Embed Size (px)
Citation preview

CompanyOverviewJuly 2018
Forward Looking Statements
This presentation includes statements that are, or may be deemed, “forward-looking statements.” In some cases, you can identify forward-looking statements by terminology including “anticipates,” “believes,” “can,” “continue,” “could,” “estimates,” “expects,” “intends,” “may,” “plans,” “potential,” “predicts,” “should,” “will,” “would” or the negative thereof or other variations thereon or other comparable terminology.
We operate in a very competitive and rapidly-changing environment and new risks emerge from time to time. As a result, it is not possible for our management to predict all risks, nor can we assess the impact of all factors on our business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward-looking statements we may make. In light of these risks, uncertainties and assumptions, the forward-looking events and circumstances discussed in this presentation may not occur and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements. You are cautioned not to place undue reliance upon such forward-looking statements as predictions of future events. Although we believe that the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee that the future results, levels of activity, performance or events and circumstances reflected in the forward-looking statements will be achieved or occur. We direct you to our Annual Report on Form 10-K for the year ended December 31, 2017, our subsequent current reports on Form 8-K and our other filings with the Securities and Exchange Commission.
Any forward-looking statement included in this presentation speaks only as of the date hereof. Except as required by law, we do not undertake any obligation to update or revise, or to publicly announce any update or revision to, any of the forward-looking statements, whether as a result of new information, future events or any other reason after the date of this presentation. For all forward-looking statements, we claim the protection of the safe harbor for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995.
Company Overview2
Safe Harbor Statement
Company Overview3
GT Biopharma is a clinical‐stage biotechnology company primarily focused on utilizing its proprietary platforms to develop next‐generation, targeted immuno‐oncology therapies for hematological malignancies, sarcomas and solid tumors
Investment Thesis
