Embed Size (px)
Citation preview
LARS™Gluteal Tendon Repair and Reinforcement
Surgical technique
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 1 17/07/2014 09:17
Corin would like to thank Dr Greg Janes, Perth Orthopaedic and Sports Medicine Centre - Australia, for his contribution to this surgical technique.
ContentsGluteal tendon pathology 3
LARS™ overview 4
Material 4
General considerations 4
Graft options 4
Fixation 5
Indications 5
Contraindications 5
Surgical approach 5
Deep/complete gluteal lesions technique 6
Repair choice 6
A1. Identification of tendon involvement 6
A2. Tunnel placement and drilling 6
A3. Suturing of the LARS™ 7
A4. Fixation of LARS™ in the bone tunnel 8
A5. Completion of repair 8
Superficial/incomplete gluteal lesions technique 9
Repair choice 9
B1. Tunnel position and drilling 9
B2. Suturing of the tendon 10
B3. Suturing of the LARS™ 10
B4. Final fixation 10
Rehabilitation guidelines 11
Ordering information 11
References 12
2
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 2 17/07/2014 09:17

The next generation in soft tissue internal fixationLARS™
Greater trochanteric pain syndrome (GTPS) is a term used to describe chronic pain overlying the lateral and sometimes posterior aspect of the hip, previously described as trochanteric bursitis1.
The prevalence of unilateral GTPS is 15.0% in women and 8.5% in men, and that of bilateral GTPS is 6.6% in women and 1.9% in men2.
Recent improvements in the understanding of the pathology of GTPS have revealed that tears in the gluteal tendons are the most common cause of GTPS3,4. Gluteal tendon tears are similar in pathology to a rotator cuff tear in the shoulder5 and can be a result of traumatic injury, degenerative changes or total hip arthroplasty surgery6. Degenerate tears of the gluteal tendons were seen by Bunker et al5 in 22% of patients with intracapsular femoral neck fractures.
Whilst surgical repair of gluteal tendon tears by transosseous or bone anchor suture techniques report good pain relief7,8,9, high re-rupture rates of 11% at six months and 31% at twelve months8,9 indicate a more substantial repair construct may be required.
As a synthetic scaffold LARS™ (Ligament Augmentation & Reconstruction System) is designed to provide initial stability, allowing biological healing to take place, while eliminating post-operative elongation. The LARS™ ligament is used to reinforce primary suture and anchor based repairs, providing immediate strength and stability to the repair10.
Recent publications, including those by Bucher et al10 and Bajwa et al6, describe the use of a LARS™ synthetic ligament to reinforce the repair of gluteal tendon tears with significant improvements in patient outcomes.
Gluteal tendon pathology
3 |Responsible Innovation
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 3 17/07/2014 09:17
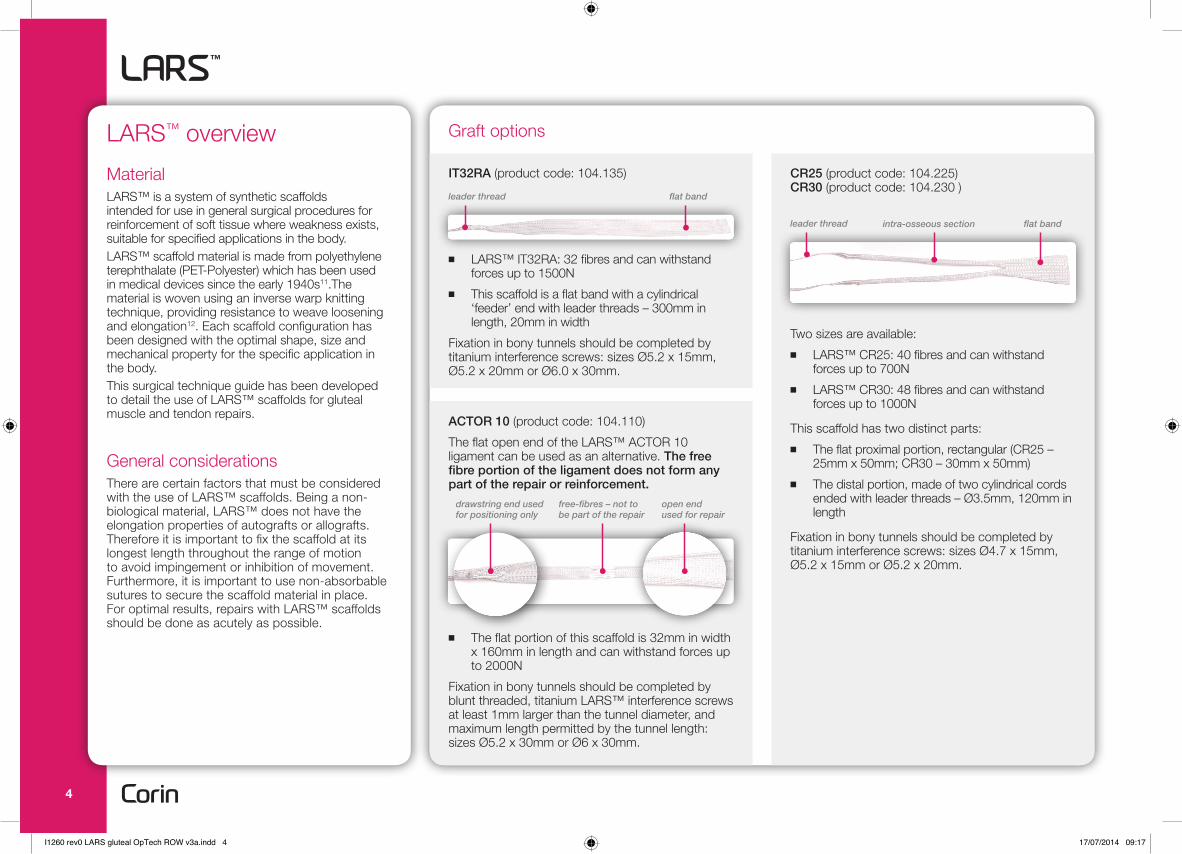
IT32RA (product code: 104.135)
■ LARS™ IT32RA: 32 fibres and can withstand forces up to 1500N
■ This scaffold is a flat band with a cylindrical ‘feeder’ end with leader threads – 300mm in length, 20mm in width
Fixation in bony tunnels should be completed by titanium interference screws: sizes Ø5.2 x 15mm, Ø5.2 x 20mm or Ø6.0 x 30mm.
