Embed Size (px)
Citation preview

GlucocorticoidFrom Wikipedia, the free encyclopediaJump to: navigation, search
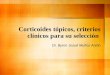
Chemical structure of cortisol, a glucocorticoid
Dexamethasone binds more powerfully to the glucocorticoid receptor than cortisol does. Dexamethasone is based on the cortisol structure but differs in three positions (extra double bond in the A-ring between carbons 1 and 2 and addition of a 9-α-fluoro group and a 16-α-methyl substituent).
Glucocorticoids (GC) are a class of steroid hormones that bind to the glucocorticoid receptor (GR), which is present in almost every vertebrate animal cell. The name glucocorticoid (pertaining to glucose + cortex ) derives from its role in the regulation of the metabolism of glucose, its synthesis in the adrenal cortex, and its steroidal structure (see structure to the right).
GCs are part of the feedback mechanism in the immune system that turns immune activity (inflammation) down. They are therefore used in medicine to treat diseases caused by an overactive immune system, such as allergies, asthma, autoimmune diseases and sepsis. GCs have many diverse (pleiotropic) effects, including potentially harmful side effects, and as a result are rarely sold over the counter.[1] They also interfere with some of the abnormal mechanisms in cancer cells, so they are used in high doses to treat cancer. This includes mainly inhibitory effects on lymphocyte proliferation (treatment of lymphomas and leukaemias) and mitigation of side effects of anticancer drugs.
GCs cause their effects by binding to the glucocorticoid receptor (GR). The activated GR complex, in turn, up-regulates the expression of anti-inflammatory proteins in the nucleus (a

process known as transactivation) and represses the expression of proinflammatory proteins in the cytosol by preventing the translocation of other transcription factors from the cytosol into the nucleus (transrepression).[1]
Glucocorticoids are distinguished from mineralocorticoids and sex steroids by their specific receptors, target cells, and effects. In technical terms, "corticosteroid" refers to both glucocorticoids and mineralocorticoids (as both are mimics of hormones produced by the adrenal cortex), but is often used as a synonym for "glucocorticoid".
Cortisol (or hydrocortisone) is the most important human glucocorticoid. It is essential for life, and it regulates or supports a variety of important cardiovascular, metabolic, immunologic, and homeostatic functions. Various synthetic glucocorticoids are available; these are used either as replacement therapy in glucocorticoid deficiency or to suppress the immune system.
Contents
[hide]
1 Effects o 1.1 Immune o 1.2 Metabolic o 1.3 Developmental o 1.4 Arousal and cognition o 1.5 Body fluid homeostasis
2 Mechanism of action o 2.1 Transactivation o 2.2 Transrepression o 2.3 Dissociation o 2.4 Nongenomic o 2.5 Glucocorticoid-induced neutrophilia o 2.6 Glucocorticoid-induced diuresis
3 Pharmacology 4 Therapeutic use
o 4.1 Physiological replacement o 4.2 Therapeutic immunosuppression o 4.3 Anti-inflammatory o 4.4 Hyperaldosteronism o 4.5 Resistance o 4.6 Heart failure
5 Side effects o 5.1 Immunodeficiency o 5.2 Withdrawal
6 Chemical synthesis 7 See also 8 References 9 External links

[edit] Effects
Steroidogenesis showing glucocorticoids in green ellipse at right - it is not a strictly bounded group, but a continuum of structures with increasing glucocorticoid effect, with the primary example being cortisol.
Glucocorticoid effects may be broadly classified into two major categories: immunological and metabolic. In addition, glucocorticoids play important roles in fetal development and body fluid homeostasis.
[edit] Immune
As discussed in more detail below, glucocorticoids function through interaction with the glucocorticoid receptor:
up-regulate the expression of anti-inflammatory proteins. down-regulate the expression of proinflammatory proteins.
Glucocorticoids are also shown to play a role in the development and homeostasis of T lymphocytes. This has been shown in transgenic mice with either increased or decreased sensitivity of T cell lineage to glucocorticoids.[2]
[edit] Metabolic
The name "glucocorticoid" derives from early observations that these hormones were involved in glucose metabolism. In the fasted state, cortisol stimulates several processes that collectively serve to increase and maintain normal concentrations of glucose in blood.
Metabolic effects:

Stimulation of gluconeogenesis, in particular, in the liver: This pathway results in the synthesis of glucose from nonhexose substrates, such as amino acids and glycerol from triglyceride breakdown, and is particularly important in carnivores and certain herbivores. Enhancing the expression of enzymes involved in gluconeogenesis is probably the best-known metabolic function of glucocorticoids.
Mobilization of amino acids from extrahepatic tissues: These serve as substrates for gluconeogenesis.
Inhibition of glucose uptake in muscle and adipose tissue: A mechanism to conserve glucose
Stimulation of fat breakdown in adipose tissue: The fatty acids released by lipolysis are used for production of energy in tissues like muscle, and the released glycerol provide another substrate for gluconeogenesis.
Excessive glucocorticoid levels resulting from administration as a drug or hyperadrenocorticism have effects on many systems. Some examples include inhibition of bone formation, suppression of calcium absorption (both of which can lead to osteoporosis), delayed wound healing, muscle weakness, and increased risk of infection. These observations suggest a multitude of less-dramatic physiologic roles for glucocorticoids.[2]
[edit] Developmental
Glucocorticoids have multiple effects on fetal development. An important example is their role in promoting maturation of the lung and production of the surfactant necessary for extrauterine lung function. Mice with homozygous disruptions in the corticotropin-releasing hormone gene (see below) die at birth due to pulmonary immaturity. In addition, glucocorticoids are necessary for normal brain development, by initiating terminal maturation, remodeling axons and dendrites, and affecting cell survival.[3]
[edit] Arousal and cognition
A graphical representation of the Yerkes-Dodson curve
Glucocorticoids act on the hippocampus, amygdala, and frontal lobes. Along with adrenaline, these enhance the formation of flashbulb memories of events associated with strong emotions, both positive and negative.[4] This has been confirmed in studies, whereby blockade of either glucocorticoids or noradrenaline activity impaired the recall of emotionally relevant information. Additional sources have shown subjects whose fear learning was accompanied by high cortisol levels had better consolidation of this memory (this effect was more important in men). Glucocorticoids have also been shown to have a significant impact on

