Embed Size (px)
DESCRIPTION
GI POSTER SESSION ESOPHAGEAL CANCER. Joel Tepper, MD Dept of Radiation Oncology UNC School of Medicine. A Scandinavian randomized trial of Chemoradiotherapy versus Surgery alone in patients with resectable esophageal cancer. - PowerPoint PPT Presentation
Citation preview

GI POSTER SESSIONESOPHAGEAL CANCER
Joel Tepper, MD
Dept of Radiation Oncology
UNC School of Medicine

A Scandinavian randomized trial of Chemoradiotherapy versus Surgery alone in patients with resectable esophageal cancer
Hanna Carstens, Maria Albertsson, Signe Friesland, Gunnar Adell, Gunnar
Wagenius, Gunilla Frykholm, Ivan Farago, Helge E. Myrvold, Dag Stockeld
2007 ASCO Annual Meeting

Methods• Accrual between 2000 and 2004 • 91 patients with esophageal cancer• Resectable squamous cell
carcinoma or adenocarcinoma • Primary located above the cardia• No metastases• Endoscopy (+/- EUS) + CT staging

Chemotherapy• One cycle induction, 2 cycles with
RT• Cisplatin 100 mg/m2, day 1 • 5-fluorouracil 750 mg/m2/24 hours,
infusion day 1-5, • Three weeks cycles

Local Therapy
• 64 Gy , 5 days/wk, 200 cGy/fx
• 5 cm proximal and distal margin to 44 Gy
• Supraclav nodes treated for tumors above the carina, celiac nodes for tumors below the carina
• 2 cm margins to 64 Gy
• Surgery- Ivor-Lewis esophagectomy

Results• Survival defined from randomisation• Intent to treat analysis• 50% adenoca• 80% male• 55% Stage III• Treatments generally well tolerated• Surgery performed in 39 pts
– 32/39 (76%) had radical resection• 10 pts with micro or macro residual disease
– Median hospital stay- 18 days

Survival1 year 2 year 4 year Median
(mos)
RT + chemo
56% 37% 29% 12.8
Surgery alone
55% 25% 23% 15.8

Esophageal cancer• Reasonable treatment arms• Only 91 pts accrued
– Low power to detect a survival difference between the two approaches
• No suggestion of a survival difference• Supports other data suggesting that primary radiation
therapy with concurrent chemo is equivalent to surgery in survival
• No obvious morbidity differences• No local control data provided
– May be of great importance for QOL analysis
• Quality of life data could be of importance

Combination of endoscopic mucosal resection and
chemoradiotherapy as a nonsurgical treatments for patients with clinical stage I esophageal squamous cell
carcinoma.K. Minashi, A. Ohtsu, K. Mera, M. Muto, T. Yano, M. Tahara, T. Doi, M. Nishimura, K. Nihei

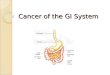
Tumors: • depth < focal SM invasion &• width < 2/3 circumference
Pathology: M & vessel infiltration (-)
Primary CRT
Prophylactic CRTObservation only
Treatment algorithm of EMR/CRT for clinical Stage I ESCC
Primary EMR
Salvage EMR
Local residual, recurrent ormetachronous lesion
Pathology: SM or M with vessel infiltration (+)
Incomplete resectionComplete resection
Tumors: • depth > focal SM invasion or• width > 2/3 circumference

A saline solution of dilute epinephrine (0.02 mg/ml) was injected into the SM layer.
The lesion was held up by forceps and resected using a high-frequency electrified snare wire.
When en bloc resection was not possible, the lesions were removed piecemeal.
Procedure of EMR

Eligibility• Squamous cell ca• Clinical Stage I• Age < 75• PS < 2• Only focal submucosal invasion• < 2/3 circumference• RT (40 Gy with 1 week break)/5-FU (400 mg/m2/d x
10)/platinum (40 mg/m2/d x 2) for submucosal invasion at EMR
• Other pts received 60 Gy (with 2 week break)/5-FU (800 mg/m2 x5, twice)/platinum (80 mg/m2/d x 2) without EMR

