Embed Size (px)
Citation preview
Journal of Nursing Scholarship Fourth Quarter 2001 369
Clinical Scholarship
W ith new gene discoveries emerging from theHuman Genome Project and other geneticsresearch, genetics components of health and
disease are becoming integrated into health care at all levels(Collins, 1999). Genetics nursing is a relatively new aspectof professional nursing practice in some countries, such asIsrael, Japan, South Africa, and Korea (Feetham, 2001).However, in Canada, the United Kingdom (UK), and theUnited States (US), genetics nursing has evolved over the past20 years as a component of genetic counseling. In theselocations, genetics nurse specialists function as members ofinterdisciplinary teams. As knowledge of genetic aspects ofcommon diseases is generated, genetics nursing is likely toexpand beyond the specialty clinic service location and willbecome part of nursing functions in many primary andspecialty care settings. These developments require that nursesseek answers to questions about outcomes of geneticcounseling services based on client health and health careservices (Feetham, 1997).
Genetic Counseling Outcomes Validationby Genetics Nurses in the UK and USJanet K. Williams, Heather Skirton, David Reed, Marion Johnson,Meridean Maas, Sandra Daack-Hirsch
Purpose: To validate genetic counseling outcomes with a sample of genetics nurses from theUnited Kingdom (UK), and to compare elements of genetic counseling outcomes with thosefrom a sample of genetics nurses from the United States (US).
Design: Descriptive-comparative survey.Methods: Concept analysis and literature review were used to designate outcomes, and genetics
nurses were surveyed to validate the outcomes. A revision of Fehring’s 1987 methodologyfor assessing content validity was used to estimate content validity and sensitivity of thegenetic counseling outcomes. Data are reported on a convenience sample of 50 UK nursemembers of the Association of Genetic Nurses and Counsellors. Findings were correlatedwith prior data from a convenience sample of 92 U.S. nurse members of the InternationalSociety of Nurses in Genetics, Inc., and data were compared between groups.
Findings: A significant positive correlation was found between samples of U.K. and U.S.nurses regarding components of outcomes of the genetic counseling process and betweengroups regarding extent of contribution of nurses to the outcomes. Strength of nursingcontributions to knowledge of disease and indicators of coping varied according to country.
Conclusions: Genetics nurses in the UK and US had similar definitions of outcomes of geneticcounseling, but priorities of indicators differed between countries. Terminology used inmeasures to identify outcomes of the process of genetic counseling must be consistent withcultural norms.
JOURNAL OF NURSING SCHOLARSHIP, 2001; 33:4, 369-374. ©2001 SIGMA THETA TAU INTERNATIONAL.
[Key words: nursing outcomes, genetic counseling, international nursing]
* * *
Background
The American Society of Human Genetics defines geneticcounseling as a communication process to deal with thehuman problems associated with the occurrence or risk of
Janet K. Williams, RN, PhD, CPNP, CGC, FAAN, Gamma, Associate Professor,College of Nursing, University of Iowa, Iowa City, IA; Heather Skirton, RGN,RM, MSc, PhD, Gamma, Nurse Consultant in Clinical Genetics and Lecturer,University of Wales College of Medicine, Cardiff, UK; David Reed, PhD, AssistantResearch Scientist, Marion Johnson, RN, PhD, Gamma, Professor, MerideanMaas, RN, PhD, FAAN, Gamma, Sally Mathis Hartwig Professor of GerontologicNursing, Director of Hartford Center of Geriatric Nursing Excellence, Director ofDoctoral Students, Sandra Daack-Hirsch, RN, MSN, Gamma, Program Associate,all at College of Nursing, University of Iowa, Iowa City, IA. The authorsacknowledge Lori Penaluna for her technical assistance. This research was madepossible by funding from Sigma Theta Tau International, 1992-1993 and theNational Institute for Nursing Research (Grant RO1NR03437), 1993-1996 and1998-2002. Correspondence to Dr. Williams, 338 Nursing Building, The Universityof Iowa, Iowa City, IA 52242. E-mail: [email protected]
Accepted for publication July 30, 2001.

