Embed Size (px)
Citation preview

HAPSHUNTER AREA PATHOLOGY SERVICE
news
Inside this issue• Contacting
Pathology North
• Pathology North’s new Coffs Harbour Collection Centre
• INR series tests
• New book on Abnormal Laboratory tests
• Northern Sydney Awards
• Research into the effects of snake venom on the haemostatic system
• QF – The blood test for TB infection
• Anti-RNA Polymerase III Antibodies
• PTHrP
• Summer and Infectious Diseases – Salmonella
MID NoRTH CoAST NoRTHERN RIVERS

FRoM THE DIRECToR
Every time I believe that I have completed my editorial for this
Pathology North Newsletter some further development
occurs to compromise the completeness or accuracy of my comments. No doubt the time to publication will also add its share of antiquity to the detail.
There can be no revision now however as
deadlines are here.
Let me acknowledge some things that you may take for
granted or already know.
I am pleased to be the Director of Pathology North. I am excited by the prospect of delivering better care to the patients of northern NSW. I believe that all Pathology North staff are likewise, committed to this endeavour.
Pathology North is in the late stage of developing an Expression of Interest for a tender for a new Laboratory Information System. This EoI is likely to be mature, in early 2012, with the hope that serious progress in development and implementation will be demonstrated quickly thereafter.
We are beginning the processes for ‘harmonising’ our individual local-regional services. These changes will be communicated to our clients well before any implementation, and are only considered for the benefit of enhanced service, efficiency of operation and organisational identity.
We are working hard to fill all vacant specialist positions throughout Pathology North laboratories. Whilst it is our desire to maintain local onsite pathologists to serve local clinicians we also have the benefit of our large
geographically dispersed pool of expert pathologists, providing a great deal of expertise across all pathology specialties. As well as many other significant services, Pathology North provides, through our Division of Molecular Genetics, one of the largest somatic cancer mutation services in Australia. We also employ the largest number of laboratory immunologists in regional NSW, and have a large group of haematologists, clinical chemists and anatomical pathologists on staff.
We all know that there has been some uncertainty in the NSW health services, induced by change of Government and the subsequent Ministry of Health rearrangements. This uncertainty has been felt by pathology, no less than other clinical services. The government has announced its intention of developing a business case for the production of Pathology NSW, coalescing the Analytical Laboratory, Forensic Medicine and four state pathology clusters into a single entity. The activity of the Ministry of Health, toward pathology, has lately been directed to developing new governance structures for public pathology services and it is likely that these will be in place by early 2012. Although the dramatic changes induced by the National Health Reform implementation in NSW, and subsequent government change, have been challenging, to our understanding and patience, Pathology North has continued to deliver improving service to our patients throughout this time.
I thank Pathology North staff for their commitment and integrity. I thank our clients and patients for their support and patience.
Please have a safe and enjoyable Christmas and New Year. We look forward to working for you all next year.
Dr. Stephen Braye Director, Pathology North
Merry Christmas!

CoNTACTING PATHoLoGY NoRTHThe formation of Pathology North is through the amalgamation of the existing pathology services of:
• Pathology New England (PNE)
• Hunter Area Pathology Services (HAPS)
• Pacific Laboratory Medicine Services (PaLMS)
• Mid-North Coast Pathology Service
• Northern Rivers Pathology Service
For more information, including Collection Centres, please visit:
www.pathologynorth.com.au
or
www.palms.com.au
www.pathologynewengland.com.au
www.haps.nsw.gov.au
NoRTHERN SYDNEY AWARDSDr. Anthony Gill, PaLMS Anatomical Pathology, was awarded the 2011 Benjamin Castleman award by the United States and Canadian Academy of Pathology (USCAP). This award is given in recognition of the most outstanding publication in the field of human pathology by a first author under the age of 40 and is considered the premier award for young researchers in the field of anatomical pathology. The paper for which the award was given was:
Gill AJ, Chou A, Vilain R, Clarkson A, Lui M, Jin R, Tobias V, Samra J, Goldstein D, Smith C, Sioson L, Parker N, Smith RC, Sywak M, Sidhu SB, Ma Wyatt J, Robinson BG, Benn DE, Clifton-Bligh RJ Immunohistochemistry for SDHB divides Gastrointestinal Stromal Tumors (GISTs) into two distinct types. American Journal of Surgical Pathology 2010 34:636-44 describes a new and highly clinically significant type of tumour known as the “Type 2 (SDHB negative) GIST”.
