Embed Size (px)
Citation preview
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines January 2011
1 of 21
Diphtheria
Case Definition
Confirmed Case Clinical Illness[1] or systemic manifestations compatible with diphtheria in a person with an upper respiratory tract infection or infection at another site [2] PLUS at least one of the following: Laboratory confirmation of infection using the modified ELEK assay or assay for presence of
the diphtheria tox gene, which, if detected, should be tested for expression of diphtheria toxin using the modified ELEK assay: o isolation of Corynebacterium diphtheriae with confirmation of toxin from an appropriate
clinical specimen, including the exudative membrane OR o Histopathologic diagnosis of diphtheria
OR Epidemiological link to a laboratory-confirmed case. (contact within 2 weeks prior to onset of
symptoms)
Probable Case Clinical illness[1] in the absence of laboratory confirmation or epidemiologic link to a laboratory-confirmed case. Suspect Case Upper respiratory tract infection (naso-pharyngitis, laryngitis, or tonsillitis) with nasal, tonsillar, pharyngeal and/or laryngeal membrane.
[1]Clinical illness is characterized as an upper respiratory tract infection (naso-pharyngitis, laryngitis, or tonsillitis) with or without an adherent nasal, tonsillar, pharyngeal and/or laryngeal membrane plus at least one of the following:
Gradually increasing stridor Cardiac (myocarditis) and/or neurological involvement (motor and/or sensory palsies) 1 to 6 weeks after
onset Death, with no known cause.
[2] Infection at another site includes any site that is not in the respiratory tract (e.g. wound, cutaneous, etc)
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 2 of 21
Reporting Requirements 1. Physicians/Health Practitioners and Others
Physicians, health practitioners and others listed in Section 22 of the Public Health Act shall notify the Medical Officer of Health (MOH) (or designate) of all confirmed, probable, and suspect cases by the fastest means possible (FMP) i.e., direct voice communication.
2. Laboratories
All laboratories (including regional laboratories and the PLPH) shall report all positive laboratory results by the fastest means possible i.e., direct voice communication to the: Chief Medical Officer of Health (CMOH) (or designate), MOH (or designate) and Attending/ordering physician. Lab Surveillance ONLY: Isolation of other toxigenic Corynebacterium species (C. ulcerans or C. pseudotuberculosis) from an appropriate clinical specimen, including the exudative membrane.
N.B. Faxed reports to CMOH (or designate) containing C. ulcerans or C.pseudotuberculosis are acceptable.
3. Alberta Health Services The MOH (or designate) shall notify the CMOH (or designate) of all confirmed, probable and
suspect cases by FMP. The MOH (or designate) shall forward the preliminary NDR of all confirmed, probable and
suspect cases to the CMOH (or designate) within seven days (one week) of notification and the final NDR (amendments) within two weeks of notification.
For out-of-zone reports, the MOH (or designate) first notified shall notify the MOH (or designate) where the client resides by FMP and immediately fax a copy of the positive laboratory report.
For out-of-province and out-of-country reports, the following information should be forwarded to the CMOH (or designate) by FMP including: o name, o date of birth, o out-of-province health care number, o out-of-province address and phone number, o attending physician (locally and out-of-province), o positive laboratory report faxed, o and contact information (if applicable).
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 3 of 21
Etiology (1;2)
Diphtheria is caused by toxigenic strains of Corynebacterium diphtheriae. C. diphtheriae is an irregularly staining, gram-positive, non-spore-forming, non-motile, pleomorphic bacillus with four biotypes (mitis, intermedius, belfanti and gravis). Toxigenic strains express an exotoxin that inhibits cellular protein synthesis and is responsible for local tissue destruction and membrane formation. The toxin produced at the membrane site is absorbed into the bloodstream and then distributed to the tissues. The most severe disease is associated with the gravis biotype, but any biotype may produce the toxin. Non-toxin producing strains generally produce milder illness. Clinical Presentation (1–17)
Diphtheria is an acute bacterial disease that can involve almost any mucous membrane. The characteristic lesion, caused by liberation of a specific cytotoxin, is marked by a patch or patches of an adherent grayish-white membrane with surrounding inflammation. The infection most often manifests as membranous naso-pharyngitis or obstructive laryngotracheitis. The toxin produced by some strains can cause severe damage to the throat or other tissues. Occasionally, C. diphtheriae disseminates from the skin or respiratory tract and causes invasive systemic infections including bacteremia, endocarditis and arthritis. Diphtheria can be classified based on site of infection:
Pharyngeal/tonsillar: This is the most common site of infection and is associated with the absorption of toxin. The onset is insidious. Early symptoms include malaise, sore throat, anorexia and low-grade fever. Two to three days later the membrane appears in the pharyngeal/tonsillar area. The membrane initially appears white and glossy, but evolves into a dirty gray color with patches of green or black necrosis. The extent of the membrane correlates with the severity of symptoms (i.e., with posterior pharynx, soft palate and periglottal area involvement, profound malaise and obstructed breathing may occur). In cases of severe disease the individual may also develop edema of the submandibular areas and the anterior neck, along with lymphadenopathy, giving the characteristic “bullneck” appearance. The individual may recover or, depending on the amount of toxin absorbed, develop severe illness, pallor, rapid pulse, stupor and coma with death occurring in six to 10 days. Nasal: Infection limited to the anterior nares presents with a serosanguinous or seropurulent nasal discharge often associated with a subtle whitish mucosal membrane, particularly on the septum. Signs indicating toxin effect are rare. Laryngeal: This may be either an extension of the pharyngeal form or be the only site involved. Symptoms include fever, hoarseness and a barking cough. Development of the membrane may lead to airway obstruction, coma, and death. Cutaneous: C. diphtheriae can cause clinical skin infections characterized by a scaling rash or by chronic non-healing ulcers with a dirty gray membrane and are often associated with Staphylococcus aureus and group A streptococci. This type of diphtheria is often associated with overcrowding, impoverished groups and homeless persons. Cutaneous sites of C. diphtheriae have been shown both to contaminate the inanimate environment and to induce throat infections in others. Bacterial shedding from cutaneous infections continues longer than from the respiratory tract. Because C. diphtheriae is usually isolated in association with other known skin pathogens, and because the ulcers do not respond to antitoxin therapy, there is debate as to whether or not the isolates are actually causing clinical illness.