• Proprietary technology platforms: Tri- and Tetra-specific Natural Killer Cell Engagers (TriKE) & (TetraKE) and bi-specific Antibody Drug Conjugates (ADC)
• Collaboration with Dr. Jeffrey Miller, Deputy Director, The Masonic Cancer Center, University of Minnesota, a recognized leader in Natural Killer (NK) cell therapy and IL-15 biology
• Two clinical programs in progress/planned for most advanced immuno-oncology candidates• OXS-3550, novel TriKE for CD33+ hematologic malignancies expect to initiate First-in-Human trial 2H ’18
• Dose finding and extended efficacy component• OXS-1550, novel bi-specific antibody drug conjugate (ADC) for B-cell lymphomas and leukemias
• Two durable responses seen in Phase 1 dose escalation study• Bi-Specific ADC Ad Board, encouraging clinical results from interim review
• Potential for rapid pipeline progression • Targeting three TriKE/TetraKE product candidates to be in the clinic by 2H ‘19
• Exclusive license to broad IP estate covering oncology pipeline with exclusive rights to TriKEand TetraKE platform, Bi-Specific ADC platform as well as a portfolio of CNS product candidates for potential licensing
• Management Team, Board of Directors and Scientific Advisory Board with track record of success
Company Overview4
Natural Killer Cell Targeting: Potential to be the Next Frontier in Cancer Immunotherapy
Company Overview5
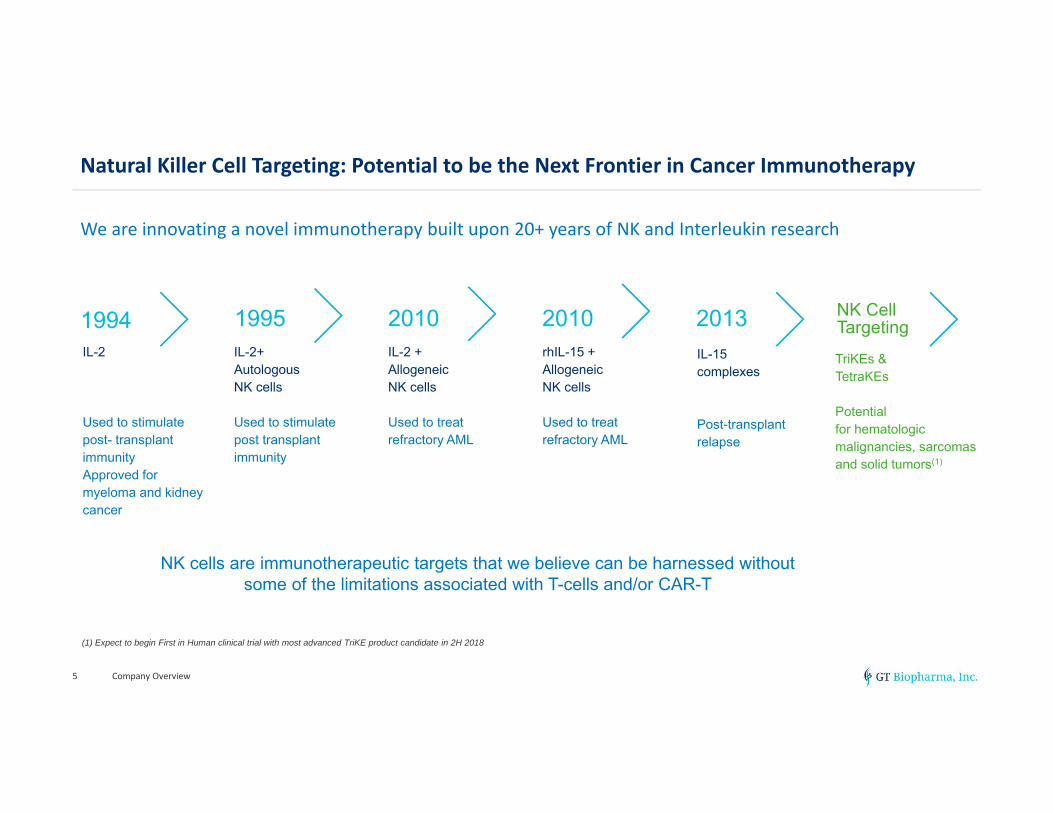
We are innovating a novel immunotherapy built upon 20+ years of NK and Interleukin research
IL-2
Used to stimulate post- transplant immunityApproved for myeloma and kidney cancer
1994IL-2+ AutologousNK cells
Used to stimulate post transplant immunity
1995IL-2 + AllogeneicNK cells
Used to treat refractory AML
2010rhIL-15 + Allogeneic NK cells
Used to treat refractory AML
2010IL-15 complexes
Post-transplant relapse
2013 NK Cell Targeting
NK cells are immunotherapeutic targets that we believe can be harnessed without some of the limitations associated with T-cells and/or CAR-T
TriKEs & TetraKEs
Potential for hematologic malignancies, sarcomas and solid tumors(1)
(1) Expect to begin First in Human clinical trial with most advanced TriKE product candidate in 2H 2018
Harnessing Natural Killer (NK) Cells to Fight Cancer
NK cells are cytotoxic lymphocytes of the innate immune system that have been increasingly recognized in immune surveillance against cancer
• Analogous to cytotoxic T cells in the adaptive immune response
• Provide rapid response to both viral infected cells and tumor cells
