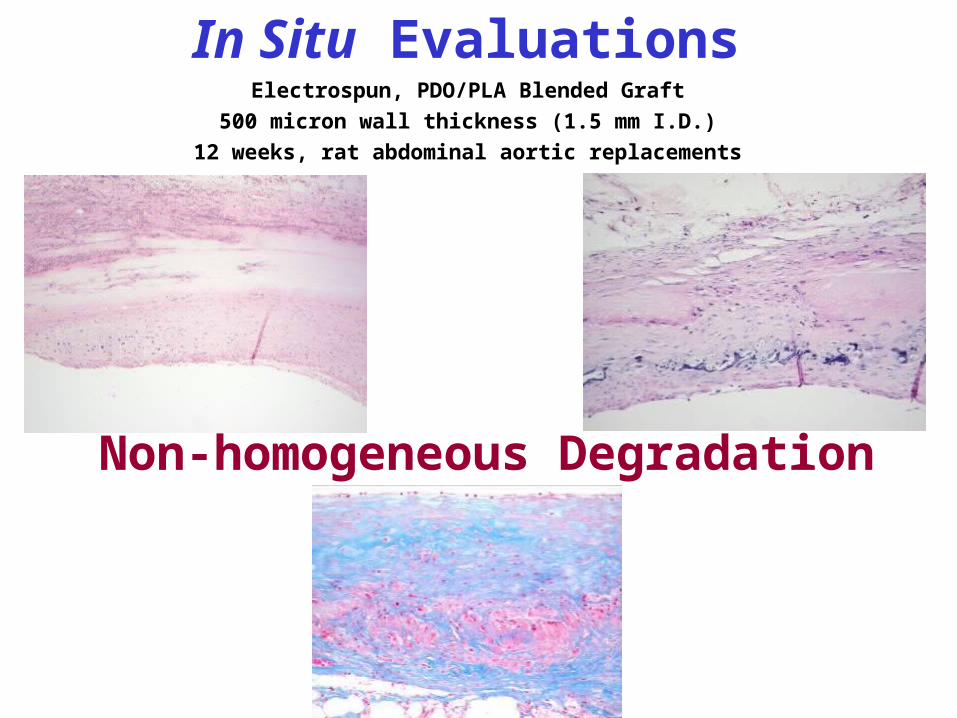
Non-homogeneous Degradation
In Situ EvaluationsElectrospun, PDO/PLA Blended Graft
500 micron wall thickness (1.5 mm I.D.)
12 weeks, rat abdominal aortic replacements
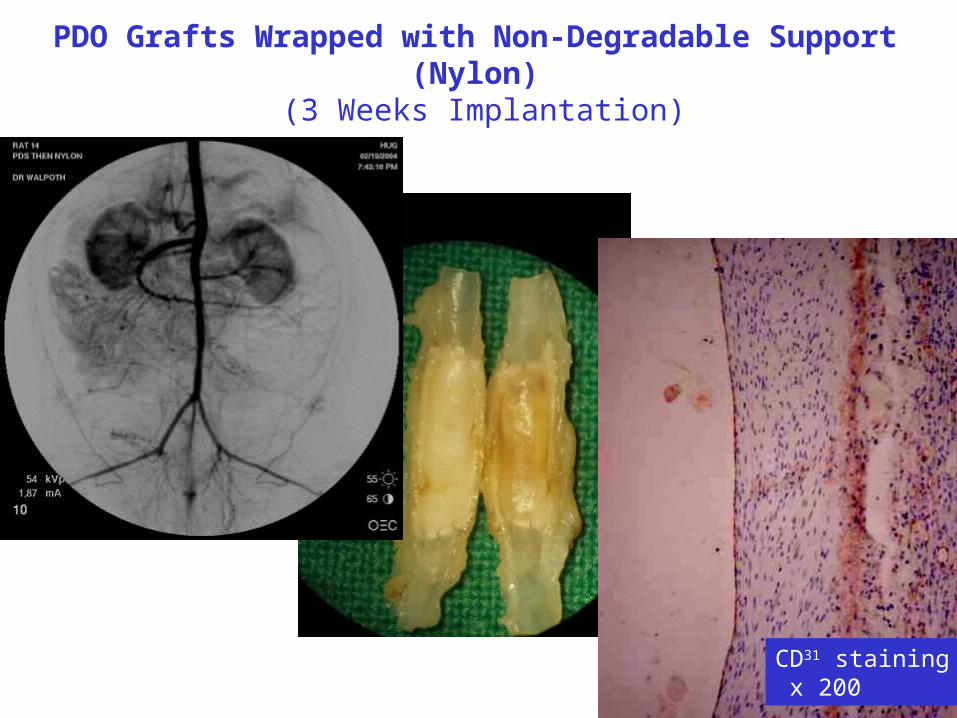
PDO Grafts Wrapped with Non-Degradable Support (Nylon) (3 Weeks Implantation)
CD31 staining x 200
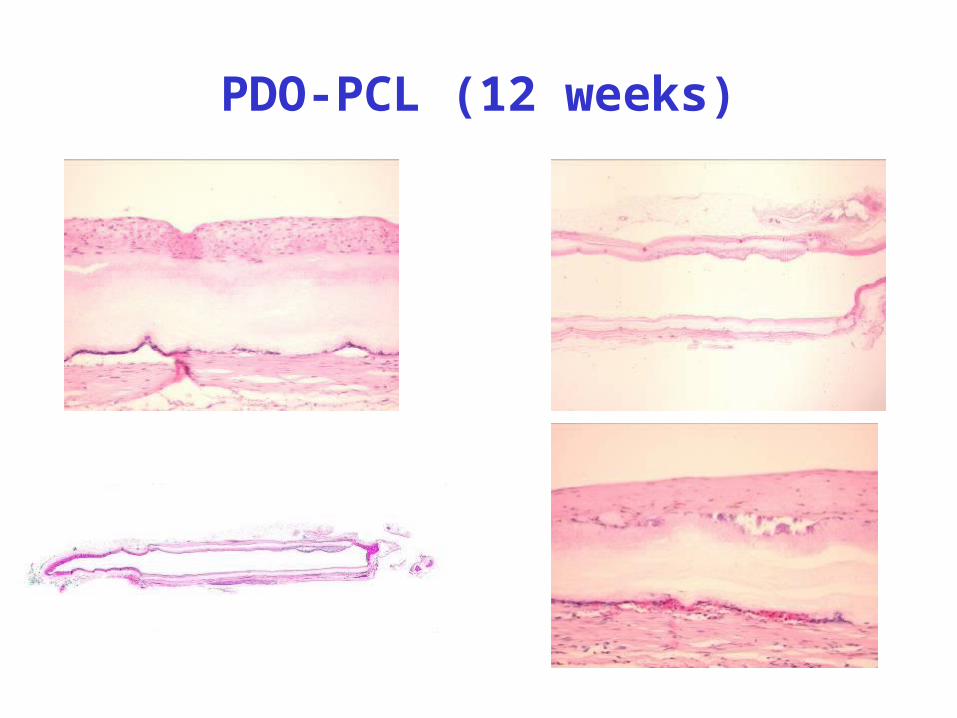