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 4 of 21
Invasive Disease: Complications are predominantly attributable to the effects of the toxin. The two most common complications are myocarditis and neuritis. In most cases, the cardiac manifestations appear during the latter part of disease progression. The more extensive the local lesion and the more delayed the initiation of antitoxin therapy, the more frequently myocarditis occurs. Neuritis most often affects motor nerves and usually resolves completely. Other complications include otitis media and respiratory insufficiency due to airway obstruction, especially in infants. (2;10–18)
Diagnosis (17;18)
Diagnosis is usually made based on history and clinical presentation as it is essential to begin therapy as soon as possible. Diphtheria should be suspected based on the following clinical clues:
mildly painful tonsillitis and/or pharyngitis with associated membrane, especially if the membrane extends to the uvula and soft palate;
adenopathy and cervical swelling, especially if associated with the membranous pharyngitis and signs of systemic toxicity;
hoarseness and stridor; palatal paralysis; serosanguinous nasal discharge with associated mucosal membrane; and temperature elevation rarely in excess of 39.4ºC (103ºF).
The differential diagnosis includes infectious mononucleosis, streptococcal or viral pharyngitis and tonsillitis, Vincent’s angina and acute epiglotitis. The role of the laboratory in the diagnosis of diphtheria is to assist the clinicians in confirming their clinical diagnosis. Diagnosis is confirmed by bacteriologic examination of specimens. Call the Microbiologist on call at Provincial Laboratory Public Health (PLPH) prior to specimen collection. Cultures of lesions, if present and the nasopharynx are done to confirm the diagnosis. Swab(s) from the nasopharynx, especially the membrane, is essential. Isolates should be tested for toxigenicity. Toxigenicity tests require an additional 48 to 72 hours. Epidemiology (4;5;6;18–29)
Reservoir Humans Transmission The most common modes of spread are via respiratory droplets or direct contact with either respiratory secretions or exudate from infected skin lesions. Close face to face contact with a case or carrier is usually required in order for transmission to occur. Fomites can play a role in transmission, and epidemics have been caused by contaminated milk. Articles soiled with discharges from infected lesions are also potential sources of transmission. Most respiratory disease occurs in the colder months in temperate climates and is associated with crowded indoor living conditions and hot dry air. Sporadic cases most often result from exposure to carriers who are asymptomatic as these carriers are responsible for perpetuating the spread of disease. Exact carriage rates are unknown but in endemic areas 3–5% of healthy individuals may harbour the organism in their throats.(19) Skin infection, which was thought to be primarily a problem in tropical environments, has caused recent epidemics in Europe and North America among destitute inner city dwellers and substance
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 5 of 21
abusers.(4;21) Skin carriage can become a silent reservoir for the organism and it has been shown that person to person transmission from infected skin sites is more efficient than from the respiratory tract.(5;8)
Incubation Period Typically two to five days with a range of one to 10 days. Period of Communicability Transmission may occur as long as virulent bacilli are present in discharges and lesions: two weeks or less and seldom more than four weeks without treatment. With appropriate antibiotic therapy, persons are usually communicable for fewer than four days. Occasionally, chronic carriage occurs even after treatment. Chronic carriers may shed the organism for six months or more. Host Susceptibility Infection can occur in immunized as well as unimmunized persons. Lifelong immunity is generally (but not always) acquired following disease or inapparent infection. Prior immunization reduces the frequency and severity of disease and carriage. Immunization provides prolonged but not lifelong immunity. The protection is antibody related and immunity is primarily against the toxin rather than the bacteria; therefore, immune persons can still harbour the organism. There is no clearly defined level of antitoxin demonstrated to provide complete protection. Levels between 0.01 IU/mL and 0.09 IU/mL are regarded as providing basic immunity, while levels of > 0.1 IU/mL may be needed for full protection.(30) Additional factors that may increase an individual’s susceptibility include the dose and virulence of the bacteria, as well as the person’s general immune status. Occurrence (2;22;31–34)
General Diphtheria is typically a disease of colder months in temperate climates. Cutaneous diphtheria is more common in the tropics where seasonal trends are less distinct. Those affected most commonly are unimmunized children under 15 years of age or groups of adults whose immunization has been neglected. Diphtheria is rare in countries where children and adults are immunized. The overall case-fatality rate for diphtheria has changed very little in the past 50 years and is between 5–10%, with higher rates (up to 20%) among persons younger than 5 or older than 40 years of age. Diphtheria is uncommon in industrialized countries, such as the United States and Canada, where routine immunization has virtually eliminated endemic disease. From 1980 to 2004 an average of two to three cases per year were reported in the United States. The majority of individuals affected were 20 years of age or older. In the early 1990s, numbers began to reach epidemic proportions in the Newly Independent States (NIS), formerly the Soviet Union, particularly the Russian Federation and Ukraine. From 1990 to 1995 approximately 157,000 cases and 5,000 deaths were reported from the NIS. The NIS accounted for more than 90% of worldwide diphtheria cases reported to the World Health Organization. The outbreak and the age distribution of cases are believed to be due to several factors, including a lack of routine immunization of adults in these countries.
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 6 of 21
Canada The highest ever recorded number of diphtheria cases in Canada was in 1924 when approximately 9,000 cases were reported. In 1926, diphtheria toxoid was licensed for use in Canada and was introduced as routine immunization in 1930. This led to a substantial decline in diphtheria morbidity and mortality. Since 1983, there have been fewer than five cases reported per year and no deaths, with only one case per year in 2002–2004. The majority of cases have occurred in adults ( 20 years old) without adequate immunization. Alberta (36) Between 1981 and 2003, there were five cases reported (two in 1982, one in 1984, one in 1986 and one in 1989) and four carriers (one in 1990, one in 1992, two in 1994). Two cases of cutaneous diphtheria were reported, one in 2004 and one in 2007. Both individuals indicated that they remembered being immunized as children but documented proof of immunization could not be produced.