• Kill cancer cell by releasing cytotoxic granules
• TriKEs and TetraKEs designed to make NK cells antigen specific (targeted) yet do not require genetic manipulation
Company Overview6
Proprietary TriKEs and TetraKEs Have Potential Broad Applicability in Oncology
Company Overview7
Recombinant fusion proteins designed to harness NK cells, stimulate NK cell activity and proliferation,and target a specific tumor antigen
TriKEs and TetraKEs may have the potential to:
• Target a broad range of oncology indications including solid tumors
• Be dosed in an outpatient setting
• Be used alone or in combination regimens w/ potential to:
• Augment checkpoint inhibitors
• Be used in conjunction with more traditional cancer therapies
TriKE™ and TetraKE™ Technology Platform Highlights
Novel, scalable Tri- and Tetra-specific Natural Killer Cell Engagers (TriKEs™ & TetraKEs)
• Constructs designed to:• Bind to NK cell via CD16 receptor
• Provide activating cytokine (IL15) to stimulate NK cell activity and proliferation
• Regardless of NK-cell-inhibitor presence such as killer cell immunoglobulin-like receptor (KIR) ligands
• Target cancer cells for identification and attack by NK cells
Company Overview8
Antibody Directed Cell-Mediated Cytotoxicity (ADCC) scFvs
targeting CD33, CD133, EpCAM, among others
All TriKEs and TetraKEs contain:
NK Cell Ligand: CD16 (binding and activation)
IL-15 linker – NK cell activity & proliferation
Tumor Antigen Target(s)
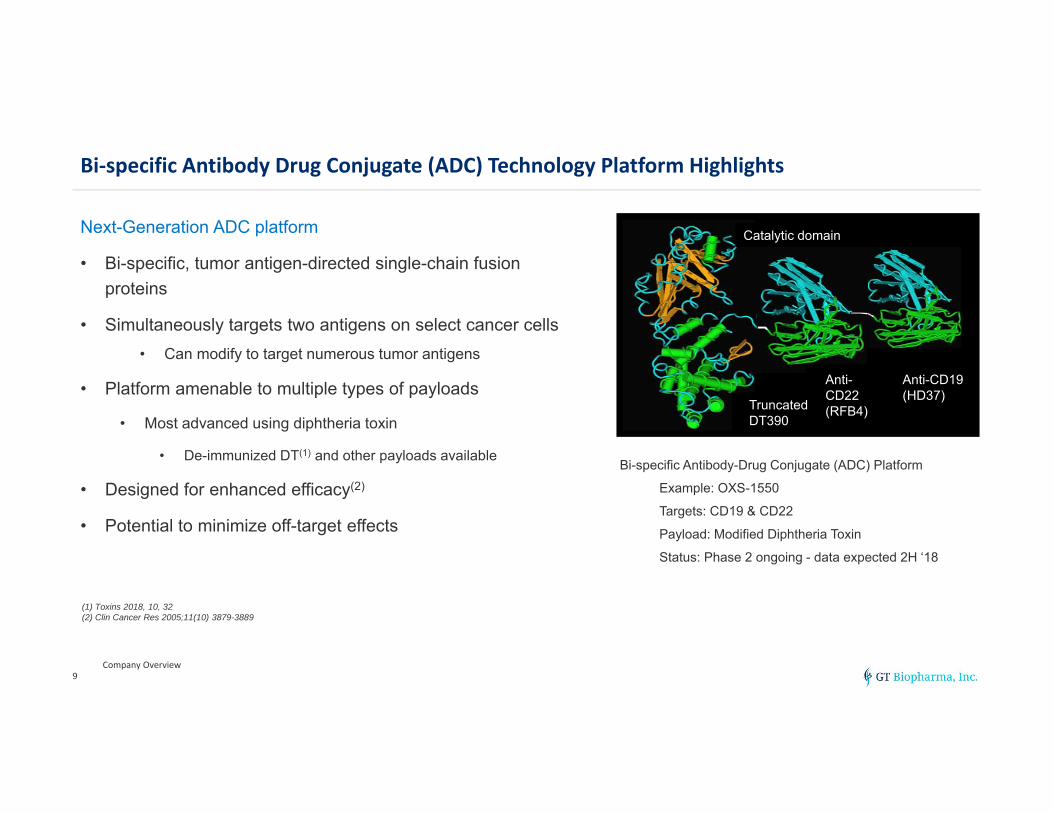
Bi‐specific Antibody Drug Conjugate (ADC) Technology Platform Highlights
Next-Generation ADC platform
• Bi-specific, tumor antigen-directed single-chain fusion proteins
• Simultaneously targets two antigens on select cancer cells• Can modify to target numerous tumor antigens
• Platform amenable to multiple types of payloads
• Most advanced using diphtheria toxin
• De-immunized DT(1) and other payloads available
• Designed for enhanced efficacy(2)
• Potential to minimize off-target effects
Company Overview9
Bi-specific Antibody-Drug Conjugate (ADC) Platform
Example: OXS-1550
Targets: CD19 & CD22
Payload: Modified Diphtheria Toxin
Status: Phase 2 ongoing - data expected 2H ‘18
translocationdomain
catalyticdomain
1st sFv 2nd sFv
translocationdomain
catalyticdomain
1st sFv 2nd sFvAnti-CD19(HD37)
TruncatedDT390
Anti-CD22(RFB4)
Catalytic domain
(1) Toxins 2018, 10, 32(2) Clin Cancer Res 2005;11(10) 3879-3889
Targeting Substantial Market Opportunities
