Embed Size (px)
Citation preview
January 2013 no. 5
2013 Healthcare Common Procedure Coding System (HCPCS) Special BulletinHCPCS Special BulletinHCPCS Special Bulletin
2013 HCPCS ImplementationOn January 1, 2013, the Texas Medicaid & Healthcare Partnership (TMHP) applied the 2013 annual Healthcare Common Procedure Coding System (HCPCS) updates that are effective for dates of service on or after January 1, 2013.
This combined Special Bulletin includes the HCPCS updates for Texas Medicaid and the Children with Special Health Care Needs (CSHCN) Services Program. This bulletin is intended to notify providers of program and coding changes related to the 2013 updates for HCPCS and Current Procedural Terminology (CPT®).
All providers are encouraged to review the “General Information” section of this bulletin. Policy updates for a specific program or provider type are discussed in designated sections of the bulletin.
Rate Hearings and Expenditure ReviewNew and increased benefits that are adopted by Texas Medicaid must complete the rate hearing process in order to receive comments on new and increased Texas Medicaid reimbursement rates. The CSHCN Services Program reviews the adopted Texas Medicaid rates to determine whether the rates are fiscally feasible for the CSHCN Services Program.
The proposed expenditures for Texas Medicaid and the CSHCN Services Program are reviewed by the Texas Legislative Budget Board (LBB), and upon approval of expenditures, Texas Medicaid and the CSHCN Services Program implement the approved rates.
All new, revised, and discontinued 2013 HCPCS procedure codes are effective for dates of service on or after January 1, 2013. The new procedure codes that are designated with asterisks (*) in the “Texas Medicaid Allowable” and the “CSHCN Services Program Allowable” columns of the table located on page 23 of this bulletin must complete the rate hearing process, and expenditures must be approved before the rates are adopted by Texas Medicaid and the CSHCN Services Program. Providers will be notified in a future banner message or web article if a new procedure code will not be reimbursed because the expenditures were not approved.
Providers may refer to the following resources for more information about the public rate hearings and approval of expenditures:
• Title 2 Human Resources Code, §32.0282, and Title 1 Texas Administrative Code (TAC), §355.201, which require public hearings
• House Bill 1, 80th Legislature, Regular Session, 2007, Article II, Department of State Health Services, Rider 79a
Important: To avoid fraudulent billing, providers must submit the procedure codes that are most appropriate for the services provided.
Code Updates Web PageProviders are encouraged to refer to the TMHP Code Updates – HCPCS web page at www.tmhp.com/Pages/CodeUpdates/HCPCS_2012.aspx for reimbursement rates, quarterly HCPCS updates, and all other notifications about HCPCS procedure codes.
Copyright AcknowledgmentsUse of the AMA’s copyrighted CPT® is allowed in this publication with the following disclosure:
“Current Procedural Terminology (CPT) is copyright 2012 American Medical Association. All rights reserved. No fee schedules, basic units, relative
values, or related listings are included in CPT. The AMA assumes no liability for the data contained herein. Applicable Federal Acquisition Regula
tion System/ Defense Federal Acquisition Regulation Supplement (FARS/DFARS) apply.”
The American Dental Association requires the following copyright notice in all publications containing Current Dental Terminology (CDT) codes:
“Current Dental Terminology (including procedure codes, nomenclature, descriptors, and other data contained therein) is copyright © 2011 American
Dental Association. All rights reserved. Applicable FARS/DFARS apply.”
ALL PROVIDERS 1
2013 HCPCS Implementation .................................................................................................................... 1Rate Hearings and Expenditure Review .................................................................................................... 1Code Updates Web Page .......................................................................................................................... 1
Medicaid Fee-for-Service and Managed Care Providers 3
Texas Medicaid HCPCS Updates ..............................................................................................................3
Behavioral Health Services Providers 10
Texas Medicaid Behavioral Health Services ............................................................................................10New and Deleted Procedure Codes ........................................................................................................10Behavioral Health Services Procedure Code Changes .......................................................................... 11
DSHS Family Planning Providers 12
DSHS Family Planning Program Benefit Changes .................................................................................. 12
Home Health and Comprehensive Care Program Providers 13
Home Health Services Benefit Changes ................................................................................................. 13CCP Services Benefit Changes ............................................................................................................... 13
Texas Health Steps Dental Providers 14
THSteps Dental Benefit Changes ............................................................................................................ 14
Texas Women’s Health Program Providers 15
Texas Women’s Health Program Benefit Changes .................................................................................. 15
Children With Special Health Care Needs (CSHCN) Services Program Providers 16
CSHCN Services Program Updates ........................................................................................................16CSHCN Services Program Benefit Changes ..........................................................................................16
All Code Changes: Added, Revised, Replacement, and Discontinued 23
2012 HCPCS Procedure Code Additions ................................................................................................23Discontinued Procedure Codes ...............................................................................................................38Replacement Procedure Codes ...............................................................................................................39Procedure Code Description Changes ....................................................................................................39Modifiers .................................................................................................................................................. 41
Prior Authorization Changes 41
Authorization or Prior Authorization ......................................................................................................... 41
InSIDE
Texas Medicaid Special Bulletin, No. 5 2 2013 HCPCS Special BulletinCPT only copyright 2012 American Medical Association. All rights reserved.
