-
7/30/2019 Guidelines SAH AHA
1/71
-
7/30/2019 Guidelines SAH AHA
2/71
1/12/2013 2009, American Heart Association. All rights
reserved.
AHA/ASA Scientific StatementGuidelines for the Management of
Aneurysmal Subarachnoid
Hemorrhage (SAH)
A Statement for Healthcare Professionals from a Special
Writing
Group of the Stroke Council, American Heart Association
Joshua B. Bederson, MD, Chair; E. Sander Connolly, Jr., MD,
FAHAVice-Chair; H. Hunt Batjer, MD; Ralph G. Dacey, MD, FAHA;
Jacques E. Dion, MD, FRCPC; Michael N. Diringer, MD, FAHA,FCCM;
John E. Duldner, Jr., MD, MS; Robert E. Harbaugh, MD,
FACS, FAHA; Aman B. Patel, MD; Robert H.Rosenwasser, MD, FACS,
FAHA
-
7/30/2019 Guidelines SAH AHA
3/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Stroke Council ProfessionalEducation Committee
This slide presentation was
developed by members of theStroke Council ProfessionalEducation
committee. Opeolu Adeoye MD
Dawn Kleindorfer MD
-
7/30/2019 Guidelines SAH AHA
4/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Citation Information Key words included in the paper:
aneurysm; angiography; cerebrovascular disorders;hemorrhage;
stroke; surgery; vasospasm
Bederson JB, Connolly ES Jr, Batjer HH, Dacey RG, DionJE,
Diringer MN, Duldner JE Jr, Harbaugh RE, Patel AB,Rosenwasser RH.
Guidelines for the management ofaneurysmal subarachnoid hemorrhage:
a statement for
healthcare professionals from a special writing group ofthe
Stroke Council, American Heart Association. Stroke2009: published
online before print January 22,
2009,10.1161/STROKEAHA.108.191395.
-
7/30/2019 Guidelines SAH AHA
5/71
1/12/2013 2009, American Heart Association. All rights
reserved.
This slide set was adapted from the
Guidelines for the Management ofAneurysmal Subarachnoid
Hemorrhagepaper
This guideline reflects a consensus of expert opinionfollowing
thorough literature review that consisted of alook at clinical
trials and other evidence related to the
management of subarachnoid hemorrhage.
-
7/30/2019 Guidelines SAH AHA
6/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Applying classification of recommendationsand levels of
evidence
-
7/30/2019 Guidelines SAH AHA
7/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Outline Introduction
Epidemiology
Acute Evaluation and MedicalManagement
Surgical and Endovascular Management
Management of Common In-HospitalSAH Complications
Summary and Conclusions
-
7/30/2019 Guidelines SAH AHA
8/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Introduction SAH is a common and devastating
condition
SAH affects up to 30,000 personsannually in the United States
(US)
Mortality rates are as high as 45% withsignificant morbidity
among survivors
These recommendations summarize thebest available evidence for
treatment ofpatients with aneurysmal SAH
-
7/30/2019 Guidelines SAH AHA
9/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Stroke
-
7/30/2019 Guidelines SAH AHA
10/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Aneurysm
-
7/30/2019 Guidelines SAH AHA
11/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Epidemiology SAH incidence varies greatly between
countries, from 2 cases/ 100,000 in
China to 22.5/100,000 in Finland Many cases of SAH are
misdiagnosed
Thus, the annual incidence ofaneurysmal SAH in the US may
exceed
30,000 Incidence increases with age, occurring
most commonly between 40 and 60years of age (mean age > 50
years)
-
7/30/2019 Guidelines SAH AHA
12/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Epidemiology SAH is ~1.6 times higher in women thanmen
Risk factors for SAH include
hypertension, smoking, female genderand heavy alcohol use
Cocaine-related SAH occurs in youngerpatients
Familial intracranial aneurysm (FIA)syndrome occurs when two
first-through third-degree relatives haveintracranial aneurysms
-
7/30/2019 Guidelines SAH AHA
13/71
1/12/2013 2009, American Heart Association. All rights
reserved.