Key Investigation (35;37–45) Rapid clinical and public health responses are required to control diphtheria. The two primary goals of investigation are:
prompt diagnosis and management of case(s) and rapid identification of close contacts with their effective management in order to prevent
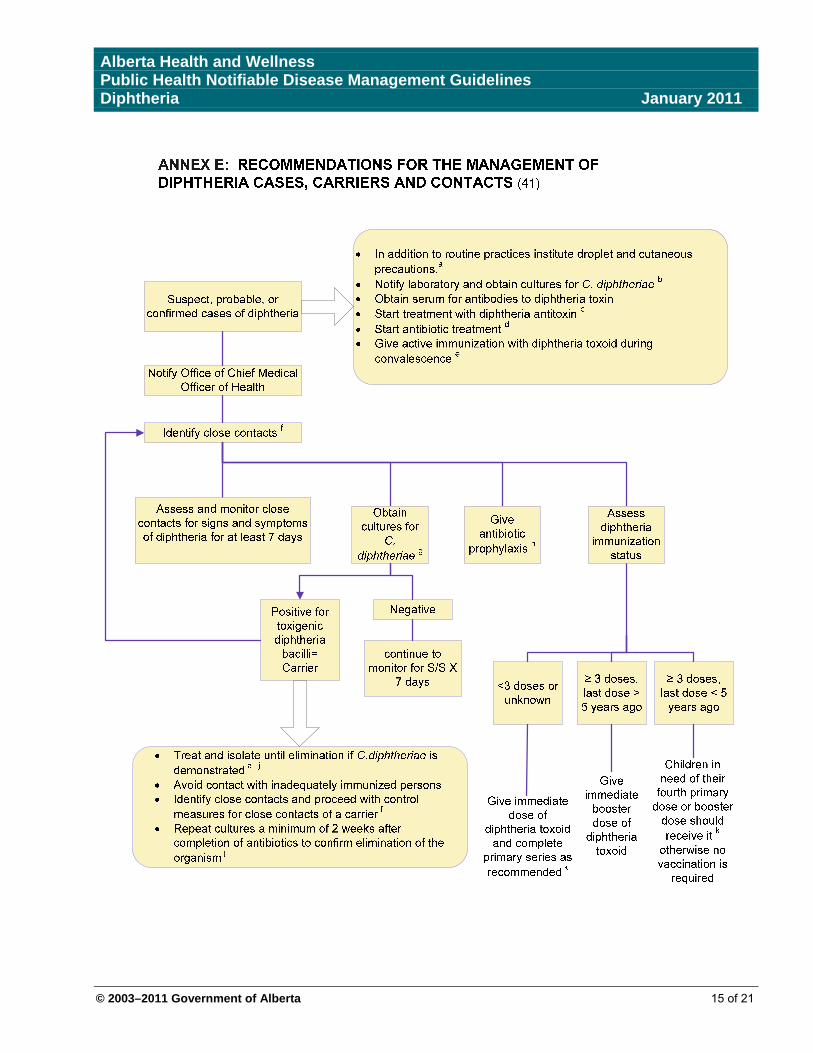
secondary cases. Refer to Annex E: Recommendations for the Management of Diphtheria Cases, Carriers and Contacts for summary. Single Case/Household Cluster Confirm the diagnosis and strain. Notify Provincial Laboratory for Public Health (PLPH) as soon as diagnosis is suspected.
o The successful isolation of C.diphtheriae depends of the rapid inoculation of special culture media.
Take throat, nasopharyngeal swabs and/or lesion swabs prior to commencing antibiotic therapy. o If membrane is present, sample the membrane itself or beneath its edge. o Lab guidelines for the current identification techniques for C. diphtheriae and direction for
the proper specimen collection are obtained from the Microbiologist on call at the PLPH. Obtain serum for antibodies to diphtheria antitoxin (prior to administering diphtheria antitoxin).
o If the levels are non-protective (<0.01 IU/ml) this may be useful to support the diagnosis when cultures are negative.
Identify if had recent contact with a case or carrier, or contact with articles soiled with the discharges from lesions of infected individuals.
Determine immunization history. Promptly identify close contacts* and assess immunization history.
o The risk of transmission is directly related to the closeness, duration of contact, and intensity of the exposure.
*Close contacts are defined as: Individuals who were in contact with the case in the previous seven days AND are: o household members, o friends, relatives, and caretakers who regularly visit the home, o kissing and/or sexual contacts, o those who share the same room at school, work, or homeless shelter and
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 7 of 21
o healthcare staff exposed to oropharyngeal secretions of the infected person. (Healthcare staff that have taken appropriate infection prevention and control precautions need not be considered contacts).
Assess recent travel history of case i.e., travelled within the last two weeks to a region that is endemic or experiencing an outbreak.
Determine recent immigration (within the last 6 months) from an area with known disease. Annex F: Countries with endemic Diphtheria
Control (1;46;47)
Management of a Case and Environment Hospitalized Case Isolation, routine practices and droplet precautions (pharyngeal diphtheria) or contact
precautions (cutaneous diphtheria) must be instituted until there is proof of elimination* of C. diphtheriae.
Non-Hospitalized (Community) Case Individuals are most commonly treated and followed by a community physician with support
from Public Health practitioners. Minimal contact with other persons in the home is recommended until proof of elimination** of
C. diphtheriae organism is demonstrated. Routine practices and droplet precautions (pharyngeal diphtheria) or contact precautions
(cutaneous diphtheria) must be instituted until there is proof of elimination** of C. diphtheriae. Cleaning all articles in contact with infected individual and articles soiled by discharges of the
case should be washed as per normal practices. Since infection with diphtheria does not always confer immunity, persons recovering from
diphtheria disease should be given a complete primary course of diphtheria containing vaccine, (as indicated by age and immunization history), unless serological testing indicates protective levels of antitoxin. **Proof of Elimination: The elimination of C. diphtheriae is confirmed in the following manner: o Respiratory diphtheria: two consecutive cultures from the nose and two from the throat
are negative for toxigenic diphtheria bacilli. These specimens are taken not less than 24 hours apart and not less than 24 hours after cessation of antibiotic therapy. A repeat culture should be done 2 weeks after antibiotic therapy is completed.
o Non-respiratory diphtheria; two consecutive cultures are negative for toxigenic diphtheria. These specimens are taken from skin lesions not less than 24 hours apart and not less than 24 hours after antibiotic therapy is completed.
Treatment of a Case: See Annex A: Sensitivity testing, Annex B: Desensitization protocol and Annex C: Administration Dosage of Diphtheria Antitoxin and Antibiotic Treatment for Cases. Treatment should begin as soon as possible based on clinical symptoms. Diphtheria antitoxin (DAT) is considered the mainstay of treatment, while antibiotic therapy is
required to eradicate the organism, to stop toxin production and prevent transmission. DAT neutralizes circulating toxin. Toxin already bound to tissue is unaffected. DAT does not
reverse symptoms, but it does prevent progression of the disease by binding circulating toxin. A person’s eligibility for DAT will be determined through discussion between the treating
physician, MOH and CMOH. o If after the discussion, it is the decision of the treating physician to give DAT it will be
released by the CMOH. The final decision to administer DAT lies with the treating physician.
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 8 of 21
DAT is made from equine serum and has as its main side effects hypersensitivity, anaphylaxis and serum sickness.
Diphtheria Antitoxin (DAT) General Use Guidelines: Currently there is no licensed product made in Canada. An antidiphtheria serum is made
available from Health Canada’s Special Access Program (SAP). o Access to and shipment of DAT is facilitated by the Senior Manager, Immunization Team
at Alberta Health and Wellness. o It is shipped under strict cold-chain management from the Provincial Vaccine Depot (PVD)
to the facility pharmacy. o All shipments of DAT will have a SAP “Form C” (Patient follow-up form) accompanying it.
This form must be completed by the MOH (or Designate) and sent back to the CMOH. o The CMOH will contact Health Canada’s Special Access Program (SAP) for urgent
delivery of more vials if required. o Delivery will occur by the most rapid mode of transport available. o If the DAT is not used, the product can be shipped (maintaining cold-chain) back to the
PVD. o Serum should be collected to identify the specific toxin before antitoxin is administered;
however, the administration of antitoxin should not be withheld pending test results. o Approximately 9% of people treated with equine antitoxin experience some degree of
hypersensitivity to equine serum but severe reactions are rare.
