Embed Size (px)
Citation preview

Clin Res Cardiol 96:730–737 (2007)DOI 10.1007/s00392-007-0551-7 ORIGINAL PAPER
R. ZahnT. IschingerM. HochadelB. MarkU. ZeymerJ. Jung
A. SchrammK. E. HauptmannH. SeggewißI. JanickeH. MudraJ. Senges
Glycoprotein IIb/IIIa antagonistsduring carotid artery stenting:
Results from the Carotid Artery Stenting (CAS) Registryof the Arbeitsgemeinschaft Leitende KardiologischeKrankenhausärzte (ALKK)
Received: 17 December 2006Accepted: 7 May 2007Published online: 27 June 2007
Priv.-Doz. Dr. Ralf Zahn ())Kardiologie/Angiologie/InternistischeIntensivmedizinKlinikum NürnbergBreslauer Straße 20190471 Nürnberg, GermanyTel.: 0911/398 29 89Fax: 0911/398 29 88E-Mail: [email protected]
Thomas IschingerKardiologie, Städtisches KlinikumEnglschalkinger Str. 7781925 München-Bogenhausen, Germany
Bernd Mark · Matthias HochadelUwe Zeymer · Jochen SengesHerzzentrum, KardiologieBremserstr. 7967063 Ludwigshafen, Germany
Jens JungMed. Klinik 1Kardiologie, StadtkrankenhausGabriel-von-Seidl-Str. 3167550 Worms, Germany
Alexander SchrammKlinik für Innere Medizinund Kardiologie, MarienhospitalJohannisfreiheit 2–449074 Osnabrück, GermanyMed. Abt. 1, KardiologieMarien HospitalPastor Janssen Str. 8–3846483 Wesel, Germany
Karl-Eugen HauptmannKardiologieKrankenhaus der Barmherzigen BrüderNordallee 154292 Trier, Germany
Hubert SeggewißAbt. für KardiologieKlinikum SchweinfurtGustav Adolfstr. 897422 Schweinfurt, Germany
Ilse JanickeAbteilung für KardiologieKWK-HerzzentrumGerrickstr. 2147137 Duisburg, Germany
Harald MudraAbteilung für KardiologieStädtisches KlinikumOskar-Maria-Graf-Ring 5181737 München – Neu-Perlach, Germany
n Abstract Background Glyco-protein II b/IIIa antagonists(GPII b/IIIa-A) lower the peri-procedural rate of ischemic eventsduring high risk percutaneouscoronary interventions. Theirclinical impact on carotid arterystenting (CAS) remains to be de-termined. Methods We analyzeddata from the Carotid Artery Stent(CAS) Registry. Results From 01/2000 to 06/2005 1322 CAS inter-ventions were registered. In 94(7.1%) procedures a GPII b/IIIa-Awas used: abciximab in 8 cases(8.6%), tirofiban in 53 cases (57%)and eptifibatide in 32 cases(34.4%). The use of a GPII b/IIIa-Aduring CAS decreased significantlyover time: from 17.6% in 2000 to3% in 2005, p for trend < 0.0001.The mean use of a GPII b/IIIa-A atthe hospitals was 5.2%. More than
50% of the hospitals never used aGPII b/IIIa-A. There were no sig-nificant differences in baselinecharacteristics and concomitantdiseases in CAS patients treatedwith GPII b/IIIa-A compared tothose without GPII b/IIIa-A. A bi-lateral intervention was performedmore often in patients treated withGPII b/IIIa-A (2.1 vs 0.2%,p = 0.04), a thrombus was moreoften visible (27 vs 12.4%,p < 0.001) and an ulcer more fre-quently diagnosed (50 vs 37.5%,p = 0.03). There was no significantdifference in the combined deathor stroke rate between the twogroups (5.3 vs 3.0%, p = 0.22,OR = 1.81, 95% CI: 0.69–4.72),which was confirmed by logisticregression analysis after adjustingfor possible confounders(OR = 1.67, 95% CI: 0.62–4.46,p = 0.31). Conclusions Our dataneither demonstrate a significantbenefit nor a significant risk withthe use of GPIIb/IIIa-A duringCAS. However, only an adequatelysized randomized controlled clin-ical trial could establish the realvalue of GPII b/IIIa-A during CAS.Until then, considering the poten-tial increase in cerebral hemor-rhage, we should not use GPII b/IIIa-A routinely during CAS.
n Key words carotid artery –carotid stenting – angioplasty –glycoprotein IIb/IIIa antagonists
for the ArbeitsgemeinschaftLeitende KardiologischeKrankenhausärzte (ALKK)

Introduction
Carotid artery stenting (CAS) currently is emergingas an alternative to carotid endarterectomy for thetreatment of severe stenoses of the carotid arteries[3, 18, 26, 27]. This approach has been recently in-corporated into the actual guidelines for secondaryprevention after a transient ischemic attack (TIA) orstroke [19].