Pictured at right, Dr. Anthony Gill, with David Louis Pathologist in chief, Mass Gen Hospital, when he was
presenting in San Antonio Texas.
Dr Julie Paik (registrar Anatomical Pathology) was recognised for her
achievement, being awarded the inaugural Jeanette Philips award. This award is granted by the Australasian Endocrine Pathology Society in recognition of the best presentation of original research by a first author in the field of endocrine pathology.
The award is named for A/Prof Jeanette Philips who was a long serving and well
respected anatomical pathologist at PaLMS Royal North Shore Hospital.
Pictured above left, Dr Julie Paik receiving the inaugural Jeanette Philips award. This award was presented by Jeanette’s husband, Dr Ron Joffe.
Coffs Harbour ColleCtIon CentreWe are pleased to announce the opening of our new Coffs Harbour Collection Centre located at 1/40 Little Street, Coffs Harbour. For further information, please contact 02 6657 7500.
Inr serIes testsFor all INR series tests, the following rule applies.
‘A doctor can issue a patient with a referral for unlimited INR’s for a period of up to 6 months from the date of the request. After the 6 months has expired, a new referral form must be issued’.
NEW Book oN ABNoRMAL LABoRAToRY TESTSHunter Area Pathology Service is pleased to announce the recent publication of Professor kellerman’s latest book entitled ‘Abnormal laboratory Tests, 3rd Edition, 2011, McGraw-Hill’. Please contact our Executive office 4921 4444 for its availability.
3

However, contrary to previous studies using traditional clotting tests and factor substrates, the venoms differed in their calcium requirements. Venom potency also varied depending on the assay used, with ETP ranging from least potent with Taipan venom to intermediate with tiger snake and Stephen’s banded snake (Hoplocephalus stephensii) venoms to most potent with brown snake and rough-scale snake (Tropidechis carinatus) venoms. Antivenom neutralized the thrombin generating capacity but not the prothrombin substrate cleaving ability of all venoms.
We went on to examine the effects of VICC on the human haemostatic system in vivo by analysing changes in clotting parameters and factor levels over time in 130 patients recruited to the Australian Snakebite Project. Complete VICC occurred in 86% of cases and was characterised by near/total depletion of fibrinogen, factor V and VIII, as well as international normalised ratio and activated partial thromboplastin times that exceeded the upper limits of detection within two hours of the snake bite, suggesting that antivenom cannot be practically administered in time to prevent VICC. Curiously, prothrombin levels never fell to below 60%
of normal, indicating that the toxins were quickly eliminated or inactivated. onset of VICC was
twice as rapid for envenomation with brown snakes (Pseudonaja spp.)
compared to the tiger snake group, most likely due to the
time required for formation of the Xa snake-toxin Va human complex in the latter compared to the ready made Xa snake-toxin
Va snake-toxin complex in the former. Regardless, resolution of VICC occurred within 24 hours and was
independent of the time of antivenom administration.
our results suggest that Australasian elapid prothrombin
activators have a potent but short duration of action, and raise questions
about the effectiveness of antivenom for the treatment of VICC.
Dr Lisa Lincz [email protected] 5
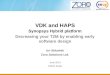
4 RESEARCH INTo THE EFFECTS oF
snake venom oN THE HAEMoSTATIC SYSTEMLisa Lincz, Margaret O’Leary, Fiona Scorgie, Michael Seldon, Geoff Isbister Collaboration between the Departments of Haematology and Clinical Toxicology & Pharmacology at the CMN
Australia has a reputation for being home to the world’s most venomous collection of snakes. Almost all venomous terrestrial snakes in Australia belong to the Elapidae family, of which there are five major groups of clinical importance: brown snakes (genus Pseudonaja), tiger snakes (genus Notechis), black snakes (genus Pseudechis), death adders (genus Acanthophis) and Taipans (genus Oxyuranus). Estimates suggest that there are between 500 and 3000 snake bites annually, with antivenom required in about 200 to 500 cases. Although uncommon, snake envenomation is a potentially life-threatening medical condition that can affect numerous systems within the body, causing neurotoxicity, haematotoxicity, myotoxicity, and/or renal damage. Almost all Australian elapids contain toxins that effect blood clotting, ie. pro- or anticoagulant toxins, with coagulopathy being the most common important clinical effect, accounting for over 80% of patients admitted to hospital with snake envenoming.
