Embed Size (px)
Citation preview
The Journal of Molecular Diagnostics, Vol. 16, No. 1, January 2014
jmd.amjpathol.org
See related article on page 89.
COMMENTARYGenomic Technologies and the New Era of GenomicMedicineArunkanth Ankala and Madhuri Hegde
From the Department of Human Genetics, Emory University School of Medicine, Atlanta, Georgia
Address correspondence to Madhuri Hegde, Ph.D., Department ofHuman Genetics, Emory University School of Medicine, 615 Michael St,Atlanta, GA 30322. E-mail address: [email protected]
Genetic technologies have been used extensively in thediscovery and diagnosis of constitutional disorders and cancer.These technologies range from cytogenetic analysis andstandard PCR-based methods to the more informative quanti-tative PCR, Southern blot analysis, microarrays, and Sangersequencing. In the last decade, we have witnessed the emer-gence of next-generation sequencing (NGS) technology withrapidly evolving sequencing chemistries and instruments,whichhas led to a boom in clinically available NGS-based assays. Theresearch community at large has since adopted rapidly NGStechnology for the discovery of new genes as well as genome-wide association studies. More importantly, NGS technologyhas made its way into the arena of clinical diagnostics forgenetically heterogeneous constitutional disorders (such asneuromuscular disorders, cardiomyopathy, and intellectualdisability), with several disease-specific diagnostic assays thatare now available.1e3 However, application of NGS to clinicaloncology testing, especially those involving somatic (acquired)mutations, is still in its infancy. In this issue of The Journal ofMolecularDiagnostics,Cottrell et al4 discuss thedesign, clinicalvalidation, and utility of a targeted NGS panel involving 25cancer-associated genes for somatic mutation detection.
Molecular Diagnosis of Cancer
Until recently, the molecular diagnosis of cancer relied mainlyon interrogating the most frequent mutations, or hotspot mu-tations or regions, and involved low-throughput molecular andcytogenetic methods, all of which are limited by the number ofmutations or target regions that can be tested in one assay.Nonetheless, over the years, a growing number of mutationsand genes have been identified in a variety of cancers such aslung, breast, melanoma, and brain cancer.
Often, the presence or absence of variants in a certaingene, like the KRAS mutations in colorectal cancers,
Copyright ª 2014 American Society for Investigative Pathology
and the Association for Molecular Pathology.
Published by Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.jmoldx.2013.11.001
modulates the efficacy and therapeutic outcome of anotherwise highly effective drug.5 Therefore, regardless ofthe cancer type, establishing a molecular diagnosis andknowing the exact causative gene and mutation are crucialfor directing therapeutic options and stratifying the overallrisk as well as in predicting the prognosis of cancer patients.This has driven a paradigm shift from single-gene, or hot-spot, testing, to parallel multigene testing using NGS tech-nology. However, given the nature of cancer mutations(which can be inherited or somatically acquired) and thecomplexity of the disease, the performance of NGS assaysneeds thorough evaluation before clinical application.
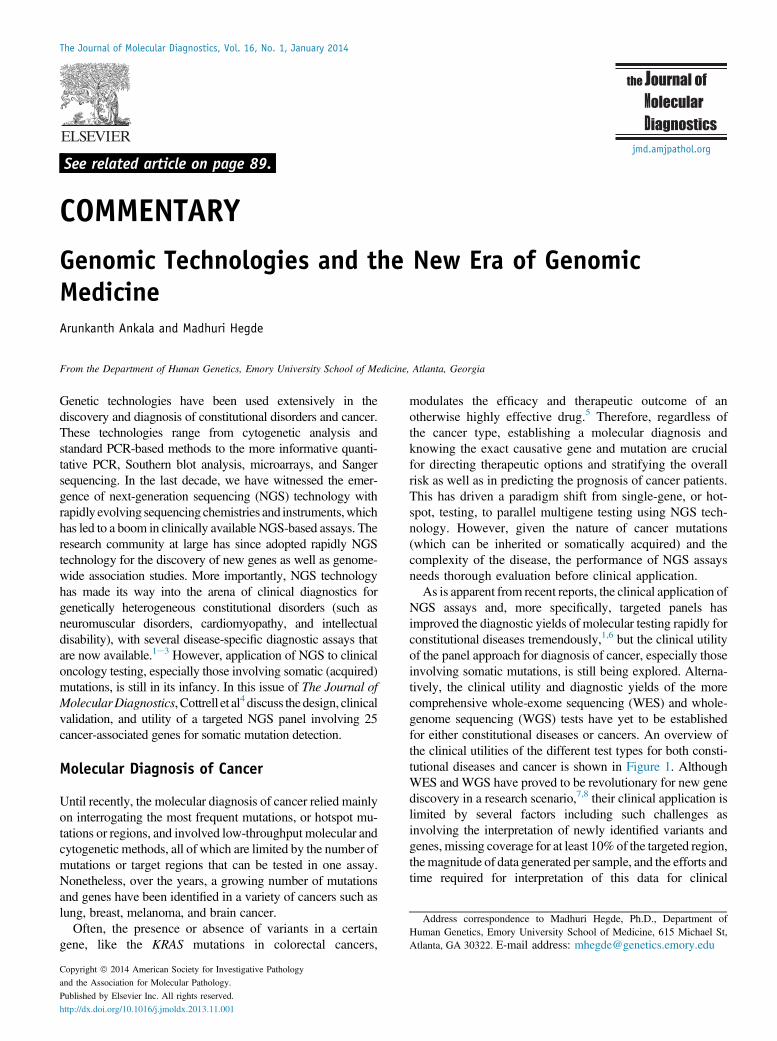