Medicaid Fee-For-Service and Managed care ProviderS
Texas Medicaid HCPCS UpdatesThe 2013 Healthcare Common Procedure Coding System (HCPCS) updates including prior authorization updates for Texas Medicaid are included in the HCPCS tables in the “All Code Changes” section of this bulletin beginning on page 23. The 2013 HCPCS deletions and replacements are effective January 1, 2013, for dates of service on or after January 1, 2013, for Texas Medicaid. Providers may refer to the “General Information” section for more information.
authorization and Prior authorization update reminderEffective January 1, 2013, the 2013 HCPCS deleted procedure codes are no longer reimbursed by Texas Medicaid. Unless otherwise indicated on page 38 of this bulletin, providers who have received prior authorization for dates of service that occur on, after, or encompass January 1, 2013, must submit a written request on the appropriate, completed Texas Medicaid prior authorization request form in order to update the HCPCS procedure codes authorized for those services.
Providers may refer to the section of this bulletin titled, “Services That Require Authorization or Prior Authorization,” for information about obtaining authorization or prior authorization.
Texas Medicaid Benefit ChangesThe following Texas Medicaid benefit changes have been made to support the 2013 HCPCS and Current Procedural Terminology (CPT) updates and are effective for dates of service on or after January 1, 2013. For more information, call the Texas Medicaid & Healthcare Partnership (TMHP) Contact Center at 18009259126.
Note: These changes apply to Texas Medicaid fee-for-service and Medicaid managed care claims and authorization requests that are submitted to TMHP for processing.
The policy articles in this bulletin contain the following information:
• Revised: The description has been revised for these procedure codes. Providers may refer to the appropriate copyright holder for the revised descriptions.
• Discontinued: Discontinued procedure codes are no longer reimbursed after December 31, 2012.
• Added: Added procedure codes are new procedure codes added by the Centers for Medicare & Medicaid Services (CMS). Procedure codes noted with an asterisk (*) require a rate hearing for pricing.
• Limitations: Additional benefit and limitation information for the added procedure codes.
• Replacement: Replacement procedure codes directly replace the indicated discontinued procedure code. The discontinued procedure codes are no longer reimbursed after December 31, 2012, and the replacement procedure codes are effective for dates of service on or after January 1, 2013. Not all discontinued procedure codes have direct replacements.
Allergy Testingadded Procedure Codes95017 95018 95076Discontinued Procedure Codes95010 95015
Texas Medicaid Special Bulletin, No. 532013 HCPCS Special Bulletin
Medicaid FeeForService/Managed Care Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
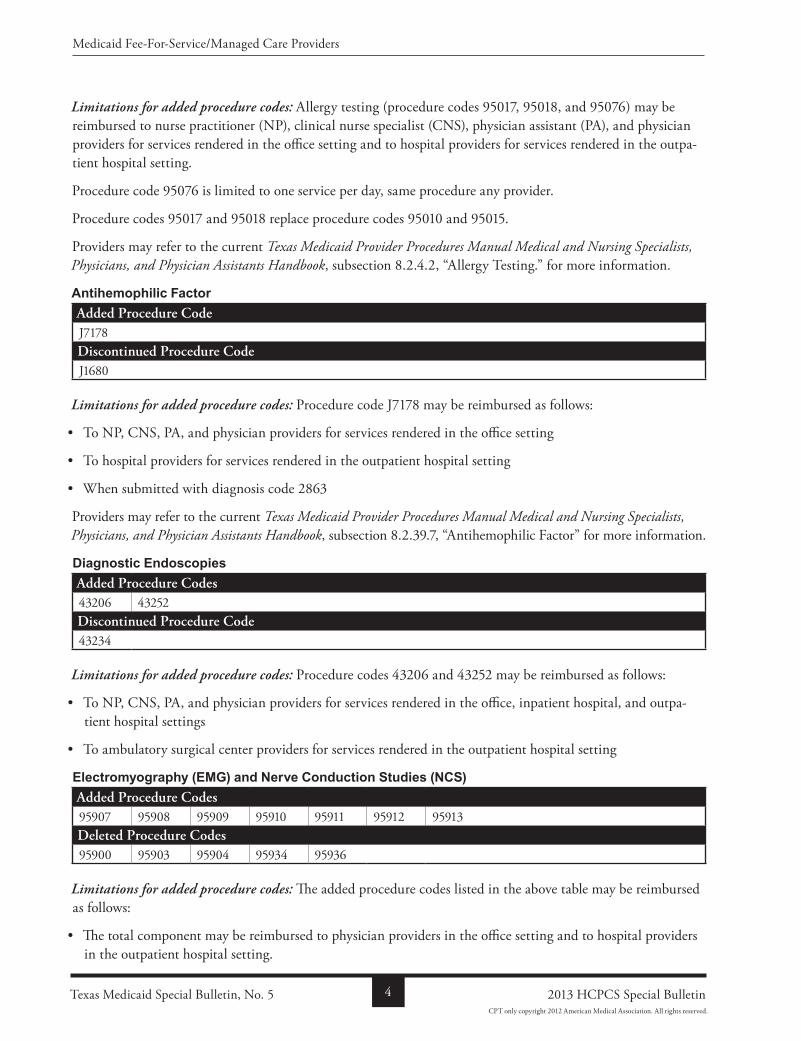
Limitations for added procedure codes: Allergy testing (procedure codes 95017, 95018, and 95076) may be reimbursed to nurse practitioner (NP), clinical nurse specialist (CNS), physician assistant (PA), and physician providers for services rendered in the office setting and to hospital providers for services rendered in the outpatient hospital setting.