vigilance and cognitive performance. This appears to follow the Yerkes-Dodson curve, as studies have shown circulating levels of glucocorticoids vs. memory performance follow an upside-down U pattern, much like the Yerkes-Dodson curve. For example, long-term potentiation (the process of forming long-term memories) is optimal when glucocorticoid levels are mildly elevated, whereas significant decreases of LTP are observed after adrenalectomy (low-GC state) or after exogenous glucocorticoid administration (high-GC state). Elevated levels of glucocorticoids enhance memory for emotionally arousing events, but lead more often than not to poor memory for material unrelated to the source of stress/emotional arousal.[5] In contrast to the dose-dependent enhancing effects of glucocorticoids on memory consolidation, these stress hormones have been shown to inhibit the retrieval of already stored information.[6][7]
[edit] Body fluid homeostasis
Glucocorticoids could act centrally, as well as peripherally, to assist in the normalization of extracellular fluid volume by regulating body’s action to atrial natriuretic peptide (ANP). Centrally, glucocorticoids could inhibit dehydration induced water intake;[8] peripherally, glucocorticoids could induce a potent diuresis.[9] The overall effect of glucocorticoids is to keep the body from volume overload.
[edit] Mechanism of action
[edit] Transactivation
Glucocorticoids bind to the cytosolic glucocorticoid receptor (GR). This type of receptor is activated by ligand binding. After a hormone binds to the corresponding receptor, the newly formed receptor-ligand complex translocates itself into the cell nucleus, where it binds to glucocorticoid response elements (GRE) in the promoter region of the target genes resulting in the regulation of gene expression. This process is commonly referred to as transactivation.[10]
The proteins encoded by these up-regulated genes have a wide range of effects, including, for example:[10]
anti-inflammatory – lipocortin I, p11/calpactin binding protein and secretory leukoprotease inhibitor 1 (SLPI)
increased gluconeogenesis – glucose-6-phosphatase and tyrosine aminotransferase
[edit] Transrepression
The opposite mechanism is called transrepression. The activated hormone receptor interacts with specific transcription factors (such as AP-1 and NF-κB) and prevents the transcription of targeted genes. Glucocorticoids are able to prevent the transcription of proinflammatory genes, including interleukins IL-1B, IL-4, IL-5, and IL-8, chemokines, cytokines, GM-CSF, and TNFA genes.[10]
[edit] Dissociation

The ordinary glucocorticoids do not distinguish among transactivation and transrepression and influence both the "wanted" immune and the "unwanted" genes regulating the metabolic and cardiovascular functions. Intensive research is aimed at discovering selectively acting glucocorticoids that will be able to repress only the immune system.[11][12]
Genetically modified mice that express a modified GR incapable of DNA binding are still responsive to the anti-inflammatory effects of glucocorticoids, while the stimulation of gluconeogenesis by glucocorticoids is blocked.[13] This result strongly suggests most of the desirable anti-inflammatory effects are due to transrepression, while the undesirable metabolic effects arise from transactivation, a hypothesis also underlying the development of selective glucocorticoid receptor agonists.
[edit] Nongenomic
Glucocorticoids have been shown to exert a number of rapid actions that are independent of the regulations of gene transcription. Binding of corticosteroids to the glucocorticoid receptor (GR) stimulates phosphatidylinositol 3-kinase and protein kinase AKT, leading to endothelial nitric oxide synthase (eNOS) activation and nitric oxide-dependent vasorelaxation.[14] Membrane associated GR has been shown to mediate lymphocytolysis.[15][16][17] In addition, some glucocorticoids have been shown to rapidly inhibit the release of the inflammatory prostaglandin PGE2, this effect is blocked by the glucocorticoid receptor antagonist mifepristone (RU-486) and is not affected by protein synthesis inhibitors. These data together suggest a nongenomic mechanism of action.[18][19]
[edit] Glucocorticoid-induced neutrophilia
Acute or chronic administration of corticosteroids causes neutrophilia,[20] suggesting the enhanced release of PMNs from the bone marrow is an important mechanism of the glucocorticoid-induced granulocytosis. An alternative mechanism for the granulocytosis induced by glucocorticoids is an influx of PMNs from the intravascular marginated PMN pools.[21] The response is caused by a shift of cells from the marginal to the circulating pool; hence, it frequently is referred to as demargination.[22]
Some of the immunosuppressive effects of glucocorticoids are mediated by nongenomic signalling involving the glucocortiocid receptor (GR). A multiprotein complex composed of the unliganded glucocorticoid receptor, Hsp90, and the tyrosine kinases LCK and FYN is recruited to the antigen-activated T cell receptor (TCR) in T cells. This GR complex is necessary for TCR signalling. On binding of glucocorticoids to GR, this complex dissociates, thus blocking TCR signalling.[23]
[edit] Glucocorticoid-induced diuresis
Glucocorticoids could mediate the gene expression of ANP and its primary receptor, natriuretic peptide receptor A (NPR-A). It is well documented that glucocorticoids could up-regulate the expression of ANP gene in the cardiomyocytes in vitro and stimulated ANP release in vivo without negative effects on renal sodium and water excretion.[24][25] Additionally, glucocorticoids could up-regulate NPR-A expression in the kidney and hypothalamus. In the kidney, glucocorticoids improve renal responsiveness to ANP by upregulating NPR-A expression in the renal inner medullary collecting duct, inducing a potent diuresis.[9] In hypothalamus, glucocorticoids inhibited dehydration or angiotensin II