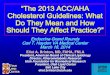
CT Scan non-contrast showing bloodin basal cisterns (SAH) so
calledStar-Sign
CT Scan courtesy: University of Texas Health Science Center at
San Antonio, Department of Neurosurgery
-
7/30/2019 Guidelines SAH AHA
14/71
1/12/2013 2009, American Heart Association. All rights
reserved.
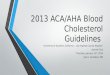
CT Scan of a 65 yo woman, Hunt andHess of 4 Subarachnoid
Hemorrhage
Arrow:Hyperintensesignal.Blood in thesubarachnoidspace
CT Scan courtesy: University of Texas Health Science Center at
San Antonio, Department of Neurosurgery
-
7/30/2019 Guidelines SAH AHA
15/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Angiogram - Giant ICA Aneurysm
Angio image courtsey: University of Texas Health Science Center
at San Antonio - Department of Neurosurgery
-
7/30/2019 Guidelines SAH AHA
16/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Prevention of SAH No randomized controlled trials haveexamined
whether treatment of medicalrisk factors reduces SAH occurrence
Hypertension is a common risk factorfor hemorrhagic stroke
Indirect evidence suggests that smokingcessation reduces risk
for SAH
Screening for asymptomatic intracranialaneurysms in the general
population isnot supported by the available literature
-
7/30/2019 Guidelines SAH AHA
17/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Recommendations for Preventionof SAH Class I Recommendations
The relationship between
hypertension and aneurysmal SAH isuncertain. However, treatment
of highblood pressure with antihypertensivemedication is
recommended to
prevent ischemic stroke andintracerebral hemorrhage,
cardiac,renal, and other end-organ injury(LOE A)
-
7/30/2019 Guidelines SAH AHA
18/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Recommendations for Preventionof SAH Class II
Recommendations
Cessation of smoking is reasonable to
reduce the risk of SAH, although evidencefor this association is
indirect (LOE B).
Screening of certain high-risk populationsfor unruptured
aneurysms is of uncertain
value (LOE B); advances in noninvasiveimaging may be used for
screening, butcatheter angiography remains the goldstandard when it
is clinically imperative toknow if an aneurysm exists.
-
7/30/2019 Guidelines SAH AHA
19/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Natural History and Outcome of anAneurysmal SAH 30-day mortality
rate after SAH ranges from 33-
50%
Severity of initial hemorrhage, age, sex, time totreatment, and
medical comorbidities impactSAH outcome
Aneurysm size, location in the posteriorcirculation, and
morphology may also impact
outcome Endovascular services at a given institution, the
volume of SAH patients treated, and the facilitywhere the
patient is first evaluated may alsoimpact outcome
-
7/30/2019 Guidelines SAH AHA
20/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Natural History of an AneurysmalSAH: Recommendations
Class I Recommendations
The severity of the initial bleed shouldbe determined rapidly as
it is the mostuseful indicator of outcome followinganeurysmal SAH
and grading scales
which heavily rely on this factor arehelpful in planning future
care withfamily and other physicians (LOE B)
-
7/30/2019 Guidelines SAH AHA
21/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Natural History of an AneurysmalSAH: Recommendations
Class I Recommendations Case review and prospective cohorts have
shown that
for untreated, ruptured aneurysms, there is at least a3% to 4%