Precautions: Patients should be assessed and tested for hypersensitivity to equine sera prior to
administration. (See Annex A) Conduct a thorough history of asthma, hay fever, and sensitivity/distress in presence of horses
and/or previous doses of horse serum (i.e., Botulism Antitoxin, DAT or anti-snake venom). o These persons may develop serious anaphylactic-like reactions especially if previous
doses were administered intravenously. Patients found to be sensitive to DAT should follow the desensitization protocol outlined in
Annex B.
It has been recommended that 0.3 mL of epinephrine HCl solution (1:1000) be given to every patient before receiving diphtheria anti-toxin irrespective of their history of allergy, prior equine serum or positive sensitivity.(48)
Management of Contacts of Cases and Carriers The same preventive measures should be taken for contacts of cases and carriers, but the
former should be given a higher priority. The goals of contact management include: o Close monitoring o Assessing prior immunization status o Adherence to prophylaxis
The MOH (or designate) will attempt to identify all contacts. All contacts must be tested to determine unrecognized cases and carriers
All persons who have been in contact with a case of diphtheria caused by toxigenic C.diphtheriae in the previous seven days should be considered at risk.
Prior to administering any prophylaxis, all close contacts should have a single swab for culture taken from each of the nose, the throat and skin lesions (where present) and be kept under surveillance for seven days from the date of last contact with the case.
Daily surveillance includes:
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 9 of 21
o Assessing for signs and symptoms of diphtheria o Inspection of throat for presence of membrane o Measurement of temperature o Assessment of wounds if any
Special Measures: The MOH must exclude all contacts from: (47) o Contact with children, o Occupations involving the care of the sick and dependent, o Occupations involving the handling of foods; and o School.
Until cultures from the nose, throat and any lesion(s) are proved to be negative for toxigenic diphtheria bacilli.
Prophylaxis and Care for Contacts (44-47) Diphtheria contacts are given prophylaxis to:
o Treat incubating disease; and o Eliminate carriage and, therefore, decrease risk of exposure to other susceptible contacts.
See Annex D: Antibiotic Prophylaxis for Contacts, and Treatment for Carriers of Diphtheria. Antibiotic prophylaxis should be given to all contacts regardless of their immunization status. Close contacts should be given a dose of a diphtheria containing vaccine appropriate to their
age, unless they are known to be fully immunized with the last dose given in the previous five years. o The remaining doses required to provide full immunization should be given to any contacts
that were previously unimmunized or incompletely immunized. There is no acceptable clinical evidence for prophylactic use of DAT for contacts. Contacts who can not be kept under surveillance should receive penicillin G benzathine IM.
(see Annex D) Any asymptomatic contact identified as having a positive swab for toxic diphtheria should be
treated as a carrier and have additional swabs taken at completion of treatment and again two weeks following treatment.(49)
Management of Carriers: A carrier is defined as a person who harbours and may transmit C. diphtheriae but who has no
symptoms. Carriers can include those with otitis media or nasal infections and asymptomatic pharyngeal infection due to toxigenic C. diphtheriae.
The carrier state has a slow rate of spontaneous resolution (12% after 1 month) and so should be treated to prevent the spread of infection. (4) (see Annex D)
Use routine practices and droplet precautions for hospitalized pharyngeal or nasal carriers of toxigenic strains until proof of elimination** can be demonstrated.
A carrier must have additional swabs taken at completion of treatment and again two weeks following treatment.
Community (non-hospital) carriers should be excluded from the workplace or school until proof of elimination** is demonstrated. o Contact with other individuals living in the household should be minimized. o Carriers should be instructed to pay strict attention to personal hygiene by: Covering mouth and nose with tissue when coughing, Placing all contaminated tissues directly into garbage, Washing hands with soap and water every time there is contact with respiratory
secretions or infected wounds, Cleaning wounds and skin lesions vigorously with soap and water, and
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 10 of 21
Keeping all infected wounds covered. Promptly identify *close contacts and assess immunization history. Preventive measures may be extended to close contacts of carriers but should be considered
lower priority than control measures for contacts of a case.
Care and Treatment of Carriers: See Annex D Carriers should be given antibiotic prophylaxis regardless of immunization status. Erythromycin eradicates C. diphtheriae from the nose and throat of carriers in an average of 3
days. DAT has no proven role in the treatment of diphtheria carriers. If not immunized, all carriers should receive active immunization promptly with measures taken
to ensure completion of series. If carrier has been immunized previously, but has not received a booster within 5 years, a booster dose of diphtheria-containing vaccine should be given.
Because antimicrobial regimes are not 100% effective and bacterial relapse is possible, specimens from carriers should be cultured a minimum of 2 weeks after completion of treatment to ensure the organism has been eradicated.(49)
If cultures are positive, an additional 10 day course of antibiotics should be given with repeat follow-up cultures.
Preventive Measures Educate the public regarding the hazards of diphtheria infection. Primary immunization with a diphtheria-containing vaccine should be provided to all individuals
(including new immigrants) as per the current Alberta Immunization Manual. The immunization status of adults (especially travellers to areas where they may be exposed
to diphtheria) should be reviewed at least once during adult life and a single dose of diphtheria-containing vaccine be offered to those who have not been immunized within the previous 10 years.
Persons requiring a booster dose of a tetanus-containing vaccine for wound management should receive Td (Adacel for adolescents) as a convenient means of reinforcing diphtheria protection.
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 11 of 21
ANNEX A: Sensitivity Testing Sensitivity testing: (1;48;50)
Each person who is to be given animal serum should be skin tested before administration of that animal serum. Intradermal (ID) skin tests have resulted in fatalities, but the scratch test usually is safe. Therefore, scratch test should always precede ID testing. Scratch, Prick or Puncture Test *(1): Apply 1 drop of a 1:100 dilution of serum in preservative-free isotonic sodium chloride (0.9% NaCl) solution to the site of a superficial scratch, prick or puncture of the inner aspect of the forearm. Positive (histamine) and negative (0.9%NaCl) control tests for the scratch test should also be applied. In 15–20 minutes, a positive test result is a wheal with surrounding erythema at least 3 mm larger than the negative control test area. The histamine control must be positive for valid interpretation. If the scratch test result is negative, an ID test is performed. Intradermal Skin test*: Inject 0.1 mL of freshly prepared 1:100 volume for volume (v/v) dilution of antitoxin diluted in 0.9% sodium chloride (NaCl) to the dorsal forearm. Apply a negative control test of the same volume of 0.9% NaCl to the opposite extremity. (50) Note: Use a dose of 0.05 mL of a 1:1000 v/v or weaker dilution for preliminary skin testing if the history of scratch, prick or puncture test suggests hypersensitivity.
