Embed Size (px)
Citation preview

In the Literature
Guidelines for the Older Adult With CKDCommentary on Leipzig RM, Whitlock EP, Wolff TA, et al; for the US Preventive Services Task ForceGeriatric Workgroup. Reconsidering the approach to prevention recommendations for older adults.
Ann Intern Med. 2010;153(12):809-814.
When treating older patients, clinicians have tomake complex decisions to prioritize among
many available preventive and therapeutic interven-tions. There is a large overlap between older age andchronic kidney disease (CKD): in the United States,25 million individuals are 70 years or older andalmost half of them have CKD.1 Vice versa, 23million US residents have CKD and almost half are 70years or older.1,2
Nephrology guidelines are a driving force for stan-dardization of care and professional self-improve-ment in the management of patients with CKD.3
Clinical practice guidelines are tools to support deci-sion making by practitioners, patients, and policymakers. However, they repeatedly have been criti-cized as not being applicable to complex patients.4-6
There is an inherent tension between making guide-lines simple and evidence-based versus sufficientlydetailed and applicable to individuals with varyingdisease severity, comorbidity, and prognosis. Guide-lines may never perfectly address complex patientsbecause this usually requires judgment along withextrapolation of evidence from less complex andoften younger populations. Ultimately, guideline pan-els must choose between providing no recommenda-tion when evidence is of low quality versus issuingdiscretionary recommendations based on extrapola-tion of evidence and experts’ best guesses. Someclinicians have voiced frustration with the formerapproach7 and a preference for the latter.8 This sug-gests that some clinicians may be willing to tolerategreater uncertainty for guideline panels to addressmore complex issues.9 Therefore, guideline panelshave to develop new approaches to purposefully andtransparently consider important complexity and itspotential impact on expected benefits and harms ofrecommended actions.10 Leipzig et al11 propose arefined approach, which published in 2010 in the
Originally published online June 13, 2011.Address correspondence to Katrin Uhlig, MD, MS, Division of
Nephrology, Tufts Medical Center, 800 Washington St, Boston, MA02111. E-mail: [email protected].
© 2011 by the National Kidney Foundation, Inc.0272-6386/$36.00
doi:10.1053/j.ajkd.2011.05.001162
Annals of Internal Medicine, to better address theneeds of older adults when developing guidelines onpreventive services.
WHAT DOES THIS IMPORTANT STUDY SHOW?
The US Preventive Services Task Force (USPSTF)issues evidence-based recommendations for screen-ing and prevention. Its recommendations are devel-oped using an evidence-based framework that guidesthe approach and scope of systematic evidence re-view. The USPSTF convened a geriatric subgroup ofits methods work group to address challenges in topicprioritization, evidence review, and guideline develop-ment regarding preventive services for older adults.The article by Leipzig et al on behalf of this group11
and its accompanying editorial12 refer to and build onthe USPSTF’s systematic review of fall prevention ingeriatric populations.13 The USPSTF proposes 3 newapproaches, stating that selection of the most appropri-ate approach for each of its guideline topics will bedetermined on the basis of the available evidence forthe condition under review, an understanding of itsnatural history and pathophysiologic process, and anunderstanding of the intervention mechanisms underconsideration.
First, the USPSTF plans to address issues specificto persons of older age when commissioning a system-atic review for diseases prevalent in older adults (eg,primary care screening for depression). It proposes tospecifically consider adults 65 years or older and tostratify recommendations according to age.
Second, the USPSTF proposes to expand the typi-cal analytic framework when developing recommen-dations concerning geriatric syndromes. In the case ofthe USPSTF recommendations for prevention of falls,this entailed consideration of several common interre-lated risk factors for falls and functional limitations,along with the various interventions targeting eachrisk factor.
Third, the USPSTF proposes to bundle recommen-dations for related topics to make recommendationsmore consistent, interlinked, and comprehensive. Forexample, a guideline for prevention of bone fractureswould contain sections with recommendations aboutcalcium and vitamin D supplements, screening for
osteoporosis, and prevention of falls.Am J Kidney Dis. 2011;58(2):162-165
tric s
In the Literature
HOW DOES THIS STUDY COMPARE WITHPRIOR STUDIES?