Procedure code 95076 is limited to one service per day, same procedure any provider.
Procedure codes 95017 and 95018 replace procedure codes 95010 and 95015.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, subsection 8.2.4.2, “Allergy Testing.” for more information.
Antihemophilic Factoradded Procedure CodeJ7178Discontinued Procedure CodeJ1680
Limitations for added procedure codes: Procedure code J7178 may be reimbursed as follows:
• To NP, CNS, PA, and physician providers for services rendered in the office setting
• To hospital providers for services rendered in the outpatient hospital setting
• When submitted with diagnosis code 2863
Providers may refer to the current Texas Medicaid Provider Procedures Manual Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, subsection 8.2.39.7, “Antihemophilic Factor” for more information.
Diagnostic Endoscopiesadded Procedure Codes43206 43252Discontinued Procedure Code43234
Limitations for added procedure codes: Procedure codes 43206 and 43252 may be reimbursed as follows:
• To NP, CNS, PA, and physician providers for services rendered in the office, inpatient hospital, and outpatient hospital settings
• To ambulatory surgical center providers for services rendered in the outpatient hospital setting
Electromyography (EMG) and Nerve Conduction Studies (NCS)added Procedure Codes95907 95908 95909 95910 95911 95912 95913Deleted Procedure Codes95900 95903 95904 95934 95936
Limitations for added procedure codes: The added procedure codes listed in the above table may be reimbursed as follows:
• The total component may be reimbursed to physician providers in the office setting and to hospital providers in the outpatient hospital setting.
Texas Medicaid Special Bulletin, No. 5 4 2013 HCPCS Special Bulletin
Medicaid FeeForService/Managed Care Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
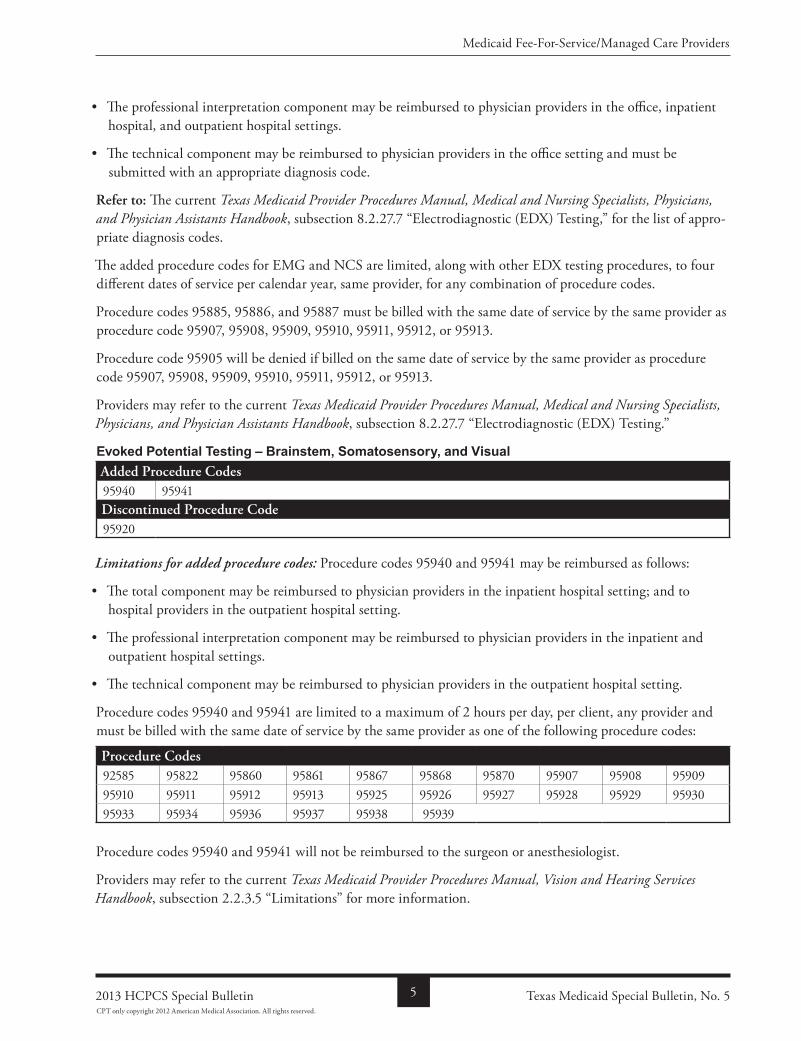
• The professional interpretation component may be reimbursed to physician providers in the office, inpatient hospital, and outpatient hospital settings.