A positive reaction to an ID skin test occurs within 5–30 minutes, manifested by a wheal with surrounding erythema. In a marked reaction, the wheal is likely to have irregular projections, known as pseudopods. The extent of the wheal and its projections and the dimensions of the hyperemic area provide a rough idea of the degree of the patient’s hypersensitivity and the likelihood of adverse reaction to horse serum-based products.
*Antihistamines may inhibit reactions in the scratch, prick or puncture and ID tests; therefore, testing should not occur for at least 24 hours or, preferably, 48 hours after receipt of these drugs. Except in preschoolers, a conjunctival test (50) is often simpler and less likely to show nonspecific reactions than an ID test. Instill 1 drop of freshly prepared, sterile 1:10 v/v dilution of antitoxin in 0.9% NaCl in either eye, with a negative control of one drop of 0.9% NaCl instilled in the other eye.
A positive test consists of itching, burning, redness and lacrimation within 10–30 minutes. Interpreting results: If the history and hypersensitivity test are negative, proceed with therapeutic antitoxin administration as described in the product monograph and Annex C. NOTE: A negative history and skin/conjunctiva test does not preclude the possibility of adverse, immediate-hypersensitivity reactions and have no bearing on whether or not delayed serum reactions will occur after administration of the full dose. If the history is positive and the hypersensitivity test is highly positive, administration may be dangerous. Weigh risk of giving against risk of withholding. If the history is negative and the hypersensitivity test is mildly or questionably positive administer the antitoxin according to the desensitization protocol outlined in Annex B. It has been recommended that 0.3 ml of epinephrine HCl solution (1:1000) be given to every patient before receiving diphtheria antitoxin irrespective of their history of allergy, prior equine serum or positive sensitivity.(48)
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 12 of 21
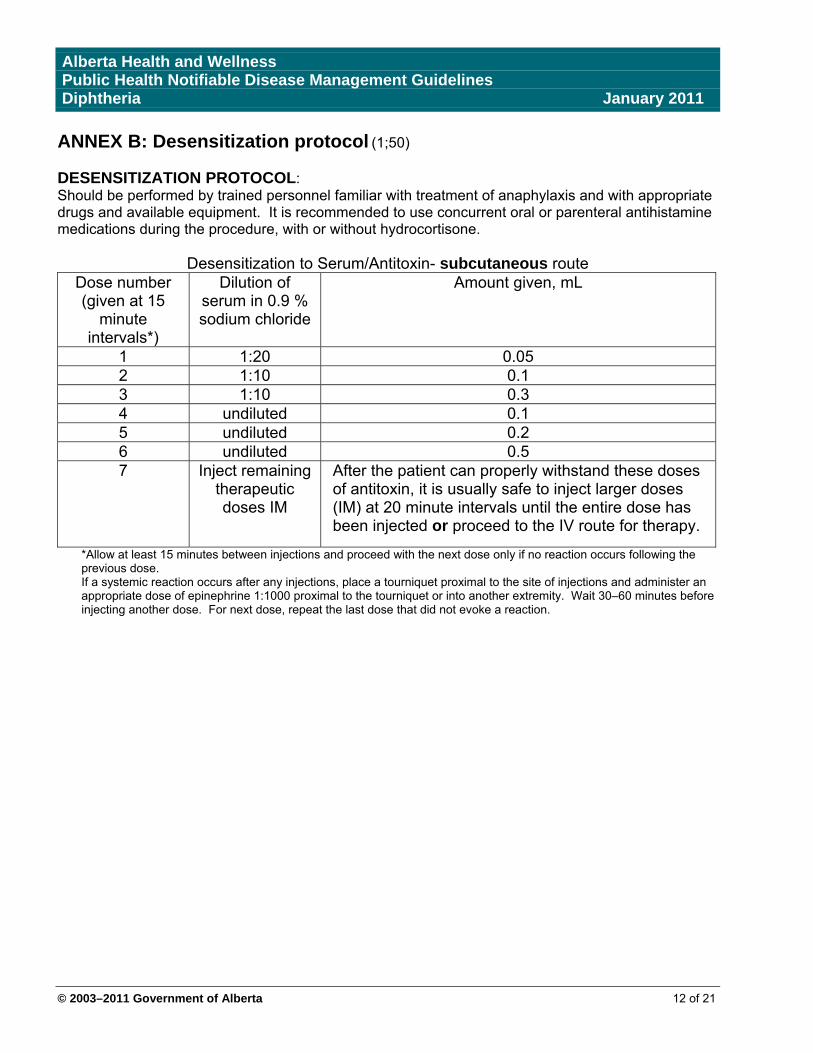
ANNEX B: Desensitization protocol (1;50) DESENSITIZATION PROTOCOL: Should be performed by trained personnel familiar with treatment of anaphylaxis and with appropriate drugs and available equipment. It is recommended to use concurrent oral or parenteral antihistamine medications during the procedure, with or without hydrocortisone.
Desensitization to Serum/Antitoxin- subcutaneous route Dose number (given at 15
minute intervals*)
Dilution of serum in 0.9 % sodium chloride
Amount given, mL
1 1:20 0.05 2 1:10 0.1 3 1:10 0.3 4 undiluted 0.1 5 undiluted 0.2 6 undiluted 0.5 7 Inject remaining
therapeutic doses IM
After the patient can properly withstand these doses of antitoxin, it is usually safe to inject larger doses (IM) at 20 minute intervals until the entire dose has been injected or proceed to the IV route for therapy.
*Allow at least 15 minutes between injections and proceed with the next dose only if no reaction occurs following the previous dose. If a systemic reaction occurs after any injections, place a tourniquet proximal to the site of injections and administer an appropriate dose of epinephrine 1:1000 proximal to the tourniquet or into another extremity. Wait 30–60 minutes before injecting another dose. For next dose, repeat the last dose that did not evoke a reaction.