370 Fourth Quarter 2001 Journal of Nursing Scholarship
U.S. & U.K. Outcomes
occurrence of a genetic disorder in a family. This process isaimed at helping the person or family to (a) comprehend themedical facts, including the diagnosis, probable course ofthe disorder, and the available management, (b) understandhow heredity contributes to the disorder and the risk ofrecurrence in specified relatives, (c) understand thealternatives for dealing with the risk of recurrence, (d) choosea course of action which seems to be appropriate in view oftheir risk, family goals, and ethical and religious standards,and (e) make the best possible adjustment to the disorder orrisk of recurrence of the disorder (Ad Hoc Committee onGenetic Counseling of the American Society of HumanGenetics, 1975). This definition reflects a nondirectiveapproach to counseling that promotes informed andautonomous decision making, especially when reproductivedecisions are under consideration. However, the desire forguidance and advice by some consumers of genetics healthservices has led to discussions of circumstances in which amore directive approach may be indicated (Bernhardt, 1997;Elwyn, Gray, & Clark, 2000). When health teaching isprovided, or genetic information is used to make clinicaldecisions about further diagnosis or treatment decisions, amore directive approach may be used. Examples are teachingregarding recommendations for folic acid intake for womenof reproductive age, or cancer surveillance guidelines forpeople who have particular mutations in a gene thatpredisposes them to familial cancer.
In the US, nurses were part of genetics health care teamsfrom the beginning of specialty genetics practice and incommunity health; in the 1960s and 1970s, genetics wasrecognized as a component of case finding and follow-upmanagement by community health nurses (Forbes, 1966;Hillsman, 1966) and disease management teams (Ferrer,1975; Sahin, 1976). Fibison (1983) described a geneticsclinical nurse specialist role. In 1998, the American NursesAssociation (ANA) approved the definition of the Scope andStandards for Genetics Nursing Practice that was developedby the International Society of Nurses in Genetics (ISONG).ISONG represents nurses whose professional practice isfocused on clients with, or at risk to develop a geneticcondition. Members include nurses from eight countries, butthe majority of members are U.S. nurses.
A similar initiative is currently underway in the UK. TheAssociation of Genetic Nurses and Counsellors (AGNC) hasrecently completed the task of defining the core competenciesfor the practice of genetic counselling in the UK (AGNCEducation Working Group, 2001). Farnish (1988)documented the role of genetics nurses in the UK in the mid1980s. In 1995, the AGNC Working Party was formed toundertake research on the role of genetics nurses (Skirton,Barnes, Curtis, & Walford-Moore, 1997), documenting theviews of genetics nurses and their medical geneticistcolleagues. Findings were used as a basis for a set of guidelinesfor education and training of genetics nurses (Skirton et al.,1998). In 2001, a formal registration process for geneticsnurses and genetic counsellors practicing in the UK will beintroduced, enabling self-regulation of practitioners by the
profession. In the UK, nurses and counsellors work togetheron clinical genetics teams and the registration criteria andprocess are identical for both groups. The term geneticcounsellor has been adopted as the professional name forpractitioners from both nursing and non-nursingbackgrounds.
Much attention is currently directed toward identificationof appropriate educational preparation for nurses who willuse genetics principles in their professional practice. In theUS, one strategy is the participation of several professionalnursing organizations in the National Coalition for HealthProfessional Education in Genetics (NCHPEG). Founded in1996 by the ANA, the American Medical Association, andthe National Human Genome Research Institute, thisorganization was created for the purpose of interdisciplinarycollaboration to develop core competencies in genetics healthcare for health professionals and to disseminate geneticseducational materials that can be shared by all health caredisciplines (Anderson, Monsen, Prows, Tinley, & Jenkins,2000). In 2000, this organization issued a list of corecompetencies in genetics that are recommended for all healthcare professionals (www.nchpeg.org). Other examples arethe revised Essentials of Baccalaureate Education forProfessional Nursing Practice (American Association ofColleges of Nursing, 1998), and core competencies foroncology nurses who integrate genetics concepts into theirnursing practice (Jenkins, Masny, & Tranin, in press). Asimilar initiative is occurring in Japan where nurse leadersare investigating the roles of professional nurses in emerginggenetics health care practice (Ando, 2000).