ACTOR 10 (product code: 104.110)
The flat open end of the LARS™ ACTOR 10 ligament can be used as an alternative. The free fibre portion of the ligament does not form any part of the repair or reinforcement.
■ The flat portion of this scaffold is 32mm in width x 160mm in length and can withstand forces up to 2000N
Fixation in bony tunnels should be completed by blunt threaded, titanium LARS™ interference screws at least 1mm larger than the tunnel diameter, and maximum length permitted by the tunnel length: sizes Ø5.2 x 30mm or Ø6 x 30mm.
flat bandleader thread
LARS™ overview
MaterialLARS™ is a system of synthetic scaffolds intended for use in general surgical procedures for reinforcement of soft tissue where weakness exists, suitable for specified applications in the body. LARS™ scaffold material is made from polyethylene terephthalate (PET-Polyester) which has been used in medical devices since the early 1940s11.The material is woven using an inverse warp knitting technique, providing resistance to weave loosening and elongation12. Each scaffold configuration has been designed with the optimal shape, size and mechanical property for the specific application in the body.This surgical technique guide has been developed to detail the use of LARS™ scaffolds for gluteal muscle and tendon repairs.
General considerationsThere are certain factors that must be considered with the use of LARS™ scaffolds. Being a non-biological material, LARS™ does not have the elongation properties of autografts or allografts. Therefore it is important to fix the scaffold at its longest length throughout the range of motion to avoid impingement or inhibition of movement. Furthermore, it is important to use non-absorbable sutures to secure the scaffold material in place. For optimal results, repairs with LARS™ scaffolds should be done as acutely as possible.
Graft options
CR25 (product code: 104.225) CR30 (product code: 104.230 )
Two sizes are available: ■ LARS™ CR25: 40 fibres and can withstand
forces up to 700N ■ LARS™ CR30: 48 fibres and can withstand
forces up to 1000N
This scaffold has two distinct parts: ■ The flat proximal portion, rectangular (CR25 –
25mm x 50mm; CR30 – 30mm x 50mm) ■ The distal portion, made of two cylindrical cords
ended with leader threads – Ø3.5mm, 120mm in length
Fixation in bony tunnels should be completed by titanium interference screws: sizes Ø4.7 x 15mm, Ø5.2 x 15mm or Ø5.2 x 20mm.
flat bandleader thread intra-osseous section
free-fibres – not to be part of the repair
drawstring end used for positioning only
open end used for repair
4
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 4 17/07/2014 09:17
IndicationsLARS™ is indicated for the reinforcement of tears in the gluteus medius and minimus tendons in patients presenting with lateral hip pain, focal tenderness over the greater trochanter and tenderness on resisted abduction, and a positive FABERE (Flexion, ABduction, External Rotation, Extension) test. LARS™ can also be used in patients who have failed conservative treatment options and when the gluteal tendons are damaged during antero-lateral approach to total hip replacement surgery.
Diagnosis of gluteal tendon tears can be confirmed by MRI scan with 91% accuracy13.
In the context of gluteal tendon repairs, LARS™ should be used as reinforcement after direct suturing of the tear with non-resorbable sutures. If the tear cannot be sutured directly, then the tissue should be re-attached to the insertion point on the greater trochanter using transosseous or bone anchor suturing to ensure correct tensioning of the tissue prior to reinforcement with LARS™.
LARS™ acts as an internal splint to reinforce the repair and aid healing. In supporting the primary repair, the addition of the LARS™ ligament facilitates earlier mobilisation and rehabilitation by permitting immediate weight bearing as tolerated by the patient10,14 .
ContraindicationsLARS™ should not be used in patients with evidence of hip joint osteoarthritis, as evidenced by x-ray or MRI. The device is contraindicated for use in patients with:
■ Active or latent infection, ■ Decreased vascularity, ■ Pathologic soft tissue conditions that would
prevent secure fixation.