induced water intake by potentiating hypothalamic response to ANP.[8] They work in concert to keep the body fluid volume in homeostasis.
[edit] Pharmacology
A variety of synthetic glucocorticoids, some far more potent than cortisol, have been created for therapeutic use. They differ in both pharmacokinetics (absorption factor, half-life, volume of distribution, clearance) and pharmacodynamics (for example the capacity of mineralocorticoid activity: retention of sodium (Na+) and water; renal physiology). Because they permeate the intestines easily, they are administered primarily per os (by mouth), but also by other methods, such as topically on skin. More than 90% of them bind different plasma proteins, though with a different binding specificity. Endogenous glucocorticoids and some synthetic corticoids have high affinity to the protein transcortin (also called corticosteroid-binding globulin), whereas all of them bind albumin. In the liver, they quickly metabolize by conjugation with a sulfate or glucuronic acid, and are secreted in the urine.
Glucocorticoid potency, duration of effect, and overlapping mineralocorticoid potency varies. Cortisol (hydrocortisone) is the standard of comparison for glucocorticoid potency. Hydrocortisone is the name used for pharmaceutical preparations of cortisol. Data refer to oral dosing, except when mentioned. Oral potency may be less than parenteral potency because significant amounts (up to 50% in some cases) may not be absorbed from the intestine. Fludrocortisone, DOCA (Deoxycorticosterone acetate), and aldosterone are, by definition, not considered glucocorticoids, although they may have minor glucocorticoid potency, and are included in this table to provide perspective on mineralocorticoid potency.
Comparative steroid potencies [26] [27]
NameGlucocorticoid potency
Mineralocorticoid potency
Duration of action (t1/2 in hours)
Hydrocortisone (cortisol) 1 1 8
Cortisone 0.8 0.8oral 8, intramuscular 18+
Prednisone 3.5-5 0.8 16-36
Prednisolone 4 0.8 16-36
Methylprednisolone 5-7.5 0.5 18-40
Dexamethasone 25-80 0 36-54
Betamethasone 25-30 0 36-54
Triamcinolone 5 0 12-36
Beclometasone
8 puffs 4 times a dayequals 14 mg oralprednisone once a day[clarification needed]
- -
Fludrocortisone acetate 15 200 24
Deoxycorticosterone acetate (DOCA)
0 20 -

Aldosterone 0.3 200-1000 -
[edit] Therapeutic use
Glucocorticoids may be used in low doses in adrenal insufficiency. In much higher doses, oral or inhaled glucocorticoids are used to suppress various allergic, inflammatory, and autoimmune disorders. Inhaled glucocorticoids are the second-line treatment for asthma. They are also administered as post-transplantory immunosuppressants to prevent the acute transplant rejection and the graft-versus-host disease. Nevertheless, they do not prevent an infection and also inhibit later reparative processes. Newly emerging evidence showed that glucocorticoids could be used in the treatment of heart failure to increase the renal responsiveness to diuretics and natriuretic peptides.
[edit] Physiological replacement
Any glucocorticoid can be given in a dose that provides approximately the same glucocorticoid effects as normal cortisol production; this is referred to as physiologic, replacement, or maintenance dosing. This is approximately 6–12 mg/m²/day (m² refers to body surface area (BSA), and is a measure of body size; an average man's BSA is 1.7 m²).
[edit] Therapeutic immunosuppression
See section on "Immunodeficiency" below for adverse effects
Glucocorticoids cause immunosuppression, and the therapeutic component of this effect is mainly the decreases in the function and numbers of lymphocytes, including both B cells and T cells.
The major mechanism for this immunosuppression through inhibition of nuclear factor kappa-light-chain-enhancer of activated B cells(NF-κB). NF-κB is a critical transcription factor involved in the synthesis of many mediators (i.e., cytokines) and proteins (i.e., adhesion proteins) that promote the immune response. Inhibition of this transcription factor, therefore, blunts the capacity of the immune system to mount a response.[1]
Glucocorticoids suppress cell-mediated immunity by inhibiting genes that code for the cytokines IL-1, IL-2, IL-3, IL-4, IL-5, IL-6, IL-8 and IFN-γ, the most important of which is IL-2. Smaller cytokine production reduces the T cell proliferation.[28]
Glucocorticoids, however, not only reduce T cell proliferation, but also lead to another well known effect - glucocorticoid-induced apoptosis. The effect is more prominent in immature T cells still inside in the thymus, but peripheral T cells are also affected. The exact mechanism underlying this glucocorticoid sensitivity still remains to be elucidated.[citation needed]
Glucocorticoids also suppress the humoral immunity, thereby causing a humoral immune deficiency. Glucocorticoids cause B cells to express smaller amounts of IL-2 and of IL-2 receptors. This diminishes both B cell clone expansion and antibody synthesis. The diminished amounts of IL-2 also cause fewer T lymphocyte cells to be activated.