Many guideline recommendations currently focuson only single diseases, do not stratify their recommen-dations for older versus younger adults, do not con-sider burden of comorbid illnesses, or do not specifi-cally state the expected time frame for a favorablerisk-benefit ratio.4,6,14-16
First, older individuals often are under-representedin clinical trials, thus limiting the quality and scope ofdirect evidence in this population. However, olderadults and individuals with greater comorbidity gener-ally have an increased mortality risk, a greater numberof potentially relevant outcomes, and an increased
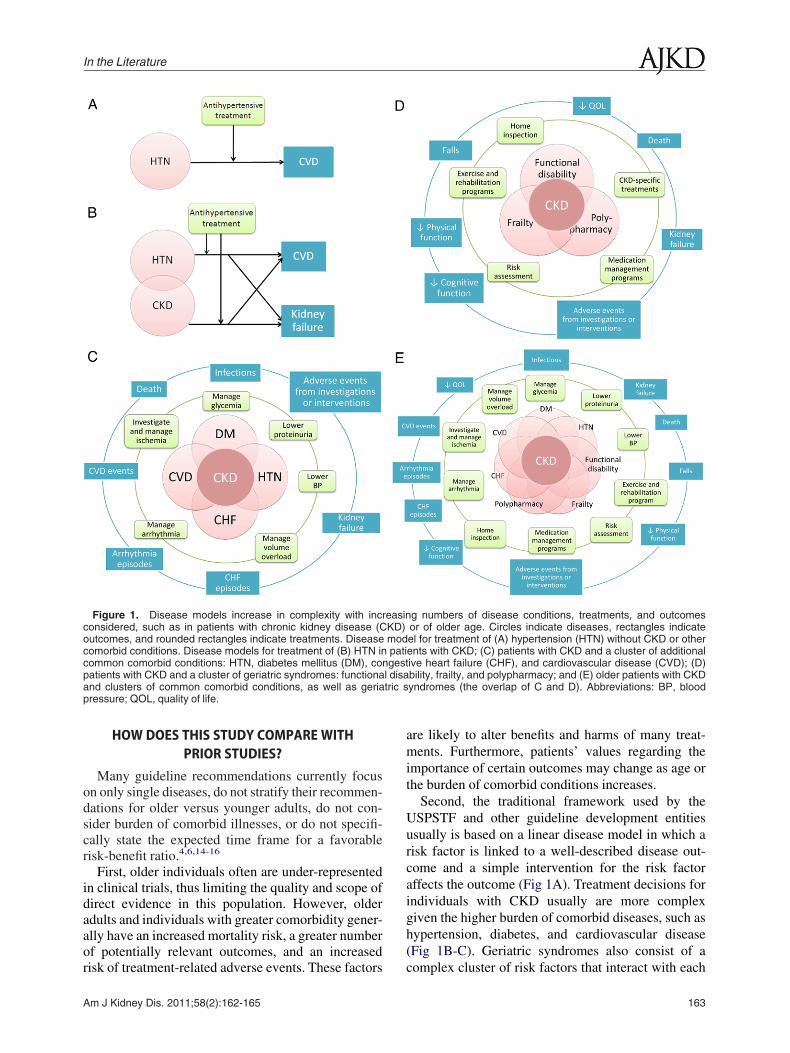
Figure 1. Disease models increase in complexity with incconsidered, such as in patients with chronic kidney disease (Coutcomes, and rounded rectangles indicate treatments. Diseasecomorbid conditions. Disease models for treatment of (B) HTN incommon comorbid conditions: HTN, diabetes mellitus (DM), copatients with CKD and a cluster of geriatric syndromes: functionaand clusters of common comorbid conditions, as well as geriapressure; QOL, quality of life.
risk of treatment-related adverse events. These factors
Am J Kidney Dis. 2011;58(2):162-165
are likely to alter benefits and harms of many treat-ments. Furthermore, patients’ values regarding theimportance of certain outcomes may change as age orthe burden of comorbid conditions increases.
Second, the traditional framework used by theUSPSTF and other guideline development entitiesusually is based on a linear disease model in which arisk factor is linked to a well-described disease out-come and a simple intervention for the risk factoraffects the outcome (Fig 1A). Treatment decisions forindividuals with CKD usually are more complexgiven the higher burden of comorbid diseases, such ashypertension, diabetes, and cardiovascular disease(Fig 1B-C). Geriatric syndromes also consist of a
g numbers of disease conditions, treatments, and outcomesor of older age. Circles indicate diseases, rectangles indicateel for treatment of (A) hypertension (HTN) without CKD or otherents with CKD; (C) patients with CKD and a cluster of additionalive heart failure (CHF), and cardiovascular disease (CVD); (D)bility, frailty, and polypharmacy; and (E) older patients with CKDyndromes (the overlap of C and D). Abbreviations: BP, blood
reasinKD)modpati
ngestl disa
complex cluster of risk factors that interact with each
163

Uhlig and Boyd
other and variably impact on a spectrum of clinicaloutcomes and disease states (Fig 1D), and this com-plexity is compounded further in the overlap of CKDcomorbidities and geriatric syndromes (Fig 1E). Im-provements in multifactorial conditions may requiremultipronged interventions. Along with traditionaldiscrete clinical events, meaningful outcomes for olderadults include functional disability and cognitive im-pairment. A major challenge lies in the current lack ofroutine and standardized collection of valid and respon-sive measures for functional outcomes. Even whenavailable, it is challenging to define clinically mean-ingful differences and compare effects, often on con-tinuous scales, across different outcomes.