Fixation
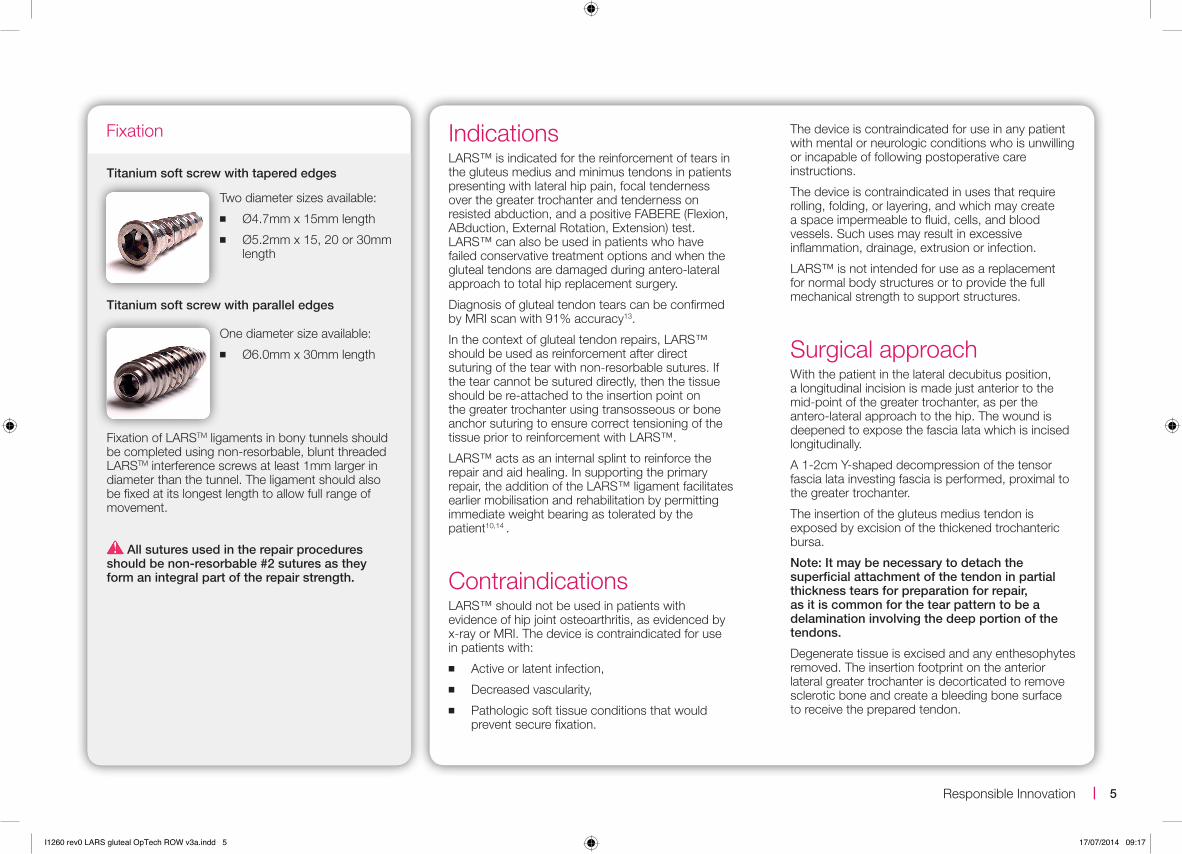
Titanium soft screw with tapered edges
Two diameter sizes available: ■ Ø4.7mm x 15mm length ■ Ø5.2mm x 15, 20 or 30mm
length
Titanium soft screw with parallel edges
One diameter size available: ■ Ø6.0mm x 30mm length
Fixation of LARSTM ligaments in bony tunnels should be completed using non-resorbable, blunt threaded LARSTM interference screws at least 1mm larger in diameter than the tunnel. The ligament should also be fixed at its longest length to allow full range of movement.
All sutures used in the repair procedures should be non-resorbable #2 sutures as they form an integral part of the repair strength.
The device is contraindicated for use in any patient with mental or neurologic conditions who is unwilling or incapable of following postoperative care instructions.
The device is contraindicated in uses that require rolling, folding, or layering, and which may create a space impermeable to fluid, cells, and blood vessels. Such uses may result in excessive inflammation, drainage, extrusion or infection.
LARS™ is not intended for use as a replacement for normal body structures or to provide the full mechanical strength to support structures.
Surgical approachWith the patient in the lateral decubitus position, a longitudinal incision is made just anterior to the mid-point of the greater trochanter, as per the antero-lateral approach to the hip. The wound is deepened to expose the fascia lata which is incised longitudinally.
A 1-2cm Y-shaped decompression of the tensor fascia lata investing fascia is performed, proximal to the greater trochanter.
The insertion of the gluteus medius tendon is exposed by excision of the thickened trochanteric bursa.
Note: It may be necessary to detach the superficial attachment of the tendon in partial thickness tears for preparation for repair, as it is common for the tear pattern to be a delamination involving the deep portion of the tendons.
Degenerate tissue is excised and any enthesophytes removed. The insertion footprint on the anterior lateral greater trochanter is decorticated to remove sclerotic bone and create a bleeding bone surface to receive the prepared tendon.
5 |Responsible Innovation
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 5 17/07/2014 09:17
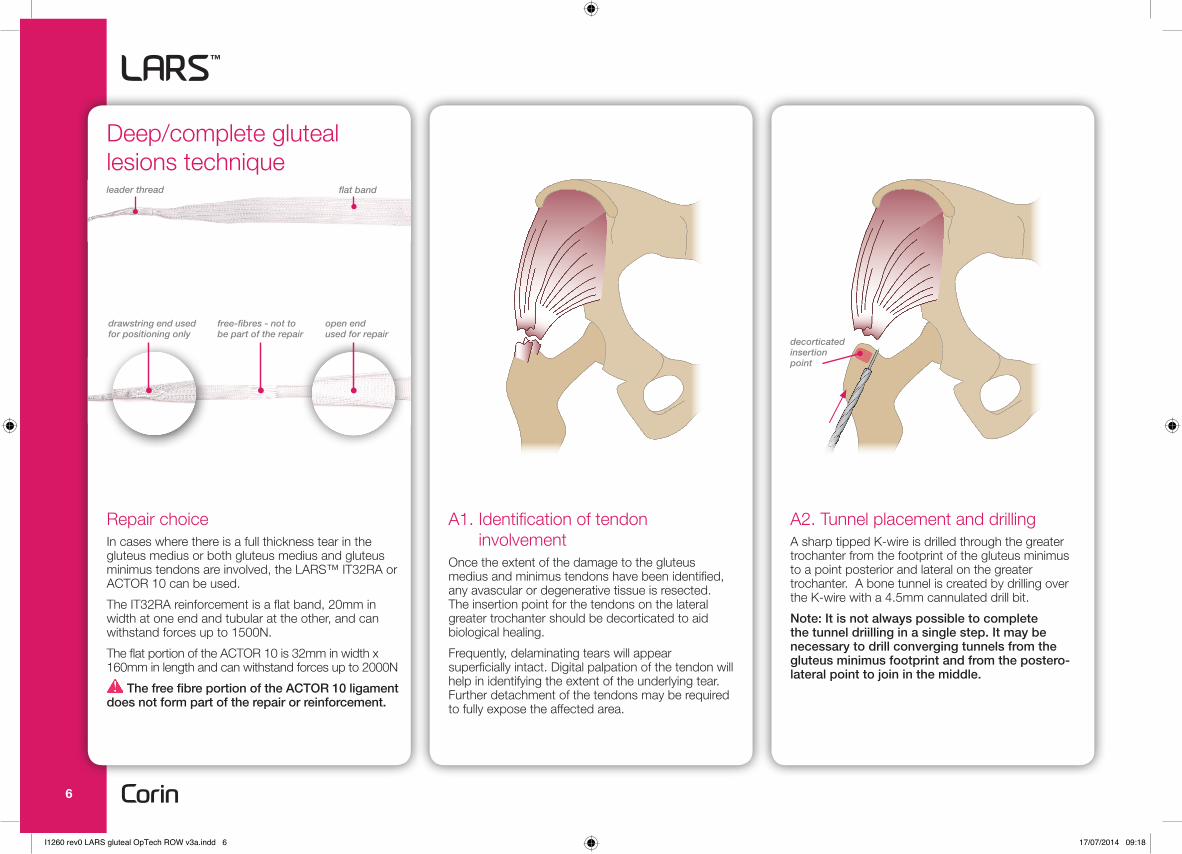
A2. Tunnel placement and drillingA sharp tipped K-wire is drilled through the greater trochanter from the footprint of the gluteus minimus to a point posterior and lateral on the greater trochanter. A bone tunnel is created by drilling over the K-wire with a 4.5mm cannulated drill bit.