risk of re-bleeding in the first 24 hours andpossibly significantly
higher, with a high percentageoccurring immediately (within 2 to 12
hours) after theinitial ictus, a 1% to 2% per day risk in the first
month,
and a long-term risk of 3% per year after 3 months.Urgent
evaluation and treatment of patients withsuspected SAH is therefore
recommended (LOE B)
-
7/30/2019 Guidelines SAH AHA
22/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Natural History of an AneurysmalSAH: Recommendations
Class II Recommendations
In triaging patients for aneurysm repair,
factors that can be useful in determiningthe risk of re-bleeding
include severity ofthe initial bleed, interval to admission,blood
pressure, gender, aneurysm
characteristics, hydrocephalus, earlyangiography, and the
presence of aventricular drain (LOE B)
-
7/30/2019 Guidelines SAH AHA
23/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Acute Evaluation - Diagnosis The worst headache of my life
is
described by ~80% of patients
Sentinel headache is described by ~20%
Nausea/vomiting, stiff neck, loss ofconsciousness, or focal
neurologicaldeficits may occur
Misdiagnosis of SAH occurred in as many
as 64% of cases prior to 1985 Recent data suggest an SAH
misdiagnosis rate of approximately 12%
-
7/30/2019 Guidelines SAH AHA
24/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Acute Evaluation - Diagnosis Importance of recognition of a
warning
or sentinel leak cannot be
overemphasized A high index of suspicion is warranted in
the ED
The diagnostic sensitivity of CT
scanning is not 100%, thus diagnosticlumbar puncture should be
performed ifthe initial CT scan is negative
-
7/30/2019 Guidelines SAH AHA
25/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Diagnosis of SAH -Recommendations Class I Recommendations
SAH is a medical emergency that isfrequently misdiagnosed. A
high level
of suspicion for SAH should exist inpatients with acute onset of
severeheadache (LOE B)
CT scanning for suspected SAH is
strongly recommended, and lumbarpuncture for analysis of
cerebrospinalfluid is strongly recommended whenthe CT scan is
negative (LOE B)
-
7/30/2019 Guidelines SAH AHA
26/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Diagnosis of SAHRecommendations Class I Recommendations
Selective cerebral angiography to documentthe presence and
anatomic features of
aneurysms is strongly recommended inpatients with documented SAH
(LOE B)
Class II Recommendations
MRA or CTA can serve as useful alternative
diagnostic tools when conventionalangiography cannot be
performed in atimely fashion (LOE B)
-
7/30/2019 Guidelines SAH AHA
27/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Acute EvaluationEmergency Evaluation Emergency medical services
(EMS) is first
medical contact in about 2/3 of SAH
patients EMS personnel should receive continuing
education regarding signs and symptomsand the importance of
rapid neurological
assessment in cases of possible SAH On-scene delays should be
avoided
Rapid transport and advanced notificationof the ED should
occur
-
7/30/2019 Guidelines SAH AHA
28/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Acute EvaluationEmergency Evaluation Airway, breathing, and
circulation should
be rapidly assessed and managed
Emergency care providers shouldevaluate SAH patients with an
acceptedneurologic assessment scale and record itin the ED Hunt and
Hess, Fisher Scale, Glasgow Coma Scale,
World Federation of Neurological Surgeons Scale.