Therapy Received
• 86 pts• 41 primary EMR
– 11 received planned RT + chemo• 1 required salvage surgery
– 1 esophagectomy
• 45 primary RT/chemo– 11 required salvage EMR– 2 required salvage surgery– 1 chemotherapy for local recurrence

4 - Year Survival
• Median 5 year followup
• All patients 75%
• Primary EMR 78%
• Primary RT + chemo 73%

Discussion
• Group of patients not commonly seen in the US
• Can these pts be easily identified?• Good survival results, but very early
subset of patients• Radiation dose scheme unconventional• Unclear whether better outcomes could
result from more aggressive therapy

Impact of radiation regimen on local relapse-free Impact of radiation regimen on local relapse-free survival and palliative procedures for patients with survival and palliative procedures for patients with
resectable locally advanced esophageal cancer treated resectable locally advanced esophageal cancer treated with chemoradiation with chemoradiation
Results based on a phase III trial from the Fédération Results based on a phase III trial from the Fédération Francophone de Cancérologie Digestive (FFCD 9102).Francophone de Cancérologie Digestive (FFCD 9102).
G CREHANGEG CREHANGE, F BONNETAIN, P MAINGON , L BEDENNE, F BONNETAIN, P MAINGON , L BEDENNE
et al. on behalf of the et al. on behalf of the

Background and PurposeBackground and Purpose
FFCD 9102 trial demonstrated that exclusive FFCD 9102 trial demonstrated that exclusive chemoradiation (ECRT) is an alternative to surgery (S) chemoradiation (ECRT) is an alternative to surgery (S) for responding patients. for responding patients.
To compare 2 schemes of RT allowed by the protocol- To compare 2 schemes of RT allowed by the protocol- short or long course RTshort or long course RT
To explore their impact on palliative procedures, Local To explore their impact on palliative procedures, Local Relapse-Free Survival and Overall SurvivalRelapse-Free Survival and Overall Survival
Analysis : all eligible patientsAnalysis : all eligible patients Subgroup analysis : operated and non-operated Subgroup analysis : operated and non-operated
patientspatients
(1) Bedenne L et al: Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol 25:1160-1168, 2007

Eligibility CriteriaEligibility Criteria
SCC or adenocarcinoma SCC or adenocarcinoma Upper, middle or inferior 1/3 (except cervical)Upper, middle or inferior 1/3 (except cervical) T3 N0-1 according to CT or EUS staging T3 N0-1 according to CT or EUS staging M0M0 Judged resectable Judged resectable WHO WHO 2 2

PopulationPopulation 1993 – 2000 = 57 Centers1993 – 2000 = 57 Centers
5not eligible
285Split Course RT
(SRT)
161Conventional protracted RT
(PRT)
446included
451registered

FFCD 9102FFCD 9102RT DesignRT Design
- Split-course :- Split-course : R R
D1 D1 D22 D22 A : Surgery A : Surgery CTCT
D43D43 D64 D64 D92D92
RTRT B : B :
- Conventional:- Conventional: R R
D1 D1 D22 D22 A : Surgery A : Surgery CTCT
B : B :
D43 D43 D64 D64 D92 D92
RTRT
15Gy/5*3Gy/1w
46Gy/5*2Gy/4.5w
20Gy/5*2Gy/2w
15Gy/5*3Gy/1w
15Gy/5*3Gy/1w