Note: It is not always possible to complete the tunnel driilling in a single step. It may be necessary to drill converging tunnels from the gluteus minimus footprint and from the postero-lateral point to join in the middle.
A1. Identification of tendon involvement
Once the extent of the damage to the gluteus medius and minimus tendons have been identified, any avascular or degenerative tissue is resected. The insertion point for the tendons on the lateral greater trochanter should be decorticated to aid biological healing.
Frequently, delaminating tears will appear superficially intact. Digital palpation of the tendon will help in identifying the extent of the underlying tear. Further detachment of the tendons may be required to fully expose the affected area.
Repair choiceIn cases where there is a full thickness tear in the gluteus medius or both gluteus medius and gluteus minimus tendons are involved, the LARS™ IT32RA or ACTOR 10 can be used.
The IT32RA reinforcement is a flat band, 20mm in width at one end and tubular at the other, and can withstand forces up to 1500N.
The flat portion of the ACTOR 10 is 32mm in width x 160mm in length and can withstand forces up to 2000N
The free fibre portion of the ACTOR 10 ligament does not form part of the repair or reinforcement.
Deep/complete gluteal lesions technique
flat bandleader thread
decorticated insertion point
free-fibres - not to be part of the repair
drawstring end used for positioning only
open end used for repair
6
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 6 17/07/2014 09:18
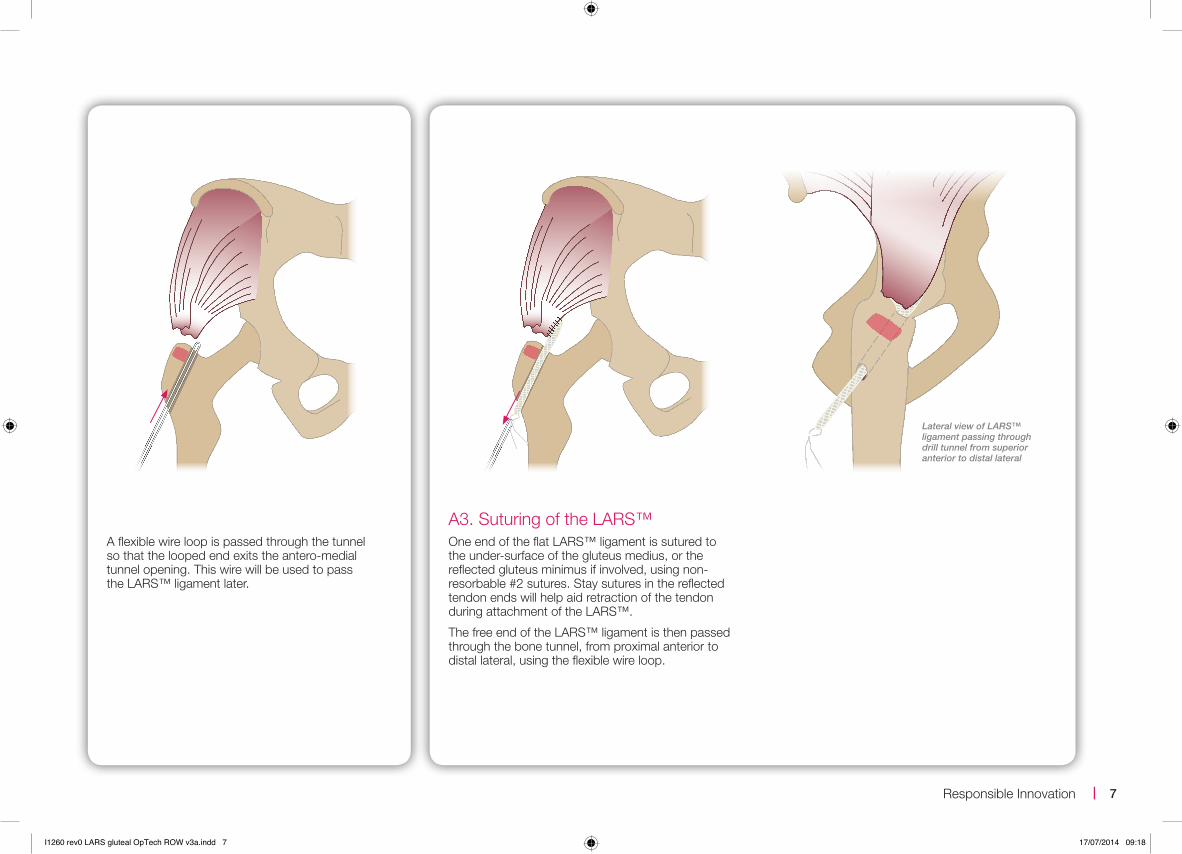
A3. Suturing of the LARS™One end of the flat LARS™ ligament is sutured to the under-surface of the gluteus medius, or the reflected gluteus minimus if involved, using non-resorbable #2 sutures. Stay sutures in the reflected tendon ends will help aid retraction of the tendon during attachment of the LARS™.