In the UK, Kirk and colleagues (1999) identified the needsof preregistration nursing students in the field of genetics,and the Royal College of Nursing set up a Genetics WorkingGroup to improve access of nurses and midwives to essentialgenetics knowledge. Other initiatives have been undertakenin Europe to create a core curriculum in genetics fornonmedical health care workers, including nurses. Such workshould not be focused in one country, but it should reflectthe globalization of nursing practice, especially with regardto newly developing health services (Henry, 1998).
In studies of genetic counseling, outcomes have traditionallybeen defined as changes in client knowledge (Abramovsky,Godmilow, Hirschhorn, & Smith, 1980; Carter, Fraser Roberts,Evans, & Buck, 1971), changes in reproductive intention orbehavior (D’Amico, Jacopini, Vivona, & Frontali, 1992; Wertz& Sorenson, 1986), or client satisfaction (Hallowell, Murton,Statham, Green, & Richards, 1997; Shiloh, Avdor, & Gooman,1990). These studies were focused on measuring outcomesdefined by practitioners, and clients’ perspectives on outcomesof genetic counseling have not been well-established. Recentwork by Skirton (2001) confirmed that psychologicaladaptation to the genetic condition or risk is an importantoutcome to clients, but the relationship between client andcounselor is also integral to the process.
Since the mid 1960s the importance of determiningoutcomes of nursing practice has been recognized. A majoreffort, the Nursing Outcomes Classification (NOC) research

Journal of Nursing Scholarship Fourth Quarter 2001 371
U.S. & U.K. Outcomes
(Iowa Outcomes Project, 2000), is focused on the creationof a common language for the nursing profession regardingpatient outcomes. These outcomes at the level of theindividual, family, and community can be used to evaluatenursing care across the patient care continuum. SimilarlyDaack-Hirsch and colleagues (2001) identified outcomes thatwere related to genetics nursing practice. Although nursesintegrate genetics concepts into their practice in manycountries, genetics nursing organizations have beenestablished in the US and UK, thus enabling identification ofexpert nurses in genetics nursing practice. The purpose ofthis study was to validate genetic counseling outcomes witha sample of U.K. genetics nurses, and to compare theirresponses to those of a sample of U.S. genetics nurses.
Methods
To validate the outcomes and indicators that are importantto the process of genetic counseling, and to determine thecontributions of genetics nurses to the achievement of theseoutcomes, a mailed survey was sent to all U.K. or U.S. nursemembers of AGNC and ISONG.
SampleU.S. residents who were members of ISONG (n=216), and
U.K. residents who were members of the AGNC (n=135)received the survey. The names were obtained frommembership records from ISONG for 1998, and AGNC for1999. The final sample was 99 U.S. nurses and 50 U.K. nurses.
InstrumentsThe questionnaire included three outcomes and indicators
derived by a review of the genetic counseling literature, andfrom review of the NOC outcomes including Knowledge:Disease Process, Decision-Making, and Coping (IowaOutcomes Project, 2000). A fourth outcome, Satisfaction withGenetic Counseling, was developed by Daack-Hirsch throughliterature review and concept analysis (Daack-Hirsch et al.,2001). Each outcome has from 8 to 14 indicators. Nurse expertswere asked to rate on a 1-5 scale (1= not at all important to 5=very important) the importance of each indicator for measuringthat outcome. Respondents were also asked to rate the nursingsensitivity, or strength of nursing contribution, to theachievement of the indicator on a 1-5 scale (1= no contributionto 5= contribution is mainly nursing).