• CD22+ and CD19+ hematological malignancies
• ~100,000 B-cell leukemia and lymphoma patients(1)
• ~30,000 CD33+ myeloid malignancies (AML & MDS)(1)
• Broad potential solid tumor applicability targeting multiple solid tumor antigens(1)
• >268,000 new breast cancers
• >230,000 new lung cancers
• >160,000 new prostate cancers
• >140,000 new colorectal cancers
• CD133 cancer stem cell marker
• Designed to target cancer stem cells which are resistant to current therapy(2)
Company Overview10
Our programs have the potential to provide meaningful patient benefit across many different types of cancers
Our platform technologies have the potential to treat large patient populations and substantial markets
(1) American Cancer Society: Cancer Facts and Figures 2018(2) Exp Hematol Oncol. 2013, 2:17
Company Overview11
Immuno‐Oncology Portfolio
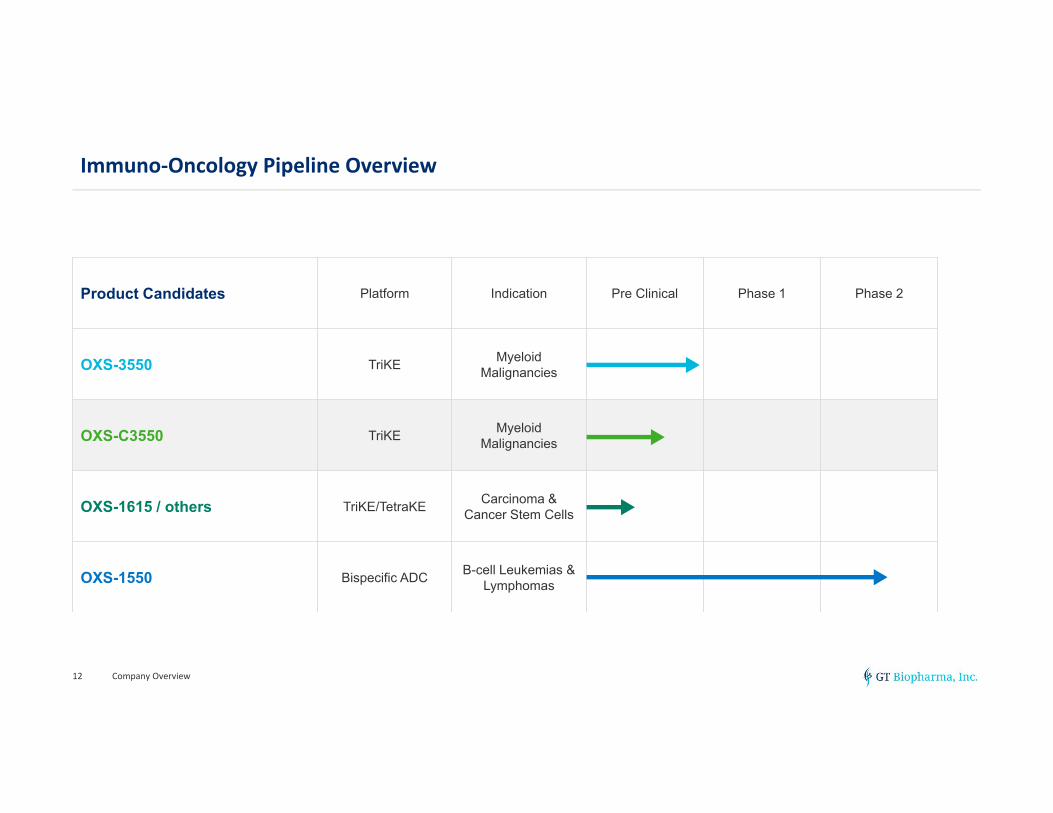
Immuno‐Oncology Pipeline Overview
Company Overview12
Product Candidates Platform Indication Pre Clinical Phase 1 Phase 2
OXS-3550 TriKE Myeloid Malignancies
OXS-C3550 TriKE Myeloid Malignancies
OXS-1615 / others TriKE/TetraKE Carcinoma & Cancer Stem Cells
OXS-1550 Bispecific ADC B-cell Leukemias & Lymphomas
Company Overview13
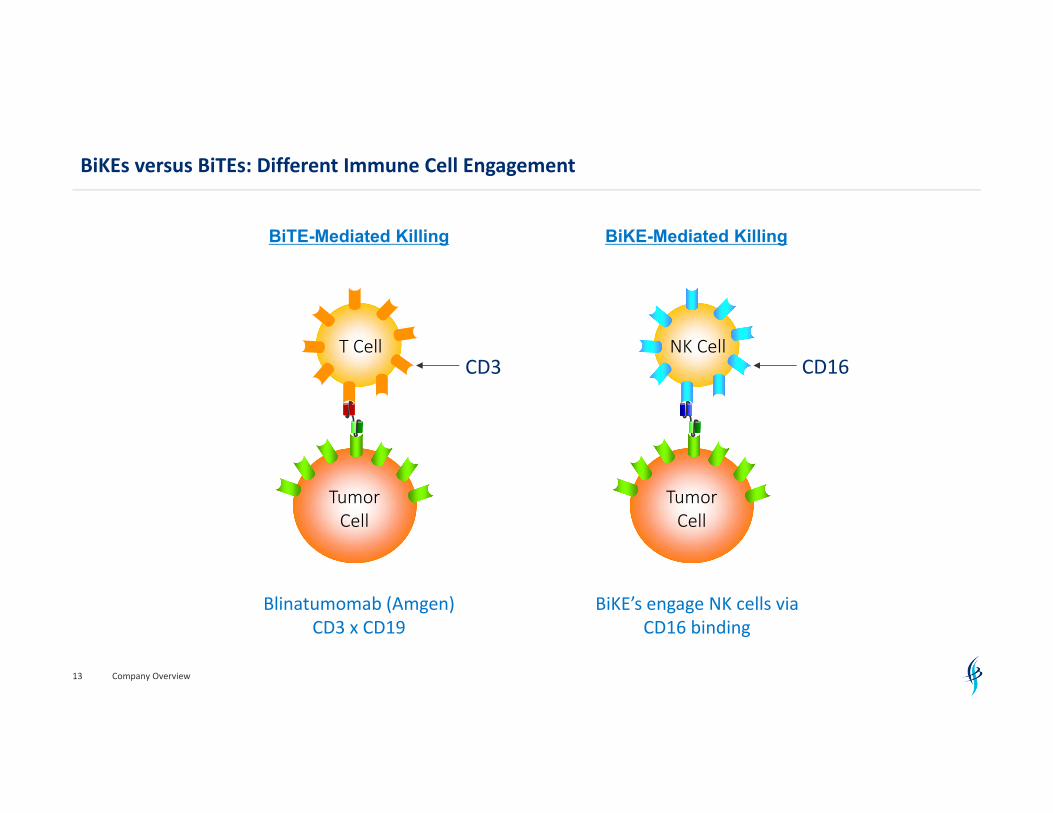
NK Cell
Tumor Cell
CD16
BiKE-Mediated Killing
T Cell
Tumor Cell
CD3
BiTE-Mediated Killing
Blinatumomab (Amgen)CD3 x CD19
BiKE’s engage NK cells via CD16 binding
BiKEs versus BiTEs: Different Immune Cell Engagement
Company Overview14
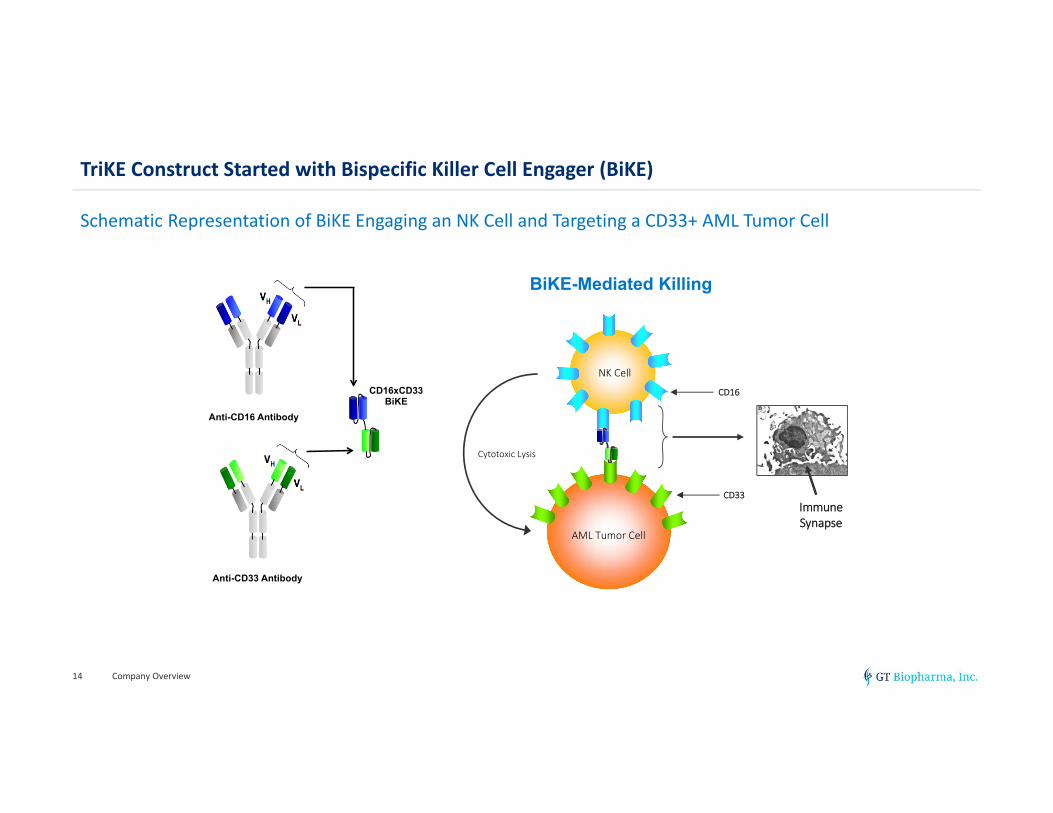
Anti-CD16 Antibody
Anti-CD33 Antibody
CD16xCD33 BiKE
NK Cell
AML Tumor Cell
CD16
CD33
Cytotoxic Lysis
BiKE-Mediated Killing
Immune Synapse
TriKE Construct Started with Bispecific Killer Cell Engager (BiKE)
Schematic Representation of BiKE Engaging an NK Cell and Targeting a CD33+ AML Tumor Cell
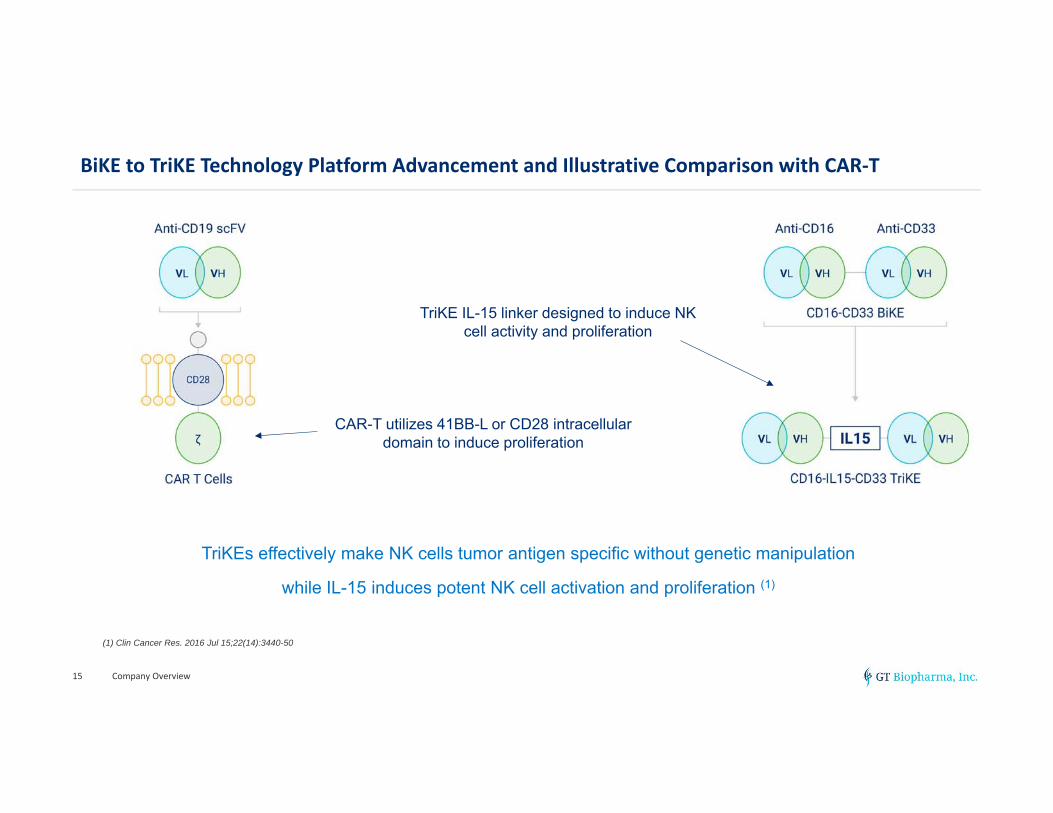
BiKE to TriKE Technology Platform Advancement and Illustrative Comparison with CAR‐T
Company Overview15
TriKEs effectively make NK cells tumor antigen specific without genetic manipulation
while IL-15 induces potent NK cell activation and proliferation (1)
TriKE IL-15 linker designed to induce NK cell activity and proliferation
CAR-T utilizes 41BB-L or CD28 intracellular domain to induce proliferation
(1) Clin Cancer Res. 2016 Jul 15;22(14):3440-50
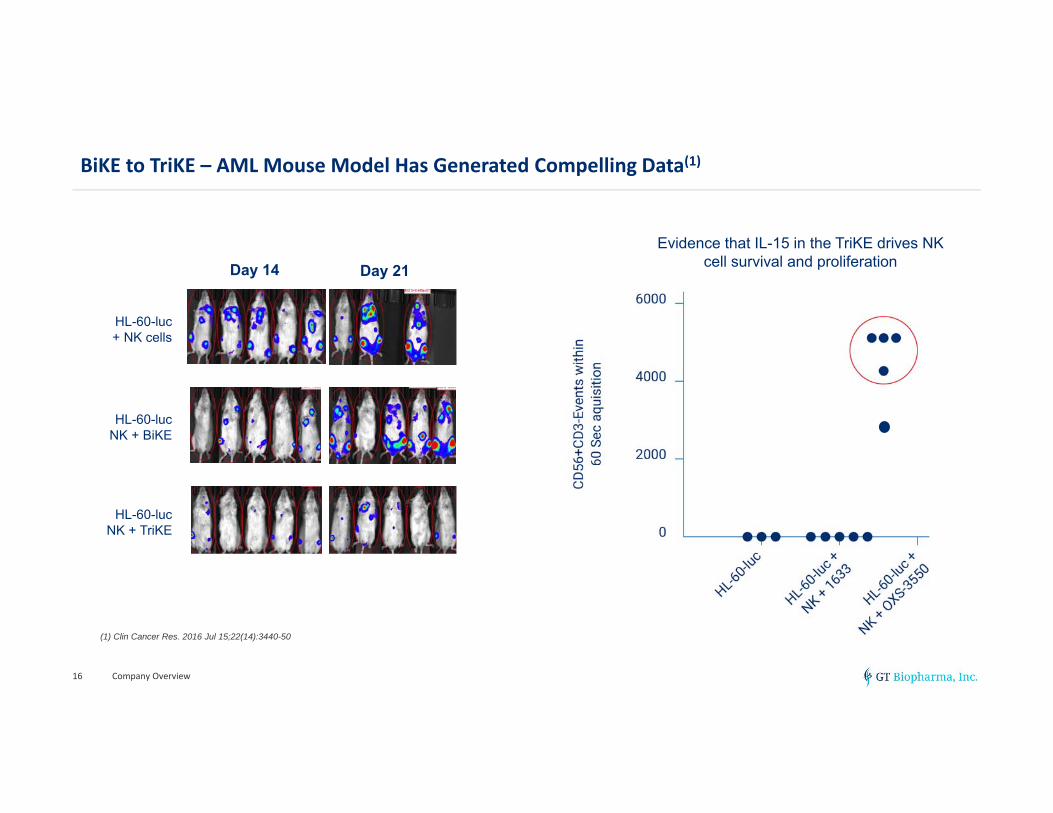
BiKE to TriKE – AML Mouse Model Has Generated Compelling Data(1)
Company Overview16
Day$21$Image!Day$14$Image!