PDO-PCL (12 weeks)
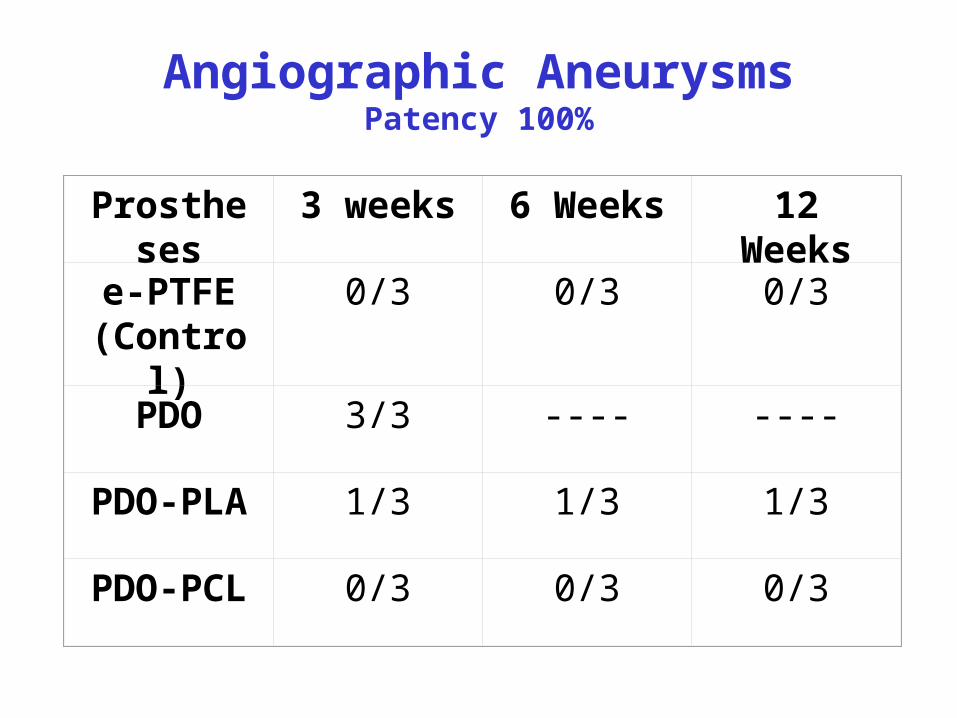
Angiographic AneurysmsPatency 100%
Prostheses 3 weeks 6 Weeks 12 Weeks
e-PTFE(Control)
0/3 0/3 0/3
PDO 3/3 ---- ----
PDO-PLA 1/3 1/3 1/3
PDO-PCL 0/3 0/3 0/3
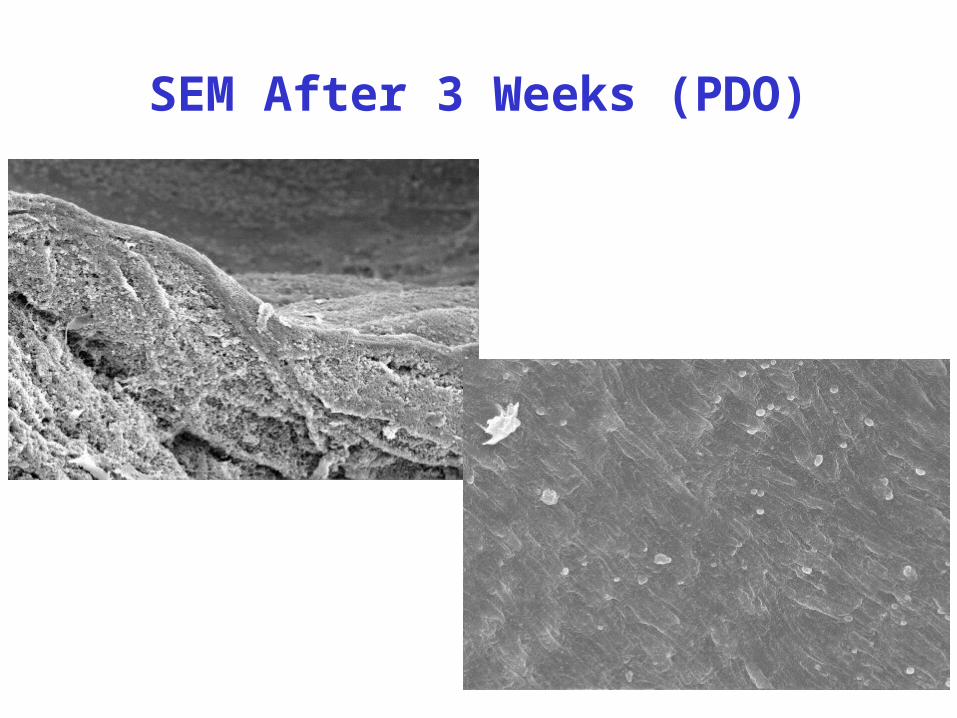
SEM After 3 Weeks (PDO)
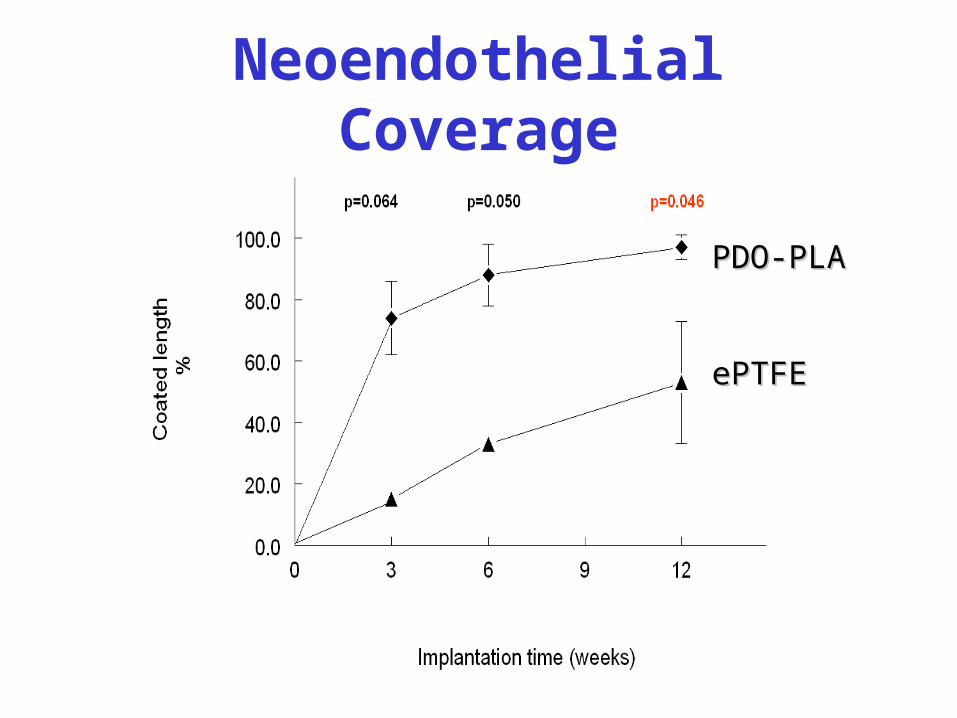
Neoendothelial Coverage
PDO-PLAPDO-PLA
ePTFEePTFE