ProcedureFollowing approval by the institutional review board, a
list of ISONG members was obtained from the ISONGmembership committee. ISONG members were sent themailed questionnaire with a return envelope. A follow-uppostcard was sent 3 weeks after the initial mailing. A secondmailing was sent to nonrespondents approximately 5 monthsafter mailing the reminder postcard. In 1999 a list of registerednurse members of AGNC was obtained from the AGNCcommittee. The same mailing procedure was used.
Data Management and AnalysisFor data management and analysis the same procedures
were followed as were used by the NOC research team. SPSSfor Windows software was used to manage and analyze thedata. Analysis followed an adaptation of Fehring’smethodology (Fehring, 1987) used by the NOC research team(Johnson & Maas, 1997), consisting of establishing weightedratios for each rating of importance and sensitivity. The ratioswere obtained by adding the weights assigned to eachresponse and dividing the sum by the total number ofresponses, yielding weights of 5=1, 4=.75, 3=.50, 2=.25, and1=0. For each outcome respondents were asked to make tworatings. The first was to identify the importance of theindicators for that outcome, and the second was to rate thesensitivity of each indicator to nursing intervention. Finally,summing and averaging the ratings across all respondentsformed the outcome content validity and outcome sensitivityscores. Those indicator and sensitivity ratings equal to orgreater than .80 were rated as critical, and items ratedbetween .79-.60 were regarded as supporting factors fornursing contribution to the outcome. Those with ratings ofless than .60 were regarded as needing further study orpossible deletion as outcome indicators. A complete listingof the four outcomes with indicators is found in themanuscript detailing the validation with U.S. nurses (Daack-Hirsch et al., 2001).
Multivariate analysis of variance was used to examinedifferences between the U.K. and U.S. groups in ratings ofimportance and contribution. After determining a statisticallysignificant overall effect on a set of indicator ratings,individual indicators were examined for between-groupdifferences.
Findings
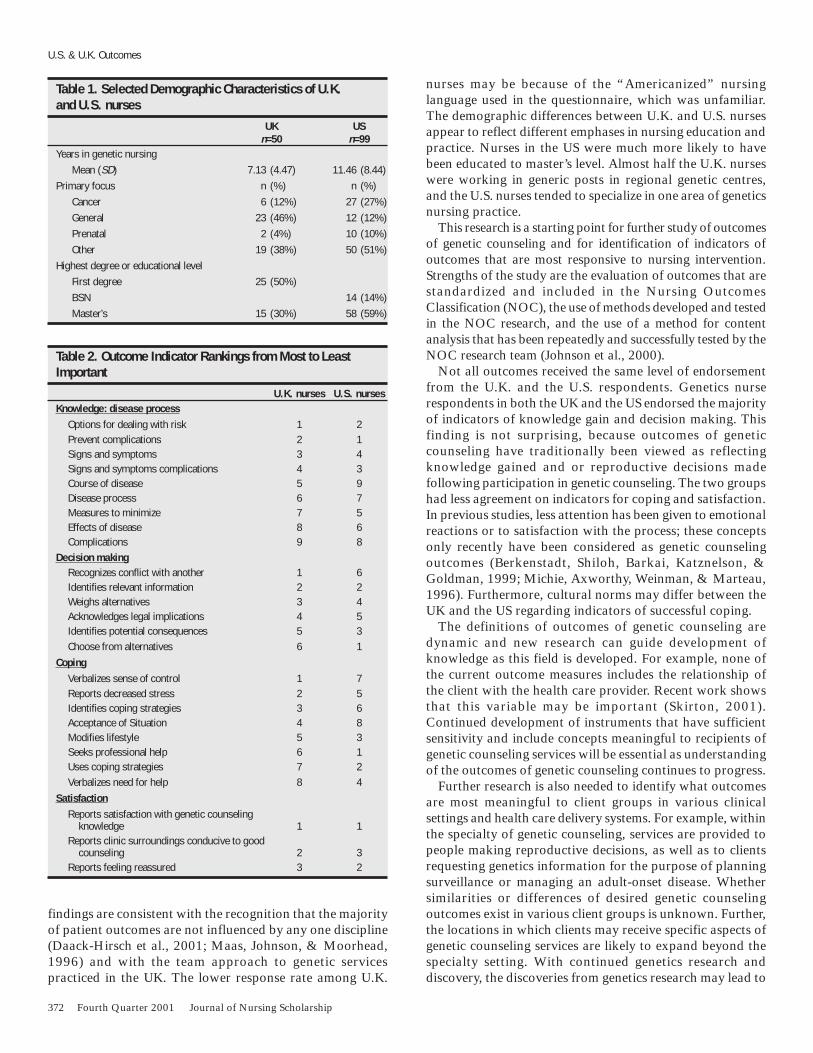
A total of 50 (37%) U.K. nurses and 99 (46%) U.S. geneticsnurses responded to the survey. Selected demographiccharacteristics are shown in Table 1. Results of Pearsoncorrelation analysis indicate strong agreement between theU.K. and U.S. nurse respondents regarding the overallimportance of outcome indicators (r=.72, p<.01) and thenursing contributions to each outcome (r=.60, p<.01).Respondents rated a portion of indicators for each outcomeas being critical to (>.80) or supporting factors (.79-.60) foreach outcome. Those indicators that both groups rated at.60 or above are presented in Table 2. Neither group ratednursing contributions to indicators for the outcomes at the.80 level or above.
Discussion