The free end of the LARS™ ligament is then passed through the bone tunnel, from proximal anterior to distal lateral, using the flexible wire loop.
A flexible wire loop is passed through the tunnel so that the looped end exits the antero-medial tunnel opening. This wire will be used to pass the LARS™ ligament later.
Lateral view of LARS™ ligament passing through drill tunnel from superior anterior to distal lateral
7 |Responsible Innovation
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 7 17/07/2014 09:18
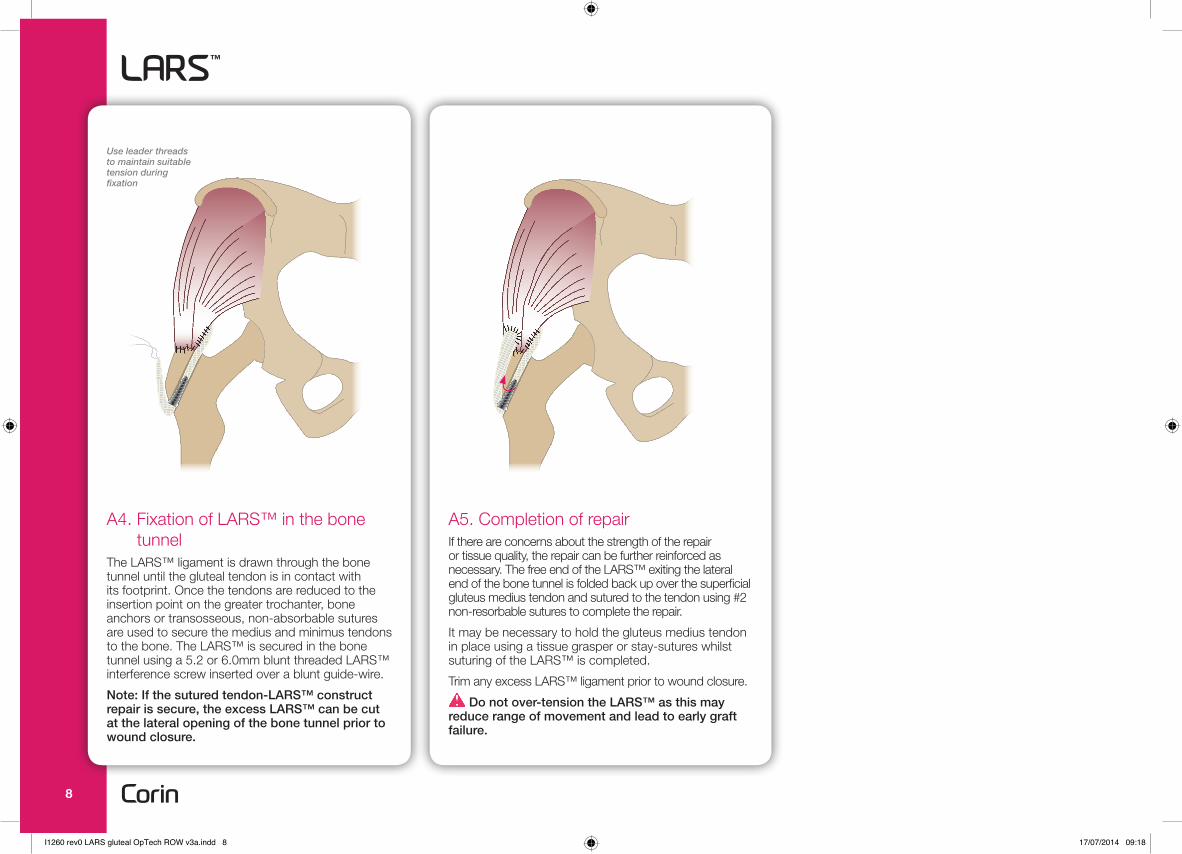
A5. Completion of repairIf there are concerns about the strength of the repair or tissue quality, the repair can be further reinforced as necessary. The free end of the LARS™ exiting the lateral end of the bone tunnel is folded back up over the superficial gluteus medius tendon and sutured to the tendon using #2 non-resorbable sutures to complete the repair.
It may be necessary to hold the gluteus medius tendon in place using a tissue grasper or stay-sutures whilst suturing of the LARS™ is completed.
Trim any excess LARS™ ligament prior to wound closure.
Do not over-tension the LARS™ as this may reduce range of movement and lead to early graft failure.
Use leader threads to maintain suitable tension during fixation
A4. Fixation of LARS™ in the bone tunnel
The LARS™ ligament is drawn through the bone tunnel until the gluteal tendon is in contact with its footprint. Once the tendons are reduced to the insertion point on the greater trochanter, bone anchors or transosseous, non-absorbable sutures are used to secure the medius and minimus tendons to the bone. The LARS™ is secured in the bone tunnel using a 5.2 or 6.0mm blunt threaded LARS™ interference screw inserted over a blunt guide-wire.
Note: If the sutured tendon-LARS™ construct repair is secure, the excess LARS™ can be cut at the lateral opening of the bone tunnel prior to wound closure.