Since glucocorticoid is a steroid, it regulates transcription factors; another factor it down-regulates is the expression of Fc receptors on macrophages, so there is a decreased phagocytosis of opsonised cells.[citation needed]
[edit] Anti-inflammatory
Glucocorticoids are potent anti-inflammatories, regardless of the inflammation's cause; their primary anti-inflammatory mechanism is lipocortin-1 (annexin-1) synthesis. Lipocortin-1 both suppresses phospholipase A2, thereby blocking eicosanoid production, and inhibits various leukocyte inflammatory events (epithelial adhesion, emigration, chemotaxis, phagocytosis, respiratory burst, etc.). In other words, glucocorticoids not only suppress immune response, but also inhibit the two main products of inflammation, prostaglandins and leukotrienes. They inhibit prostaglandin synthesis at the level of phospholipase A2 as well as at the level of cyclooxygenase/PGE isomerase (COX-1 and COX-2),[29] the latter effect being much like that of NSAIDs, potentiating the anti-inflammatory effect.
In addition, glucocorticoids also suppress cyclooxygenase expression.
Glucocorticoids marketed as anti-inflammatories are often topical formulations, such as nasal sprays for rhinitis or inhalers for asthma. These preparations have the advantage of only affecting the targeted area, thereby reducing side effects or potential interactions. In this case, the main compounds used are beclometasone, budesonide, fluticasone, mometasone and ciclesonide. In rhinitis, sprays are used. For asthma, glucocorticoids are administered as inhalants with a metered-dose or dry powder inhaler.[30]
[edit] Hyperaldosteronism
Glucocorticoids can be used in the management of familial hyperaldosteronism type 1. They are not effective, however, for use in the type 2 condition.
[edit] Resistance
Resistance to the therapeutic uses of glucocorticoids can present difficulty; for instance, 25% of cases of severe asthma may be unresponsive to steroids. This may be the result of genetic predisposition, ongoing exposure to the cause of the inflammation (such as allergens), immunological phenomena that bypass glucocorticoids, and pharmacokinetic disturbances (incomplete absorption or accelerated excretion or metabolism).[28]
[edit] Heart failure
Glucocorticoids could be used in the treatment of decompensated heart failure to potentiate renal responsiveness to diuretics, especially in heart failure patients with refractory diuretic resistance with large dose of loop diuretics.[31][32][33][34][35][36][37]
[edit] Side effects
Glucocorticoid drugs currently being used act nonselectively, so in the long run they may impair many healthy anabolic processes. To prevent this, much research has been focused recently on the elaboration of selectively acting glucocorticoid drugs. Side effects include:

immunodeficiency (see separate section below) hyperglycemia due to increased gluconeogenesis, insulin resistance, and impaired
glucose tolerance ("steroid diabetes"); caution in those with diabetes mellitus increased skin fragility, easy bruising negative calcium balance due to reduced intestinal calcium absorption[38]
steroid-induced osteoporosis : reduced bone density (osteoporosis, osteonecrosis, higher fracture risk, slower fracture repair)
weight gain due to increased visceral and truncal fat deposition (central obesity) and appetite stimulation
adrenal insufficiency (if used for long time and stopped suddenly without a taper) muscle breakdown (proteolysis), weakness, reduced muscle mass and repair expansion of malar fat pads and dilation of small blood vessels in skin anovulation , irregularity of menstrual periods growth failure, delayed puberty increased plasma amino acids, increased urea formation, negative nitrogen balance excitatory effect on central nervous system (euphoria, psychosis) glaucoma due to increased cranial pressure cataracts
In high doses, hydrocortisone (cortisol) and those glucocorticoids with appreciable mineralocorticoid potency can exert a mineralocorticoid effect as well, although in physiologic doses this is prevented by rapid degradation of cortisol by 11β-hydroxysteroid dehydrogenase isoenzyme 2 (11β-HSD2) in mineralocorticoid target tissues. Mineralocorticoid effects can include salt and water retention, extracellular fluid volume expansion, hypertension, potassium depletion, and metabolic alkalosis.
The combination of clinical problems produced by prolonged, excess glucocorticoids, whether synthetic or endogenous, is termed Cushing's syndrome.
[edit] Immunodeficiency
Glucocorticoids cause immunosuppression, decreasing the function and/or numbers of neutrophils, lymphocytes (including both B cells and T cells), monocytes, macrophages, and the anatomical barrier function of the skin.[39] This suppression, if large enough, can cause manifestations of immunodeficiency, including T cell deficiency, humoral immune deficiency and neutropenia.
Main pathogens of concern in glucocorticoid-induced immunodeficiency:[39]
Bacteria
Enterobacteriaceae Legionella micdadei Listeria monocytogenes Mycobacterium tuberculosis Nontuberculous mycobacteria Nocardia asteroides Rhodococcus equi Salmonella species Staphylococcus aureus Streptococci
Fungi Aspergillus

Blastomyces Candida albicans and nonalbicans species Coccidioides immitis Cryptococcus neoformans Fusarium species Histoplasma capsulatum Penicillium marneffei Pseudallescheria boydii Zygomycosis
Viruses
Adenovirus Cytomegalovirus Herpes simplex virus Human papillomavirus Influenza /parainfluenza Respiratory syncytial virus Varicella zoster
Other
Cryptosporidiosis /lsospora belli Pneumocystis carinii Strongyloides stercoralis Toxoplasma gondii
[edit] Withdrawal
In addition to the effects listed above, use of high-dose steroids for more than a week begins to produce suppression of the patient's adrenal glands because the exogenous glucocorticoids suppress hypothalamic corticotropin-releasing hormone and pituitary adrenocorticotropic hormone. With prolonged suppression, the adrenal glands atrophy (physically shrink), and can take months to recover full function after discontinuation of the exogenous glucocorticoid.
During this recovery time, the patient is vulnerable to adrenal insufficiency during times of stress, such as illness. While suppressive dose and time for adrenal recovery vary widely, clinical guidelines have been devised to estimate potential adrenal suppression and recovery, to reduce risk to the patient. The following is one example, but many variations exist or may be appropriate in individual circumstances.[citation needed]
If patients have been receiving daily high doses for five days or less, they can be abruptly stopped (or reduced to physiologic replacement if patients are adrenal-deficient). Full adrenal recovery can be assumed to occur by a week afterward.
If high doses were used for six to 10 days, reduce to replacement dose immediately and taper over four more days. Adrenal recovery can be assumed to occur within two to four weeks of completion of steroids.
If high doses were used for 11–30 days, cut immediately to twice replacement, and then by 25% every four days. Stop entirely when dose is less than half of replacement. Full adrenal recovery should occur within one to three months of completion of withdrawal.