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 13 of 21
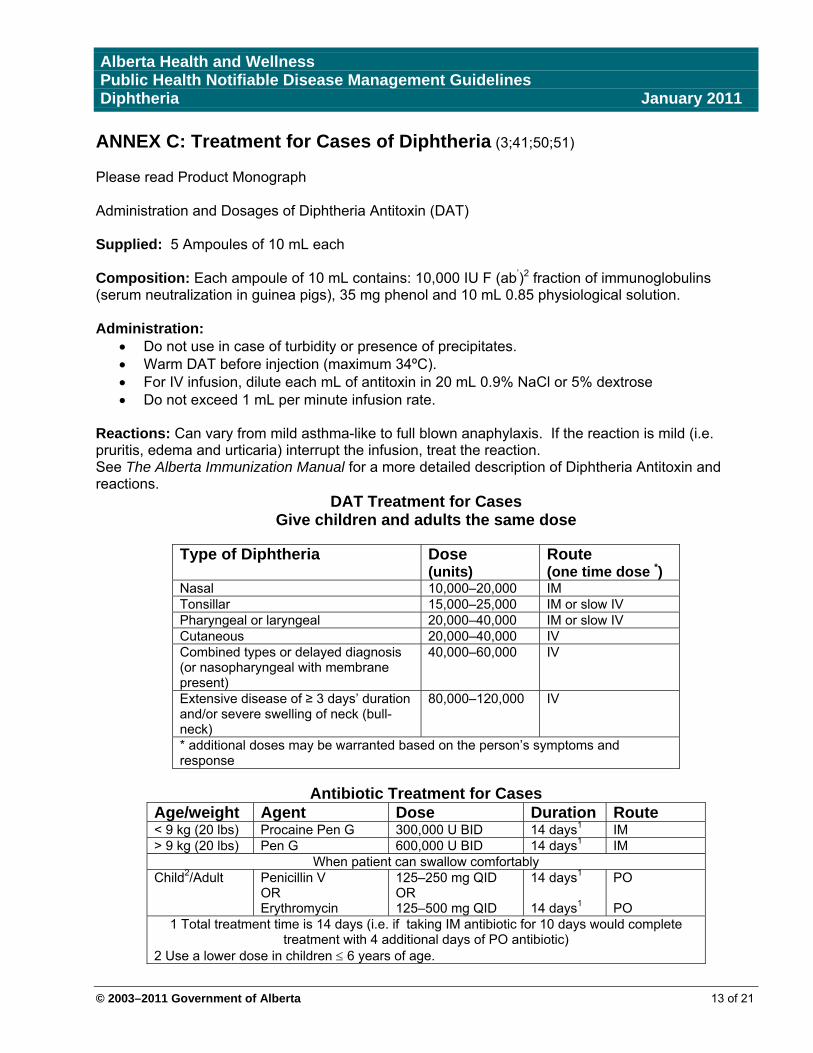
ANNEX C: Treatment for Cases of Diphtheria (3;41;50;51) Please read Product Monograph Administration and Dosages of Diphtheria Antitoxin (DAT) Supplied: 5 Ampoules of 10 mL each Composition: Each ampoule of 10 mL contains: 10,000 IU F (ab’)2 fraction of immunoglobulins (serum neutralization in guinea pigs), 35 mg phenol and 10 mL 0.85 physiological solution. Administration:
Do not use in case of turbidity or presence of precipitates. Warm DAT before injection (maximum 34ºC). For IV infusion, dilute each mL of antitoxin in 20 mL 0.9% NaCl or 5% dextrose Do not exceed 1 mL per minute infusion rate.
Reactions: Can vary from mild asthma-like to full blown anaphylaxis. If the reaction is mild (i.e. pruritis, edema and urticaria) interrupt the infusion, treat the reaction. See The Alberta Immunization Manual for a more detailed description of Diphtheria Antitoxin and reactions.
DAT Treatment for Cases Give children and adults the same dose
Type of Diphtheria Dose
(units) Route (one time dose *)
Nasal 10,000–20,000 IM Tonsillar 15,000–25,000 IM or slow IV Pharyngeal or laryngeal 20,000–40,000 IM or slow IV Cutaneous 20,000–40,000 IV Combined types or delayed diagnosis (or nasopharyngeal with membrane present)
40,000–60,000 IV
Extensive disease of ≥ 3 days’ duration and/or severe swelling of neck (bull-neck)
80,000–120,000 IV
* additional doses may be warranted based on the person’s symptoms and response
Antibiotic Treatment for Cases
Age/weight Agent Dose Duration Route < 9 kg (20 lbs) Procaine Pen G 300,000 U BID 14 days1 IM > 9 kg (20 lbs) Pen G 600,000 U BID 14 days1 IM
When patient can swallow comfortably Child2/Adult Penicillin V
OR Erythromycin
125–250 mg QID OR 125–500 mg QID
14 days1
14 days1
PO PO
1 Total treatment time is 14 days (i.e. if taking IM antibiotic for 10 days would complete treatment with 4 additional days of PO antibiotic)
2 Use a lower dose in children 6 years of age.
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
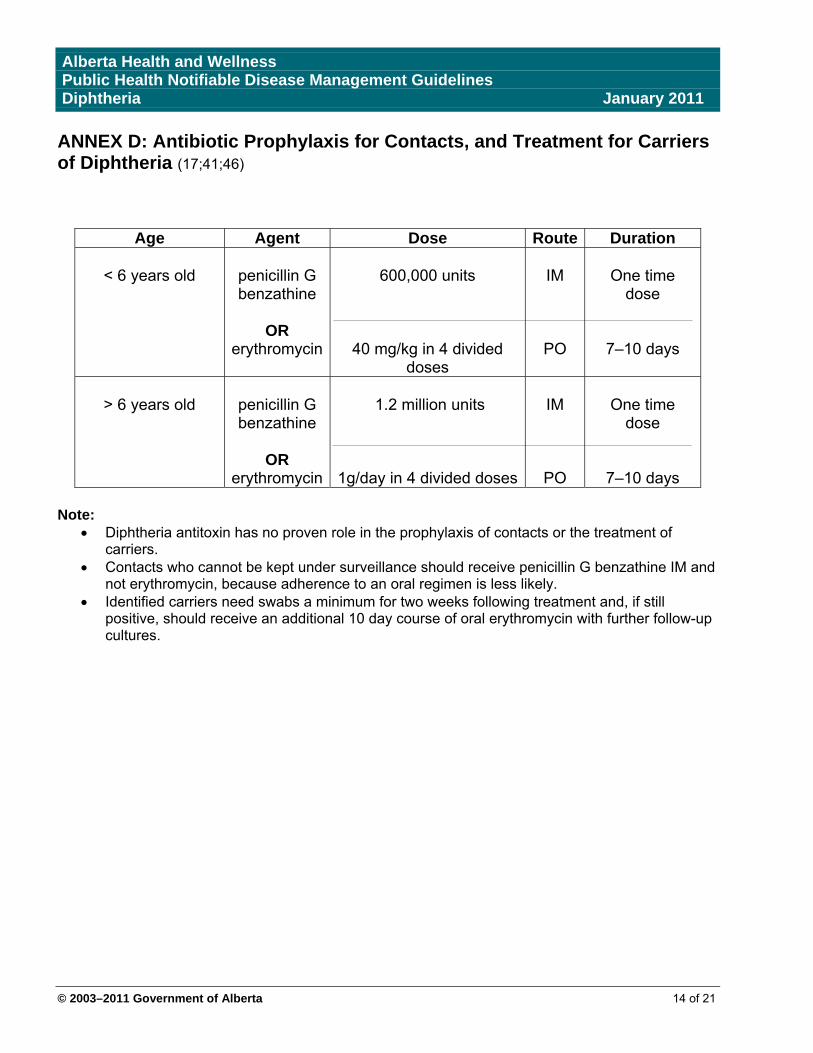
ANNEX D: Antibiotic Prophylaxis for Contacts, and Treatment for Carriers of Diphtheria (17;41;46)
Age Agent Dose Route Duration
< 6 years old
penicillin G benzathine
OR
erythromycin
600,000 units
40 mg/kg in 4 divided doses
IM
PO
One time
dose
7–10 days
> 6 years old
penicillin G benzathine
OR
erythromycin
1.2 million units
1g/day in 4 divided doses
IM
PO
One time
dose
7–10 days
Note: Diphtheria antitoxin has no proven role in the prophylaxis of contacts or the treatment of
carriers. Contacts who cannot be kept under surveillance should receive penicillin G benzathine IM and
not erythromycin, because adherence to an oral regimen is less likely. Identified carriers need swabs a minimum for two weeks following treatment and, if still
positive, should receive an additional 10 day course of oral erythromycin with further follow-up cultures.