Expedient transfer to an appropriatereferral center should be
considered ifnecessary
-
7/30/2019 Guidelines SAH AHA
29/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Emergency EvaluationRecommendations
Class II Recommendations
The degree of neurologicalimpairment using an accepted
SAHgrading system can be useful forprognosis and triage (LOE B)
A standardized ED managementprotocol for the evaluation of
patientswith headaches and other symptomsof potential SAH does not
currentlyexist and needs development (LOE C)
-
7/30/2019 Guidelines SAH AHA
30/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Acute Evaluation PreventingRe-bleeding
Up to 14% of SAH patients may
experience re-bleeding within 2 hours ofthe initial
hemorrhage
Re-bleeding was more common in thosewith a systolic blood
pressure
>160mm Hg Anti-fibrinolytic therapy may reduce re-
bleeding but has not been shown toimprove outcomes
-
7/30/2019 Guidelines SAH AHA
31/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Preventing Re-bleeding -Recommendations
Class I Recommendations
Blood pressure should be monitored andcontrolled to balance the
risk of strokes,hypertension-related re-bleeding, andmaintenance of
cerebral perfusion pressure(LOE B)
Class II Recommendations Bed rest alone is not enough to prevent
re-
bleeding after SAH. It may be considered asa component of a
broader treatment strategyalong with more definitive measures (LOE
B)
-
7/30/2019 Guidelines SAH AHA
32/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Preventing Re-bleeding -Recommendations
Class II Recommendations
Recent evidence suggests that earlytreatment with
antifibrinolytic agents,when combined with a program ofearly
aneurysm treatment followed by
discontinuation of the antifibrinolyticand prophylaxis against
hypovolemiaand vasospasm (LOE B)
-
7/30/2019 Guidelines SAH AHA
33/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Preventing Re-bleedingClass II Recommendations
Antifibrinolytic therapy to prevent
rebleeding may be considered incertain clinical situations,
e.g.,patients with a low risk ofvasospasm and/or a beneficialeffect
of delaying surgery (LOE B)
-
7/30/2019 Guidelines SAH AHA
34/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and EndovascularManagement of SAH Occluding aneurysms
using
endovascular coils was described in
1991 Improved outcomes have been linked tohospitals that provide
endovascularservices
Use of endovascular versus surgical
techniques varies greatly across centers Coil embolization is
associated with a
2.4% risk of aneurysmal perforation andan 8.5% risk of ischemic
complications
-
7/30/2019 Guidelines SAH AHA
35/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and EndovascularManagement of SAH
A study of 431 patients undergoingcoiling of a ruptured aneurysm
found anearly re-bleeding rate of 1.4%, with 100%mortality
The ISAT Trial reported a 1-year re-
hemorrhage rate of ~2.9% in aneurysmstreated with endovascular
therapy
Aneurysm size is an important predictorof hemorrhage risk
-
7/30/2019 Guidelines SAH AHA
36/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and EndovascularManagement of SAH
The Cooperative Study evaluated 979patients who underwent
intracranialsurgery only
Nine of 453 patients (2%) rebled aftersurgery
Nearly half (n=4) of these hemorrhagesoccurred in patients with
multipleaneurysms
-
7/30/2019 Guidelines SAH AHA
37/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and EndovascularManagement of SAH
In the International Subarachnoid
Aneurysm Trial (ISAT) post-treatmentSAH occurred at an
annualized rate of0.9% with surgical clipping, compared to2.9% with
endovascular treatment
The rate of incomplete obliteration andrecurrence appears
significantly lowerwith surgical clipping than withendovascular
treatment
-
7/30/2019 Guidelines SAH AHA
38/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and EndovascularManagement of SAH Increased time to
treatment is
associated with increased rates of
preoperative re-bleeding 0 to 3 days, 5.7% 4 to 6 days, 9.4% 7
to 10 days, 12.7% 11 to 14 days, 13.9% 15 to 32 days, 21.5%
Postoperative re-bleeding did not differamong time intervals
(1.6% overall)
-
7/30/2019 Guidelines SAH AHA
39/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and EndovascularManagement of SAH
Estimating the consequences of
complications attributable to anoperation may be possible from
dataregarding surgery for unrupturedaneurysms
In-hospital mortality rates vary from1.8% to 3.0% in large
multicenter studies
Adverse outcomes in survivors varyfrom 8.9% to 22.4%
-
7/30/2019 Guidelines SAH AHA
40/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and EndovascularManagement of SAH
The only large prospective, randomized
trial to date comparing surgery andendovascular techniques is
ISAT
At one year, there was no significantdifference in mortality
rates (8.1% vs.
10.1% endovascular vs. surgical) Disability rates were greater
in surgical
versus endovascular patients (21.6% vs.15.6%)
-
7/30/2019 Guidelines SAH AHA
41/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and EndovascularManagement of SAH Combined morbidity
and mortality was
significantly greater in surgically treatedpatients than in
those treated with
endovascular techniques (30.9% vs. 23.5%;absolute risk reduction
7.4%, P= 0.0001)
During the short follow-up period in ISAT there-bleeding rate
for coiling was 2.9% versus0.9% for surgery
There have been no randomized comparisonsof coiling versus
clipping for unrupturedaneurysms
-
7/30/2019 Guidelines SAH AHA
42/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Clipping
-
7/30/2019 Guidelines SAH AHA
43/71
1/12/2013 2009, American Heart Association. All rights
reserved.