In recently published series acute complicationsof CAS could be reduced by increasing experience ofthe interventionalists as well as the improvement ofthe CAS technique, such as the development of em-bolic protection devices (EPD)[8, 9, 18, 28].
Another option to reduce ischemic events duringCAS could be an optimized anti-thrombotic therapy.For percutaneous coronary interventions, manystudies showed that the addition of a glycoproteinII b/IIIa antagonist (GPII b/IIIa-A) on top of thestandard therapy with heparin and aspirin could re-duce the incidence of ischemic events. This wasshown for the different available GPII b/IIIa-A: ab-ciximab, tirofiban and eptifibatide [10, 11, 21–23].
Therefore it was hypothesized that this anti-thrombotic combination therapy might be beneficialduring CAS as well. Some preliminary registry datasuggested an adequate safety profile of such a regi-men [7, 14]. However, other registry data found ahigher complication rate for CAS when GPII b/IIIa-Awere used compared to conventional CAS under hep-arin, aspirin and clopidogrel only [4, 25]. Such ahigher risk using GPII b/IIIa-A during CAS was alsoreported by a small randomized controlled clinicaltrial [6]. There are also some reports suggesting apotential danger of GPII b/IIIa-A due to an increaseof intracranial hemorrhage [12, 15].
To determine the use and evaluate the safety andeffectiveness of GPII b/IIIa-A during CAS in clinicalpractice we analyzed the data of the prospective Car-otid Artery Stent (CAS) Registry of the German Ar-beitsgemeinschaft Leitende Kardiologische Kranken-hausärzte (ALKK).
Methods
The CAS Registry of the ALKK is an ongoing regis-try which was initiated in 1996 and has been de-scribed in detail previously [28]. In brief, all inter-ventions were prospectively enrolled in the registry.All complications occurring in the catheterizationlaboratory and during the in-hospital phase weredocumented. Since 2000 the use of GPII b/IIIa-A wasregistered. All data since January 2000 until June2005 were analyzed for this report.
n Patient selection
All patients undergoing CAS for a carotid stenosis atthe participating hospitals were considered for thisanalysis. Patients with symptomatic carotid stenoseshad a history of an ipsilateral stroke, at least onetransient ischemic attack (TIA) or an episode ofamaurosis fugax. In these patients an angiographi-cally documented stenosis ≥ 70% according to thediagnostic criteria of the North American Sympto-matic Carotid Endarterectomy Trial (NASCET) [13]was suggested to be an indication for an interven-tion. In the case of asymptomatic patients a stenosis80% was suggested as an indication for an interven-tion. The decision to treat a given patient was left tothe treating physician.
n Definitions
Amaurosis fugax was defined as a retinal ischemiawith transient monocular blindness and a transientischemic attack (TIA) as a focal neurological deficitthat resolved spontaneously within 24 h. Stroke wasdefined as loss of neurological function caused byan ischemic or hemorrhagic event with residualsymptoms at least 24 h after onset; a minor strokewas diagnosed if symptoms disappeared within 1week after onset and a major stroke if symptomspersisted for at least more than 1 week after onset.
No differentiation between ischemic, hemorrhagicand strokes with unknown etiology and no quantifi-cation of the severity of stroke (such as the NationalInstitute of Health stroke scale [2]), besides its rever-sibility, was made.
Endpoints were evaluated by a neurologist eitherimmediately at the occurrence of symptoms or at theend of the hospital stay. We did not separately evalu-ate 30-day follow-up endpoints. The combined clini-cal endpoint of all death and all strokes was prospec-tively defined as the primary endpoint.
n CAS procedure
The CAS procedure was performed according to thestandard protocol of each participating center.
n Data collection Every participating center wascommitted by written consent to include each pa-tient during the study period. The patients gave in-formed consent for the processing of their anon-ymous data.
731R. Zahn et al.Glycoprotein IIb/IIIa antagonists for carotid artery stenting

n Data analysis The patient population is describedby absolute numbers and percentages. Medians andquartiles are given for continuous variables. Dichot-omous values were compared by chi-square test andcrude odds ratios with 95% confidence intervalswere computed. Continuous variables were comparedby Mann-Whitney U-test. The Cochran-Armitagetrend test was used to analyze changes in the use ofGPII b/IIIa-A over time. Determinants for the use ofGPII b/IIIa-A were assessed by multiple logistic re-gression analyses adjusting each for year of interven-tion and center differences. As the use of GPII b/IIIa-A was seen to decline steadily over time and tobe used frequently only in one single center, adjust-ment was done by including the year of interventionas a linear term and an indicator for the center X inthe model. Logistic regression analysis was also usedto adjust for factors influencing the combined clini-cal endpoint of all death and all strokes. In additionto the use of GPII b/IIIa-A, the known fundamentalrisk factors age, symptomatic stenosis and use of anembolic protection device (EPD) were included, aswell as factors showing a difference in the use ofGPII b/IIIa-A at a level of p < 0.1 were considered ifthey had additional significance. The discriminationof the model was assessed by the C statistic. P-val-ues < 0.05 were considered significant. All p-valuesare results of two-tailed tests. The calculations wereperformed using SAS©, version 9.1 (Cary, North Car-olina).