Venomous snakes worldwide are capable of inducing a venom induced consumption coagulopathy (VICC) in humans with associated morbidity and mortality from bleeding. Despite isolation and characterization of numerous prothrombin and coagulation factor activators, as well as thrombin-like enzymes, our understanding of the procoagulant process in human envenoming remains limited. This is largely due to the lack of a standardised approach to in vitro testing of snake venom clotting effects, and a paucity of data describing the clinical manifestations of snake envenoming in humans – VICC in vivo. In a number of instances this has hampered our understanding, development and clinical application of antivenom therapy for snakebite coagulopathy.
We have developed a novel modification of the traditional endogenous thrombin potential (ETP) assay using procoagulant snake venoms to trigger thrombin production. Using this assay we demonstrated that most Elapidae venoms that contain prothrombinase- like toxins were able to initiate thrombin generation in either the absence or presence of calcium.

kEY PoINTS:• Qft is six times more precise than
TST in identifying people who will progress to active TB disease.
• Qft is significantly more sensitive, nearly halving the number of infected people missed by TST.
• Qft is >99 percent specific, indicating that positive readings represents true infection; the very high specificity value (99.2%) means QFT virtually eliminates false-positive readings (false positives by TST range from 3 percent to 65 percent of all persons tested, dependent upon the population).
• QFT is a controlled laboratory test, with results showing that an individual is or is not infected with the TB bacterium with a high degree of accuracy. In contrast, the TST is a very subjective procedure, which can lead to incorrect diagnosis.
• QFT improves risk management with quick, accurate results. In comparison, TST must be read 48 to 72 hours after injection. Many people do not return for this second clinical exam.
• QFT is highly specific for diagnosis of infection with the bacteria responsible for tuberculosis, Mycobacterium tuberculosis. It is unaffected by vaccinations (such as the Bacillus Calmette-Guérin vaccination) and most environmental bacteria that adversely affect TST results.
• QFT is cost-efficient and requires only one patient visit. Results may be available from the lab within 24 hours.5
QFT – THE BLooD TEST FoR TB INFECTIoNTB is a contagious disease caused by Mycobacterium tuberculosis. Settling into the lungs, the spine, the kidneys and the brain, tuberculosis can be fatal without proper treatment.
What is the difference between tb infection (latent tb) and active tb?
Not everyone who becomes infected with TB bacteria develops TB disease. A person who is infected with the bacterium that causes TB, but who shows no symptoms and is not sick with the disease, is regarded as having latent TB infection (LTBI).
Approximately 1 in every 10 persons infected with TB bacteria will go on to develop active TB disease. Individuals with LTBI and a compromised immune system are more likely to progress to active TB. Active TB occurs when the TB bacteria overcome a person’s immune system and symptoms (e.g. cough, night sweats and weight loss) appear. A person who has active pulmonary TB is contagious.
QuantiFERoN®-TB Gold (QFT) is a simple blood test that accurately identifies people infected with Mycobacterium tuberculosis, the causative agent of Tuberculosis (TB). QFT is a modern alternative to the 110 year old Tuberculin Skin Test (TST), also known as the Mantoux. It uses human whole blood, with patented assay technology based on the measurement of Interferon-gamma (IFN-y) secreted from stimulated T-cells previously exposed to M. tuberculosis.
In data from a meta-analysis of existing literature, published April 6th in CHEST, the official journal of the American College of Chest Physicians, Interferon Gamma Release Assays (IGRAs), including QFT, was demonstrated as being superior to the previous standard in diagnostics, the 100+ year-old tuberculin skin test (TST), for detecting confirmed active TB disease.
For more information on QFT please contact the Immunology Laboratory at HAPS on 02 4921 4018.
Dr Karla Lemmert Immunology [email protected]

6Why order the test?
Approximately 5% of patients with scleroderma will develop renal crisis. Most (>75%) of these patients have, or will have, the “diffuse” subtype of scleroderma. Penn et al1 found this antibody in 59% of 95 patients with renal crisis. This group found the antibody in 12% of patients without renal crisis during the period of follow up (median of three years).