Third, guidelines for the same topic often arepresented in piecemeal fashion. Different guidelinedevelopers have ownership of particular diseases,interventions, or outcomes, which may lead toredundancy and differences in recommendations.Bundling of recommendations for a patient with acluster of diseases requires reconciling the exper-tise of generalists with that of multidisciplinaryspecialists.
WHAT SHOULD CLINICIANS ANDRESEARCHERS DO?
The implications of the USPSTF recommendationsdetailed by Leipzig et al are directly applicable toguideline development and clinical research in nephrol-ogy. Most current evidence-based CKD guidelinespertain to treatment rather than screening. Neverthe-less, the approaches for prevention recommendationsfor older adults suggested by the USPSTF are relevantto evidence review and guideline development forindividuals with CKD. Many patients with CKD areolder and there may be important differences in thepathophysiologic process and natural history of CKDfor older versus younger adults.5,17,18
Following the first suggestion of the USPSTF,adults of older age a priori should be a subgroup ofinterest for clinical practice recommendations aboutCKD. Evidence review should involve assessment ofthe degree to which older individuals were included inrelevant studies and how risk relationships and treat-ment effects may differ. Harms assessments need toconsider alterations in drug metabolism, possible druginteractions, and greater risks from invasive interven-tions in older patients. Estimating the expected bal-ance between benefits and harms needs to considerolder adults’ overall shorter life expectancy versus thechronicity of the disease and the possibility of differ-ent preferences or values regarding treatment goals.Recommendations for older adults with CKD mayneed to be worded differently or assigned a different
strength. Going forward, older adults should consti-164
tute prespecified subgroups in trials and cohort studiesof CKD. To overcome limitations of subgroup effects,risk-stratification tools should incorporate age alongwith level of estimated glomerular filtration rate andalbuminuria and other risk factors to more comprehen-sively categorize risks and explore the heterogeneityof treatment effects.14,19
Following the second USPSTF recommendation,CKD guidelines need to address topics of particularimportance to older individuals, for example, func-tional disability, frailty, falls, polypharmacy, depres-sion, and decision making regarding renal replacementtherapy, among others. Outcome measures that willreliably assess quality of life and functional performancein meaningful increments need to be studied.20 Futureresearch needs to evaluate the preferences of individualswith CKD and the value that these individuals attachto various states of health and risk, along with thedegree of variability and factors that impact on thesepreferences and values, such as older age.21
Finally, as suggested by the USPSTF, we need toreconcile and prioritize across myriad guidelines forthe same target population. Weighing the relativemerits of various strategies necessitates stepping backfrom a focus on a particular intervention or outcomeand shifting to a focus on improving overall healthand survival. Synthesis of research evidence acrossvarious interventions requires advances in methods todeal with indirect comparisons and combine dispa-rate benefits and harms. In guideline groups, thiswidens both the scope and needed clinical andmethod expertise. Regardless, any guideline panelattempting to extrapolate imperfect evidence to acomplex patient, be it an older adult or a patientwith CKD, will need to exercise more judgmentthan for simpler target populations. Guideline userswill have to accept that differences of opinion willalter assessments and recommendations, as mightfuture research. Guideline developers bear the re-sponsibility of transparently communicating uncer-tainty and judgments to their audience.
Katrin Uhlig, MD, MSTufts Medical Center
Boston, Massachusetts
Cynthia Boyd, MD, MPHJohns Hopkins University School of Medicine
Baltimore, Maryland
ACKNOWLEDGEMENTSWe thank Jenny Lamont, MS, for editorial support and help
drafting the figure.Dr Boyd is supported by the Paul Beeson Career Development
Award Program (NIA K23 AG032910, AFAR, the John A. Hart-
ford Foundation, the Atlantic Philanthropies, the Starr Foundation,Am J Kidney Dis. 2011;58(2):162-165

In the Literature
and an anonymous donor), the Robert Wood Johnson PhysicianFaculty Scholars Program, and the Johns Hopkins Bayview Centerfor Innovative Medicine.
Financial Disclosure: Dr Uhlig is supported by the NationalKidney Foundation for conducting evidence reviews and provid-ing methods support for KDIGO (Kidney Disease: ImprovingGlobal Outcomes) guidelines. Drs Uhlig and Boyd are supportedby a grant from the Agency for Healthcare Research and Quality todevelop an approach for improving clinical practice guidelines forcomplex patients (AHRQ R21 HS18597-01).