FFCD 9102FFCD 9102CT DesignCT Design
Chemotherapy :Chemotherapy :
- 5 FU- CI :800 mg/m- 5 FU- CI :800 mg/m22/d x 5/d x 5
- CDDP :- CDDP : 75 mg/m75 mg/m2 2 D2 or 15 mg/mD2 or 15 mg/m22/d x 5/d x 5 Radiation TherapyRadiation Therapy
– Short course- 3 Gy x 5, weeks 1 and 4, (total 30 Short course- 3 Gy x 5, weeks 1 and 4, (total 30 Gy), Gy),
» plus 3 Gy x 5 if no surgery (total 45 Gy)plus 3 Gy x 5 if no surgery (total 45 Gy)
– Long course- 2 Gy x 23- (total 46 Gy), Long course- 2 Gy x 23- (total 46 Gy), » plus 2 Gy x 10 if no surgery (total 66 Gy)plus 2 Gy x 10 if no surgery (total 66 Gy)

Patients’ baseline characteristicsPatients’ baseline characteristics
All patientsAll patients
n (%)n (%)
SRT SRT
285 (64)285 (64)
PRTPRT
161(36)161(36)
pp
Mean tumor length - cmMean tumor length - cm 6.86.8 6.56.5 0.860.86
Mean diameter - cmMean diameter - cm 3.23.2 3.23.2 0.650.65
N+ - n (%)N+ - n (%)
SCC - no. (%)SCC - no. (%)
122 (43)122 (43)
158 (92)158 (92)
70 (44)70 (44)
72 (82)72 (82)
0.970.97
0.010.01

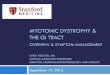
Results –Results –Local Relapse Free SurvivalLocal Relapse Free Survival
log-rank p=0.002
n=446
77%
57%
HR = 0.52 ; [CI95 0.34 – 0.79]

Results – Results – Overall SurvivalOverall Survival
log-rank p =0.25

PP according to the radiation scheme all PP according to the radiation scheme all eligible patients (n= 446)eligible patients (n= 446)
P-RTP-RT SC-RTSC-RT pp
Mean length of Mean length of hospital stayhospital stay
48.0 d48.0 d 60.5 d60.5 d 0.00030.0003
Mean number of Mean number of dilatation sessionsdilatation sessions
0.60.6 0.70.7 0.40.4
Mean number of Mean number of stentsstents
0.20.2 0.30.3 0.030.03
Mean number of any Mean number of any PPPP
1.01.0 1.51.5 0.0010.001
Mean dysphagia Mean dysphagia gradegrade
3.03.0 3.13.1 0.20.2

DISCUSSION
• Little data on RT technique in esophageal cancer
• Major interest in more accelerated radiation schemes in a variety of tumors– Minimal comparative data– Risk of increased acute and late toxicity– Biological basis to be concerned about late effects
with high doses per fraction– Potential advantage to decreasing overall time of
treatment to prevent repopulation

DISCUSSION
• Study not randomized regarding radiation treatment schedule, so results could be biased
• Although adenocarcinomas were allowed on trial this was a study of squamous cell carcinomas– Toxicity end-points are unlikely to be effected by the
histology of the primary
• Substantial patient numbers

DISCUSSION
• Local control was inferior with short course therapy
• Acute toxicity was the same• Late toxicity was worse with short course
– Stent rate– Number of palliative procedures– Length of hospital stay (total)
• An increased radiation dose in short course arm could have resulted in equivalent local control, but probably with substantially more acute and late toxicity

DISCUSSION
• Even as a non-randomized retrospective analysis this trial provides valuable information on likely role of short course radiation therapy
• Standard radiation fractionation should be used except in the clinical trial setting.

DEFINITIVE CHEMORADIOTHERAPY (CRT) WITH FOLFOX 4 OR 5FU-CISPLATIN AS FIRST-LINE TREATMENT OF PATIENTS (PTS) WITH INOPERABLE ESOPHAGEAL
CANCER (IEC) : FINAL RESULTS OF A RANDOMIZED PHASE II STUDY
T. Conroy (1), Y. Yataghene (2), PL. Etienne (3), P. Michel (4), H. Senellart (5), JL. Raoul (6), L. Mineur (7), M. Rives (8), X. Mirabel (9), A. Adenis (9).
(1) Centre Alexis Vautrin, Nancy ; (2) sanofi-aventis france, Paris ; (3) Clinique Armoricaine, St-Brieuc ; (4) University Hospital, Rouen; (5) Centre Rene Gauducheau, Nantes ; (6) Centre Eugene Marquis Rennes ; (7) Clinique Sainte Catherine, Avignon ; (8) Centre Claudius Regaud, Toulouse; (9) Centre Oscar Lambret, Lille; France.