Using this data:
of 100 people with Scleroderma:
– 95 will never get renal crisis
– 5 will get renal crisis
of those 5 with renal crisis:
– 3 will have anti-RNAPIII antibodies
– 2 will not have antibodies (“false negative”)
of the 95 without renal crisis:
– 11 will have antibodies (“false positive”)
asking for the test
Serum (red top), no special requirements for collection. Currently no charge for Medicare eligible patients (item 71119).
NB. This test (RNAPIII) should be distinguished from anti-RNP. Anti-RNP (also called U1RNP) is associated with Mixed (or “Undifferentiated) Connective Tissue Disorder and/or Systemic Lupus Erythematosus. Patients with anti-RNP antibodies may also have scleroderma, so this is an obvious source of confusion. Anti-RNP is routinely included in the ENA (Extractable Nuclear Antigen) testing panel, whereas anti-RNAPIII is not.
Dr Theo de Malmanche Immunology [email protected]
What does the test detect?
Patients with Anti-RNA Polymerase III antibodies detected in their blood are at risk of “Scleroderma Renal Crisis”. Scleroderma renal crisis is accelerated hypertension, which leads to a life-threatening cycle of worsening renal failure and hypertension.
This type of renal crisis is far more common in patients with Scleroderma (also called Systemic Sclerosis, SSc). Patients with the “Diffuse” type of Scleroderma are more at risk than those with the “Limited” type (also called CREST syndrome).
Which patients should have this test?
Any patient with:
• possible scleroderma, and/or
• progressive hypertension, and/or
• worsening renal function of unknown cause
Renal crisis may precede the diagnosis of scleroderma.
What should I do with a positive result?
Any scleroderma patient with hypertension or detected anti-RNAPIII antibodies should seriously be considered for Angiotensin Converting Enzyme Inhibitor anti-hypertensive medications (“ACE inhibitors”). These patients should also have frequent blood pressure (BP) monitoring, and nephrologist review may be indicated. These antibodies are also hardly ever present in patients without SSc, so the presence is also confirmatory for the presence of SSc. These patients might also have less lung disease and more skin involvement than other SSc patients.
Patients with scleroderma, particularly those with these antibodies, should avoid known precipitants of renal injury such as dehydration and some medications.
ANTI-RNA PoLYMERASE III ANTIBoDIES

Clinical significance
Parathyroid Hormone Related Peptide (PTHrP) is a peptide hormone of 141 amino acid residues with the N-terminal 1-13 residues showing some homology with PTH. It binds to the same PTH-1 receptors in bone and kidney as PTH, producing the same biological effect. PTHrP is widely expressed in malignant tumours, as well as a wide range of normal tissues. PTHrP is measurable at very low levels in most normal subjects and levels are not suppressed in primary hyperparathyroidism or postsurgical hypoparathyroidism.
Assays for PTHrP have the potential to be very useful in the differential diagnosis of hypercalcaemia, distinguishing between the two common causes, primary hyperparathyroidism and humoural hypercalcaemia of malignancy. Individuals with hypercalcaemia of malignancy have the biochemical features of primary hyperparathyroidism – hypercalcaemia, hypophosphataemia and raised alkaline phosphatase – but with a low serum PTH level.
Current reference interval for PTHrP is <1.3pmol/L (Ikeda et al 1994).
PtHrP aassay and potential sources of variability
The PaLMS Endocrine laboratory measures PTHrP by immunoradiometric assay (IRMA), with immobilised monoclonal antibodies on a polystyrene bead solid phase. The largest source of variability stems from pre-analytical sources. The highly labile nature of PTHrP requires strict collection and transport conditions and any failure in compliance may lead to diagnostic inaccuracy. Samples collected in tubes without aprotinin will not be accepted for this assay.
PaLMS Endocrine Laboratory RNSH is currently the only known laboratory performing this assay in Australia. Assays for PTHrP are performed fortnightly depending upon demand. Currently, with no local suppliers, reagents are sourced directly from overseas manufacturers. A fee of $100 per test is charged to cover costs. Please note that there is no MBS item number for PTHrP.
specimen requirements
Sample requirements are 3mL blood in k2EDTA tubes with two stabilisers, aprotinin (0.33μg) and leupeptin (10μg) per tube. These tubes must be immediately placed in and kept on ice until centrifugation. Samples are to be centrifuged ASAP, the plasma separated, and then the plasma frozen at -20 degrees C. Plasma samples must remain frozen in transit to PaLMS Endocrine Laboratory. Repeated Freeze/thaw cycles should be avoided.