8
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 8 17/07/2014 09:18
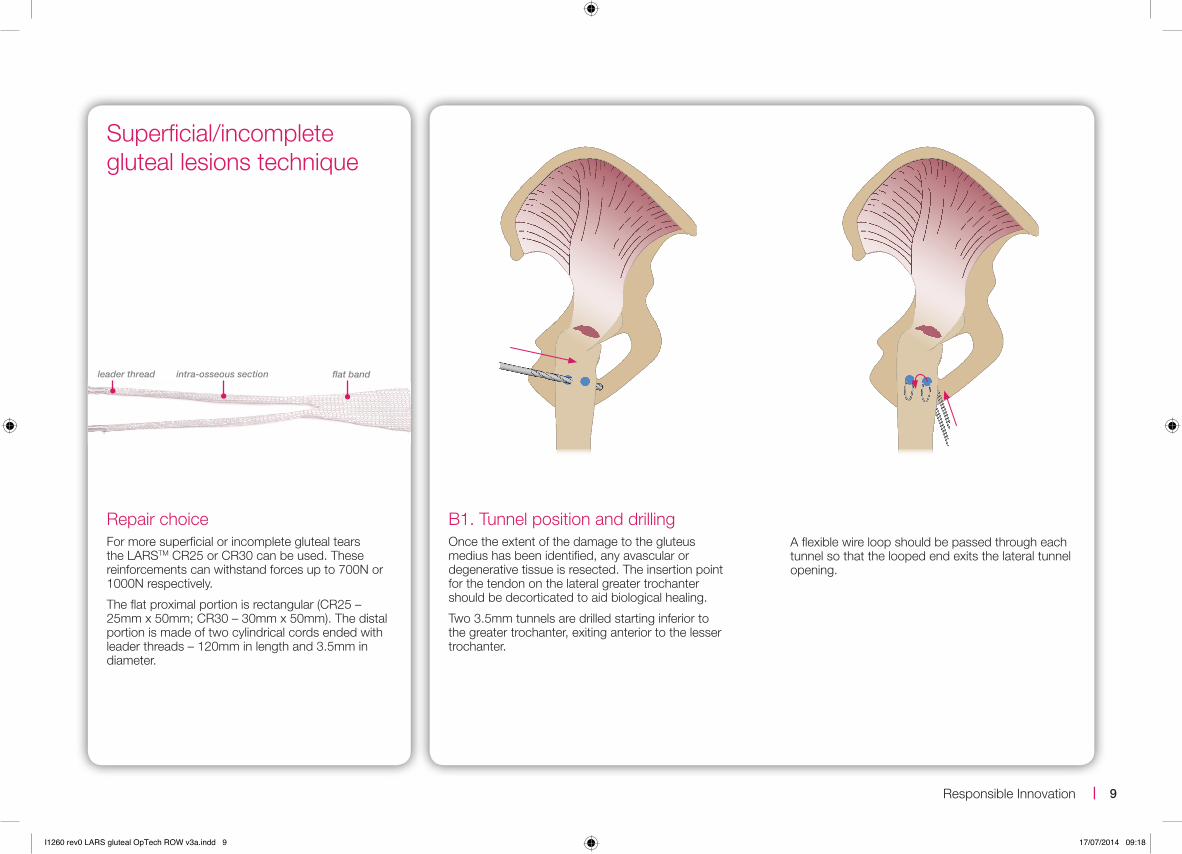
Repair choiceFor more superficial or incomplete gluteal tears the LARSTM CR25 or CR30 can be used. These reinforcements can withstand forces up to 700N or 1000N respectively.
The flat proximal portion is rectangular (CR25 – 25mm x 50mm; CR30 – 30mm x 50mm). The distal portion is made of two cylindrical cords ended with leader threads – 120mm in length and 3.5mm in diameter.
B1. Tunnel position and drillingOnce the extent of the damage to the gluteus medius has been identified, any avascular or degenerative tissue is resected. The insertion point for the tendon on the lateral greater trochanter should be decorticated to aid biological healing.
Two 3.5mm tunnels are drilled starting inferior to the greater trochanter, exiting anterior to the lesser trochanter.
Superficial/incomplete gluteal lesions technique
intra-osseous section flat bandleader thread
A flexible wire loop should be passed through each tunnel so that the looped end exits the lateral tunnel opening.