M1$$$$$$$$$$$M2 $$$$$$$$$$M3$ $M4 $$$$$M5$ M1$$$$$$$$$M2 $$$$$M3$$$$$$$M4 $$$$$$$$M5$
M6$$$$$$$$$$$M7 $$$$$$$$$$M8$ $M9 $$M10$ M6$$$$$$$$$M7 $$$$$M8$$$$$$$M9 $$$$$$$$M10$
M11$$$$$$$$M12$$$$$$$M13$$$$$$M14 $$M15$ M11$$$$M12 $$$$M13$$$$$$$M14$$$$$$M15$
HL-60-luc
HL-60-luc +NK +1633
HL-60-luc +NK +
161533
HL-60-lucNK + TriKE
HL-60-lucNK + BiKE
HL-60-luc + NK cells
Day 14 Day 21
Evidence that IL-15 in the TriKE drives NK cell survival and proliferation
(1) Clin Cancer Res. 2016 Jul 15;22(14):3440-50
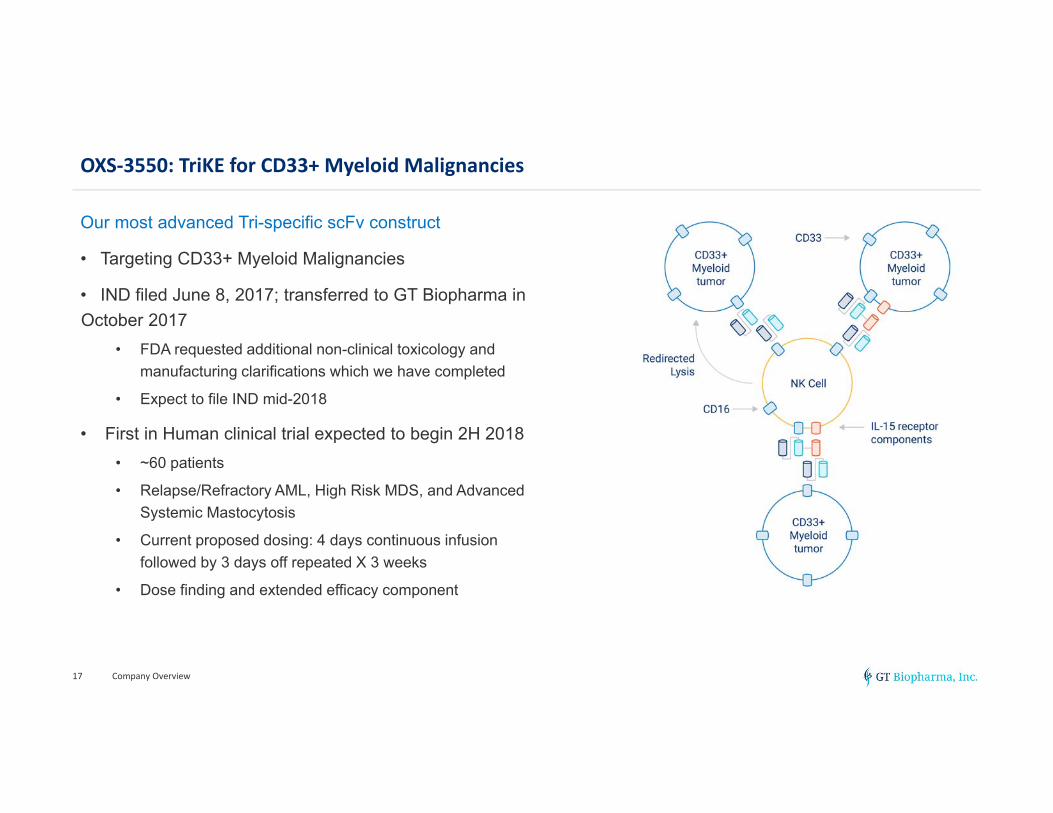
OXS‐3550: TriKE for CD33+ Myeloid Malignancies
Our most advanced Tri-specific scFv construct
• Targeting CD33+ Myeloid Malignancies
• IND filed June 8, 2017; transferred to GT Biopharma in October 2017
• FDA requested additional non-clinical toxicology and manufacturing clarifications which we have completed
• Expect to file IND mid-2018
• First in Human clinical trial expected to begin 2H 2018• ~60 patients
• Relapse/Refractory AML, High Risk MDS, and Advanced Systemic Mastocytosis
• Current proposed dosing: 4 days continuous infusion followed by 3 days off repeated X 3 weeks
• Dose finding and extended efficacy component
Company Overview17
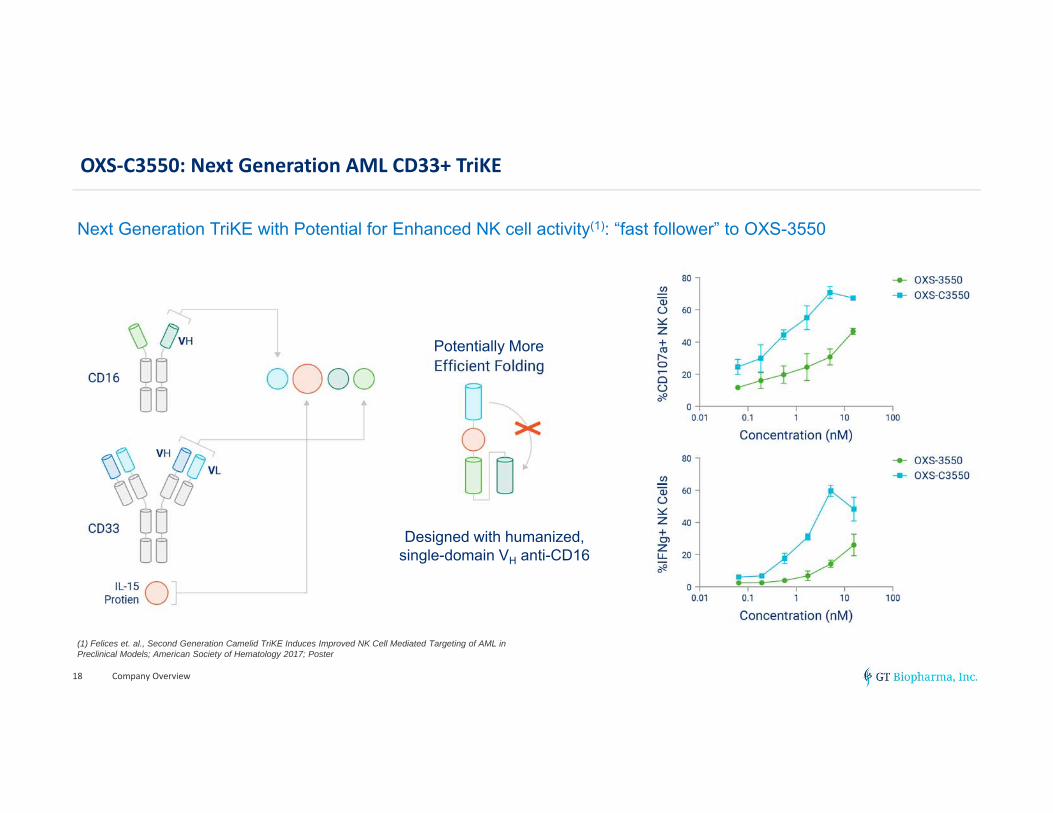
OXS‐C3550: Next Generation AML CD33+ TriKE
Company Overview18
Next Generation TriKE with Potential for Enhanced NK cell activity(1): “fast follower” to OXS-3550
Designed with humanized, single-domain VH anti-CD16
(1) Felices et. al., Second Generation Camelid TriKE Induces Improved NK Cell Mediated Targeting of AML in Preclinical Models; American Society of Hematology 2017; Poster
Potentially More
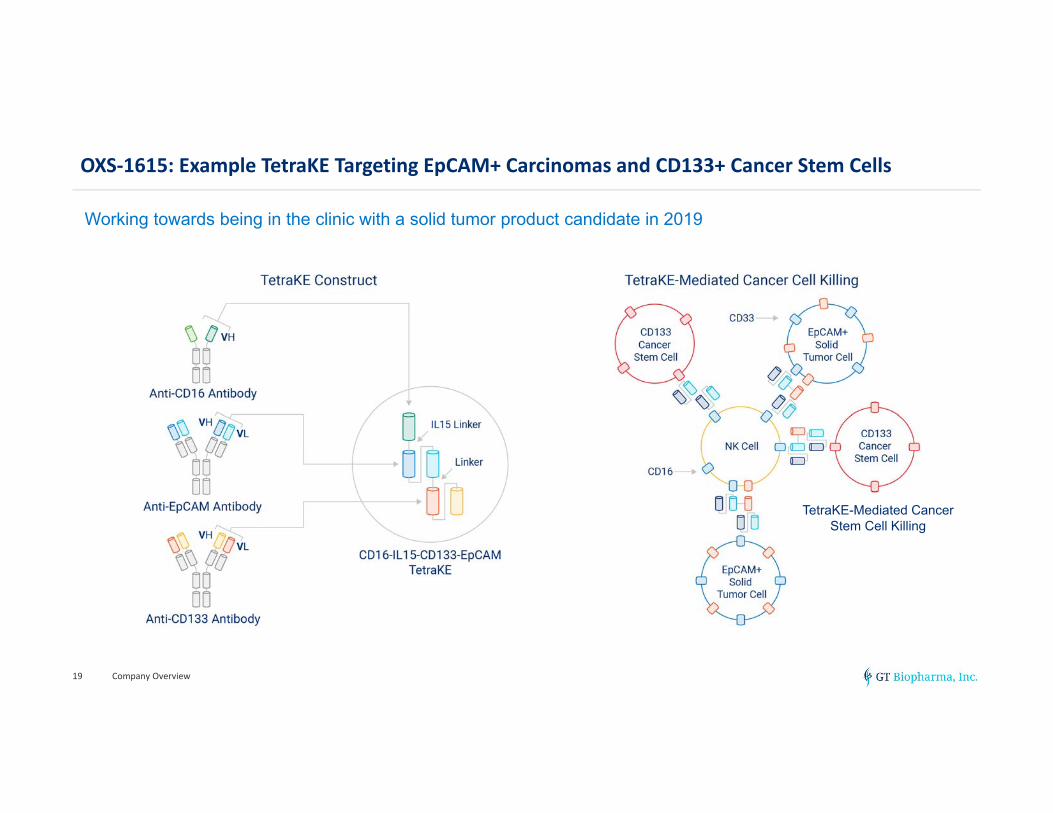
OXS‐1615: Example TetraKE Targeting EpCAM+ Carcinomas and CD133+ Cancer Stem Cells
Company Overview19
Working towards being in the clinic with a solid tumor product candidate in 2019
TetraKE-Mediated Cancer Stem Cell Killing
Potential Benefits of TriKE and TetraKE Therapeutics