• The technical component may be reimbursed to physician providers in the office setting and must be submitted with an appropriate diagnosis code.
refer to: The current Texas Medicaid Provider Procedures Manual, Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, subsection 8.2.27.7 “Electrodiagnostic (EDX) Testing,” for the list of appropriate diagnosis codes.
The added procedure codes for EMG and NCS are limited, along with other EDX testing procedures, to four different dates of service per calendar year, same provider, for any combination of procedure codes.
Procedure codes 95885, 95886, and 95887 must be billed with the same date of service by the same provider as procedure code 95907, 95908, 95909, 95910, 95911, 95912, or 95913.
Procedure code 95905 will be denied if billed on the same date of service by the same provider as procedure code 95907, 95908, 95909, 95910, 95911, 95912, or 95913.
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, subsection 8.2.27.7 “Electrodiagnostic (EDX) Testing.”
Evoked Potential Testing – Brainstem, Somatosensory, and Visual added Procedure Codes95940 95941Discontinued Procedure Code95920
Limitations for added procedure codes: Procedure codes 95940 and 95941 may be reimbursed as follows:
• The total component may be reimbursed to physician providers in the inpatient hospital setting; and to hospital providers in the outpatient hospital setting.
• The professional interpretation component may be reimbursed to physician providers in the inpatient and outpatient hospital settings.
• The technical component may be reimbursed to physician providers in the outpatient hospital setting.
Procedure codes 95940 and 95941 are limited to a maximum of 2 hours per day, per client, any provider and must be billed with the same date of service by the same provider as one of the following procedure codes:
Procedure Codes92585 95822 95860 95861 95867 95868 95870 95907 95908 9590995910 95911 95912 95913 95925 95926 95927 95928 95929 9593095933 95934 95936 95937 95938 95939
Procedure codes 95940 and 95941 will not be reimbursed to the surgeon or anesthesiologist.
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Vision and Hearing Services Handbook, subsection 2.2.3.5 “Limitations” for more information.
Texas Medicaid Special Bulletin, No. 552013 HCPCS Special Bulletin
Medicaid FeeForService/Managed Care Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
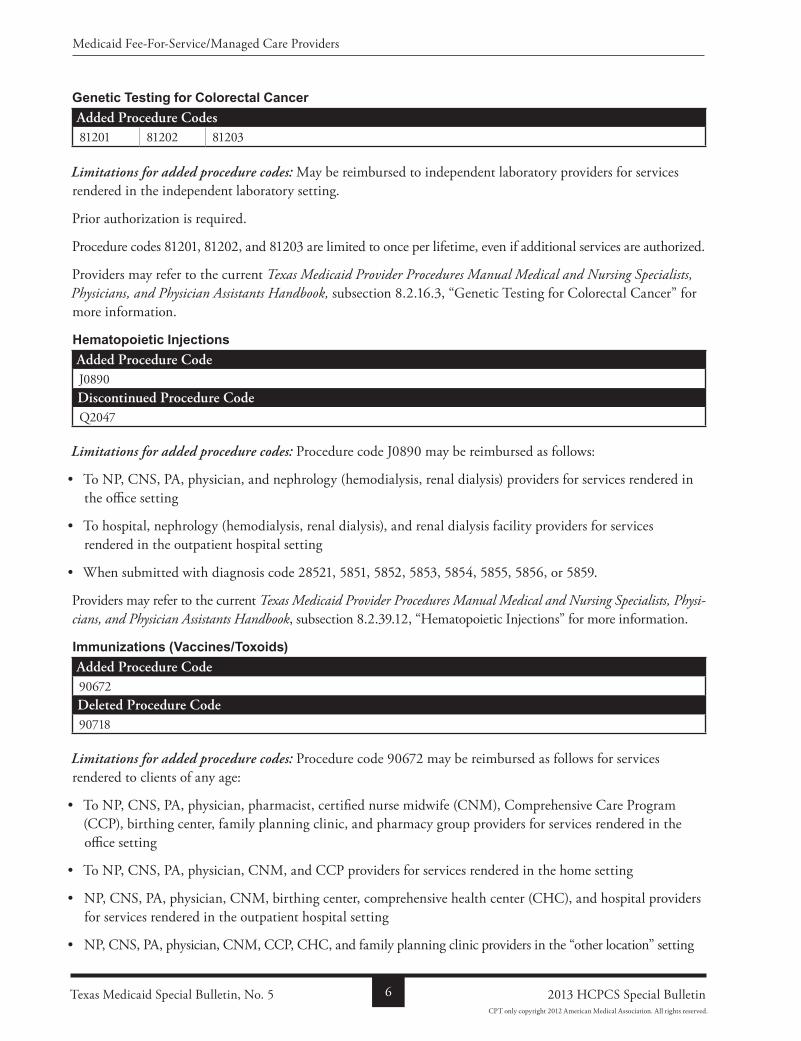
Genetic Testing for Colorectal Canceradded Procedure Codes81201 81202 81203
Limitations for added procedure codes: May be reimbursed to independent laboratory providers for services rendered in the independent laboratory setting.