9 |Responsible Innovation
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 9 17/07/2014 09:18
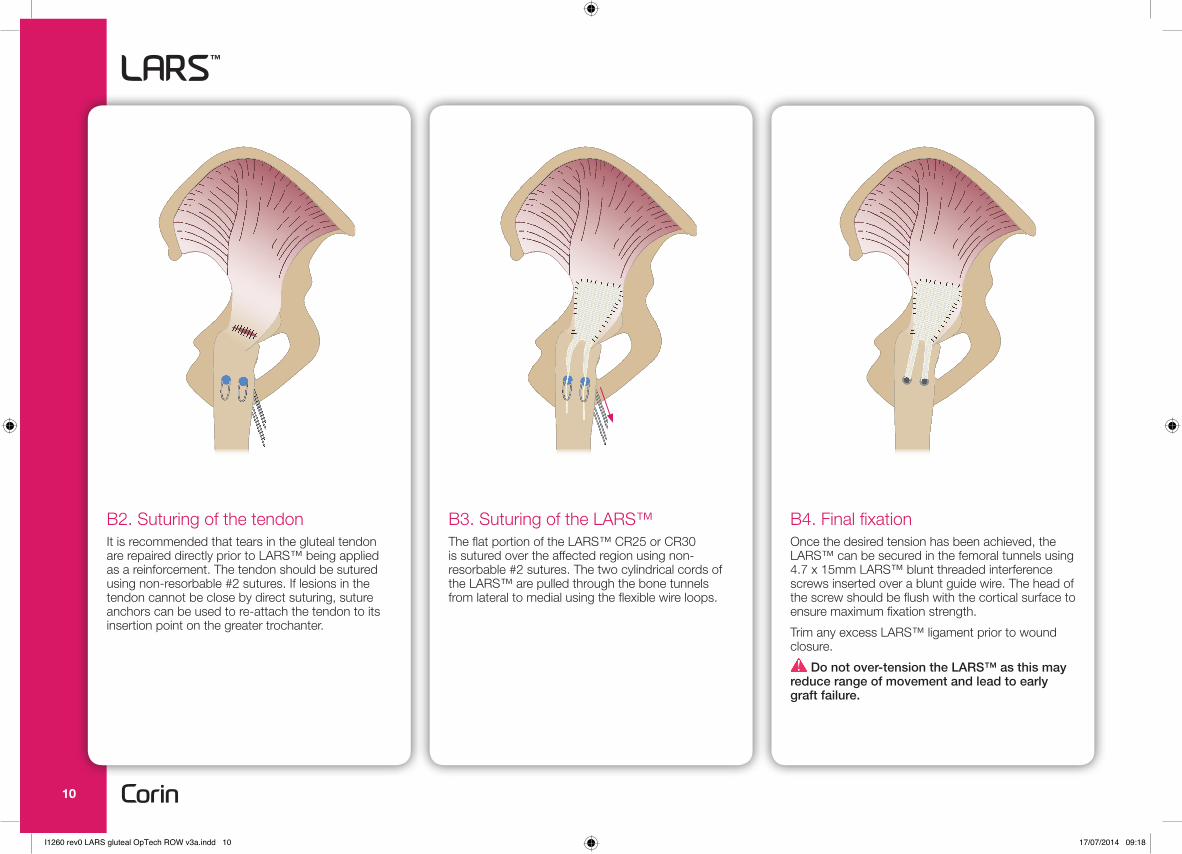
B2. Suturing of the tendonIt is recommended that tears in the gluteal tendon are repaired directly prior to LARS™ being applied as a reinforcement. The tendon should be sutured using non-resorbable #2 sutures. If lesions in the tendon cannot be close by direct suturing, suture anchors can be used to re-attach the tendon to its insertion point on the greater trochanter.
B3. Suturing of the LARS™The flat portion of the LARS™ CR25 or CR30 is sutured over the affected region using non-resorbable #2 sutures. The two cylindrical cords of the LARS™ are pulled through the bone tunnels from lateral to medial using the flexible wire loops.
B4. Final fixationOnce the desired tension has been achieved, the LARS™ can be secured in the femoral tunnels using 4.7 x 15mm LARS™ blunt threaded interference screws inserted over a blunt guide wire. The head of the screw should be flush with the cortical surface to ensure maximum fixation strength.
Trim any excess LARS™ ligament prior to wound closure.
Do not over-tension the LARS™ as this may reduce range of movement and lead to early graft failure.
10
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 10 17/07/2014 09:18
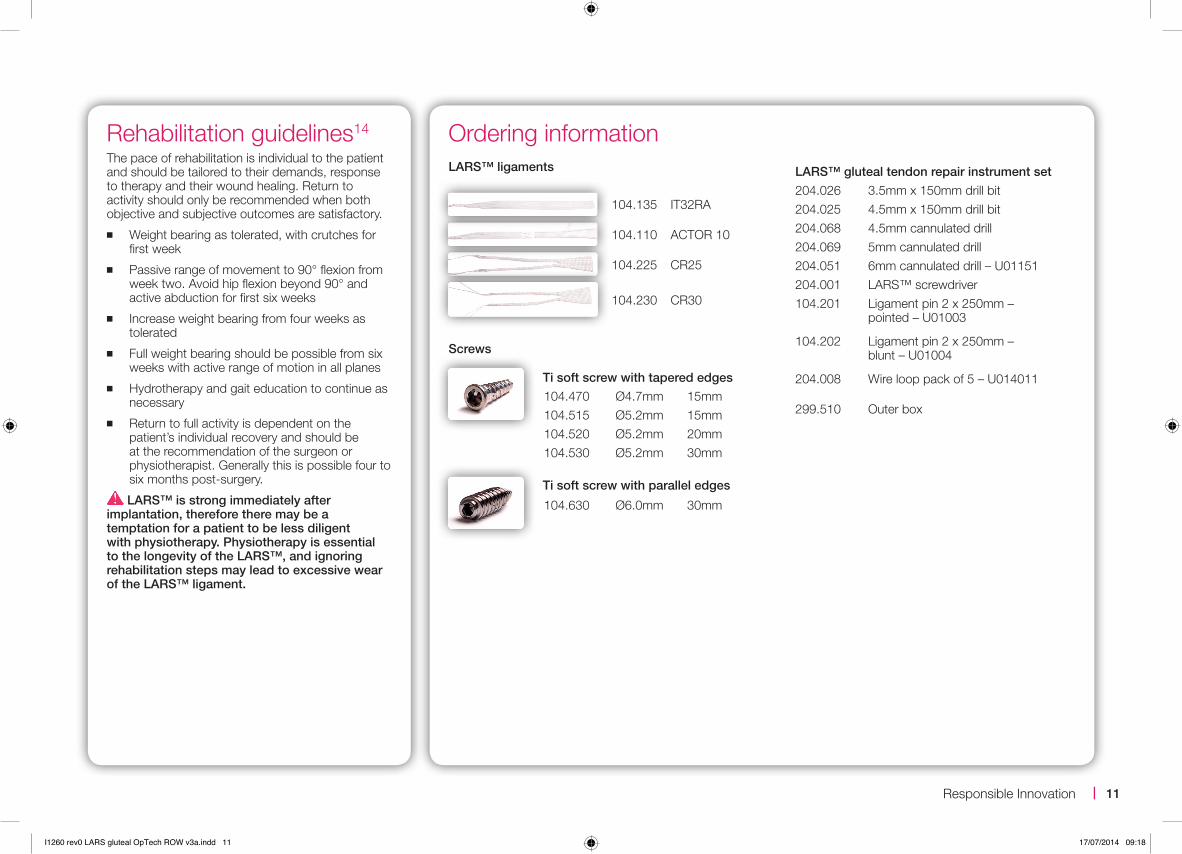
Ordering informationLARS™ gluteal tendon repair instrument set204.026 3.5mm x 150mm drill bit204.025 4.5mm x 150mm drill bit204.068 4.5mm cannulated drill204.069 5mm cannulated drill204.051 6mm cannulated drill – U01151204.001 LARS™ screwdriver104.201 Ligament pin 2 x 250mm –
pointed – U01003
104.202 Ligament pin 2 x 250mm – blunt – U01004
204.008 Wire loop pack of 5 – U014011
299.510 Outer box
104.135 IT32RA
104.110 ACTOR 10
104.225 CR25
104.230 CR30
LARS™ ligaments
Ti soft screw with tapered edges
104.470 Ø4.7mm 15mm104.515 Ø5.2mm 15mm104.520 Ø5.2mm 20mm104.530 Ø5.2mm 30mm
Ti soft screw with parallel edges
104.630 Ø6.0mm 30mm
Screws
Rehabilitation guidelines14
The pace of rehabilitation is individual to the patient and should be tailored to their demands, response to therapy and their wound healing. Return to activity should only be recommended when both objective and subjective outcomes are satisfactory.