As is apparent from recent reports, the clinical application ofNGS assays and, more specifically, targeted panels hasimproved the diagnostic yields of molecular testing rapidly forconstitutional diseases tremendously,1,6 but the clinical utilityof the panel approach for diagnosis of cancer, especially thoseinvolving somatic mutations, is still being explored. Alterna-tively, the clinical utility and diagnostic yields of the morecomprehensive whole-exome sequencing (WES) and whole-genome sequencing (WGS) tests have yet to be establishedfor either constitutional diseases or cancers. An overview ofthe clinical utilities of the different test types for both consti-tutional diseases and cancer is shown in Figure 1. AlthoughWES and WGS have proved to be revolutionary for new genediscovery in a research scenario,7,8 their clinical application islimited by several factors including such challenges asinvolving the interpretation of newly identified variants andgenes, missing coverage for at least 10% of the targeted region,themagnitude of data generated per sample, and the efforts andtime required for interpretation of this data for clinical

Figure 1 Overview of the clinical utility of available clinical test types for constitutional disease and cancer diagnosis. A representative chromosome ismarked with gray horizontal bars with dark centromeres and telomeres. Different regions along the chromosome are highlighted or faded depending onwhether or not it is interrogated in the corresponding test. In whole-genome sequencing, most of the entire chromosome is interrogated, whereas in whole-exome sequencing, exons alone are interrogated. Likewise, although all exons of select genes associated with the disease are interrogated in targeted panels,only certain known causative variants or mutations are tested in site-specific hotspot mutation panels. The arrow bars on either side of the figure representthe measure of clinical utility of the different test types in disease diagnosis. VOUS, variant of unknown significance.
Ankala and Hegde
relevance. Compared to WES, however, WGS has theadvantage of being able to detect novel rearrangements incancer testing.9 Given all these factors, disease-specific tar-geted panels are constantly being developed and validated foruse in routine clinical diagnostics.
In contrast to some recently reported targeted cancerpanels that focus more on hotspot mutations in multiplecancer genes,10 the Washington University Cancer MutationProfiling (WUCaMP) assay developed by Cottrell et al4
interrogates the entire coding region of 25 cancer-associated genes for mutation detection. Such a compre-hensive assay is likely to have a higher diagnostic yieldcompared to those that only target hotspots within thesegenes, as mutations outside hotspots are equally important.
Clinical Design of the WUCaMP Assay
The WUCaMP assay involves deep sequencing of the entire300-kb targeted 25-gene region with an average coverage of>1000 � across the entire targeted region. The assay has100% sensitivity and specificity for single nucleotide variantdetection as well as 100% sensitivity for detecting variantsat an observed 10% allele fraction, confirming strong reli-ability of the assay for cancer diagnostics. Such thoroughvalidation of performance and sensitivity is critical sincethese are high-complexity assays as defined by ClinicalLaboratory Improvement Amendments and require anextensive investment in technology and informatics.
Several organizations, such as the College of American Pa-thologists and the CDC, have released detailed guidelines andrecommendations for validation and clinical implementation of
8
NGS assays.11 Nevertheless, given the differences in se-quencing chemistries, platforms, and the assortment of stepsinvolved in the entire assay, from sample preparation to dataanalysis and interpretation, clinical labs developing these assaysface significant challenges and, hence, seek guidance. Toaddress these concerns, Cottrell et al4 report the validation of theWUCaMP assay in detail.