Results
From 01/2000 to 06/2005, 1322 CAS interventionswith information on the use of GPIIb/IIIa-A wereperformed. In 94 out of these 1322 CAS procedures(7.1%) a GPIIb/IIIa-A was used. The different GPIIb/IIIa-A agents were used as follows: abciximab in 8cases (8.6%), tirofiban in 53 cases (57%) and eptifi-batide in 32 cases (34.4%).
n Patient, lesion and interventional characteristics
As shown in Table 1 there were no significant differ-ences in baseline characteristics and concomitantdiseases in CAS patients treated with GPII b/IIIa-Acompared to those without GPII b/IIIa-A. A bilateralintervention was performed more often in patientstreated with GPII b/IIIa-A (2.1 vs 0.2%, p = 0.04), athrombus was more often visible (27 vs 12.4%,p < 0.001) and an ulcer more frequently diagnosed(50 vs 37.5%, p = 0.03) (Table 2). No important dif-ferences in interventional characteristics between the
two groups were observed. Concerning hospitalmedication there were no differences between thegroups with the exception that patients treated witha GPIIb/IIIa-A were more likely to receive also an-giotensin converting enzyme inhibitors (80 vs 66.8%,p = 0.01) (Table 3).
n Determinants of the use of GPII b/III a-A
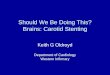
As shown in Figure 1, the use of a GPII b/IIIa-A dur-ing CAS decreased significantly during the years:from 17.6% in 2000 to 3% in 2005, p for trend< 0.0001. Whereas abciximab was mainly used in2000 and 2001, eptifibatide and tirofiban were usedin the following years, but only tirofiban until 2005(Fig. 2).
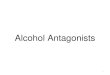
The use of a GPII b/IIIa-A at the different hospi-tals was quite different (Fig. 3). The mean use of aGPII b/IIIa-A at the hospitals was 5.2%. However,
732 Clinical Research in Cardiology, Volume 96, Number 10 (2007)© Steinkopff Verlag 2007
Table 1 Baseline characteristics and concomitant diseases
GPIIb/IIIa-An = 94 (100%)
No GPIIb/IIIa-An = 1228 (100%)
p-value
Age (years) a 70 (64–77) 71 (65–76) 0.98Male gender 73/94 (77.7%) 883/1228 (71.9%) 0.23Symptomaticcarotid stenosis
40/94 (42.6%) 545/1228 (44.4%) 0.73
Kind of ipsilateral symptoms (in symptomatic patients):Amaurosis fugax 7/40 (17.5%) 79/545 (14.5%) 0.60TIA 19/40 (47.5%) 234/545 (42.9%) 0.57Stroke 15/40 (37.5%) 247/545 (45.3%) 0.34Prior carotid arterysurgery
7/94 (7.4%) 70/1228 (5.7%) 0.49
Prior carotid arterydilatation
9/94 (9.6%) 75/1228 (6.1%) 0.18
Concomitant diseasesCoronary heartdisease
72/92 (78.3%) 850/1216 (69.9%) 0.09
Prior myocardialinfarction
29/92 (31.5%) 353/1213 (29.1%) 0.62
Peripheral arterialdisease
28/89 (31.5%) 325/1207 (26.9%) 0.35
Heart failure(≥ NYHA class III)
1/88 (1.1%) 63/1205 (5.2%) 0.09
Atrial fibrillation 5/89 (5.6%) 98/1210 (8.1%) 0.40Chronic obstructivepulmonary disease
6/88 (6.8%) 42/1208 (3.5%) 0.11
Arterialhypertension
84/90 (93.3%) 1117/1220 (91.6%) 0.56
Diabetes mellitus 27/89 (30.3%) 414/1206 (34.3%) 0.44Hyperlipidemia 74/90 (82.2%) 1053/1215 (86.7%) 0.24Current smoker 36/90 (40.0%) 375/1204 (31.1%) 0.08
a median and quartiles

more than 50% of the hospitals never used a GPII b/IIIa-A, most of the remaining hospitals used it inless than 10% of their CAS procedure and only onehospital used them in 67% of procedures.
Adjusted for the effect of hospital X and the tem-poral trend, logistic regression analysis revealed onlystenosis calcification and smoking as factors beingindependently associated with their use (Table 4).
n Use of GPII b/III a-A and clinical event rate
There was a significant higher rate of ipsilateralTIAs in the GPII b/IIIa-A group (7.4 vs 2.7%;p = 0.01, OR = 2.91, 95% CI: 1.25–6.78) as well as ahigher rate of ipsilateral minor strokes (4.3 vs 0.7%,p < 0.001, OR = 6.02, 95% CI: 1.82–19.9). However,there was no significant difference in the com-bined death or stroke rate between the two groups(5.3 vs 3.0%, p = 0.22, OR = 1.81, 95% CI: 0.69–4.72)(Table 3).