Results of this survey provide support for validation ofoutcomes of the genetic counseling process by U.K. geneticsnurses and documentation of their perceptions of thecollaborative role in the genetic counseling process. These
372 Fourth Quarter 2001 Journal of Nursing Scholarship
U.S. & U.K. Outcomes
findings are consistent with the recognition that the majorityof patient outcomes are not influenced by any one discipline(Daack-Hirsch et al., 2001; Maas, Johnson, & Moorhead,1996) and with the team approach to genetic servicespracticed in the UK. The lower response rate among U.K.
nurses may be because of the “Americanized” nursinglanguage used in the questionnaire, which was unfamiliar.The demographic differences between U.K. and U.S. nursesappear to reflect different emphases in nursing education andpractice. Nurses in the US were much more likely to havebeen educated to master’s level. Almost half the U.K. nurseswere working in generic posts in regional genetic centres,and the U.S. nurses tended to specialize in one area of geneticsnursing practice.
This research is a starting point for further study of outcomesof genetic counseling and for identification of indicators ofoutcomes that are most responsive to nursing intervention.Strengths of the study are the evaluation of outcomes that arestandardized and included in the Nursing OutcomesClassification (NOC), the use of methods developed and testedin the NOC research, and the use of a method for contentanalysis that has been repeatedly and successfully tested by theNOC research team (Johnson et al., 2000).
Not all outcomes received the same level of endorsementfrom the U.K. and the U.S. respondents. Genetics nurserespondents in both the UK and the US endorsed the majorityof indicators of knowledge gain and decision making. Thisfinding is not surprising, because outcomes of geneticcounseling have traditionally been viewed as reflectingknowledge gained and or reproductive decisions madefollowing participation in genetic counseling. The two groupshad less agreement on indicators for coping and satisfaction.In previous studies, less attention has been given to emotionalreactions or to satisfaction with the process; these conceptsonly recently have been considered as genetic counselingoutcomes (Berkenstadt, Shiloh, Barkai, Katznelson, &Goldman, 1999; Michie, Axworthy, Weinman, & Marteau,1996). Furthermore, cultural norms may differ between theUK and the US regarding indicators of successful coping.
The definitions of outcomes of genetic counseling aredynamic and new research can guide development ofknowledge as this field is developed. For example, none ofthe current outcome measures includes the relationship ofthe client with the health care provider. Recent work showsthat this variable may be important (Skirton, 2001).Continued development of instruments that have sufficientsensitivity and include concepts meaningful to recipients ofgenetic counseling services will be essential as understandingof the outcomes of genetic counseling continues to progress.