Background (1)
• In inoperable esophageal cancer, concurrent chemoradiotherapy using 5FU-Cisplatin is the standard of care
• 5FU-Cisplatin regimen: – 20% of patients experienced major toxicities– 40 % of patients could not complete full sequence of treatment
• Oxaliplatin has shown encouraging activity in tumors that respond to cisplatin or carboplatin
• Oxaliplatin/5-fluorouracil/leucovorin is active in gastric adenocarcinoma
• Phase I data demonstrate safety of RT/FU/oxaliplatin

Objectives
• Primary Objectives :
- feasibility (completion of full planned treatment)1 of FOLFOX 4 regimen or 5-FU/Cisplatin regimen with concomitant radiotherapy as first-line treatment of inoperable advanced esophageal cancer.
- To assess endoscopic complete response2 rate in both arms.

Methods
• Initial randomized Phase II • At the end of the first part of the trial (randomised phase
II)- 88 patients (44 in each arm), decision to continue the study will be based on
-Good accrual rates (88 patients < 18 months) -Completion of full treatment in over 60% in the experimental arm (Folfox)-Endoscopic complete response rate of Folfox arm equal or superior to the endoscopic response rate of 5FU/Cisplatin arm.

Methods
Main inclusion criteria
• adenocarcinoma, squamous cell or adenosquamous carcinoma of the esophagus
• Patients unfit for surgery or locally advanced esophageal carcinoma (disease status : any T, N0 or N1, M0 or M1a)
• No prior treatment for esophageal cancer

Treatment
Chemotherapy in Folfox arm : six bi-weekly cycles of FOLFOX 4, the first 3 cycles starting on D1, D15 and D29 concomitant with 5 weeks’ radiotherapy; On day 1, Oxaliplatin 85mg/m² , on D1 and D2: leucovorin 200mg/m², 5-FU bolus 400mg/m²/d + 600mg/m²/d continuous IV infusion
(1) Giovannini M et al.; J Clin. Oncol. 2004; 22 (14S) : 324 s; Abstract 4044
Arm Folfox 4-RT (50Gy) (1)
CRT
d29-30
RT
d31-33 d36-40
RT
Cycle 3
d22-26
RTCRT
d15-16
RT
d17-19
Cycle 2
CRT
d1-2
RT
d3-5 d8-12
RT
Cycle 1
CT
d71-72
Cycle 6
CT
d57-58
Cycle 5
CT
d43-44
Cycle 4 Tumor assessment
W 1 W 3 W 5
W 7 W 9 W 11 W 15

Treatment
Chemotherapy in 5FU-Cisplatin arm : two cycles of 5-FU/Cisplatin on week 1 and 5 of radiotherapy and two cycles of chemotherapy with 5-FU / Cisplatin on weeks 8 and 11; On D1, Cisplatin 75 mg/m² and from day 1 to 4, 5-FU 1000 mg/m²/day
(2) Herskovic A et al, N Engl J Med 1992;326:1593-8
Arm 5FU-Cisplatin-RT (50Gy) (2)
d34-49
RTCRT
d29-32
RT
d33
Cycle 2
d22-26
RTRT
d15-19
CRT
d1-4
RT
d5 d8-12
RT
Cycle 1
CT
d71-74
Cycle 4
CT
d50-53
Cycle 3
W 1
Tumor assessment
W 8 W 11 W 15
W 5

RESULTS
• 80% of pts with squamous cell ca• 55% Stage III- almost all the others Stage II• App 90% pts completed planned RT/chemo• App 75% pts completed planned chemo• Toxicities very similar between arms
(except neurotoxicity in FOLFOX arm)• Endoscopic CR- 45% vs 30% favoring
FOLFOX