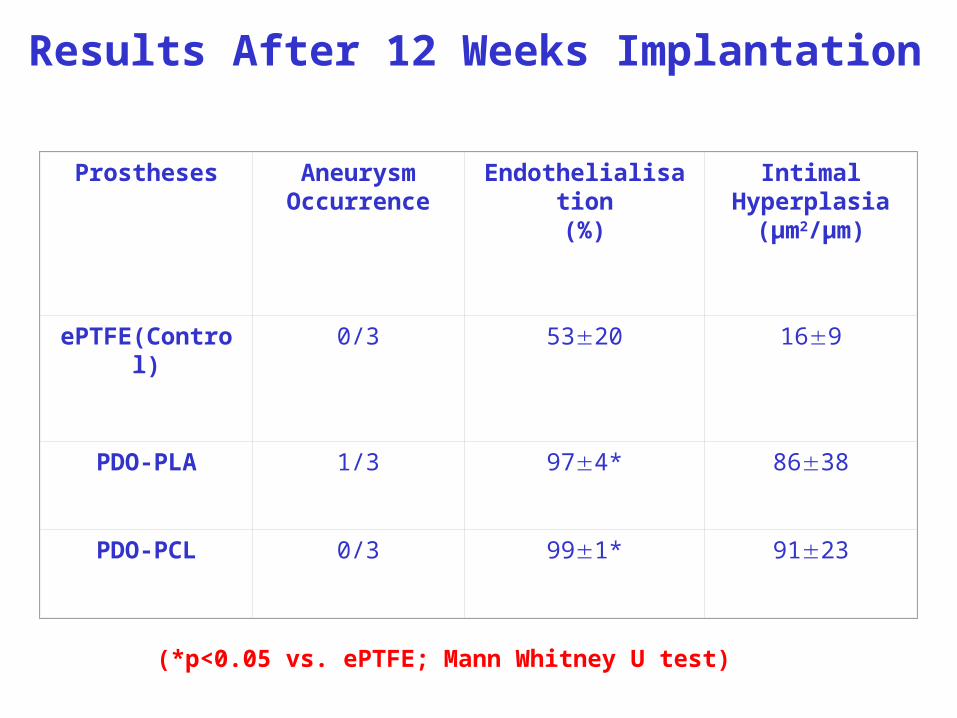
Results After 12 Weeks Implantation
Prostheses Aneurysm Occurrence
Endothelialisation(%)
Intimal Hyperplasia
(µm2/µm)
ePTFE(Control) 0/3 5320 169
PDO-PLA 1/3 974* 8638
PDO-PCL 0/3 991* 9123
(*p<0.05 vs. ePTFE; Mann Whitney U test)
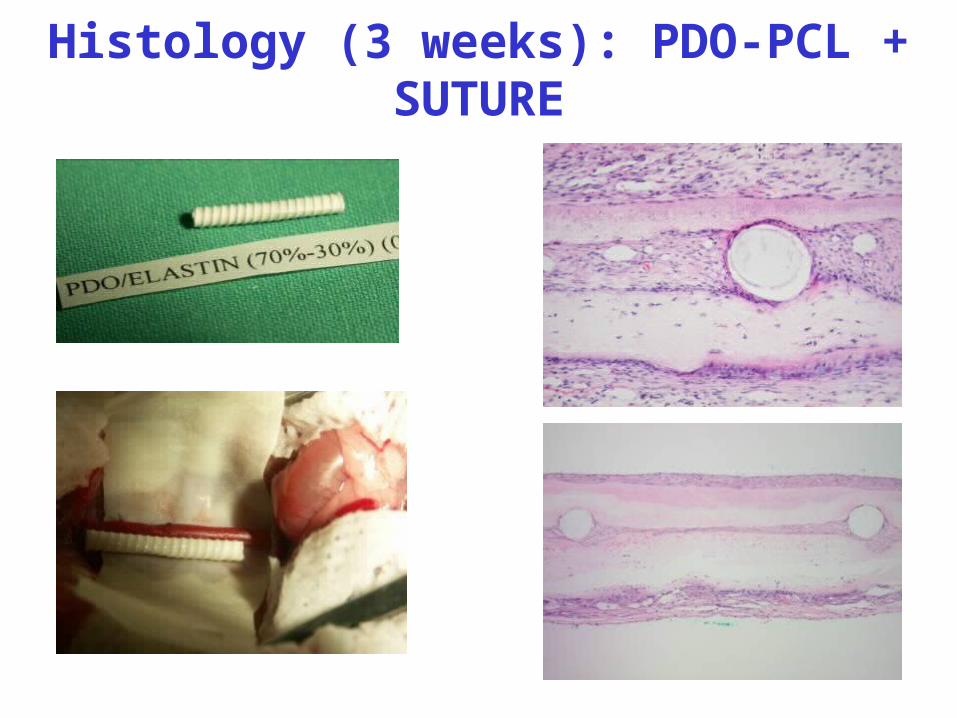
Histology (3 weeks): PDO-PCL + SUTURE
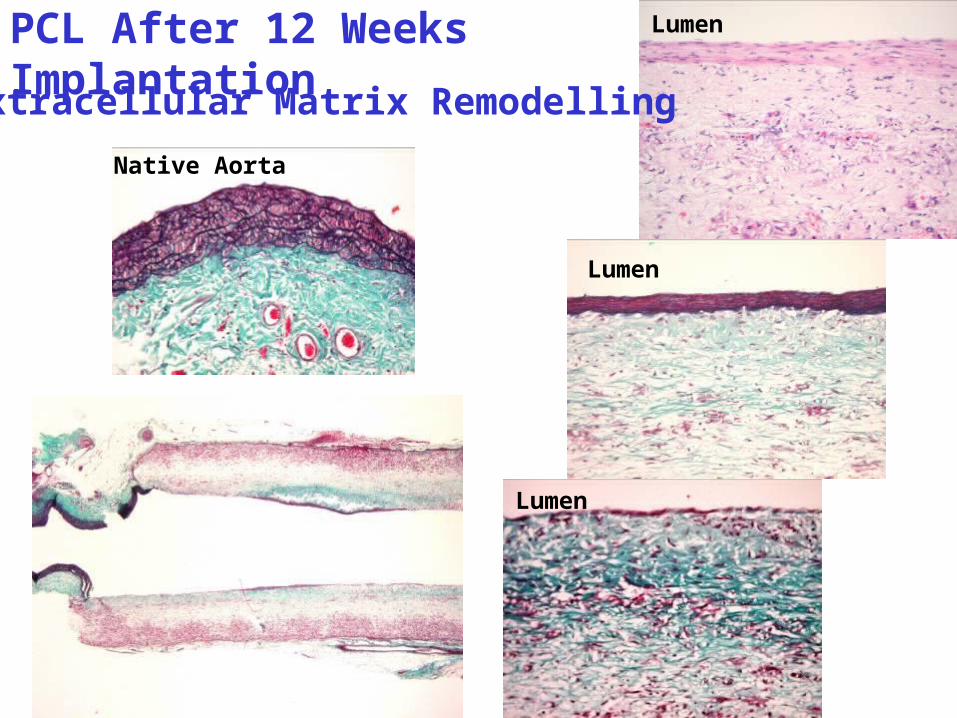