A logistic regression model on the death or strokerate showed borderline significance for symptomaticstenosis, EPD, bilateral intervention, and age (all p-values between 0.04 and 0.07) and reached a C indexof 0.65. The use of a GPIIb/IIIa-A was not indepen-dently associated with the combined endpoint(OR = 1.67, 95%CI: 0.62–4.46, p = 0.31).
Discussion
An optimized anti-thrombotic regimen can reduceischemic complications during percutaneous coro-nary interventions. The addition of a GPIIb/IIIa-Aon top of the standard therapy with heparin and as-pirin has shown to further reduce the incidence ofischemic events. This could be shown for the differ-ent available GPII b/IIIa-A: abciximab, tirofiban andeptifibatide [10, 11, 21–23]. Therefore it seemedplausible to apply this anti-thrombotic combinationtherapy from coronary interventions to CAS.
The data from this large CAS registry over thelast 5 years showed that GPII b/IIIa-A were used inonly 94 out of 1322 CAS procedures (7.1%): abcixi-mab in 8.6%, tirofiban in 57% and eptifibatide in34.4%. The most important determinants of the useof GPII b/IIIa-A weren the policy of the individual hospitals: more than
50% of the hospitals never used a GPII b/IIIa-A,most of the remaining hospitals used it in less than10% of their CAS procedures and only one hospitalused them in 67% of procedures, with a mean use ofa GPII b/IIIa-A at the hospitals of 5.2%.
n the time of the treatment of patients. The use of aGPII b/IIIa-A during CAS significantly decreasedover time: from 17.6% in 2000 to 3% in 2005, pfor trend < 0.0001. This indicates a change in theperception of the appropriateness of the use ofGPII b/IIIa-A for CAS, which may have been trig-gered by publications on worse clinical outcomewith GPII b/IIIa-A during CAS [6, 25].
Some preliminary data suggested that GPIIb/IIIa-Amight be helpful during CAS, especially when usedfor fresh thrombi [24]. Some registries also reportedan adequate safety profile of such a regimen [7, 14].
Kapadia et al. [7] reported on 151 consecutiveCAS patients, 128 patients received adjuvant therapywith abciximab. All patients received aspirin and athienopyridine. Procedural and 30-day outcomeswere compared between the control (n = 23) and ab-ciximab (n = 128) groups. Procedural events weremore frequent in the control group (8%; 1 majorstroke and 1 neurological death) compared with theabciximab group (1.6%; 1 minor stroke and 1 retinal
733R. Zahn et al.Glycoprotein IIb/IIIa antagonists for carotid artery stenting
Table 2 Carotid lesion and interventional characteristics
GPIIb/IIIa-An = 94 (100%)
No GPIIb/IIIa-An = 1228 (100%)
p-value
Location of target stenosisRight carotid artery 50/94 (53.2%) 596/1222 (48.8%) 0.41Bilateral intervention 2/94 (2.1%) 3/1222 (0.2%) 0.004
Lesion characteristicsRestenosis after surgeryor dilatation
15/94 (16.0%) 110/1228 (9.0%) 0.03
Thrombus visible 20/74 (27.0%) 103/829 (12.4%) < 0.001Ulcer 37/74 (50.0%) 311/829 (37.5%) 0.03Severe calcification 17/74 (23.0%) 280/829 (33.8%) 0.06Length >10 mm 45/74 (60.8%) 484/829 (58.4%) 0.68Bifurcation involved 37/74 (50.0%) 383/829 (46.2%) 0.53%-stenosis beforeintervention a
86 (80–90) 90 (80–90) 0.24
Interventional characteristicsProtection device used 81/92 (88.0%) 1026/1162 (88.3%) 0.94
Pre-dilatation necessary 11/69 (15.9%) 109/983 (11.1%) 0.22Maximal balloondiameter (mm)
5.0 (4.5–5.5) 5.0 (5–6) 0.001
Maximal balloonpressure (mmHg)
12 (10–14) 12 (8–14) 0.82
Stent implantation 92/94 (97.9%) 1214/1228 (98.9%) 0.40Stent length (mm) a 30 (30–40) 30 (30–40) 0.17Numbers of dilatations 1 (1–2) 2 (1–2) 0.51%-stenosis afterinterventiona
5 (0–15) 5 (0–10) 0.06
Duration of the proce-dure (minutes)a
40 (30–55) 40 (30–56) 0.44
a median and quartiles

infarction; P = 0.05). However, on 30-day follow-up,one patient presented with delayed intracranial hem-orrhage in the abciximab group.
Qureshi et al. [15] reported on 25 patients whounderwent CAS and were treated with eptifibatide.No intracerebral hemorrhages and one minor isch-emic stroke occurred during the 1-month follow-upperiod. The minor stroke was observed on postpro-
cedure day 7 in a patient for whom antiplatelet ther-apy was discontinued before a coronary artery by-pass graft operation was performed. One episode ofmajor bleeding from the femoral insertion site re-quired surgical repair and blood transfusions. Minorbleeding occurred in one patient.
