Embed Size (px)
Citation preview

Genotype-phenotype correlation studies and tailored treatment for the most common monogenic epilepsies: KCNQ2
John J. Millichap, MD, FAAN, FAESPediatric EpileptologistAssociate Professor of Pediatrics and Neurology
September 2020

Spectrum of Severity in Channelopathy-associated Epilepsy
2
Genetically determined alteration in ion channel function that results in seizures, cognitive/motor impairment, and other comorbidities
Gain-of-function or loss-of-function of these ion channels results in neuronal hyperexcitability and seizures
Multiple ion channels have been associated with childhood epilepsy so far (SCN1A, SCN1B, SCN2A, SCN8A, KCNQ2, KCNQ3, KCNT1, and KCNB1)
Spectrum of severity may be related to location and functional status of the specific variants, among other factors

3
KCNQ2Phenotypes

Benign Familial Neonatal Epilepsy
Onset of brief, multifocal, tonic or clonic seizures, +/- apnea during the first week of life.
Seizures may be treated briefly, but usually self-resolve within several months.
Normal neurologic examination, normal EEG, and negative evaluation for another etiology of the seizures.
Prognosis is good (10% seizure recurrence) with usually normal developmental outcome.
4Berg et al. Epilepsia 2010.; Ronen et al. Neurology 1993.

5
KCNQ2Phenotypes

6

7
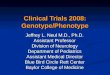
Focal Tonic Seizure in a Neonate with Pathogenic Variant in KCNQ2

EEG in KCNQ2-DEE: “Excessive discontinuity for age and multifocal epileptiform discharges”
8

9
KCNQ2 = 10SCN2A = 3

Why is it important to recognize KCNQ2Neonatal Epilepsy?

Initial presentation
• No initial concerns. • DOL #2, parents noted
events after feeding:– whole body stiffening, head
deviation, crying, heavy breathing, and perioral cyanosis
– lasted about 10 seconds and occurred a few times per day
• Not recognized as a seizure.• Discharged home with her
parents.• Pediatrician ordered EEG at 7
days old.
11

• Admitted to LCH at 3 m old– IV fosphenytoin stopped
seizures– Started carbamazepine orally– No seizures – Weaned off LVT, PB, and TPM
• KCNQ2 novel, de novo variant: c.871A>G; p.R291G
12

2 days 7 days 2.5 months 3 mos 4 mos
Events after feeding:• whole body stiffening,
head deviation, crying, heavy breathing, and perioral cyanosis
• lasted about 10 seconds and occurred a few times per day
• Recognize Genetic syndrome
• Start effective treatment
• Video EEG confirmed seizures at 7 days old
• MRI brain and other tests negative.
• 25 seizures a day• Multiple medications
failed
• Epilepsy Gene Panel confirms KCNQ2 as cause of epilepsy
Utility of Genetic Testing
Earlier genetic testing would
confirm diagnosis and
change treatment.
Referred to Epilepsy Center
Seizure free after Tailored Therapy

Potassium Channel Opener Potentially Effective Treatment
14
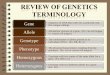
Tetramericarrangement of subunits around the ion pore
Coupling allows voltage-gated opening and closing; EZG binds pore domain
Millichap and Cooper, Epil Curr, 2012

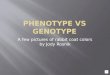
Increase in KCNQ2 Channel Activity May Improve Outcomes
Mild
MILD SEVERE
KCNQ2Activity
Normal BFNE KCNQ2-DEE
Benign Familial Neonatal Epilepsy
KCNQ2 –DEE(Ohtahara syndrome)
K ChannelOpener

Ezogabine is Only FDA-approved KCNQ2 Channel Opener: Case Series in Children*
Millichap et al., Neurol Genetics, 2016
Ezogabine associated with improvements in seizures and/or development
3 of 4 infants treated <6 months old benefited most
2 of 7 children treated later also benefited
Low Adverse Events
*FDA-approval in adults only. Expert off-label use.

Rare gain-of-function variants
17
KCNQ2Phenotypes

GOF Variant with Infantile Spasms as Initial Seizure type
18
4 infants presented with IS at 4-6 months old withoutneonatal seizures
Infantile spams in clusters and hypsarhythmia on EEG
R198Q GOF in heterologous expression studies
All eventually seizure free with moderate-severe delays

Rare gain-of-function variants
19
KCNQ2Phenotypes

GOF Variant with Neonatal Nonepileptic Myoclonus
20
Myoclonus without EEG correlate from birth
Prominent respiratory failure and/or hypoventilation
R201C/H GOF in heterologous expression studies
All with profound delays

Conclusion:Precision Medicine For KCNQ2-DEE Due to Loss-of-function Variants
21
KCNQ2-DEE is a severe and ultra-rare disease in need of new treatment options
Pathogenic variants in KCNQ2 most commonly result in decreased activity (loss-of-function) of voltage-gated potassium channels
Ezogabine, and other potassium channel agonists, specifically targets and partially corrects the potassium channel activity
Even a modest increase in potassium channel activity may improve outcomes