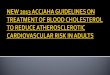
Left image arrow -Angio with Large aneurysmRight image arrow
Angio showing aneurysm post clipping
Angio Image Courtsey: The University of Texas Health Science
Center at San Antonio Department of Neurosurgery
-
7/30/2019 Guidelines SAH AHA
44/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and Endovascular
Management --Recommendations Class I Recommendations
Surgical clipping or endovascular coiling isstrongly recommended
to reduce the rate ofrebleeding after aneurysmal SAH (LOE B)
Wrapped or coated aneurysms as well asincompletely clipped or
coiled aneurysmshave an increased risk of re-hemorrhagecompared to
those completely occluded andtherefore require long-term
follow-upangiography. Complete obliteration of theaneurysm is
recommended wheneverpossible (LOE B)
-
7/30/2019 Guidelines SAH AHA
45/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and Endovascular
Management --Recommendations Class I Recommendations
For patients with ruptured aneurysms judged by an
experienced team of cerebrovascular surgeons andendovascular
practitioners to be technicallyamenable to both endovascular
coiling andneurosurgical clipping, endovascular coiling can
bebeneficial (LOE B)
Class II Recommendations
Individual characteristics of the patient and theaneurysm must
be considered in deciding the bestmeans of repair, and management
of patients incenters offering both techniques is
probablyrecommended (LOE B)
-
7/30/2019 Guidelines SAH AHA
46/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Coiling
-
7/30/2019 Guidelines SAH AHA
47/71
1/12/2013 2009, American Heart Association. All rights
reserved.
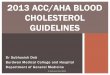
Coil system embolization: immediateresultAngio showing large
ICAaneurysm Same aneurysm - Post GDC Coiling
Angio Image Courtsey: The University of Texas Health Science
Center at San Antonio Department of Neurosurgery
-
7/30/2019 Guidelines SAH AHA
48/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Surgical and Endovascular
Management -Recommendations
Class II Recommendations
Although previous studies showed thatoverall outcome was not
different for earlyversus delayed surgery after SAH, earlytreatment
reduces the risk of rebleedingafter SAH, and newer methods may
increase
the effectiveness of early aneurysmtreatment. Early aneurysm
treatment isreasonable and is probably indicated in themajority of
cases (LOE B)
-
7/30/2019 Guidelines SAH AHA
49/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Hospital/Systems of Care Treatment volume is an important
determinant of outcome for intracranialaneurysms higher volume
equals
lower mortality This effect may be more important for
patients with unruptured aneurysmsthan for those with ruptured
aneurysms
It is uncertain whether the benefits ofreceiving care at a
high-volume centerwould outweigh the costs and risks oftransfer
-
7/30/2019 Guidelines SAH AHA
50/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Hospital/Systems of Care --Recommendations
Class II Recommendations
Early referral to high-volume centersthat have both
experiencedcerebrovascular surgeons andendovascular specialists
is
reasonable (LOE B)
-
7/30/2019 Guidelines SAH AHA
51/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of Common In-Hospital SAH Complications
Common issues related to in-
hospital management of SAHinclude: Anesthetic Management
Cerebral Vasospasm
Hydrocephalus Seizures Hyponatremia
-
7/30/2019 Guidelines SAH AHA
52/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Anesthetic Management During
Surgical and EndovascularTreatments
Goals of intraoperative anesthetic
management during aneurysm treatmentinclude:
limiting the risk of intraproceduralaneurysm rupture
protecting the brain against ischemicinjury
-
7/30/2019 Guidelines SAH AHA
53/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Anesthetic Management --Recommendations
Class II Recommendations Minimizing the degree and duration
of
intraoperative hypotension during aneurysmsurgery is probably
indicated (LOE B)
There are insufficient data onpharmacological strategies and