• Designed to be an off-the-shelf drug
• Tumor antigen targeting without the need for genetic modifications as in certain cell therapies
• Potential in hematologic and solid tumors
• Expected convenience and flexibility
• Dosing expected to be easily adjustable
• Broad potential applicability
• Attractive bio-distribution; important for solid tumor potential
• Non-immunogenic and quick clearance properties
• Can be engineered to target a variety of tumor antigens
• Estimated lower COGS and less labor intensive than cell therapies
Company Overview20
“TriKEs are the protein version of CAR-T with multiple clinical and practical advantages”Dr. Jeffrey Miller Deputy Director of the Masonic Cancer Center, University of Minnesota
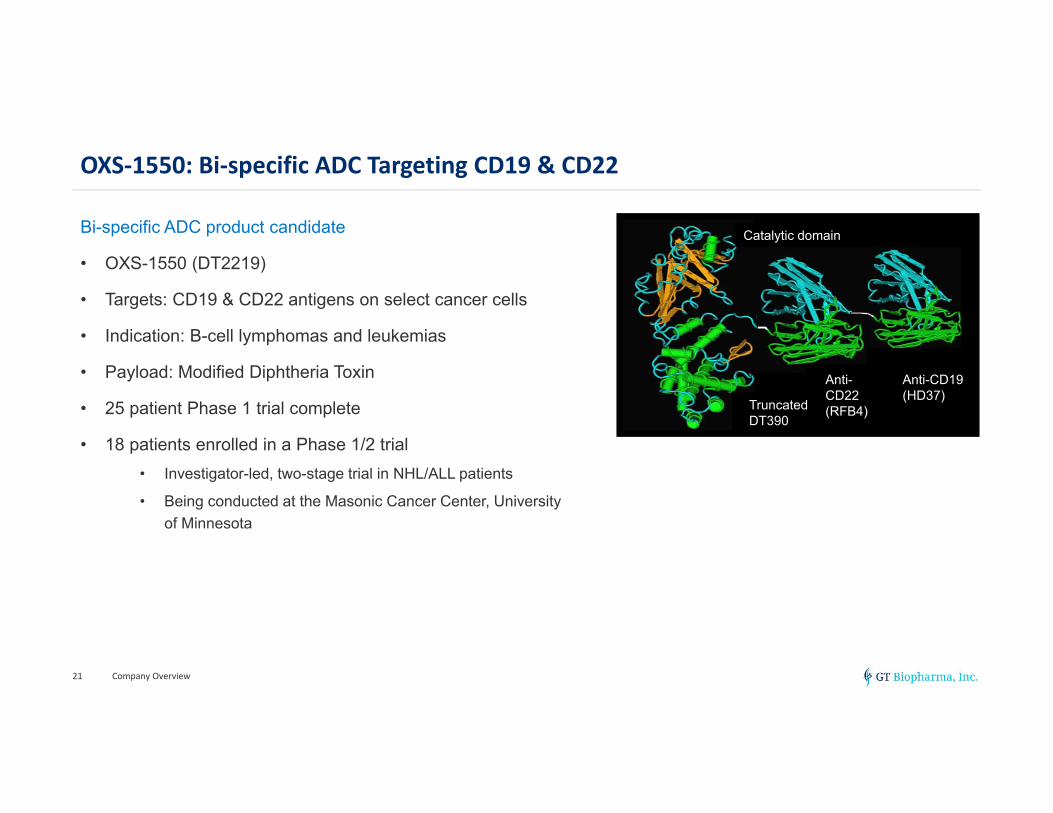
OXS‐1550: Bi‐specific ADC Targeting CD19 & CD22
Bi-specific ADC product candidate
• OXS-1550 (DT2219)
• Targets: CD19 & CD22 antigens on select cancer cells
• Indication: B-cell lymphomas and leukemias
• Payload: Modified Diphtheria Toxin
• 25 patient Phase 1 trial complete
• 18 patients enrolled in a Phase 1/2 trial• Investigator-led, two-stage trial in NHL/ALL patients
• Being conducted at the Masonic Cancer Center, University of Minnesota
Company Overview21
translocationdomain
catalyticdomain
1st sFv 2nd sFv
translocationdomain
catalyticdomain
1st sFv 2nd sFvAnti-CD19(HD37)
TruncatedDT390
Anti-CD22(RFB4)
Catalytic domain
OXS‐1550: Phase 1 Trial Design(1)
OXS-1550 Phase 1 trial design overview
• 25 patients enrolled across 9 dose cohorts
• 10 ALL, 10 NHL & 5 CLL
• 0.5 -80 µg/kg/day i.v. over 2 hours every other day (qod)
• Minimum of 3 prior lines w/ 8 failed hematopoietic stem cell transplant (HSCT)
• 12 patients treated at 0.5-20 µg/kg/day qod had no detectable drug levels
• 13 patients treated at >40 µg/kg/day qod
• 9 had measurable drug levels
Company Overview22
(1) Bachanova et. al., Clin Cancer Res. 2015 March 15; 21(6): 1267–1272.