However, other more recent registry data found ahigher complication rate for CAS when GPIIb/IIIa-A
734 Clinical Research in Cardiology, Volume 96, Number 10 (2007)© Steinkopff Verlag 2007
Table 3 Hospital medication and hospital events
GPIIb/IIIa-An = 94 (100%)
No GPIIb/IIIa-An = 1228 (100%)
p-value OR (95% CI)
Hospital medicationAspirin 90/91 (98.9%) 1148/1195 (96.1%) 0.16Ticlopidine/Clopidogrel 91/91 (100%) 1166/1197 (97.4%) 0.12Phenprocoumon 2/69 (2.9%) 59/1157 (5.1%) 0.57Statins* 62/77 (80.5%) 992/1181 (84.0%) 0.42Angiotensin converting enzyme inhibitors* 64/80 (80.0%) 784/1174 (66.8%) 0.01�-blockers* 44/80 (55.0%) 763/1176 (64.9%) 0.07
Hospital eventsIpsilateral amaurosis fugax 0/94 (0%) 2/1228 (0.2%) 0.70 -Ipsilateral TIA 7/94 (7.4%) 33/1128 (2.7%) 0.02 2.91 (1.25–6.78)Ipsilateral stroke 5/94 (5.3%) 26/1228 (2.1%) 0.06 2.60 (0.97–6.93)– ipsilateral minor stroke 4/94 (4.3%) 9/1228 (0.7%) 0.01 6.02 (1.82–19.9)– ipsilateral major stroke 1/94 (1.1%) 18/1228 (1.5%) 1.00 0.72 (0.10–5.47)Ipsilateral stroke/TIA/amaurosis fugax 12/94 (12.8%) 59/1228 (4.8%) < 0.001 2.90 (1.50–5.61)Any ischemic event contralateral 2/94 (2.1%) 16/1228 (1.3%) 0.37 1.65 (0.37–7.27)Myocardial infarction 0/94 (0%) 2/1228 (0.2%) 0.70Death 0/94 (0%) 9/1228 (0.7%) 0.40All non-fatal strokes and all death 5/94 (5.3%) 37/1228 (3.0)% 0.22 1.81 (0.69–4.72)Any death/stroke/TIA/ amaurosis fugax 14/94 (14.9%) 77/1228 (6.3%) 0.001 2.62 (1.42–4.83)
OR odds ratio, CI confidence interval; * data available only in a subset of patients
17,6
10,4 10,8
7,8
3,1 3
0
5
10
15
20
25
30
2000 2001 2002 2003 2004 2005year
(%)
p fo
r tre
nd <
0.0
001
(until 06/2005)
Fig. 1 Development in the use of GPIIb/IIIa antagonists over time
Fig. 2 Use of the different GPIIb/IIIa antagonists (abciximab, tirofiban, epti-fibatide) over time

were used compared to conventional CAS under hep-arin, aspirin and clopidogrel only [4, 25].
Chan et al. [4] from the Cleveland Clinic group(same group of as reference [7], with partial overlapof patients), reported on 305 consecutive patientswho underwent CAS. During this period, the clinicalpractice of carotid stenting evolved from the routineuse of GPII b/IIIa-A to routine embolic protectiondevice (EPD) placement. A total of 199 patients re-ceived adjunctive GPII b/IIIa-A (91% abciximab),and 106 patients underwent the procedure with anEPD. At 30 days, the composite end point of neuro-logical death, nonfatal stroke, and major bleeding,including intracranial hemorrhage, was significantlylower among patients treated with EPDs comparedwith those treated with GPII b/IIIa-A (0 vs 5.1%,p = 0.02).
Wholey et al. [25] reported on the experience in216 CAS patients treated with GPIIb/IIIa-A, whoseoutcomes were compared to a control group of 334patients who received intravenous heparin alone.The all stroke/neurological death rate in 216 patients
treated with heparin and GPIIb/IIIa-A was 6.0% (13events) compared 2.4% (8 events) in the 334 patientsin the heparin-only control group (p = 0.0430). Twoof the four neurologically-related deaths in theGPIIb/IIIa inhibitor group resulted from intracranialhemorrhages; there were no intracranial hemor-rhages in the heparin-only group.
These findings are comparable to our data: Therewas a significant higher rate of ipsilateral TIAs inthe GPII b/IIIa-A group (7.4 vs 2.7%; p = 0.01,OR = 2.91, 95% CI: 1.25–6.78) as well as a higher rateof ipsilateral minor strokes (4.3 vs 0.7%, p < 0.001,OR = 6.02, 95%CI: 1.82–19.9). However, there was nosignificant difference in the combined death orstroke rate between the two groups (5.3 vs 3.0%,p = 0.22, OR = 1.81, 95% CI: 0.69–4.72), which wasconfirmed by logistic regression analysis (OR = 1.66,95% CI: 0.62–4.43, p = 0.31).