Prior authorization is required.
Procedure codes 81201, 81202, and 81203 are limited to once per lifetime, even if additional services are authorized.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, subsection 8.2.16.3, “Genetic Testing for Colorectal Cancer” for more information.
Hematopoietic Injectionsadded Procedure CodeJ0890Discontinued Procedure CodeQ2047
Limitations for added procedure codes: Procedure code J0890 may be reimbursed as follows:
• To NP, CNS, PA, physician, and nephrology (hemodialysis, renal dialysis) providers for services rendered in the office setting
• To hospital, nephrology (hemodialysis, renal dialysis), and renal dialysis facility providers for services rendered in the outpatient hospital setting
• When submitted with diagnosis code 28521, 5851, 5852, 5853, 5854, 5855, 5856, or 5859.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Medical and Nursing Specialists, Physi-cians, and Physician Assistants Handbook, subsection 8.2.39.12, “Hematopoietic Injections” for more information.
Immunizations (Vaccines/Toxoids)added Procedure Code90672Deleted Procedure Code90718
Limitations for added procedure codes: Procedure code 90672 may be reimbursed as follows for services rendered to clients of any age:
• To NP, CNS, PA, physician, pharmacist, certified nurse midwife (CNM), Comprehensive Care Program (CCP), birthing center, family planning clinic, and pharmacy group providers for services rendered in the office setting
• To NP, CNS, PA, physician, CNM, and CCP providers for services rendered in the home setting
• NP, CNS, PA, physician, CNM, birthing center, comprehensive health center (CHC), and hospital providers for services rendered in the outpatient hospital setting
• NP, CNS, PA, physician, CNM, CCP, CHC, and family planning clinic providers in the “other location” setting
Texas Medicaid Special Bulletin, No. 5 6 2013 HCPCS Special Bulletin
Medicaid FeeForService/Managed Care Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
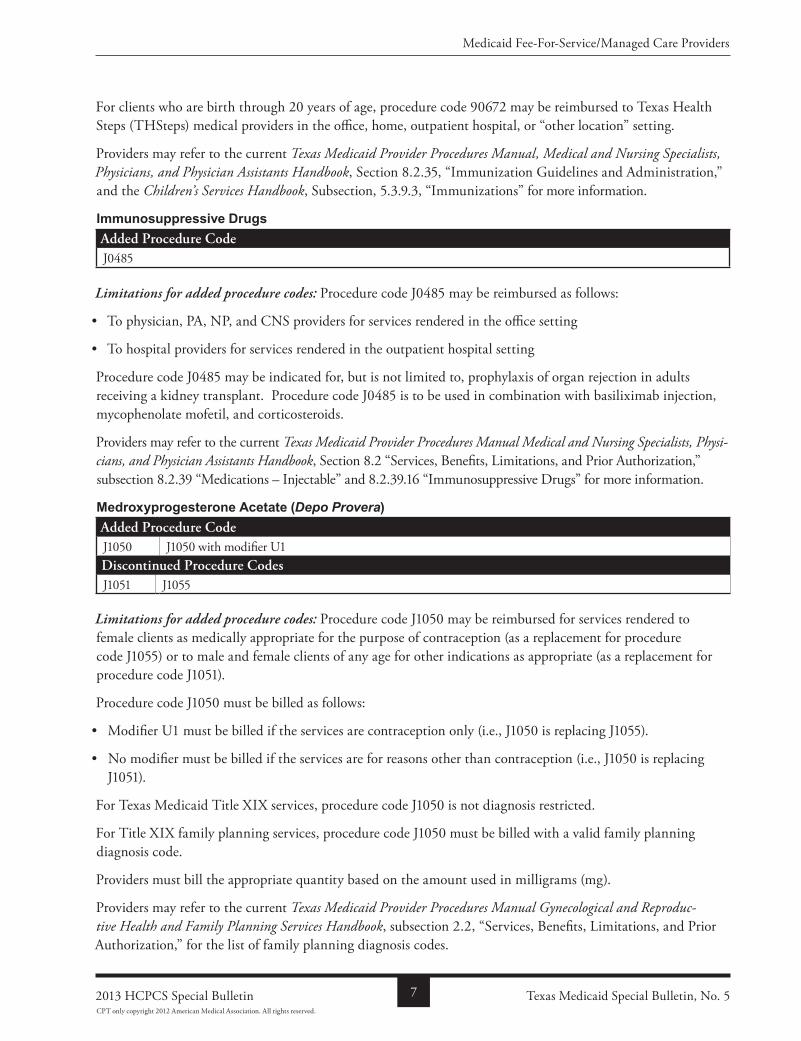
For clients who are birth through 20 years of age, procedure code 90672 may be reimbursed to Texas Health Steps (THSteps) medical providers in the office, home, outpatient hospital, or “other location” setting.