OXS‐1550: Phase 1 Highlights(1)
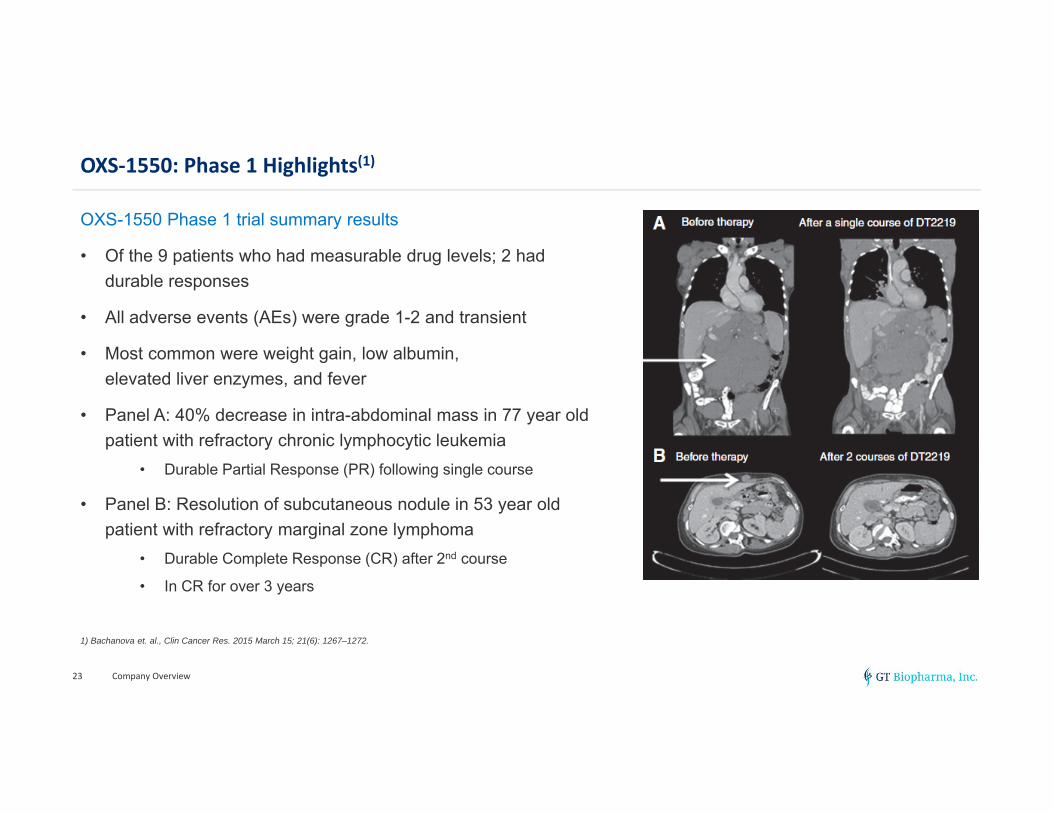
OXS-1550 Phase 1 trial summary results
• Of the 9 patients who had measurable drug levels; 2 had durable responses
• All adverse events (AEs) were grade 1-2 and transient
• Most common were weight gain, low albumin, elevated liver enzymes, and fever
• Panel A: 40% decrease in intra-abdominal mass in 77 year old patient with refractory chronic lymphocytic leukemia
• Durable Partial Response (PR) following single course
• Panel B: Resolution of subcutaneous nodule in 53 year old patient with refractory marginal zone lymphoma
• Durable Complete Response (CR) after 2nd course
• In CR for over 3 years
Company Overview23
1) Bachanova et. al., Clin Cancer Res. 2015 March 15; 21(6): 1267–1272.
OXS‐1550: Phase 1/2 Trial Design – currently in Phase 2 component (1)
Company Overview24
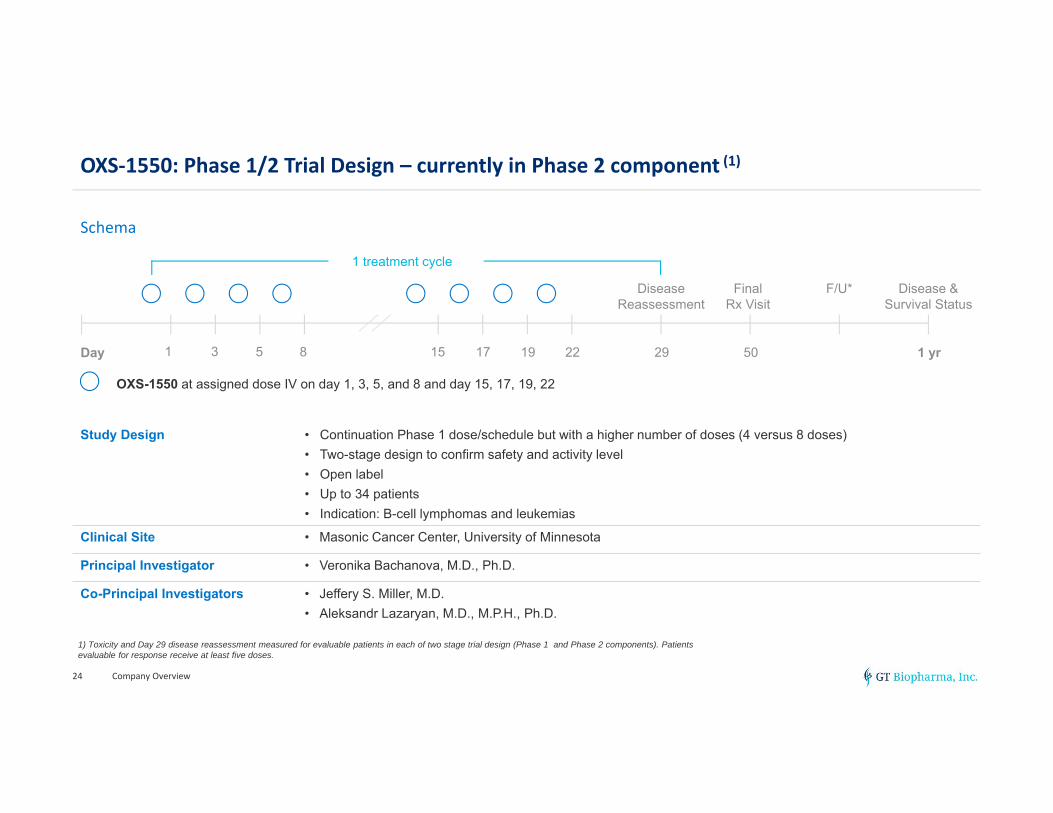
Schema
1 3 5 8 15 17 19 22 29 50 1 yrDay
Disease Reassessment
FinalRx Visit
F/U* Disease &Survival Status
OXS-1550 at assigned dose IV on day 1, 3, 5, and 8 and day 15, 17, 19, 22
1 treatment cycle
Study Design • Continuation Phase 1 dose/schedule but with a higher number of doses (4 versus 8 doses)• Two-stage design to confirm safety and activity level• Open label• Up to 34 patients• Indication: B-cell lymphomas and leukemias
Clinical Site • Masonic Cancer Center, University of Minnesota
Principal Investigator • Veronika Bachanova, M.D., Ph.D.