If high doses were used more than 30 days, cut dose immediately to twice replacement, and reduce by 25% each week until replacement is reached. Then change to oral hydrocortisone or cortisone as a single morning dose, and gradually decrease by 2.5 mg each week. When the morning dose is less than replacement, the return of normal basal adrenal function may be documented by checking 0800 cortisol levels prior to the morning dose; stop drugs when 0800 cortisol is 10 μg/dl. Predicting the time to full adrenal recovery after prolonged suppressive exogenous steroids is difficult; some people may take nearly a year.
Flare-up of the underlying condition for which steroids are given may require a more gradual taper than outlined above.
[edit] Chemical synthesis
Hogg, J. A.; Beal, P. F.; Nathan, A. H.; Lincoln, F. H.; Schneider, W. P.; Magerlein, B. J.; Hanze, A. R.; Jackson, R. W. (1955). Journal of the American Chemical Society 77 (16): 4436. doi:10.1021/ja01621a092.
[edit] See also
GITR (glucocorticoid-induced TNF receptor)

Glucocorticoid receptor Immunosuppressive drug Selective glucocorticoid receptor agonist (SEGRA) Topical steroid Aminoglutethimide blocks GC secretion Metyrapone blocks GC secretion
[edit] References
1. ^ a b c Rhen T, Cidlowski JA (October 2005). "Antiinflammatory action of glucocorticoids--new mechanisms for old drugs". N. Engl. J. Med. 353 (16): 1711–23. doi:10.1056/NEJMra050541. PMID 16236742.
2. ^ a b Pazirandeh A, Xue Y, Prestegaard T, Jondal M, Okret S (May 2002). "Effects of altered glucocorticoid sensitivity in the T cell lineage on thymocyte and T cell homeostasis". FASEB J. 16 (7): 727–9. doi:10.1096/fj.01-0891fje. PMID 11923224.
3. ̂ Lupien JS, et al. (June 2009). "Effects of stress throughout the lifespan on the brain, behaviour and cognition". Nature Reviews Neuroscience 10 (6): 434–445. doi:10.1038/nrn2639. PMID 19401723.
4. ̂ Cahill, L., McGaugh, J. L. (1998). "Mechanisms of emotional arousal and lasting declarative memory". Trends in Neuroscience 21 (7): 294–299. doi:10.1016/S0166-2236(97)01214-9. PMID 9683321.
5. ̂ Lupien, S. J., Maheu, F., Tu, M.,Fiocco, A., Schramek, T.E. (2007). "The effects of stress and stress hormones on human cognition: Implications for the field of brain and cognition". Brain and Cognition 65 (3): 209–237. doi:10.1016/j.bandc.2007.02.007. PMID 17466428.
6. ̂ de Quervain, D et al., Stress and glucocorticoids impair retrieval of long-term spatial memory. Nature, 394, 787-790 (1998)
7. ̂ de Quervain, D et al., Acute cortisone administration impairs retrieval of long-term declarative memory in humans. Nature Neuroscience, 3, 313-314 (2000)
8. ^ a b Liu, C; Guan, J; Kang, Y; Xiu, H; Chen, Y; Deng, B; Liu, K (2010 Dec 20). "Inhibition of dehydration-induced water intake by glucocorticoids is associated with activation of hypothalamic natriuretic peptide receptor-A in rat.". PloS one 5 (12): e15607. PMID 21187974.
9. ^ a b Liu, C; Chen, Y; Kang, Y; Ni, Z; Xiu, H; Guan, J; Liu, K (2011 Oct). "Glucocorticoids improve renal responsiveness to atrial natriuretic peptide by up-regulating natriuretic peptide receptor-A expression in the renal inner medullary collecting duct in decompensated heart failure.". The Journal of pharmacology and experimental therapeutics 339 (1): 203–9. PMID 21737535.
10. ^ a b c Newton R (July 2000). "Molecular mechanisms of glucocorticoid action: what is important?". Thorax 55 (7): 603–13. doi:10.1136/thorax.55.7.603. PMC 1745805. PMID 10856322. //www.ncbi.nlm.nih.gov/pmc/articles/PMC1745805/.
11. ̂ Schäcke H, Rehwinkel H, Asadullah K (May 2005). "Dissociated glucocorticoid receptor ligands: compounds with an improved therapeutic index". Curr Opin Investig Drugs 6 (5): 503–7. PMID 15912964.
12. ̂ Newton R, Holden NS (October 2007). "Separating transrepression and transactivation: a distressing divorce for the glucocorticoid receptor?". Mol. Pharmacol. 72 (4): 799–809. doi:10.1124/mol.107.038794. PMID 17622575.
13. ̂ Reichardt HM, Tronche F, Bauer A, Schütz G (2000). "Molecular genetic analysis of glucocorticoid signaling using the Cre/loxP system". Biol. Chem. 381 (9–10): 961–4. doi:10.1515/BC.2000.118. PMID 11076028.
14. ̂ Hafezi-Moghadam A, Simoncini T, Yang Z, Limbourg FP, Plumier JC, Rebsamen MC, Hsieh CM, Chui DS, Thomas KL, Prorock AJ, Laubach VE, Moskowitz MA, French BA, Ley K, Liao JK (May 2002). "Acute cardiovascular protective effects of corticosteroids are mediated by non-transcriptional activation of endothelial nitric oxide synthase". Nat. Med. 8 (5): 473–9. doi:10.1038/nm0502-473. PMC 2668717. PMID 11984591. //www.ncbi.nlm.nih.gov/pmc/articles/PMC2668717/.
15. ̂ Cato AC, Nestl A, Mink S (June 2002). "Rapid actions of steroid receptors in cellular signaling pathways". Sci. STKE 2002 (138): RE9. doi:10.1126/stke.2002.138.re9. PMID 12084906.
16. ̂ Gametchu B, Watson CS, Pasko D (August 1991). "Size and steroid-binding characterization of membrane-associated glucocorticoid receptor in S-49 lymphoma cells". Steroids 56 (8): 402–10. doi:10.1016/0039-128X(91)90028-T. PMID 1788858. http://linkinghub.elsevier.com/retrieve/pii/0039-128X(91)90028-T.