A higher risk using GPIIb/IIIa-A during CAS wasalso reported by a small randomized controlled clin-ical trial. Hofmann et al. [6] reported on 74 consecu-tive patients undergoing elective CAS. Standard anti-thrombotic medication consisted of aspirin, clopido-grel, and heparin. In addition, half of the patientsreceived an abciximab bolus of 0.25 mg/kg bodyweight given prophylactically before the intervention.In patients receiving abciximab, ischemic complica-tions consisted of 4 transient ischemic attacks, 1 mi-nor stroke, 1 nonfatal major stroke, and 1 fatal strokecaused by cerebral hemorrhage. In the control group,2 transient ischemic attacks and 1 major nonfatalstroke occurred. In summary, the total number ofperiprocedural ischemic events was 7 (19%) in theabciximab group and 3 (8%) in the control group.Non-ischemic complications consisted of 1 inguinalhematoma requiring blood transfusions in eachgroup.
There are also some further reports suggesting apotential danger of GPIIb/IIIa-A due to intracranialhemorrhage [12, 15].
The major problem of the currently available puz-zling data on GPIIb/IIIa-A during CAS is that a) theregistry data may be strongly influenced by patientselection, especially when historical groups of CASpatients are compared and b) according to the over-all low number of CAS patients treated with GPIIb/IIIa-A the power to detect a real difference is toolow to really draw definite conclusions from theavailable data. Assuming a hospital death or strokerate of about 5% for conventional CAS with an EPD,about 5700 patients would be needed in a random-ized clinical trial to detect a 30% reduction of thecombined endpoint with a power of 80% with theuse of GPIIb/IIIa-A. Furthermore, the pathophysiolo-gic scenario of CAS may be more similar to venousbypass graft interventions than to native coronary
735R. Zahn et al.Glycoprotein IIb/IIIa antagonists for carotid artery stenting
0
10
20
30
40
50
60
70
80
90
100
hospitals
use
of G
P IIb
/IIIa
ant
agon
ists
(%)
Median: 0.8% (quartiles: 0% – 4.3%)Mean: 5.2% ± 15.3%
Fig. 3 Use of GPIIb/IIIa antagonists at the participating hospitals (only hos-pitals with more than 10 carotid interventions included)
Table 4 Potential determinants of the use of GPIIb/IIIa antagonists,adjusted for year of intervention and center effect
Adjusted OR(± 95%CI)
p-value
Severe calcification 0.34 (0.14–0.85) 0.02Current smoker 2.19 (1.10–4.37) 0.03Male gender 1.91 (0.89–4.11) 0.10Ulcer 1.48 (0.68–3.20) 0.32Presence of thrombus 1.63 (0.60–4.43) 0.34Heart failure (≥ NYHA class III) 0.39 (0.04–3.90) 0.42Symptomatic stenosis 1.29 (0.66–2.51) 0.45Restenosis after surgery or dilatation 0.81 (0.29–2.23) 0.68Bilateral intervention 2.55 (0.01–451.9) 0.72Coronary heart disease 0.99 (0.47–2.14) 0.99

interventions in high risk patients, especially pa-tients with acute coronary syndromes. In the latterGPII b/IIIa-A have proven their efficacy during per-cutaneous interventions [10, 11, 21–23]; however forvenous bypass graft interventions such a possibleeffect of GPII b/IIIa-A could not be shown [17]. Thismay be due to a higher percentage of plaque anddebris embolization during bypass interventionscompared to more fresh thrombi embolization dur-ing native coronary interventions. The embolizationof such more solid particles during venous bypassor carotid interventions seem to be more likely to beprevented with embolic protection devices [1, 20,28], than with GPII b/IIIa-A [4].
Conclusions
This analysis from a large CAS registry showed thatGPIIb/IIIa-A were used infrequently in the last yearswith decreasing numbers most currently and a widevariability in their use between the participatinghospitals. Our data neither demonstrate a significantbenefit nor a significant risk with the use of GPIIb/IIIa-A during CAS. However, only an adequatelysized randomized controlled clinical trial could es-tablish the real value of GPIIb/IIIa-A during CAS.Until then, considering the potential increase in ce-rebral hemorrhage, we should not use GPIIb/IIIa-Aroutinely during CAS.
n Limitations of the study
Since the CAS Registry of the ALKK is an observa-tional study it is not possible to control totally forthe selection of patients to be treated with GPII b/IIIa-A. One such factor could have been triggered bythe fact that one institution accounted for more halfof the GPII b/IIIa-A used, thus having a strong influ-ence of all characteristics and outcome of patientsreceiving a GPII b/IIIa-A during CAS.
We also obtained only limited data of the real ad-ministration of the GPII b/IIIa-A. Because the treat-ment was left to the treating physician, we do notknow the exact time of administration, such as be-fore or during the intervention, nor do we know ifACT measurements were performed, and whatamount of heparin was given in the patients.