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, Section 8.2.35, “Immunization Guidelines and Administration,” and the Children’s Services Handbook, Subsection, 5.3.9.3, “Immunizations” for more information.
Immunosuppressive Drugsadded Procedure CodeJ0485
Limitations for added procedure codes: Procedure code J0485 may be reimbursed as follows:
• To physician, PA, NP, and CNS providers for services rendered in the office setting
• To hospital providers for services rendered in the outpatient hospital setting
Procedure code J0485 may be indicated for, but is not limited to, prophylaxis of organ rejection in adults receiving a kidney transplant. Procedure code J0485 is to be used in combination with basiliximab injection, mycophenolate mofetil, and corticosteroids.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Medical and Nursing Specialists, Physi-cians, and Physician Assistants Handbook, Section 8.2 “Services, Benefits, Limitations, and Prior Authorization,” subsection 8.2.39 “Medications – Injectable” and 8.2.39.16 “Immunosuppressive Drugs” for more information.
Medroxyprogesterone Acetate (Depo Provera)added Procedure CodeJ1050 J1050 with modifier U1Discontinued Procedure CodesJ1051 J1055
Limitations for added procedure codes: Procedure code J1050 may be reimbursed for services rendered to female clients as medically appropriate for the purpose of contraception (as a replacement for procedure code J1055) or to male and female clients of any age for other indications as appropriate (as a replacement for procedure code J1051).
Procedure code J1050 must be billed as follows:
• Modifier U1 must be billed if the services are contraception only (i.e., J1050 is replacing J1055).
• No modifier must be billed if the services are for reasons other than contraception (i.e., J1050 is replacing J1051).
For Texas Medicaid Title XIX services, procedure code J1050 is not diagnosis restricted.
For Title XIX family planning services, procedure code J1050 must be billed with a valid family planning diagnosis code.
Providers must bill the appropriate quantity based on the amount used in milligrams (mg).
Providers may refer to the current Texas Medicaid Provider Procedures Manual Gynecological and Reproduc-tive Health and Family Planning Services Handbook, subsection 2.2, “Services, Benefits, Limitations, and Prior Authorization,” for the list of family planning diagnosis codes.
Texas Medicaid Special Bulletin, No. 572013 HCPCS Special Bulletin
Medicaid FeeForService/Managed Care Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
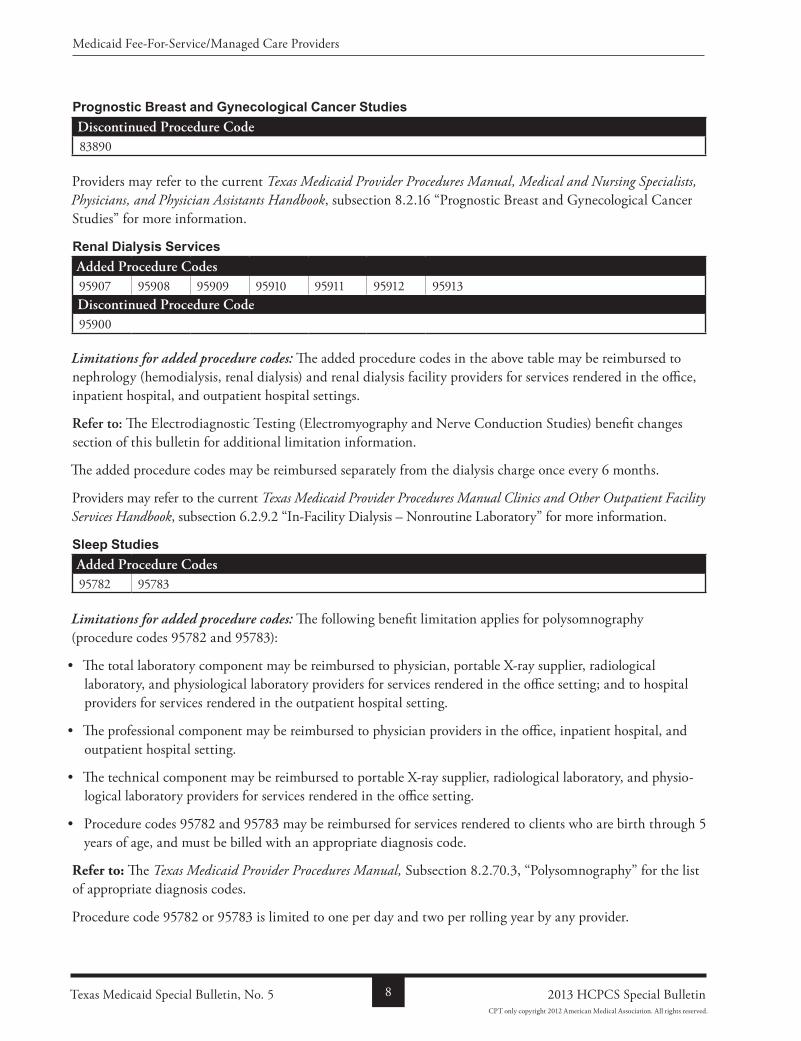
Prognostic Breast and Gynecological Cancer StudiesDiscontinued Procedure Code83890
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, subsection 8.2.16 “Prognostic Breast and Gynecological Cancer Studies” for more information.