17. ̂ Gametchu B, Watson CS, Shih CC, Dashew B (August 1991). "Studies on the arrangement of glucocorticoid receptors in the plasma membrane of S-49 lymphoma cells". Steroids 56 (8): 411–9. doi:10.1016/0039-128X(91)90029-U. PMID 1788859. http://linkinghub.elsevier.com/retrieve/pii/0039-128X(91)90029-U.
18. ̂ Croxtall JD, van Hal PT, Choudhury Q, Gilroy DW, Flower RJ (January 2002). "Different glucocorticoids vary in their genomic and non-genomic mechanism of action in A549 cells". Br. J. Pharmacol. 135 (2): 511–9. doi:10.1038/sj.bjp.0704474. PMC 1573139. PMID 11815387. //www.ncbi.nlm.nih.gov/pmc/articles/PMC1573139/.
19. ̂ Revollo JR, Cidlowski JA (October 2009). "Mechanisms generating diversity in glucocorticoid receptor signaling". Ann. N. Y. Acad. Sci. 1179: 167–78. doi:10.1111/j.1749-6632.2009.04986.x. PMID 19906239.
20. ̂ http://emedicine.medscape.com/article/208576-overview#showall21. ̂ http://circ.ahajournals.org/content/98/21/2307.full.pdf+html22. ̂ Williams Hematology, 8ed, Ch.65, Neutropenia and Neutrophylia23. ̂ Löwenberg M, Verhaar AP, Bilderbeek J, Marle J, Buttgereit F, Peppelenbosch MP, van Deventer
SJ, Hommes DW (October 2006). "Glucocorticoids cause rapid dissociation of a T-cell-receptor-associated protein complex containing LCK and FYN". EMBO Rep. 7 (10): 1023–9. doi:10.1038/sj.embor.7400775. PMC 1618362. PMID 16888650. //www.ncbi.nlm.nih.gov/pmc/articles/PMC1618362/.
24. ̂ Gardner, DG; Gertz, BJ; Deschepper, CF; Kim, DY (1988 Oct). "Gene for the rat atrial natriuretic peptide is regulated by glucocorticoids in vitro.". The Journal of clinical investigation 82 (4): 1275–81. PMID 2971674.
25. ̂ Dananberg, J; Grekin, RJ (1992 Nov). "Corticoid regulation of atrial natriuretic factor secretion and gene expression.". The American journal of physiology 263 (5 Pt 2): H1377-81. PMID 1443192.
26. ̂ From Liapi and Chrousos (ref. 2); Chapter 14. Glucocorticoid Therapy and Adrenal Suppression; http://www.endotext.org/adrenal/adrenal14/adrenalframe14.htm
27. ̂ Leung DY, Hanifin JM, Charlesworth EN, et al. (September 1997). "Disease management of atopic dermatitis: a practice parameter". Ann. Allergy Asthma Immunol. 79 (3): 197–211. doi:10.1016/S1081-1206(10)63003-7. PMID 9305225. http://www.jcaai.readyportal.net/file_depot/0-10000000/20000-30000/27387/folder/63948/Atopic_Derm1997.pdf. Retrieved 2009-07-09.
28. ^ a b Leung DY, Bloom JW (January 2003). "Update on glucocorticoid action and resistance". J. Allergy Clin. Immunol. 111 (1): 3–22; quiz 23. doi:10.1067/mai.2003.97. PMID 12532089. http://www.jacionline.org/article/PIIS009167490291359X/fulltext.
29. ̂ Goppelt-Struebe M, Wolter D, Resch K (December 1989). "Glucocorticoids inhibit prostaglandin synthesis not only at the level of phospholipase A2 but also at the level of cyclo-oxygenase/PGE isomerase". Br. J. Pharmacol. 98 (4): 1287–95. PMC 1854794. PMID 2514948. //www.ncbi.nlm.nih.gov/pmc/articles/PMC1854794/.
30. ̂ Rod Flower; Humphrey P. Rang; Maureen M. Dale; Ritter, James M. (2007). Rang & Dale's pharmacology. Edinburgh: Churchill Livingstone. ISBN 0-443-06911-5.
31. ̂ RADO, JP; BLUMENFELD, G; HAMMER, S (1959 Nov). "The effect of prednisone and 6-methylprednisolone on mercurial diuresis in patients with refractory cardiac edema.". The American journal of the medical sciences 238: 542–51. PMID 14435747.
32. ̂ RIEMER, AD (1958 Apr). "Application of the newer corticosteroids to augment diuresis in congestive heart failure.". The American journal of cardiology 1 (4): 488–96. PMID 13520608.
33. ̂ NEWMAN, DA (1959 Feb 15). "Reversal of intractable cardiac edema with prednisone.". New York state journal of medicine 59 (4): 625–33. PMID 13632954.
34. ̂ Zhang, H; Liu, C; Ji, Z; Liu, G; Zhao, Q; Ao, YG; Wang, L; Deng, B; Zhen, Y; Tian, L; Ji, L; Liu, K (2008 Sep). "Prednisone adding to usual care treatment for refractory decompensated congestive heart failure.". International heart journal 49 (5): 587–95. PMID 18971570.
35. ̂ Liu, C; Liu, G; Zhou, C; Ji, Z; Zhen, Y; Liu, K (2007 Sep). "Potent diuretic effects of prednisone in heart failure patients with refractory diuretic resistance.". The Canadian journal of cardiology 23 (11): 865–8. PMID 17876376.
36. ̂ Liu, C; Chen, H; Zhou, C; Ji, Z; Liu, G; Gao, Y; Tian, L; Yao, L; Zheng, Y; Zhao, Q; Liu, K (2006 Oct). "Potent potentiating diuretic effects of prednisone in congestive heart failure.". Journal of cardiovascular pharmacology 48 (4): 173–6. PMID 17086096.
37. ̂ Massari, F; Mastropasqua, F; Iacoviello, M; Nuzzolese, V; Torres, D; Parrinello, G (2012 Mar). "The glucocorticoid in acute decompensated heart failure: Dr Jekyll or Mr Hyde?". The American journal of emergency medicine 30 (3): 517.e5-10. PMID 21406321.
38. ̂ Gennari C (May 1993). "Differential effect of glucocorticoids on calcium absorption and bone mass". Br. J. Rheumatol. 32 Suppl 2: 11–4. ISSN 1462-0332. PMID 8495275.