Further research is also needed to identify what outcomesare most meaningful to client groups in various clinicalsettings and health care delivery systems. For example, withinthe specialty of genetic counseling, services are provided topeople making reproductive decisions, as well as to clientsrequesting genetics information for the purpose of planningsurveillance or managing an adult-onset disease. Whethersimilarities or differences of desired genetic counselingoutcomes exist in various client groups is unknown. Further,the locations in which clients may receive specific aspects ofgenetic counseling services are likely to expand beyond thespecialty setting. With continued genetics research anddiscovery, the discoveries from genetics research may lead to
Table 1. Selected Demographic Characteristics of U.K.and U.S. nurses
UK USn=50 n=99
Years in genetic nursingMean (SD) 7.13 (4.47) 11.46 (8.44)
Primary focus n (%) n (%)Cancer 6 (12%) 27 (27%)General 23 (46%) 12 (12%)Prenatal 2 (4%) 10 (10%)Other 19 (38%) 50 (51%)
Highest degree or educational levelFirst degree 25 (50%)BSN 14 (14%)Master’s 15 (30%) 58 (59%)
Table 2. Outcome Indicator Rankings from Most to LeastImportant
U.K. nurses U.S. nursesKnowledge: disease process
Options for dealing with risk 1 2Prevent complications 2 1Signs and symptoms 3 4Signs and symptoms complications 4 3Course of disease 5 9Disease process 6 7Measures to minimize 7 5Effects of disease 8 6Complications 9 8
Decision makingRecognizes conflict with another 1 6Identifies relevant information 2 2Weighs alternatives 3 4Acknowledges legal implications 4 5Identifies potential consequences 5 3Choose from alternatives 6 1
CopingVerbalizes sense of control 1 7Reports decreased stress 2 5Identifies coping strategies 3 6Acceptance of Situation 4 8Modifies lifestyle 5 3Seeks professional help 6 1Uses coping strategies 7 2Verbalizes need for help 8 4
SatisfactionReports satisfaction with genetic counseling
knowledge 1 1Reports clinic surroundings conducive to good
counseling 2 3Reports feeling reassured 3 2

Journal of Nursing Scholarship Fourth Quarter 2001 373
U.S. & U.K. Outcomes
improved health through new mechanisms for early diagnosisand health promotion activities, more targeted treatments,and increased understanding of prevention for a wide varietyof conditions (Feetham, 2001).
These discoveries will accelerate the need for all healthcare providers to become familiar with genetics aspects ofhealth and illness and much of genetics health care might beprovided by primary care providers (Collins, 1999). Thus,the amount and complexity of genetics information abouthealth conditions, as well as the settings in which geneticsinformation is provided, are changing. Research based uponclient-sensitive definitions of outcomes of genetic counselingservices will be needed as information from geneticsdiscoveries is integrated into health care practice, includingthat of nurses.
In addition, research is needed to clarify the significanceof client and population characteristics. Various individualfactors such as age, health status, or gender may be associatedwith the client’s perceived expectations or priority of geneticcounseling outcomes. Understanding the effects of culturewill be especially critical as genetics discoveries are integratedor introduced into countries in which genetic counselingservices have not yet been established. Research which buildsupon identification of outcomes may clarify those aspects ofgenetic counseling that are universal as well as outcomes thatare more culturally based.
Results of this study contribute to the body of knowledgeon genetic counseling outcomes and nursing. However, resultsmust be interpreted within the limitations of the research.The data reflect a cross-sectional data collection of nurseswho responded to a mailed survey. Unfamiliarity with theprocess of validation of standardized nursing language mayhave limited the ability of respondents in both countries toprovide complete validation responses. Further, the wordschosen for the indicators are likely to reflect Americanlanguage use and may not be the terminology most familiarto nurses in the UK. A similar situation previously occurredin the UK when members of the AGNC reviewed documentson genetic counseling practice that were developed in the USby genetic counselors. Although the competencies definedby the National Society of Genetic Counselors (Fine et al.,1996) were considered by the AGNC Education WorkingGroup to be appropriate to describe the work of geneticnurses and counsellors in the UK, the American languagedescribing those competencies was not suitable for generaluse in the UK, and those statements were reworded by theWorking Group to make them more acceptable andcomprehensible to the British reader. As genetic counselingbecomes integrated into health care across the world,conceptualization of outcomes of genetic counseling inlanguage most meaningful to the practitioners and clientswill be needed.