Renal Dialysis Servicesadded Procedure Codes95907 95908 95909 95910 95911 95912 95913Discontinued Procedure Code95900
Limitations for added procedure codes: The added procedure codes in the above table may be reimbursed to nephrology (hemodialysis, renal dialysis) and renal dialysis facility providers for services rendered in the office, inpatient hospital, and outpatient hospital settings.
refer to: The Electrodiagnostic Testing (Electromyography and Nerve Conduction Studies) benefit changes section of this bulletin for additional limitation information.
The added procedure codes may be reimbursed separately from the dialysis charge once every 6 months.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Clinics and Other Outpatient Facility Services Handbook, subsection 6.2.9.2 “InFacility Dialysis – Nonroutine Laboratory” for more information.
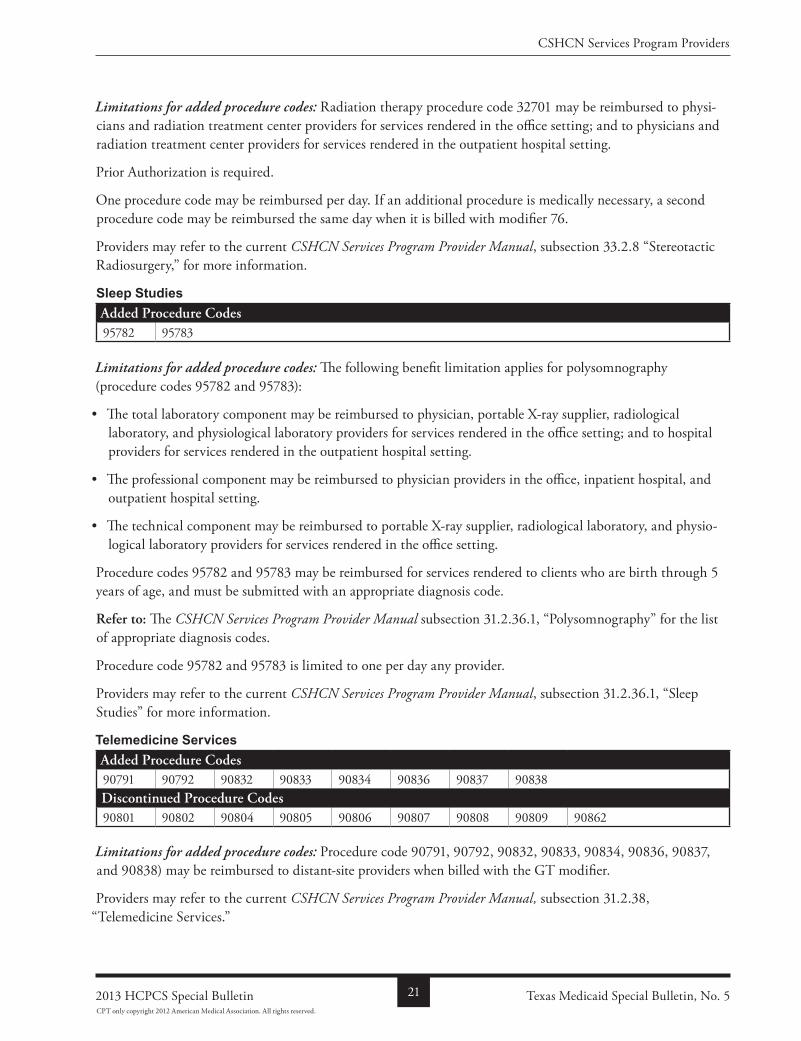
Sleep Studiesadded Procedure Codes95782 95783
Limitations for added procedure codes: The following benefit limitation applies for polysomnography (procedure codes 95782 and 95783):
• The total laboratory component may be reimbursed to physician, portable Xray supplier, radiological laboratory, and physiological laboratory providers for services rendered in the office setting; and to hospital providers for services rendered in the outpatient hospital setting.
• The professional component may be reimbursed to physician providers in the office, inpatient hospital, and outpatient hospital setting.
• The technical component may be reimbursed to portable Xray supplier, radiological laboratory, and physiological laboratory providers for services rendered in the office setting.