© 2003–2011 Government of Alberta 14 of 21
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 15 of 21
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 16 of 21
ANNEX E (cont) a. Routine practices, droplet precautions and contact precautions are described in detail at:
http://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/99pdf/cdr25s4e.pdf Maintain isolation until elimination of the organism is demonstrated by negative culture of two samples obtained at least 24 hours apart after completion of antimicrobial therapy.
b. Both nasal and pharyngeal swabs should be obtained for culture.
c. The recommended dosage and route of administration depend on the extent and duration of
disease. Refer to Annex C for detailed recommendations for Diphtheria antitoxin.
d. Refer to Annex C for details regarding dosage recommendations for treatment of cases. Antibiotic therapy is not a substitute for antitoxin treatment.
e. Immunizations required because clinical diphtheria does not confer immunity.
f. Close contacts include household members and other persons with a history of direct contact with
a case (e.g. caretakers, relatives, or friends who regularly visit the home) as well as health-care personnel exposed to oral or respiratory secretions of a case. These individuals need to be excluded from; children, occupations involving food handling and from school until their cultures are negative for toxigenic diphtheria bacilli.
g. A single swab for culture should be obtained from each of the nasal and pharyngeal sites. Swabs
should also be taken from any wounds or skin lesions.
h. Refer to Annex D for detailed dosage recommendations for prophylaxis of contacts.
i. Refer to Annex D for detailed dosage recommendations for treatment of carriers. j. In the respiratory form: elimination of C. diphtheria is demonstrated by two negative cultures of
throat and two negative cultures of the nasopharynx, taken at least 24 hours apart, a minimum of two weeks after antibiotics are completed.
In the non-respiratory form: elimination C. diphtheria is demonstrated by two consecutive
cultures that are reported negative for toxigenic diphtheria bacilli. These cultures are to be taken from skin lesions not less than 24 hours apart and a minimum of two weeks after completion of antibiotic therapy. Persistent carriage of the organism should be treated with an additional 10 day course of erythromycin with follow-up cultures.
k. Refer to the Alberta Immunization Manual for recommendations on the schedule of immunizations.

Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
ANNEX F: Countries with Endemic Diphtheria (52)
Regions Countries
Africa Algeria, Angola, Egypt, Niger, Nigeria, Sudan, and sub- Saharan countries
Americas Bolivia, Brazil, Colombia, Dominican Republic, Ecuador, Haiti, and Paraguay
Asia/South Pacific
Afghanistan, Bangladesh, Bhutan, Burma (Myanmar), Cambodia, China, India, Indonesia, Laos, Malaysia, Mongolia, Nepal, Pakistan, Papua New Guinea, Philippines, Thailand, and Vietnam
Middle East Iran, Iraq, Saudi Arabia, Syria, Turkey, and Yemen
Europe Albania, Russia, and countries of the former Soviet Union
© 2003–2011 Government of Alberta 17 of 21
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 18 of 21
References (1) American Academy of Pediatrics. Redbook - Report of the Committee on Infectious Diseases.
Pickering L. editor. 27th edition, 2006. (2) Centers for Disease Control and Prevention. Epidemiology and prevention of vaccine-
preventable diseases. The Pink Book. Eleventh Edition 2009. http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/dip.pdf
(3) Mandel G. et al. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious
Diseases – Volume 1. Elsevier Churchill, Livingstone pub. Sixth edition, Accessed online. (4) Harnisch JP, Tronca E, Nolan CM, et al. Diphtheria among alcoholic urban adults. A decade
of experience in Seattle. Ann Intern Med. 1989; 111:71-82. (5) Koopman JS, Campbell J. The role of cutaneous diphtheria infections in a diphtheria
epidemic. J Infect Dis. 1975; 131:239-244. (6) Belsey MA, Sinclair M, Roder MR, et al. Corynebacterium diphtheriae skin infections in
Alabama and Louisiana. N Engl J Med. 1969; 280:135-141. (7) Vitek CR, Wharton M. Diphtheria in the former Soviet Union: Re-emergence of a pandemic
disease. Emerg Infect Dis. 1998; 4:539-550. (8) Belsey MA, LeBlanc DR. Skin infections and the epidemiology of diphtheria: Acquisition and
persistence of C. diphtheriae infections. Am J Epidemiol. 1975; 102:179-184. (9) Lortholary O, Buu-Hoi A, Gutmann L, et al. Corynebacterium diphtheriae endocarditis in
France. Clin Infect Dis. 1993;17:1072-1074. (10) Tiley SM, Kociuba KR, Heron LG, et al. Infective endocarditis due to nontoxigenic
Corynebacterium diphtheriae: Report of seven cases and review. Clin Infect Dis. 1993;16:271-275,
(11) Gruner E, Opravil M, Altwegg M, et al. Nontoxigenic Corynebacterium diphtheriae isolated
from intravenous drug users. Clin Infect Dis. 1994;18:94-96. (12) Patey O, Bimet F, Riegel P, et al. Clinical and molecular study of Corynebacterium
diphtheriae systemic infections in France. J Clin Microbiol. 1997; 35:441-445. (13) Wilson APR. The return of Corynebacterium diphtheriae: The rise of non-toxigenic strains. J
Hosp Infect. 1995; 30(Suppl):306-312. (14) Efstratiou A, George RC, Begg NT. Non-toxigenic Corynebacterium diphtheriae var gravis in
England. Lancet. 1993; 341:1592-1593. (15) Reacher M, Ramsay M, White J, et al. Nontoxigenic Corynebacterium diphtheriae: An
emerging pathogen in England and Wales? Emerg Infect Dis. 2000; 6:640-645.