Assay Validation
As is critical in cancer diagnostics, which frequently involvethe use of highly heterogeneous tissue specimens, Cottrellet al4 thoroughly validated the WUCaMP assay for itsperformance in detecting clinically actionable somatic can-cer mutations at low variant allele fraction (VAF). VAFrefers to the fraction by which a certain variant at an allele isrepresented in the cell population within a tissue specimen.The VAF for somatic tumor variants in the tissue specimenbeing tested depends on tumor cellularity as a result of itsinvasion into stroma and infiltration by immune cells as wellas on the precision with which the tumor tissue was isolatedfrom adjacent nontumor tissue.As part of their assessment of the assay’s analytical perfor-
mance for single nucleotide variant detection in clinical cancerspecimens, Cottrell et al4 analyzed 81 individual samples (78tumor specimens and 3 HapMap DNA cell lines) usingWUCaMP. Unlike the case of constitutional variants, where theVAF is most often as high as 50% (heterozygous mutations;100% for hemizygous or homozygous variants), the VAF forsomatic pathogenic tumor variants or mutations can varywidely, frequently 20% or less. Therefore, although the
jmd.amjpathol.org - The Journal of Molecular Diagnostics

Commentary
sensitivity for VAF is not a major issue for non-cancer consti-tutional diseases with the exception of rare mosaic cases, it canbe a significant limitation in the detection of acquired or somaticcancer-causing variants. In developing theWUCaMP assay, theauthors addressed this issue by using proportionately pooledDNA samples and strategic in silico mixtures of two differentHapMap samples and assessing the analytic performance indetecting variants with a resultant VAF as low as 10% or less.These dilution experiments showed 100% sensitivity for vari-ants with VAF greater than 10% in the targeted regions, whichis compelling. They then validated the reproducibility andversatility of the assay by comparing results from differentspecimen types (formalin-fixed, paraffin-embedded tissue,fresh-frozen tissue, blood, bone marrow, and cell lines), as wellas interrun and interpersonnel performances.
Advantages
In cancer genomes, the number of somatic mutations is typi-cally on the order of thousands, with most adult cancers beingin the 1000 to 10,000 range.12 Of these mutations, only a smallnumber are driver mutations (ie, those that confer a growthadvantage to the cell by altering a fundamental cellular pro-cess). Most are so-called passenger mutations, which may notcontribute to clonal selection and tumorigenesis but accumu-late over the lifetime of the tumor.13 The ability to distinguishdriver mutations from passenger mutations is therefore criticalto establishing diagnosis. An evidence-based gene panelapproach, which specifically detects variants in clinicallyrelevant genes, skirts this issue to a certain extent, unlikeWESandWGS that often detect a significant number of variants andgenes of unknown significance. One caveat, however, is thatcertain driver mutations harbored by untargeted genes aremissed by the panel approach. The false-negative rate isequally important in terms of the clinical utility of an assay.Data from 51 clinical patients tested after successful launch ofthe WUCaMP test indicated that there were no false negativesin the targeted coding region, and all mutations detected bySanger sequencing were detectable. Also, there were no false-positive variants detected in the region targeted byWUCaMP.High false-positive and false-negative rates have plagued mostof the current NGS-based assays, despite rapid advances intarget capture and NGS technology. Although these rates canbe reduced significantly by increasing the depth of sequencing,it raises the cost of the assay. The relatively small target size ofpanels (compared toWES andWGS) allows for high coveragedepth without significant increases in the sequencing cost. Insilico sensitivity analysis performed for the WUCaMP assayindicates that as high as 1000x unique coverage levels pick100% of all variants with an allele fraction of at least 10%.
Another significant finding of the Cottrell et al4 study is thedetection of a high-quality, low-allelic fraction single nucle-otide variant that was not detected by Sanger sequencing.Detection of this true positive variant by a targeted NGSapproach emphasizes the potential of the technology over the
The Journal of Molecular Diagnostics - jmd.amjpathol.org
relatively less sensitive Sanger sequencing. With optimalcoverage depth and thorough validation of assays, the expec-tation is that NGS panels eventually can be offered as stand-alone tests without complementary Sanger confirmation.Though this is currently not the practice in clinical labs, studiessuch as this and others14 will soon make it a reality.
Limitations
Knowing the limitations of a test is critical to making aninformed decision about ordering that test for any disease,and Cottrell et al4 do indeed elaborate on the limitations of theassay. One such limitation is the lack of sufficient coverage(at least 50�) for 14 of 393 exons (3.6%), most of which areGC-rich first exons of several of the targeted genes. This istrue for most of clinically available NGS panel tests and is infact a limitation of the available sequencing chemistries.1,6
However, the authors indicate that these missed exons maynot be clinically significant since causative mutations haverarely been reported in these exons.