Conclusions
Several implications of the results of the study are importantfor nurses in the field of genetics. First, support for the validity
of standardized outcomes of genetic counseling addsconfidence to their use and offers the potential of developingclinical databases that can be analyzed to assess theeffectiveness of genetic counseling by nurses. Second, the useof outcome indicators by both U.K. and U.S. nurses holdspromise for cross-cultural collaboration and research in thearea, while recognizing the cultural perspective that must betaken into account. Third, because knowledge is developingrapidly in genetics, investigators have the opportunity to askand study salient questions. This study added to knowledgeabout the outcomes these groups of nurses believed areresponsive to genetic counseling and revealed or clarified anumber of areas for future research.
We believe this study is the first to indicate the perspectivesof professional nurses regarding the outcomes of the geneticcounseling process. Future investigators may clarifycontributions of various health professions to outcomes of thegenetic counseling process when an interdisciplinary teamprovides it, as well as when individual health care providerssuch as nurses provide components of the process. Futureresearchers may also provide insights into the effectiveness ofvarious health care providers in achieving desired clientoutcomes. Research to assess the effectiveness of individualdisciplines is highly important for ensuring clients’ rights andsafety and for holding providers accountable for ethical andcost effective care.
References
Abramovsky, I., Godmilow, L., Hirschhorn, K., & Smith, H. (1980). Analysisof a follow-up study of genetic counseling. Clinical Genetics, 17, 1-12.
Ad Hoc Committee on Genetic Counseling of the American Society ofHuman Genetics. (1975). Genetic Counseling. American Journal ofHuman Genetics, 27, 240-242
AGNC Education Working Group. (2001). Development plan forprofessional genetic counsellors. Association of Genetic Nurses andCounsellors. Retrieved from http://www.agnc.eo.uk/registration.htm
American Association of Colleges of Nursing (AACN). (1998). The essentialsof baccalaureate education for professional nursing practice. WashingtonDC: American Association of Colleges of Nursing.
Anderson, G., Monsen, R., Prows, C., Tinley, S., & Jenkins, J. (2000).Preparing the nursing profession for participation in a genetic paradigmin health care. Nursing Outlook, 48(1), 23-27.
Ando, H. (2000). Pick up nursing view: The start of genetic nursing. Journalof the Kango Gijyutsu (Nursing Practices), 46(4), 71-78.
Bernhardt, B.A. (1997). Empirical evidence that genetic counseling isdirective: Where do we go from here? American Journal of HumanGenetics, 60, 17-20.
Berkenstadt, M., Shiloh, S., Barkai, G., Katznelson, M., & Goldman, B.(1999). Perceived personal control (PPC): A new concept in measuringoutcome of genetic counseling. American Journal of Medical Genetics,82, 53-59.
Carter, C.O., Fraser Roberts, J.A., Evans, K.A., & Buck, A.R. (1971). Geneticclinic: A follow-up. Lancet, 1(7693), 281-285.
Collins, F. (1999). Shattuck lecture: Medical and social consequences ofthe Human Genome Project. New England Journal of Medicine, 341(1),28-37.
D’Amico, R., Jacopini, G., Vivona, G., & Frontali, M. (1992). Reproductivechoices in couples at risk for genetic disease: A qualitative and quantitativeanalysis. Birth Defects: Original Article Series, 28, 41-46.
Daack-Hirsch, S., Williams, J.K., & Reed, D. (2001). Validation of geneticcounseling nursing outcomes. Unpublished manuscript, The Universityof Iowa at Iowa City, IA.
374 Fourth Quarter 2001 Journal of Nursing Scholarship
Elwyn, G., Gray, J., & Clarke, A. (2000). Shared decision making and non-directiveness in genetic counselling. Journal of Medical Genetics, 37(2),135-138.