inducedhypertension during temporary vessel
occlusion to make specificrecommendations, but there may
beinstances where their use can be consideredreasonable (LOE C)
-
7/30/2019 Guidelines SAH AHA
54/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Anesthetic Management --Recommendations
Class III Recommendations
Induced hypothermia duringaneurysm surgery may be areasonable
option in some cases butis not routinely recommended (LOE B)
-
7/30/2019 Guidelines SAH AHA
55/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of CerebralVasospasm after SAH
Following aneurysmal SAH, angiographicvasospasm is seen in 30%
to 70% of patients
Typical onset is 3 to 5 days after thehemorrhage, maximal
narrowing at 5 to 14 days,and a gradual resolution over 2 to 4
weeks
15% to 20% of patients with delayed neurologicdeficits suffer
stroke or die from vasospasm
despite maximal therapy The index of suspicion needs to be
higher in
poor grade patients even with subtle changesin neurological
exam
-
7/30/2019 Guidelines SAH AHA
56/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of CerebralVasospasm after SAH
The literature is inconclusive regardingthe sensitivity and
specificity of TCDmonitoring
However, severe spasm can beidentified with fairly high
reliability usingTCD monitoring
Other modalities such as diffusionperfusion, MRI, and xenon-CT
cerebralperfusion studies may becomplementary in guiding
management
-
7/30/2019 Guidelines SAH AHA
57/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of CerebralVasospasm after SAH
Hypertensive hypervolemichemodilution (HHH) therapy has becomea
mainstay in the management ofcerebral vasospasm
Only one randomized study has beenperformed to assess its
efficacy
Two small single-center prospectiverandomized studies strongly
suggestthat avoiding hypovolemia is advisable,but there is no
evidence for prophylactichyperdynamic therapy
-
7/30/2019 Guidelines SAH AHA
58/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of CerebralVasospasm after SAH
Calcium-channel blockers, particularlynimodipine, have been
approved for usefor treatment of vasospasm
However, the reduction in morbidity andimprovement in functional
outcome mayhave been due more to cerebralprotection than actual
effect on the
cerebral vasculature Intravenous nicardipine interestingly
showed a 30% reduction in spasm butno improvement in outcome
-
7/30/2019 Guidelines SAH AHA
59/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of CerebralVasospasm after SAH
Balloon angioplasty has been shown tobe effective in reversing
cerebral
vasospasm in large proximal conductingvessels but has not been
shown toimprove ultimate outcome
Angioplasty is not effective or safe indistal perforating
branches beyond
second-order segments Angioplasty is effective in reducing
angiographic spasm, promoting anincrease in CBF, and reducing
deficits
-
7/30/2019 Guidelines SAH AHA
60/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Cerebral Vasospasm --Recommendations
Class I Recommendations
Oral nimodipine is stronglyrecommended to reduce pooroutcome
related to aneurysmalsubarachnoid hemorrhage (LOE A)
The value of other calciumantagonists, whether
administeredorally or intravenously, remainsuncertain
-
7/30/2019 Guidelines SAH AHA
61/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Cerebral Vasospasm --Recommendations
Class II Recommendations Treatment of cerebral vasospasm
begins
with early management of the rupturedaneurysm, and in most cases
maintainingnormal circulating blood volume andavoiding hypovolemia
is probably indicated(LOE B)
One reasonable approach to symptomaticcerebral vasospasm is
volume expansion,induction of hypertension and
hemodilution[Triple-H therapy] (LOE B)
-
7/30/2019 Guidelines SAH AHA
62/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Cerebral Vasospasm --Recommendations
Class II Recommendations
Alternatively, cerebral angioplastyand/or selective
intraarterialvasodilator therapy may also bereasonable, either
following, together
with, or in the place of, Triple-Htherapy depending on the
clinicalscenario (LOE B)