A second limitation discussed by the authors is the sensi-tivity of somatic variant detection. Although the WUCaMPassay can detect variants with an allele fraction as low as 10%with a sensitivity of 100%, the sensitivity for variants withallele fraction 5% and 1% is zero. Knowing this is important,especially when dealing with impure and heterogeneoustumor specimens or with challenging specimen types, likeformalin-fixed, paraffin-embedded samples, as formalin fix-ation is known to gradually degrade nucleic acids.
One added advantage of NGS assays, is their ability toprocess pooled multiple samples and perform parallelsequencing, allowing for an appreciable cost reduction. Themaximum number of samples that can be pooled togethernevertheless is dependent on the size of the targeted regionand the read and coverage depth required to make a confidentcall on the detected variant. However, this must be evaluatedand validated for each individual NGS panel assay. Oncethese parameters are determined, multiple individual sam-ples, each referred for the test, are processed simultaneouslyand pooled together after tagging each DNA sample with ashort unique sequence index, specific for each patient.Though this is a routine practice in NGS labs, it is compellingthat Cottrell et al4 saw as low as 0.18% crossover during li-brary preparation and 0.03% to 0.06% estimated crossoverduring multiplex sequencing of pooled samples.
Perspectives on the WUCaMP Assay
The validation procedures reported in this study can behelpful for organizations formulating regulations and rec-ommendations for clinical NGS practice, as well as forlaboratories developing similar assays. NGS technology hastruly shifted the paradigm of medical genetics from theconcept of one gene/one disorder to one gene/many disor-ders and many disorders/many genes.
9

Ankala and Hegde
Along with the increasing throughput and the ability tomassively sequence large sections of the genome come thechallenges of interpreting novel variants (including both dis-ease associated and unassociated) and identifying false posi-tives (which are technical artifacts). Large-scale WES datafrom various groups, such as the National Heart Lung andBlood Institute’s Exome Sequencing Project, have helped tosome extent in interpreting these variants. Moreover, recentNIH awards to Clinical Genome Resource to annotate variantsfor their clinical relevance and disease association and todisseminate this information through the National Center forBiotechnology Information’s ClinVar are expected to furtherimprove our ability to interpret variants as we move into theNGS era of genomic medicine. Meanwhile, internally curatedvariant databases and complementary software packages suchas those developed to support the WUCaMP assay are crucialto analyzing the data generated from NGS assays. Clinicallaboratories venturing into NGS testing should thus be pre-pared accordingly, so as to reduce analysis burden and improvetest efficiency.
Conclusions
Overall, the WUCaMP assay serves as a good proof-of-principle study for somatic cancer mutation detection onclinical cancer specimens and outlines the critical validationstrategies that can be adopted in developing an NGS-basedtarget panel test for cancer diagnostics. Ongoing efforts toextend the assay’s potential to detect additional sequencechanges, such as copy number variations, structural rear-rangements, and small insertions and deletions, will signif-icantly improve the overall clinical utility of targeted NGSassays, both for constitutional disease and cancer diag-nosis.15 This is a major concern for cancers, more than forconstitutional diseases, as structural rearrangements andcopy number variations leading to loss of heterozygosity aremore common.
We can state that new technology is evolving rapidly, andgreat strides are being made to bring it to bear on diagnosticsfor the betterment of patient care. However, due to a lack ofsupporting evidence and thorough validation, these emergingtechnologies are still being complemented with additionalSanger sequencing for the confirmation of observed variants.Thorough optimization to yield high positive-predictivevalues, such as those observed by Cottrell et al4 (98% to100%), and to detect true positives missed by less sensitiveconventional methods will make these NGS assays quitedependable. We fully expect comprehensive NGS-basedtesting to emerge quickly as a standalone test in routine can-cer clinical diagnosis and patient care.