PCL After 12 Weeks Implantation
Native Aorta
Lumen
Lumen
Lumen
Extracellular Matrix Remodelling
Time/Physiologic IntegrationOnce we have created tissue engineered products, time and physiologic integration will be the components that will have the attention of the field.
Will immature cells, stem cells, mature and differentiate to maintain tissue?
How will the cells implanted react over time to the new environment?
Will they maintain function indefinitely?
If used in infants or children, will they grow along with the host?
Will structural integrity be maintained or developed?
Is the scaffold degradation rate appropriate?
AcknowledgementsCollaborators:Marcus E. Carr, M.D./Ph.D.David G. Simpson, Ph.D.Gary E. Wnek, Ph.D. (Case Western)Mike McManus, M.D.Beat Walpoth, M.D. (Geneva)Kevin Ward, M.D.Steve Montante, M.DDavid Brand, Ph.D.Matthew Beckman, Ph.D.Thomas Hass, Ph.D.Hu Yang, Ph.D.
Graduate Students:Jamil Matthews, M.D. Eugene D. Boland, Ph.D.
Catherine P. Barnes, M.S. Kristin J. Pawlowski, Ph.D.Scott Sell, M.S. Danielle C. Knapp, M.S.Joel D. Stitzel, Ph.D. Matthew J. Smith, M.S.Charles D. Anderson, M.S. Michael McClure, B.S.