We also did not ask for intracranial hemorrhages,which are all summarized as strokes. However, sucha differentiation would have been of special interestconsidering the potential risk of increased cerebralbleeding with GPII b/IIIa-A. Due to the small num-bers of patients we can furthermore not evaluate dif-ferences between the 3 GPII b/IIIa-A. We obtainedonly data until hospital discharge. Therefore it maybe difficult to compare our data to 30 days outcomedata of other studies. However, clinical events are ex-tremely low after the first few days of stent implan-tation [5, 16].
736 Clinical Research in Cardiology, Volume 96, Number 10 (2007)© Steinkopff Verlag 2007
References
1. Baim DS, Wahr D, George B, LeonMB, Greenberg J, Cutlip DE, Kaya U,Popma JJ, Ho KK, Kuntz RE (2002)Randomized Trial of a Distal EmbolicProtection Device During Percuta-neous Intervention of SaphenousVein Aorto-Coronary Bypass Grafts.Circulation 105:1285–1290
2. Brott T, Adams HP, Jr., Olinger CP,Marler JR, Barsan WG, Biller J, Spil-ker J, Holleran R, Eberle R, Hertz-berg V (1989) Measurements of acutecerebral infarction: a clinical exami-nation scale. Stroke 20:864–870
3. CAVATAS Investigators (2001) Endo-vascular versus surgical treatmentin patients with carotid stenosis inthe Carotid and Vertebral ArteryTransluminal Angioplasty Study(CAVATAS): a randomised trial. Lan-cet 357:1729–1737
4. Chan AW, Yadav JS, Bhatt DL, BajzerCT, Gum PA, Roffi M, Cho L, AgahR, Topol EJ (2005) Comparison ofthe safety and efficacy of emboliprevention devices versus platelet gly-coprotein II b/IIIa inhibition duringcarotid stenting. Am J Cardiol 95:791–795
5. Cremonesi A, Manetti R, Setacci F,Setacci C, Castriota F (2003) Pro-tected carotid stenting: clinical ad-vantages and complications of em-bolic protection devices in 442 conse-cutive patients. Stroke 34:1936–1941
6. Hofmann R, Kerschner K, Steinwen-der C, Kypta A, Bibl D, Leisch F(2002) Abciximab bolus injectiondoes not reduce cerebral ischemiccomplications of elective carotid ar-tery stenting: a randomized study.Stroke 33:725–727
7. Kapadia SR, Bajzer CT, Ziada KM,Bhatt DL, Wazni OM, Silver MJ, Bev-en EG, Ouriel K, Yadav JS (2001) Ini-tial experience of platelet glycopro-tein IIb/IIIa inhibition with abcixi-mab during carotid stenting: a safeand effective adjunctive therapy.Stroke 32:2328–2332
8. Kastrup A, Groschel K, Krapf H,Brehm BR, Dichgans J, Schulz JB(2003) Early outcome of carotidangioplasty and stenting with andwithout cerebral protection devices:a systematic review of the literature.Stroke 34:813–819
9. Lanzer P, Weser R, Prettin C (2006)Carotid-artery stenting in a high-riskpatient population–single centre, sin-gle operator results. Clin Res Cardiol95:4–12
10. Lincoff AM (1998) Trials of plateletglycoprotein IIb/IIIa receptor antago-nists during percutaneous coronaryrevascularization. Am J Cardiol 82:36P–42P

737R. Zahn et al.Glycoprotein IIb/IIIa antagonists for carotid artery stenting
11. Lincoff AM, Califf RM, Moliterno DJ,Ellis SG, Ducas J, Kramer JH, Klei-man NS, Cohen EA, Booth JE, SappSK, Cabot CF, Topol EJ (1999) Com-plementary clinical benefits of coro-nary-artery stenting and blockade ofplatelet glycoprotein IIb/IIIa recep-tors. Evaluation of Platelet IIb/IIIa In-hibition in Stenting Investigators. NEngl J Med 341:319–327
12. Moshiri S, Di MC, Liistro F, Melissa-no G, Chiesa R, Colombo A (2001)Severe intracranial hemorrhage afteremergency carotid stenting and ab-ciximab administration for postoper-ative thrombosis. Catheter CardiovascInterv 53:225–228
13. North American Symptomatic Caro-tid Endarterectomy Trial Collabora-tors (1991) Beneficial effect of carotidendarterectomy in symptomatic pa-tients with high-grade carotid steno-sis. North American SymptomaticCarotid Endarterectomy Trial Collab-orators. N Engl J Med 325:445–453
14. Qureshi AI, Siddiqui AM, Hanel RA,Xavier AR, Kim SH, Kirmani JF, Bou-los AS, Hopkins LN (2004) Safety ofhigh-dose intravenous eptifibatide asan adjunct to internal carotid arteryangioplasty and stent placement: aprospective registry. Neurosurgery 54:307–316