REFERENCES1. Levey AS, Stevens LA, Schmid CH, et al. A new equation to
estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604-612.
2. Stevens LA, Coresh J, Levey AS. CKD in the elderly—oldquestions and new challenges: World Kidney Day 2008. Am JKidney Dis. 2008;51(3):353-357.
3. Uhlig K, Balk EM, Lau J, Levey AS. Clinical practiceguidelines in nephrology—for worse or for better. Nephrol DialTransplant. 2006;21(5):1145-1153.
4. Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW.Clinical practice guidelines and quality of care for older patientswith multiple comorbid diseases: implications for pay for perfor-mance. JAMA. 2005;294(6):716-724.
5. O’Hare AM, Kaufman JS, Covinsky KE, Landefeld CS,McFarland LV, Larson EB. Current guidelines for using angiotensin-converting enzyme inhibitors and angiotensin II-receptor antago-nists in chronic kidney disease: is the evidence base relevant toolder adults? Ann Intern Med. 2009;150(10):717-724.
6. Shaneyfelt TM, Centor RM. Reassessment of clinical prac-tice guidelines: go gently into that good night. JAMA. 2009;301(8):868-869.
7. Petitti DB, Teutsch SM, Barton MB, et al. Update on themethods of the U.S. Preventive Services Task Force: insufficientevidence. Ann Intern Med. 2009;150(3):199-205.
8. Balk EM, Uhlig K. Using GRADE for international guide-lines on kidney disease. 2010. http://www.guideline.gov/expert/expert-commentary.aspx?id�16436. Accessed February 23, 2011.
9. VanLare JM, Conway PH, Sox HC. Five next steps for a newnational program for comparative-effectiveness research. N Engl
J Med. 2010;362(11):970-973.Am J Kidney Dis. 2011;58(2):162-165
10. Boyd C, Leff B, Kent D, Uhlig K. A framework to improveguidelines for patients with multimorbidity [abstract]. OtolaryngolHead Neck Surg. 2010;143:42.
11. Leipzig RM, Whitlock EP, Wolff TA, et al; for the USPreventive Services Task Force Geriatric Workgroup. Reconsider-ing the approach to prevention recommendations for older adults.Ann Intern Med. 2010;153(12):809-814.
12. Tinetti ME. Making prevention recommendations relevantfor an aging population. Ann Intern Med. 2010;153(12):843-844.
13. Michael YL, Whitlock EP, Lin JS, Fu R, O’Connor EA,Gold R; US Preventive Services Task Force. Primary care-relevantinterventions to prevent falling in older adults: a systematic evi-dence review for the U.S. Preventive Services Task Force. AnnIntern Med. 2010;153(12):815-825.
14. Kent DM, Hayward RA. Limitations of applying summaryresults of clinical trials to individual patients: the need for riskstratification. JAMA. 2007;298(10):1209-1212.
15. Greenfield S, Kravitz R, Duan N, Kaplan SH. Heterogene-ity of treatment effects: implications for guidelines, payment, andquality assessment. Am J Med. 2007;120(4)(suppl 1):S3-9.
16. Scott IA, Guyatt GH. Cautionary tales in the interpretationof clinical studies involving older persons. Arch Intern Med.2010;170(7):587-595.
17. O’Hare AM, Choi AI, Bertenthal D, et al. Age affectsoutcomes in chronic kidney disease. J Am Soc Nephrol. 2007;18(10):2758-2765.
18. Murtagh FE, Addington-Hall JM, Higginson IJ. End-stagerenal disease: a new trajectory of functional decline in the last yearof life. J Am Geriatr Soc. 2011;59(2):304-308.
19. Kent DM, Rothwell PM, Ioannidis JP, Altman DG, HaywardRA. Assessing and reporting heterogeneity in treatment effects inclinical trials: a proposal. Trials. 2010;11:85.
20. No authors listed. Patient-reported outcomes in clinicaltrials of chronic kidney disease-related therapies. Workshop co-sponsored by the National Kidney Foundation and the US Foodand Drug Administration. 2011. http://www.kidney.org/profession-als/physicians/ProConference.cfm. Accessed March 15, 2011.
21. Butler M, Talley KMC, Burns R, et al. Prevention in OlderAdults: Values in Older Adults Related to Primary and SecondaryPrevention. Rockville, MD: Agency for Healthcare Research and
Quality; 2011.165

























![Older Adult new - mmLearn.org · • Water pik/oral irrigator ... < ... Older Adult new [Compatibility Mode]](https://img.pdfslide.net/doc/110x75/5b581e6f7f8b9a657c8b893a/older-adult-new-water-pikoral-irrigator-older-adult-new-compatibility.jpg)