The required collection tubes are not commercially available and specifically produced by our laboratory. Collection tubes are available from PaLMS upon request and should be stored at 4-8 degrees C until required. Instructions to prepare collection tubes are available on request.
For enquiries please contact Peter Ward, Managing Scientist Chemical Pathology PaLMS Northern Sydney, on (02) 99267505 or [email protected].
references
Strewler GJ: The physiology of parathyroid hormone-related protein. NEJM 342:177-185, 2000.
Ikeda k et al. Development of a two site IRMA for PTHrP: Evidence for elevated levels in plasma from patients with
Adult T-Cell Leukaemia/Lymphoma and B-Cell Lymphoma. JCEM 79, 5:1322-1327, 1994.
Pandian MR et al, Clin Chem 38:282, 1992.
Cameron Woods, BSc Biochemistry [email protected]
Cameron has worked for PaLMS for the past nine years and is currently the Senior Hospital Scientist in charge of the PaLMS Endocrine Laboratory and Scientific Fellow PaLMS Biochemistry.
PTHrP

With the end of winter, respiratory infections usually
decrease while gastrointestinal infections increase. Why gut
infections seem more prevalent in warmer months is not clear but
temperature abuse of food prepared during the warmer months is often blamed.
Some foods are traditionally associated with particular bacterial infections; poultry, for example, with Campylobacter and Salmonella. In those States & Territories (not including NSW) where Campylobacter is a notifiable disease, it is by far the commonest cause of reported gastrointestinal disease. With the introduction of the Primary Production and Processing Standard for Poultry Meat in May this year, Australia can expect a marked decrease in the number of cases of Campylobacter infections. This was the experience in New Zealand after their equivalent program commenced in 2006. In the meantime the traditional “buyer beware” remains the essential message from the recent Food Safety Week http://www.foodsafety.asn.au/foodsafetyweek/ and no doubt we can look forward in the coming weeks across Australia to the annual Christmas messages from health ministers advising us on the safe cooking of turkeys.
The situation with Salmonella is somewhat different. While contaminated poultry & cross contamination from raw poultry to other foods remain real hazards, experience over recent years has been that Salmonella can contaminate vegetables, fruits & almost any food production process. In 2006, for example, rockmelons were associated with cases of Salmonella infection in the Hunter & New England region.
The particular emphasis of Food Safety Week this year, though, was not on any one pathogen, but rather about protection of vulnerable people from foodborne infection. If any single pathogen is especially dangerous for this group it’s Listeria monocytogenes. Anyone from the mid-60s on is classed as vulnerable, along with the immunosuppressed (including those with cancer, leukaemia, AIDS, diabetes, liver or kidney disease) and, of course, unborn babies.
SUMMER AND
INFECTIoUS DISEASES – SALMoNELLA
The official list of risky foods is long http://www.foodstandards.gov.au/_srcfiles/Listeria_Q_%20A_Version_FINAL.pdf. Survey data suggest even for products for which the Food Standards permit no detectable Listeria (eg. packaged cooked cured/salted meat at the factory door) even more types of food can be hazardous.
People severely ill from Listeria are ordinarily diagnosed by blood or CSF culture but in cases of gastroenteritis it is hard to give all-encompassing advice on when to test faeces and what to ask for. Studies suggest that doctors will order stool examination in children first-up but in adults only if symptoms are prolonged or severe e.g. associated with bleeding or fever. This is not an unreasonable approach, given that most often gastroenteritis is a short duration disease and caused by viruses, especially norovrius.
When requesting examination for microbial pathogens, the usual option is to ask for “microscopy & culture”. At HAPS this will result in culture for Salmonella, Campylobacter and Yersinia (if there are numerous white cells) or pcr for Shiga-toxin producing E. Coli (if there are numerous red cells). A request for virology will lead to antigen detection for rotavirus, adenovirus and norovirus. Unless more extensive parasitological examination is asked for, a request for parasite examination of stool will only trigger detection for the antigens of Giardia and Crytposporidium. As always, clinical notes can be very useful in guiding the laboratory’s decisions: a history of overseas travel, for example, will prompt examination for Vibrio species.
Dr. Rodney Givney Microbiology