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 19 of 21
(16) Rakhmanova AG, Lumio J, Groundstroem KWE, et al. Fatal respiratory tract diphtheria apparently caused by nontoxigenic strains of Corynebacterium diphtheriae. Eur J Clin Microbiol Infect Dis. 1997; 16:816-820.
(17) World Health Organization. Manual for the management and control of diphtheria in the
European Region. Copenhagen: WHO Regional Office for Europe, 1994. (18) Provincial Laboratory of Public Health. Guide to Services. May 2008. Accessed July 23,
2008. http://www.provlab.ab.ca/guide-to-services.pdf (19) Kalapothaki V, Sapounas T, Xirouchaki E, et al. Prevalence of diphtheria carriers in a
population with disappearing clinical diphtheria. Infection. 1984;12:387-389. (20) Heath CW, Zusman J. An outbreak of diphtheria among skid-row men. N Engl J Med. 1962;
267:809-812. (21) Bisgard KM, Hardy IRB, Popovic T, et al. Respiratory diphtheria in the United States, 1980-
1995. Am J Publ Hlth. 1998; 88:787-791. (22) Dixon JMS. Diphtheria in North America. J Hyg (Cambridge). 1984; 93:419-32. (23) Kwantes W. Diphtheria in Europe. J Hyg (Cambridge). 1984; 93:433-437. (24) Galazka AM, Robertson SE: Diphtheria: Changing patterns in the developing world and the
industrialized world. Eur J Epidemiol. 1995; 11:107-117. (25) Golaz A, Hardy IR, Strebel P, et al. Epidemic diphtheria in the newly independent states of the
former Soviet Union: Implications for diphtheria control in the United States. J Infect Dis. 2000; 181(Suppl 1):S237-S243.
(26) Dittman S, Wharton, M Vitek C et al. Successful control of epidemic diphtheria is the states of
the former Union of Soviet Socialist Republics: lessons learned. Journal of Infectious Diseases 2000; 181 (Suppl 1):S10-22.
(27) Diphtheria Morbidity in the Russian Federation, 1999-2003. Public Health and Environment
Bulletin, Issues 1-3 (2001, 2002, 2003). Federal Center of the State Sanitary and Epidemiological Surveillance of the Public Health Ministry of the Russian Federation (Moscow, RF).
(28) Blystad H, Blad J, Giesecke J: Surveillance and trends of priority infectious diseases in the
Baltic Sea Region. Epinorth Bull Netwk Commun Dis Control N Eur. 2002; 3:62. (29) Hardy IRB, Dittmann S, Sutter RW. Current situation and control strategies for resurgence of
diphtheria in newly independent states of the former Soviet Union. Lancet. 1996; 347:1739-1744.
(30) The Immunological Basis for Immunization Series: Diphtheria-Module 2.
http://www.who.int/vaccines-documents/DocsPDF-IBI-e/mod2_e.pdf (accessed July 30, 2008).
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 20 of 21
(31) Galazka AM, Robertson SE, Oblapenko GP. Resurgence of diphtheria. Eur J Epidemiol 1995; 11:95-105.
(32) Wilson APR, Efstratiou A, Weaver E, et al. Unusual non-toxigenic Corynebacterium
diphtheriae in homosexual men. Lancet. 1992; 339:998. (33) Zuber PL, Grunner E, Altwegg M, et al. Invasive infection with Corynebacterium diphtheriae
among drug users. Lancet. 1992; 339:1359. (34) Brooks GF, Bennett JV, Feldman RA. Diphtheria in the United States, 1959-1970. J Infect
Dis. 1974; 129:172-178. (35) Farizo KM, Strebel PS, Chen RT et al. Fatal respiratory disease due to Corynebacterium
diphtheriae: Case report and review of guidelines for management, investigation and control. Clin Infect Dis. 1993; 16:59-68.
(36) Alberta Health and Wellness. Disease Control and Prevention. Communicable Disease
Reporting System. March 2003.
(37) Guidelines for the Control of Infectious Diseases: The Blue Book. Public Health Division, Victorian Government of Human Services, Australia. Accessed Jan 17,2011. Diphtheria- Blue Book: IDEAS - Victorian Government
(38) Routine Practices and Additional Precautions for Preventing the Transmission of Infection in
Health Care - CCDR Volume 25S4 July 1999.
(39) Plotkin, S, Orenstien, W. Vaccines. W.B. Saunders, 5th
ed., 2008. (40) Public Health Agency of Canada. Vaccine preventable disease – Diphtheria. Infections
Division. October 2002. http://www.phac-aspc.gc.ca/im/vpd-mev/diphtheria-eng.php
(41) Public Health Agency of Canada. Guidelines for the Control of Diphtheria in Canada. Ottawa: CCDR 1998; 24S3. http://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/98vol24/24s3/index.html
(42) Use of Diphtheria (DAT) for Suspected Diphtheria Cases. Bacterial Vaccine Preventable Diseases Branch. Division of Epidemiology and Surveillance. National Immunization Program. Centre for Disease Control and Prevention. Atlanta, Georgia. March 24, 2004.
(43) Begg NT. Control of diphtheria: guidance for consultants in communicable disease control.
Communicable Diseases and Public Health. 1999; 2:242-249. (44) Alberta Health and Wellness, Disease Control and Prevention. Alberta Immunization Manual
– Diphtheria. January 2001. (45) Public Health Agency of Canada. Canadian Immunization Guide. Seventh Edition 2006.
http://www.phac-aspc.gc.ca/publicat/cig-gci (46) Heymann D. ed. Control of Communicable Diseases Manual. American Public Health
Association. 19th edition, 2008.
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines Diphtheria January 2011
© 2003–2011 Government of Alberta 21 of 21
(47) CDC Regulations. Province of Alberta. (48) Canadian Pharmacists Association. Compendium of Pharmaceuticals and Specialties. 9th
edition. Ottawa, Ontario: Canadian Pharmacists Association, 2005. (49) Miller LW; Bickham S; Jones WL; Heather CD; Morris RH. Diphtheria Carriers and the Effect
of Erythromycin Therapy. Antimicrobial Agents and Chemotherapy 1974 Aug; Vol. 6 (2), pp. 166-9.
(50) Grabenstein JD. ImmunoFacts: Vaccines & Immunologic Drugs. St Louis, MD: Wolters
KluwerHealth; 2006. (51) Product Monograph. Antidiphtheria Serum. Instituto Butantan. Sao Paulo, Brazil. (52) Centers for Disease Control and Prevention. CDC Health Information for International Travel
2010. Atlanta: U.S. Department of Health and Human Services, Public Health Service, 2009. http://wwwnc.cdc.gov/travel/yellowbook/2010/chapter-2/diphtheria.aspx





















![1. Diphtheria [Difteri]](https://img.pdfslide.net/doc/110x75/56d6be451a28ab3016916524/1-diphtheria-difteri.jpg)