Allison Faucette, M.S. Jared Nimtz, B.S.
Branch Coleman, M.S. Lisa I. Ramdhanie, M.S.
Undergraduate Students:Tara George, B.S. Michelle Park, B.S.
John Layman, B.S. Katherine Neser, B.S.
LaVone Smith, B.S. Jon-Erik Houser, B.S
Colleen McLoughlin, B.S. Josh Grant, B.S.
Lindsay Denault
Funding:The Whitaker FoundationU.S. Department of Defense/ArmyNASA –LangleyAlkermes, Inc.NIH R01 EB003087-01 (DGS)NIH R21 EB003407-01-A1 (GLB)American Heart AssociationNanoMatrix, Inc.Ethicon, Inc.Jeffress Memorial TrustNational Science Foundation
High School Students:Annie Wysock Lindsay Denault
Dan Newton Jennifer Mejia
Teresa Tang
Residents:Michael McManus, M.D. Tommy Miller, M.D.
Paul Espy, M.D. Charles Fields, M.D.
List of Pertinent PublicationsWalpoth, B.H. and G.L. Bowlin. “The Daunting Quest for a Small Diameter Vascular Graft.” Expert Review of Medical Devices, 2
(6), 647-51, 2005.
Sell, S.A. and G.L. Bowlin. “The Potential to Create Small Diameter Bioresorbable Vascular Grafts Through Electrospinning.” Journal of Materials Chemistry, In Press.
Smith, M.J.; McClure, M.J.; Sell, S.A.; Barnes, C.P.; Walpoth, B.H.; Simpson, D.G. and G.L. Bowlin. “A Novel Suture-Reinforced Electrospun Polydioxanone-Elastin Small-Diameter Tube for Use in Vascular Tissue Engineering.” Acta Biomaterialia, In Press.
Smith, M.J.; Smith D.C.; White Jr., K.L. and G.L. Bowlin. “Immune Response Testing of Electrospun Polymers: An Important Consideration in the Evaluation of Biomaterials.” J. Engineered Fabrics and Fibers (Invited Editorial), 2(2), 41-47, 2007.
Barnes, C.P.; Pemble, C.W.; Brand, D.D.; Simpson, D.G. and G.L. Bowlin. “Cross-linking Electrospun Type II Collagen Tissue Engineering Scaffolds with Carbodiimide in Ethanol.” Tissue Engineering, 13(7), 1593-1605, 2007.
Barnes, C.P.; Sell, S.A.; Knapp, D.C.; Walpoth, B.H.; Brand, D.D. and G.L. Bowlin. “Preliminary Investigation of Electrospun Collagen and Polydioxanone for Vascular Tissue Engineering Applications.” International Journal of Electrospun Nanofibers and Applications, 1(1), 73-87, 2007.
Sell, S.A.; McClure, M.J.; Barnes, C.P.; Knapp, D.C.; Simpson, D.G.; Walpoth, B.H. and G.L. Bowlin. “Electrospun Polydioxanone – Elastin Blends: Potential for Bioresorbable Vascular Grafts.” Biomedical Materials, 1, 72-80, 2006.
Boland, E.D., Coleman, B.D.; Barnes, C.P.; Simpson, D.G., Wnek, G.E. and G.L. Bowlin. "Electrospinning Polydioxanone for Biomedical Applications.” Acta Biomaterialia, 1 (1), 115-123, 2005.
Boland, E.D., Matthews, J.A.; Pawlowski, K.J., Simpson, D.G., Wnek, G.E. and G.L. Bowlin. "Electrospinning Collagens and Elastin for Vascular Tissue Engineering.” Frontiers in Biosciences, 9, 1422-1432, May 1, 2004.
Matthews, J.A.; Simpson, D.G.; Wnek, G.E.; and G.L. Bowlin. "Electrospinning of Collagen Nanofibers." Biomacromolecules, 3 (2): 232-238, 2002.