Efficacy results
FOLFOX regimenn = 53
No. of patients (%)
5FU-Cisplatin regimenn = 44
No. of patients (%)
Median [Confidence Interval 95%]
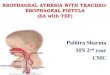
• Event-Free Survival (EFS) 14.3 mth [8.6-16.1] 7.8 mth [5.3-12.1]
• Time to Progression (TTP) 15.2 mth [9.9-18.9] 9.4 mth [7.2-ongoing]
• Overall Survival (OS) 22.7 mth [7.1-ongoing] 14.9 mth [9.6-19.0 ]

Results – Overall Survival
Folfox arm 5-FU / Cisplatin arm
Folfox arm 22.7 mth [7.1-ongoing]
5-FU / Cisplatin arm 14.9 mth [9.6-19.0]

DISCUSSION
• Definitive radiochemotherapy with FOLFOX 4 is feasible in inoperable esophageal cancer.
• Survival data are promising, but Phase II data are often encouraging
• Investigators appropriately plan to continue this approach as a phase III trial
• The hope that this regimen would decrease toxicity compared to FU/platinum was not realized

E1201: An Eastern Cooperative Oncology Group (ECOG) randomized phase II trial of neoadjuvant
preoperative paclitaxel/cisplatin/RT or irinotecan/cisplatin/RT in endoscopy with ultrasound
(EUS) staged adenocarcinoma of the esophagus
L. Kleinberg, M. E. Powell, A. Forastiere, S. Keller, P. Anne, A. B. Benson

Trial Parameters• Adenocarcinoma• T2-3N0M0, T1-3N1M0, T1-3N0M1a
• Surgically resectable• ECOG PS 0-1• Trial objectives
– Path CR rate– Toxicity– Survival
• 47 pts per arm• 45% path CR rate worthy of further study

Paclitaxel/Cisplatin
• Neoadjuvant– Paclitaxel 50 mg/m2 (1 hr) d1, 8, 15, 22, 29– Cisplatin 30 mg/m2 d1, 8, 15, 22, 29
• RT- 45 Gy• Surgery- 1 field nodal dissection• Adjuvant
– 3 cycles– Paclitaxel 175 mg/m2 and Cisplatin 75 mg/m2 on day 1

Chemotherapy: CPT-11/Cisplatin
• Neoadjuvant– CPT-11 65 mg/m2 day 1, 8, 22, 29– Cisplatin 30 mg/m2 day 1, 8, 22, 29
• RT- 45 Gy• Surgery- 1 field nodal dissection• Adjuvant
– 3 cycles– CPT-11 65 mg/m2 and Cisplatin 30 mg/m2 on day 1
and 8

Outcome
Surgery
% of all patients
R0
Resection
% of all patients
pCR of % of all patients
pCR of all going to surgery
CPT11
Cisplatin
(N=46)
89% 83% 15% 16%
Paclitaxel/
Cisplatin
(N=44)
82% 70% 16% 19%

DISCUSSION
• Regimens had complete response rates less than 20%
• Pretreatment EUS staging did not influence response to therapy
• Toxicity of both regimens similar and not superior to 5FU/platinum regimens
• 50% of patients received all planned chemotherapy
• Follow-up for survival outcome continues

DISCUSSION
• FU/cisplatin has still not been displaced as the standard chemotherapy with RT in esophageal cancer– Phase II study with FOLFOX is encouraging and is
being pursued
• Radiation therapy with concurrent chemotherapy is an option instead of surgery – Need to remember the risk of increased local failure
even if survival is no different

DISCUSSION
• Radiation delivery system does matter– Standard fractionation (180-200 cGy/fx) should
be used except in a clinical trial
• It may be possible to use much less aggressive therapy in patients with very early disease– These patients are rarely seen in the US– Specialized techniques and lack of expertise
may make the use of EMR difficult