Estrogen & the Immune System: Of mice and women (and nitric oxide)
Being female can be both an advantage and a disadvantage, immunologically speaking. It has long been
known that both innate and adaptive immune responses of females are somewhat more robust than
males. On the other hand, females are more susceptible to autoimmune disorders such as lupus,
rheumatoid arthritis, and multiple sclerosis. These gender differences are largely attributed to estrogen
levels.1,2 Estrogen-related regulation of nitric oxide (NO), and the enzymes that produce it, increasingly
appear to play a key role.1
NO synthases (NOS) catalyze the conversion of L-arginine to citrulline and NO. Macrophages, dendritic
cells (DCs), and NK cells produce both endothelial and inducible types, eNOS and iNOS, with iNOS
generating the highest NO levels.3 NO production is modulated by many mechanisms, including control of
arginases, iNOS induction, co-factors (FAD, FMN, heme, and calmodulin), calcium, dimerization, feedback
regulation, and protein stability.3 The actions of NO are also difficult to determine, since NO is a labile
and highly diffusible gas that takes many forms. However, among other reported actions, NO has
concentration-dependent anti-microbial, anti-inflammatory, and anti-apoptotic activities, and modulates
cytokine and chemokine production in specific cell types and settings.1,3,5
Recent data explain one way that estrogen stimulates NO production in mouse spleen.4 Estrogen
treatment in vivo allows profound NO production by isolated splenocytes, provided three conditions are
met. First, T cells need stimulation, for example by the T cell mitogen ConA or by CD3 antibodies.
Second, costimulation by an antigen-presenting cell is required, since CTLA-4 Ig blocks both the B7/CD28
interaction and NO production. Third, T cell production of IFN-gamma is required, since lack of NO
production by IFN-gamma-/- splenocytes is restored by exogenous IFN-gamma. Splenocytes from control
mice also produce IFN-gamma, iNOS, and NO when stimulated, but estrogen-treated mice require
considerably less stimulation. This may be a significant reason that the female immune system appears
to be “primed.”1

Figure 1. RANKL binding (shown in blue) promotes macrophage
osteoclast differentiation. The pathway from estrogen through IFN-
gamma, iNOS, and NO (shown in red) generates RANKL-blocking
osteoprotegerin (OPG) and down-regulates osteoclast formation.
Estrogen maintains the balance between bone deposition and resorption, an activity that also involves
NO (Figure 1).4,5 RANKL/TRANCE (the receptor activator of NFkB ligand) and M-CSF promote
differentiation of bone-resorbing osteoclasts (OC), while osteoprotegerin (OPG) acts as a dummy receptor
for RANKL, down-regulating OC formation and promoting bone-replenishing osteoblasts (OB). Both bone-
resorptive and retentive activities of IFN-gamma have been reported, and strong stimulation of T cells
has been proposed to tip the balance against resorption.5 NO produced by estrogen-stimulated bone
marrow cells decreases the OC/OB ratio primarily by activating the transcription factor RUNX2/CBFA1 to
induce OPG production.6,7 Differentiation of the RAW264.7 mouse macrophage cell line to OC can be
inhibited by co-culture with CD3e and CD28 antibody-activated T cells, an effect that is blocked by
neutralizing IFN-gamma.8 Interestingly, IFN-gamma, or IFN-beta induced by RANKL, promote iNOS
production and increases NO in OC-differentiating RAW cells, apparently as a self-limiting mechanism.9
Enhancement of IFN-gamma or other cytokines produced by costimulated T cells could well be involved
in the efficacy of estrogen replacement in preventing osteoporosis. The full role of IFN-gamma-stimulated
NO as a mediator of estrogen’s effects on the immune system is not yet clear. Other estrogen effects,
such as modulation of TNF-alpha, TGF-beta, and IL-1 activity in the bone marrow, and effects on B cells,
DCs, and CD4+CD25+ regulatory T cells involved in autoimmunity, are areas of active research.5,10
References
1. Verthelyi, D. (2006) Endocrinol. 147:659.
2. Carlsten, H. (2005) Immunol. Rev. 208:194.
3. Bogdan, C. (2001) Nat. Immunol. 2:907.
4. Karpuzoglu, E. et al. (2006) Endocrinol. 147:662.