-
7/30/2019 Guidelines SAH AHA
63/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of HydrocephalusAssociated With SAH
Acute hydrocephalus (ventricular enlargementwithin 72 hours)
occurs in about 20% to 30% of
SAH patients The ventricular enlargement is often, but not
always, accompanied by intraventricular blood Acute
hydrocephalus is more frequent in
patients with poor clinical grade, and higher
Fischer Scale scores Two single-center series suggested that
routine
fenestration of the lamina terminalis reducesthe incidence of
chronic hydrocephalus
-
7/30/2019 Guidelines SAH AHA
64/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of Hydrocephalus --Recommendations
Class I Recommendation
Temporary or permanent CSF diversion isrecommended in
symptomatic patients withchronic hydrocephalus following SAH(LOE
B)
Class II Recommendation
Ventriculostomy can be beneficial in patientswith
ventriculomegaly and diminished levelof consciousness following
acute SAH(LOE B)
-
7/30/2019 Guidelines SAH AHA
65/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of SeizuresAssociated With SAH
A large number of seizure-like episodes areassociated with
aneurysmal rupture
It is unclear, however, whether all theseepisodes are truly
epileptic
Retrospective reviews report that early seizuresoccur in 6% to
18% of SAH patients
Non-convulsive seizures may occur in 19% ofstuporous or comatose
SAH patients
The relationship between seizures and outcomeis uncertain
-
7/30/2019 Guidelines SAH AHA
66/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of Seizures --Recommendations
Class II Recommendations The administration of prophylactic
anticonvulsants may be considered in theimmediate
posthemorrhagic period (LOE B)
Class III Recommendations The routine long-term use of
anticonvulsants
is not recommended (LOE B) but may be considered for patients
with risk
factors such as prior seizure, parenchymalhematoma, infarct, or
MCA aneurysms(Class II, LOE B)
-
7/30/2019 Guidelines SAH AHA
67/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of Hyponatremiaand Volume Contraction
Hyponatremia occurs in 10-30% of SAHpatients
Hyponatremia has been associated withexcessive natriuresis and
volumecontraction
Volume contraction has been linked tosymptomatic vasospasm
Administration of large amounts offluids (hypervolemic
therapy)ameliorates volume contraction
-
7/30/2019 Guidelines SAH AHA
68/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of Hyponatremia --Recommendations
Class I Recommendations Administration of large volumes of
hypotonic fluids and intravascular volumecontraction should
generally be avoidedfollowing SAH (LOE B)
Class II Recommendations Monitoring volume status in certain
patients
with recent SAH using some combination ofcentral venous
pressure, pulmonary arterywedge pressure, fluid balance, and
bodyweight is reasonable as is treatment ofvolume contraction with
isotonic fluids(LOE B)
-
7/30/2019 Guidelines SAH AHA
69/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Management of Hyponatremia --Recommendations
Class II Recommendations
The use of fludrocortisone acetateand hypertonic saline is
reasonablefor correcting hyponatremia (LOE B)
In some instances, it may be
reasonable to reduce fluidadministration to maintain aeuvolemic
state (LOE B)
-
7/30/2019 Guidelines SAH AHA
70/71
1/12/2013 2009, American Heart Association. All rights
reserved.
Summary and Conclusions
The current standard of practice calls for
microsurgical clipping or endovascularcoiling of the aneurysm
neck wheneverpossible
Treatment morbidity is determined bynumerous factors, including
patient,aneurysm, and institutionalfactors
-
7/30/2019 Guidelines SAH AHA
71/71
Summary and Conclusions
Favorable outcomesare more likely ininstitutions that treat high
volumes of
patients with SAH, in institutions thatoffer endovascular
services, and inselected patients whose aneurysms arecoiled rather
than clipped
Optimal treatment requires availability of
both experienced cerebrovascularsurgeons and endovascular
surgeonsworking in a collaborative effort toevaluate each case of
SAH