■ Weight bearing as tolerated, with crutches for first week
■ Passive range of movement to 90° flexion from week two. Avoid hip flexion beyond 90° and active abduction for first six weeks
■ Increase weight bearing from four weeks as tolerated
■ Full weight bearing should be possible from six weeks with active range of motion in all planes
■ Hydrotherapy and gait education to continue as necessary
■ Return to full activity is dependent on the patient’s individual recovery and should be at the recommendation of the surgeon or physiotherapist. Generally this is possible four to six months post-surgery.
LARS™ is strong immediately after implantation, therefore there may be a temptation for a patient to be less diligent with physiotherapy. Physiotherapy is essential to the longevity of the LARS™, and ignoring rehabilitation steps may lead to excessive wear of the LARS™ ligament.
11 |Responsible Innovation
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 11 17/07/2014 09:18
The Corinium CentreCirencester, GL7 1YJ, UKt: +44 (0)1285 659 866f: +44 (0)1285 658 960e: [email protected]
©2013 Corin P No I1260 Rev0 12/2013 ECR 12720
Printed on Cocoon 100 which contains 100% total recycled fibre and is produced at a mill which folds the ISO 14001 for Environmental Management Systems. The pulp is bleached using Elemental Chlorine Free processes.
100%
References1. Williams BS, Cohen SP. Greater trochanteric pain syndrome: a review of anatomy, diagnosis and treatment. Anesthesia
and Analgesia 2009;108(5)1662-70.2. Segal NA, Felson DT, Torner JC, Zhu Y, Curtis JR, Niu J, Nevitt MC. Greater trochanteric pain syndrome: epidemiology
and associated factors. Archives of Physical Medicine and Rehabilitation 2007 August;88(8):988-992.3. Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical
examination findings in patients with greater trochanteric pain syndrome. Arthritis and Rheumatology 2001;44(9):2138-45.4. Kingzett-Taylor A, Tirman PF, Feller J, McGann W, Prieto V, Wischer T, Cameron JA, Cvitanic O, Genant HK. Tendinosis
and tears of gluteus medius and minimus muscles as a cause of hip pain: MR imaging findings. American Journal of Roentgenology 1999;173(4):1123-6.
5. Bunker TD, Esler CN, Leach WJ. Rotator-cuff tear of the hip. Journal of Bone and Joint Surgery [Br] 1997;79(4):618-20.6. Bajwa AS, Campbell DG, Comely AS, Lewis PL. Gluteal tendon reconstruction in association with hip arthroplasty.
Hip International 2011;21(3):288-92.7. Rajkumar S, Singer GC, Jones JR. Results following repair of gluteus medius defects following total hip arthroplasty.
Hip International 2011;21(3):293-8.8. Fearon AM, Scarvell JM, Cook JL, Smith PN. Does ultrasound correlate with surgical or histologic findings in greater
trochanteric pain syndrome? A pilot study. Clinical Orthopaedics and Related Research 2010;468(7):1838-44.9. Davies H, Zhaeentan S, Tavakkolizadeh A, Janes G. Surgical repair of chronic tears of the hip abductor mechanism.
Hip International 2009;19(4):372-6.10. Bucher TA, Darcy P, Ebert JR, Smith A, Janes G. Gluteal tendon repair augmented with a synthetic ligament: surgical
technique and a case series. Hip International 2014; 24(2): 187-93.11. Klinge U, Klosterhalfen B, Conze J, Limberg W, Obolenski B, Öttinger A, Schumpelick V. Modified Mesh for Hernia Repair
that is Adapted to the Physiology of the Abdominal Wall. European Journal of Surgery 1998;164;951-60.12. Tarbrizian M, Leroy-Gallisot A, Yahia L. (1996). Technical report: Evaluation of synthetic LARS knee ligaments,
Biomechanics and Biomaterials Research Group, École Polytechnique de Montréal, pp.1-34. 13. Cvitanic O, Henzie G, Skezas N, Lyons J, Minter J. MRI diagnosis of tears of the hip abductor tendons (gluteus medius
and gluteus minimus). American Journal of Roentgenology 2004;182(1):137-43.14. Janes G, Ebert J. Rehabilitation guidelines following gluteal tendon repair using synthetic ligament. Hollywood Functional
Rehabilitation Clinic, Perth.
I1260 rev0 LARS gluteal OpTech ROW v3a.indd 12 17/07/2014 09:18