5. Weitzmann, M. N. & R. Pacifici (2005) Immunol. Rev. 208:154.
6. O’Shaughnessy, M. T. et al. (2000) Biochem. Biophys. Res. Comm. 277:604.
7. Wang, F.-S. et al. (2004) Endocrinology 145:2148.
8. Wyzga, N. et al. (2004) Bone 35:614.
9. Zheng, H. et al. (2006) J. Biol. Chem. 281:15809.
10. Wood, K. J. et al. (2006) Trends Immunol. 27:183.
The Test
1. How is it used? 2. When is it ordered? 3. What does the test result mean? 4. Is there anything else I should know?
How is it used?
An indirect antiglobulin test (IAT) is used to screen an individual's blood for antibodies directed against red blood
cell (RBC) antigens other than the A and B antigens. It is performed as part of a "type and screen" whenever a
blood transfusion is anticipated. If an antibody is detected, then an antibody identification test must be done to
determine which antibodies are present. During a crossmatch, a variation of the IAT is performed if clinically
significant antibodies are present. In the case of blood transfusions, RBC antibodies must be taken into account
and donor blood must be found that does not contain the antigen(s) to which the person has produced
antibodies.
If someone has an immediate or delayed reaction to a blood transfusion, the doctor will order a direct antiglobulin
test (DAT) to help investigate the cause of the reaction. (The DAT detects RBC antibodies attached to red blood
cells.) An IAT will be performed to see if the affected person has developed any new antibodies if the DAT is
positive.
During pregnancy, the IAT is used to screen for antibodies in the blood of the mother that might cross the
placenta and attack the baby's red cells, causing hemolytic disease of the newborn (HDN). The most serious
cause is an antibody produced in response to the RBC antigen called the "D antigen" in the Rh blood group
system. A person is considered to be Rh-positive if the D antigen is present on their RBCs and Rh-negative if the
D antigen is not present. An Rh-negative mother may develop an antibody when she is exposed to blood cells
from an Rh-positive fetus. To prevent this, an Rh-negative mother should have an IAT performed early in her
pregnancy, at 28 weeks, and again at the time of delivery. If there are no Rh antibodies present at 28 weeks, then
the woman is given an injection of Rh immune globulin (RhIg) to clear any Rh-positive fetal RBCs that may be
present in her bloodstream to prevent the production of Rh antibodies by the mother.
At birth, the baby's Rh status is determined. If the baby is Rh-negative, then the mother does not require another
RhIg injection; if the baby is Rh-positive and the mother's antibody status is negative for anti-D, the mother is
given additional RhIG.

This test may be used to help diagnose autoimmune-related hemolytic anemia in conjunction with a DAT. This
condition may be caused when a person produces antibodies against their own RBC antigens. This can happen
with some autoimmune disorders, such as systemic lupus erythematosus, with diseases such as lymphoma or
chronic lymphocytic leukemia, and with infections such as mycoplasma pneumonia and mononucleosis. It can
also occur in some people with the use of certain medications, such as penicillin.
^ Back to top
When is it ordered?
An IAT is performed prior to any anticipated blood transfusion.
An IAT is performed as part of every woman's pregnancy workup. In Rh-negative women, it is also done
at 28 weeks, prior to giving an RhIg injection, and after delivery if the baby is found to be Rh-positive. In
negative pregnant women with known antibodies, the IAT is sometimes ordered as a monitoring tool to
roughly track the amount of antibody present.
^ Back to top
What does the test result mean?
If an IAT is positive, then one or more RBC antibodies are present. Some of these antibodies will be more
significant than others. When an IAT is used to screen prior to a blood transfusion, a positive IAT indicates the
need for an antibody identification test to identify the antibodies that are present. Once the antibody has been
identified, then donor blood must be found that does not contain the corresponding antigen(s) so that the
antibody will not react with and destroy donor RBC antigens following a blood transfusion.
If an Rh-negative mother has a negative IAT, then an Rh immune globulin injection is given within 72 hours to
prevent antibody production. If she has a positive IAT, then the antibody or antibodies present must be identified.
If an antibody to the D antigen has been actively formed by the mother, then the RhIg injection is not useful. If
she has a different antibody, then the RhIg injection can still be given to prevent her from producing antibodies to
the D antigen.
^ Back to top
Is there anything else I should know?
A circulating RBC antibody, once present, will never truly go away but may drop to undetectable levels. If the
person is exposed to the antigen again, production will kick quickly into gear and attack the RBCs so the antibody
will be honored (treated as though it is present) even when not detactable.
Each blood transfusion that a person has exposes them to the combination of antigens on the donor's RBCs.
Whenever the transfused RBCs contain antigens foreign to the recipient's RBCs, there is the potential to produce
an antibody. If someone has many blood transfusions over a period of time, they may produce antibodies against
many different antigens. This can make finding compatible blood increasingly difficult.