Farnish, S.A. (1988). A developing role in genetic counselling. Journal ofMedical Genetics, 25, 392-395.
Feetham, S. (1997). The genetics revolution: Outcomes andrecommendations. In F.R. Lashley (Ed.), The genetics revolution:Implications for nursing (39-46). Washington DC: American Academyof Nursing.
Feetham, S. (Ed.). (in press). Nursing and genetics: Leadership for globalhealth. Geneva, Switzerland: International Council of Nurses.
Fehring, R.J. (1987). Methods to validate nursing diagnoses. Heart & Lung,16(6), 625-629.
Ferrer, T.L. (1975). Counseling patients with genetic abnormalities. NursingClinics of North America, 10, 293-305.
Fibison, W.J. (1983). The nursing role in the delivery of genetic services.Issues in Health Care of Women, 4, 1-15.
Fine, B., Baker, D., Fiddler, M., & ABGC Consensus DevelopmentConsortium. (1996). Practice-based competencies for accreditation of andtraining in graduate programs in genetic counseling. Journal of GeneticCounseling, 5, 113-121.
Forbes, N.P. (1966). The nurse and genetic counseling. Nursing Clinics ofNorth America, 1, 679-688.
Hallowell, N., Murton, F., Statham, H., Green, J.M., & Richards, M.P.(1997). Women’s need for information before attending geneticcounselling for familial breast or ovarian cancer: A questionnaire,interview, and observational study. British Medical Journal, 314,281-283.
Henry, B. (1998). Editorial: Globalization, nursing philosophy, and nursingscience. Image: Journal of Nursing Scholarship, 30, 302.
Hillsman, G.M. (1966). Genetics and the nurse. Nursing Outlook, 14,34-39.
International Society of Nurses in Genetics, Inc. (1998). Statement on thescope and standards of genetics clinical nursing practice. WashingtonDC: American Nurses Association.
Iowa Outcomes Project. (2000). Nursing outcomes classification (NOC;2nd ed.). St. Louis, MO: Mosby.
Jenkins, J., Masny, A., & Tranin, A. (in press). Recommendations for cancergenetics nursing practice and education. Pittsburgh PA: Oncology NursingSociety.
Johnson, M., & Maas, M. (1997). Iowa nursing outcomes classification(NOC): Iowa outcomes project. St. Louis, MO: Mosby-Yearbook.
Kirk, M. (1999). Preparing for the future: The status of genetics educationin diploma-level training courses for nurses in the UK. Nurse EducationToday, 19, 107-115.
Maas, M., Johnson, M., & Moorhead, S. (1996). Classifying nursing-sensitive patient outcomes. Image: Journal of Nursing Scholarship, 28,295-301.
Michie, S., Axworthy, D., Weinman, J., & Marteau, T. (1996). Geneticcounselling: Predicting patient outcomes. Psychology and Health, 11, 797-809.
Sahin, S.T. (1976). The multifaceted role of the nurse as genetic counselor.Maternal Child Nursing, 1, 211-216.
Shiloh, S., Avdor, O., & Goodman, R.M. (1990). Satisfaction with geneticcounseling: Dimensions and measurement. American Journal of MedicalGenetics, 37, 522-529.
Skirton, H. (2001). The client’s perspective of genetic counseling—a groundedtheory study. Journal of Genetic Counseling, 10(4), 311-329.
Skirton, H., Barnes, C., Curtis, G., & Walford-Moore, J. (1997). The roleand practice of the genetic nurse: Report of the AGNC working party.Journal of Medical Genetics, 34, 141-147.
Skirton, H., Barnes, C., Guilbert, P., Kershaw, A., Kerzin-Storrar, L., Patch,C., et al. (1998). Recommendations for education and training of geneticnurses and counsellors in the United Kingdom. Journal of MedicalGenetics, 35, 410-412.
Wertz, D.C., & Sorenson, J.R. (1986). Client reactions to genetic counseling:self-reports of influence. Clinical Genetics, 30, 494-502.
U.S. & U.K. Outcomes