References
1. Jones MA, Rhodenizer D, da Silva D, Huff IJ, Keong L, Bean LJ,Coffee B, Collins C, Tanner AK, He M, Hegde MR: Molecular
10
diagnostic testing for congenital disorders of glycosylation (CDG):detection rate for single gene testing and next generation sequencingpanel testing. Mol Genet Metab 2013, 110:78e85
2. Valencia CA, Ankala A, Rhodenizer D, Bhide S, Littlejohn MR,Keong LM, Rutkowski A, Sparks S, Bonnemann C, Hegde M:Comprehensive mutation analysis for congenital muscular dystrophy: aclinical PCR-based enrichment and next-generation sequencing panel.PLoS One 2013, 8:e53083
3. Vasli N, Bohm J, Le Gras S, Muller J, Pizot C, Jost B, Echaniz-Laguna A, Laugel V, Tranchant C, Bernard R, Plewniak F, Vicaire S,Levy N, Chelly J, Mandel JL, Biancalana V, Laporte J: Next genera-tion sequencing for molecular diagnosis of neuromuscular diseases.Acta Neuropathol 2012, 124:273e283
4. Cottrell CE, Al-Kateb H, Bredemeyer AJ, Duncavage EJ, Spencer DH,Abel HJ, Lockwood CM, Hagemann IS, O’Guin SM, Burcea LC,Sawyer CS, Oschwald DM, Stratman JL, Sher DA, Johnson MR,Brown JT, Cliften PF, George B, McIntosh LD, Shrivastava S,Nguyen TT, Payton JE, Watson MA, Crosby SD, Head RD, Mitra RD,Nagarajan R, Kulkarni S, Seibert K, W. Virgin IV HW, Milbrandt J,Pfeifer JD: Validation of a next-generation sequencing assay forclinical molecular oncology. J Mol Diagn 2014, 16:89e105
5. Karapetis CS, Khambata-Ford S, Jonker DJ, O’Callaghan CJ, Tu D,Tebbutt NC, Simes RJ, Chalchal H, Shapiro JD, Robitaille S, Price TJ,Shepherd L, Au HJ, Langer C, Moore MJ, Zalcberg JR: K-ras muta-tions and benefit from cetuximab in advanced colorectal cancer. NEngl J Med 2008, 359:1757e1765
6. Punetha J, Hoffman EP: Short read (next-generation) sequencing: atutorial with cardiomyopathy diagnostics as an exemplar. Circ Car-diovasc Genet 2013, 6:427e434
7. Ng SB, Bigham AW, Buckingham KJ, Hannibal MC, McMillin MJ,Gildersleeve HI, Beck AE, Tabor HK, Cooper GM, Mefford HC,Lee C, Turner EH, Smith JD, Rieder MJ, Yoshiura K, Matsumoto N,Ohta T, Niikawa N, Nickerson DA, Bamshad MJ, Shendure J: Exomesequencing identifies MLL2 mutations as a cause of Kabuki syndrome.Nat Genet 2010, 42:790e793
8. Varela I, Tarpey P, Raine K, Huang D, Ong CK, Stephens P, et al:Exome sequencing identifies frequent mutation of the SWI/SNFcomplex gene PBRM1 in renal carcinoma. Nature 2011, 469:539e542
9. Welch JS, Westervelt P, Ding L, Larson DE, Klco JM, Kulkarni S,Wallis J, Chen K, Payton JE, Fulton RS, Veizer J, Schmidt H,Vickery TL, Heath S, Watson MA, Tomasson MH, Link DC,Graubert TA, DiPersio JF, Mardis ER, Ley TJ, Wilson RK: Use ofwhole-genome sequencing to diagnose a cryptic fusion oncogene.JAMA 2011, 305:1577e1584
10. Harismendy O, Schwab RB, Bao L, Olson J, Rozenzhak S,Kotsopoulos SK, Pond S, Crain B, Chee MS, Messer K, Link DR,Frazer KA: Detection of low prevalence somatic mutations in solidtumors with ultra-deep targeted sequencing. Genome Biol 2011, 12:R124
11. Gargis AS, Kalman L, Berry MW, Bick DP, Dimmock DP,Hambuch T, et al: Assuring the quality of next-generation sequencingin clinical laboratory practice. Nature Biotechnol 2012, 30:1033e1036
12. Greenman C, Stephens P, Smith R, Dalgliesh GL, Hunter C, Bignell G,et al: Patterns of somatic mutation in human cancer genomes. Nature2007, 446:153e158
13. Hanahan D, Weinberg RA: The hallmarks of cancer. Cell 2000, 100:57e70
14. Sikkema-Raddatz B, Johansson LF, de Boer EN, Almomani R,Boven LG, van den Berg MP, van Spaendonck-Zwarts KY, vanTintelen JP, Sijmons RH, Jongbloed JF, Sinke RJ: Targeted next-generation sequencing can replace Sanger sequencing in clinical di-agnostics. Hum Mutat 2013, 34:1035e1042
15. Spencer DH, Abel HJ, Lockwood CM, Payton JE, Szankasi P,Kelley TW, Kulkarni S, Pfeifer JD, Duncavage EJ: Detection of FLT3internal tandem duplication in targeted, short-read-length, next-gener-ation sequencing data. J Mol Diagn 2013, 15:81e93
jmd.amjpathol.org - The Journal of Molecular Diagnostics