Co-Principal Investigators • Jeffery S. Miller, M.D.• Aleksandr Lazaryan, M.D., M.P.H., Ph.D.
1) Toxicity and Day 29 disease reassessment measured for evaluable patients in each of two stage trial design (Phase 1 and Phase 2 components). Patients evaluable for response receive at least five doses.
OXS‐1550: Preliminary Clinical Results from Phase 1/2 Interim Data Review
• Data snapshot included review of toxicity profile, disease reassessment at Day 29• 13 patients met evaluation criteria of at least 5 doses – 4 ALL, 9 NHL
• >50% of patients (7 of 13) exhibited clinical benefit as defined by stable disease, partial remission or complete response at Day 29
• Efficacy signal most pronounced in ALL• 75% (3 of 4) exhibiting clinical benefit – 1CR, 1PR and 1SD
• Bi-specific ADC Advisory Board recommendation to enroll additional ALL patients
• Adverse events were mostly grade-1 and grade-2 and reversible• Four patients with dose limiting toxicity – 1 grade-4 low platelet count, 2 grade-3 increase liver function tests
and 1 grade-3 capillary leak
• Bi-specific ADC Clinical Advisory Board• Masonic Cancer Center -- Dr. Jeffrey Miller, Deputy Director, Dr. Veronika Bachanova, Dr. Daniel Vallera• Dr. Mark R. Litzow, M.D., Professor of Medicine in the Division of Hematology at Mayo Clinic• Dr. Arthur E. Frankel, M.D., Chief of Medical Oncology at Mitchell Cancer Institute (USA-MCI)
Company Overview25
Note: Toxicity and Day 29 disease reassessment measured for evaluable patients in each of two stage trial design (Phase 1 component and Phase 2 component). Patients evaluable for response receive at least five doses. Expect to enroll additional ALL patients.
CNS Pipeline Summary
• ~60,000 patients in US
• Patients can become wheelchair bound
• Pyridostigmine is the primary drug prescribed for treatment of muscle weakness
• GI side effects may lead to non-compliance or decreased dose
• Fixed dose combination of pyridostigmine and ondansetron
• IND filed – results of POC study announced 1Q 2018
Company Overview26
• ~16 MM diagnosed in US
• Peak dose-limiting side effects of carbamazepine may cause patients to be under-dosed
• Patented protected tablet designed to provide frequent, small accurate doses
• 72-hour patch containing a potent selective muscarinic receptor antagonist
• Does not act in the brain
• Current SOC for prevention is 72 hour scopolamine patch
• Acts both in and outside the brain
• Can cause sedation and cognition effects
• Investigator-led concept study – data and next steps expected 2H 2018
GTP‐004Myasthenia Gravis
PainBrakeChronic Neuropathic Pain
GTP‐011 Motion Sickness
2018 Milestones/Catalysts for Growth
• Applied for NASDAQ uplisting
• OXS-3550 expectations
• IND filing mid-2018
• Begin First-in-Human clinical trial 2H ’18
• OXS-1550
• Final data expected 4Q ’18 or 1Q ’19
• Planning End-of-Phase 2A meeting with FDA in first half of 2019
• OXS-C3550 IND-enabling studies & TetraKE pre-clinical program
• CNS – next steps and concept study results
• Other potential corporate and business development opportunities
Company Overview27
Management Team with Track Record of Success
Company Overview28
Raymond W. Urbanski, M.D., Ph.D.Chairman and Chief Executive Officer
• 25+ years of pharmaceutical, drug development and management experience
• Chief Medical Officer, MannKind Corporation
• Chief Medical Officer, Mylan
• Vice President, Business Unit CMO and Sr. Medical Director, Oncology Clinical R&D at Pfizer
Kathleen Clarence-Smith, M.D., Ph.D.Vice Chairman and President Neurology Division
• Founder and CMO, Chase Pharmaceuticals (acquired by Allergan for up to $1B in 2016) and Founder and CEO, Prestwick Pharmaceuticals (acquired by Biovail)
• Worldwide Head of CNS Development at Otsuka, Hoffmann-La Roche and Worldwide Head of CNS at Sanofi
Steven Weldon, MBA, CPAChief Financial Officer
• 15+ years of financial and accounting experience with public and private companies. CPA licensed to practice in the state of Florida.
Independent Directors with Relevant Experience
Company Overview29
Geoffrey B. Davis, Esq. • Founding partner Barker Davis, LLC
• Ropes & Gray, LLC; partner for over 25 years; significant role in establishing internationally recognized Life Sciences group
• Numerous corporate partnering, licensing, capital markets and strategic transactions for major pharmaceutical companies (e.g. Pfizer), and public and private biotechnology companies
Peter Kiener, D.Phil. • Most recently Chief Scientific Officer at Sucampo; sold to Mallinckrodt for ~$1.2bn
• Formerly Chief Scientific Officer of Ambrx Inc. (Antibody Drug Conjugate company) and Executive Vice President and Global Head of Biologics Research and Development, MedImmune LLC
• 20+ years experience in all aspects of drug development, including discovery, regulatory approval, and post marketing and execution of multiple deal types, including private placements, IPO, M&A, strategic partnerships, and licensing deals; NK experience (board of NKT)
John N Bonfiglio, Ph.D., MBA • 30+ years of pharmaceutical and management experience including President, COO and CEO roles
• President and COO of TapImmune Inc.; previous Board member
• Previous President and CEO of Oragenics, Argos Therapeutics and The Immune Response Corporation
Advisors Provide Additional Resource Depth
Company Overview30
Oncology Scientific Advisory Board
Jeffrey Miller, M.D. • Professor of Medicine, Division of Hematology, Oncology and Transplantation University of Minnesota, Masonic Cancer Center
Bruce Blazar M.D. • Professor of Pediatrics, Division of Blood and Marrow Transplantation, University of Minnesota
James J. Mulé, Ph.D. • Associate Center Director and Michael McGillicuddy Endowed Chair in Melanoma Research/Treatment at Moffitt Cancer Center
Robin Parihar, M.D., Ph.D. • Assistant Professor, Department of Pediatrics, Section of Pediatric Hematology-Oncology Center for Cell and Gene Therapy Texas Children's Hospital Baylor College of Medicine
Ad Hoc Oncology Scientific Advisory Board Members
Sarah Cooley, M.D., M.S. • Associate Professor of Medicine, Division of Hematology, Oncology and Transplantation, Director of Investigator Initiated Clinical Research, Masonic Cancer Center
Martin Felices, Ph.D. • Assistant Professor of Medicine, Co-director of the Translational Therapy Laboratory, Division of Hematology, Oncology, and Transplantation, University of Minnesota





