15. Qureshi AI, Suri MF, Ali Z, Kim SH,Lanzino G, Fessler RD, Ringer AJ,Guterman LR, Hopkins LN (2002)Carotid angioplasty and stent place-ment: a prospective analysis of perio-perative complications and impact ofintravenously administered abcixi-mab. Neurosurgery 50:466–473
16. Reimers B, Schlüter M, Castriota F,Tubler T, Corvaja N, Cernetti C,Manetti R, Picciolo A, Liistro F, DiMario C, Cremonesi A, Schofer J, Co-lombo A (2004) Routine use of cere-bral protection during carotid arterystenting: results of a multicenter reg-istry of 753 patients. Am J Med 116:217–222
17. Roffi M, Mukherjee D, Chew DP,Bhatt DL, Cho L, Robbins MA, ZiadaKM, Brennan DM, Ellis SG, Topol EJ(2002) Lack of benefit from intrave-nous platelet glycoprotein IIb/IIIa re-ceptor inhibition as adjunctive treat-ment for percutaneous interventionsof aortocoronary bypass grafts: apooled analysis of five randomizedclinical trials. Circulation 106:3063–3067
18. Roubin GS, New G, Iyer SS, Vitek JJ,Al Mubarak N, Liu MW, Yadav J, Go-mez C, Kuntz RE (2001) Immediateand late clinical outcomes of carotidartery stenting in patients with symp-tomatic and asymptomatic carotid ar-tery stenosis: a 5-year prospectiveanalysis. Circulation 103:532–537
19. Sacco RL, Adams R, Albers G, Al-berts MJ, Benavente O, Furie K, Gold-stein LB, Gorelick P, Halperin J, Har-baugh R, Johnston SC, Katzan I,Kelly-Hayes M, Kenton EJ, Marks M,Schwamm LH, Tomsick T (2006)Guidelines for prevention of stroke inpatients with ischemic stroke or tran-sient ischemic attack: a statement forhealthcare professionals from theAmerican Heart Association/Ameri-can Stroke Association Council onStroke: co-sponsored by the Councilon Cardiovascular Radiology and In-tervention: the American Academy ofNeurology affirms the value of thisguideline. Stroke 37:577–617
20. Stone GW, Rogers C, Hermiller J,Feldman R, Hall P, Haber R, MasudA, Cambier P, Caputo RP, Turco M,Kovach R, Brodie B, Herrmann HC,Kuntz RE, Popma JJ, Ramee S, CoxDA (2003) Randomized comparisonof distal protection with a filter-basedcatheter and a balloon occlusion andaspiration system during percuta-neous intervention of diseased saphe-nous vein aorto-coronary bypassgrafts. Circulation 108:548–553
21. The EPIC Investigators (1994) Use ofa monoclonal antibody directedagainst the platelet glycoprotein IIb/IIIa receptor in high-risk coronaryangioplasty. The EPIC Investigation.N Engl J Med 330:956–961
22. The EPILOG Investigators (1997)Platelet glycoprotein IIb/IIIa receptorblockade and low-dose heparin dur-ing percutaneous coronary revascu-larization. N Engl J Med 336:1689–1696
23. The EPISTENT Investigators (1998)Randomised placebo-controlled andballoon-angioplasty-controlled trialto assess safety of coronary stentingwith use of platelet glycoprotein-II b/IIIa blockade. The EPISTENT Inves-tigators. Evaluation of Platelet II b/IIIa Inhibitor for Stenting. Lancet352:87–92
24. Tong FC, Cloft HJ, Joseph GJ, Sa-muels OB, Dion JE (2000) Abciximabrescue in acute carotid stent throm-bosis. AJNR Am J Neuroradiol 21:1750–1752
25. Wholey MH, Wholey MH, Eles G,Toursakissian B, Bailey S, Jarmolows-ki C, Tan WA (2003) Evaluation ofglycoprotein II b/IIIa inhibitors incarotid angioplasty and stenting. JEndovasc Ther 10:33–41
26. Yadav JS, Wholey MH, Kuntz RE,Fayad P, Katzen BT, Mishkel GJ, Baj-wa TK, Whitlow P, Strickman NE,Jaff MR, Popma JJ, Snead DB, CutlipDE, Firth BG, Ouriel K (2004) Pro-tected carotid-artery stenting versusendarterectomy in high-risk patients.N Engl J Med 351:1493–1501
27. Zahn R, Hochadel M, Grau A, SengesJ (2005) Stent-supported angioplastyversus endarterectomy for carotid ar-tery stenosis Evidence from currentrandomized trials. Z Kardiol 94:836–8343
28. Zahn R, Mark B, Niedermaier N,Zeymer U, Limbourg P, Ischinger T,Haerten K, Hauptmann KE, LeitnerER, Kasper W, Tebbe U, Senges J(2004) Embolic protection devices forcarotid artery stenting: better resultsthan stenting without protection? EurHeart J 25:1550–1558