• Procedure codes 95782 and 95783 may be reimbursed for services rendered to clients who are birth through 5 years of age, and must be billed with an appropriate diagnosis code.
Refer to: The Texas Medicaid Provider Procedures Manual, Subsection 8.2.70.3, “Polysomnography” for the list of appropriate diagnosis codes.
Procedure code 95782 or 95783 is limited to one per day and two per rolling year by any provider.
Texas Medicaid Special Bulletin, No. 5 8 2013 HCPCS Special Bulletin
Medicaid FeeForService/Managed Care Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
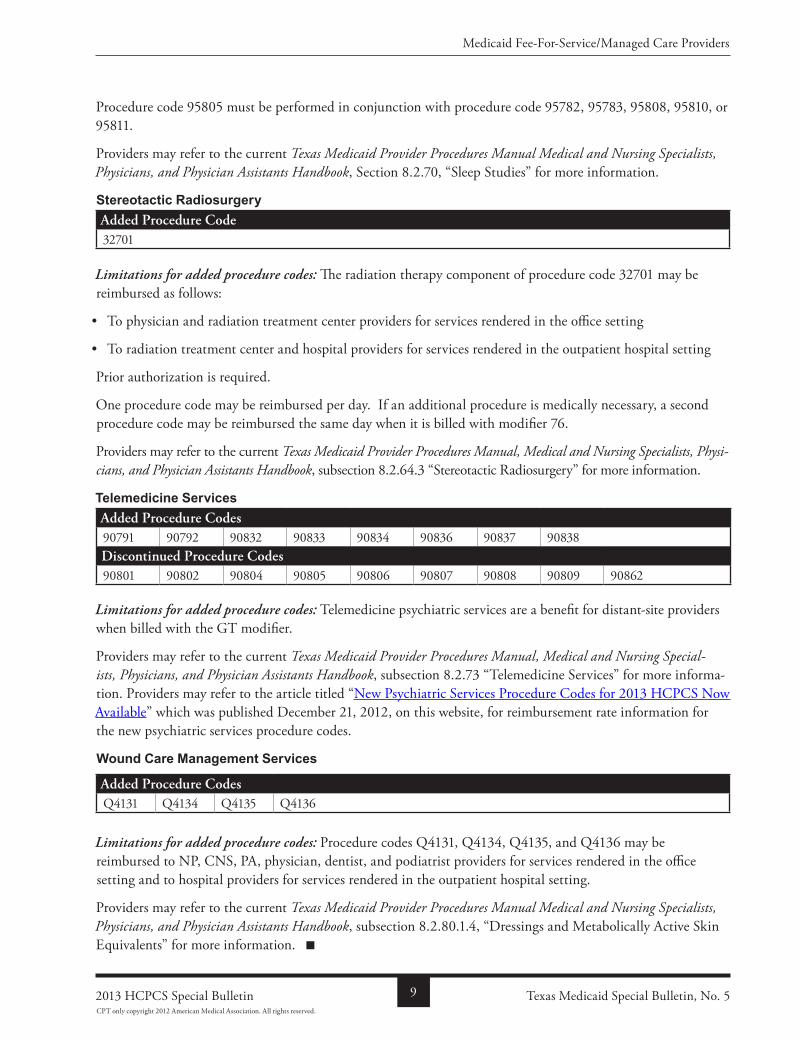
Procedure code 95805 must be performed in conjunction with procedure code 95782, 95783, 95808, 95810, or 95811.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, Section 8.2.70, “Sleep Studies” for more information.
Stereotactic Radiosurgeryadded Procedure Code32701
Limitations for added procedure codes: The radiation therapy component of procedure code 32701 may be reimbursed as follows:
• To physician and radiation treatment center providers for services rendered in the office setting
• To radiation treatment center and hospital providers for services rendered in the outpatient hospital setting
Prior authorization is required.
One procedure code may be reimbursed per day. If an additional procedure is medically necessary, a second procedure code may be reimbursed the same day when it is billed with modifier 76.
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Medical and Nursing Specialists, Physi-cians, and Physician Assistants Handbook, subsection 8.2.64.3 “Stereotactic Radiosurgery” for more information.
Telemedicine Servicesadded Procedure Codes90791 90792 90832 90833 90834 90836 90837 90838Discontinued Procedure Codes90801 90802 90804 90805 90806 90807 90808 90809 90862
Limitations for added procedure codes: Telemedicine psychiatric services are a benefit for distantsite providers when billed with the GT modifier.
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Medical and Nursing Special-ists, Physicians, and Physician Assistants Handbook, subsection 8.2.73 “Telemedicine Services” for more information. Providers may refer to the article titled “New Psychiatric Services Procedure Codes for 2013 HCPCS Now Available” which was published December 21, 2012, on this website, for reimbursement rate information for the new psychiatric services procedure codes.
Wound Care Management Services
added Procedure CodesQ4131 Q4134 Q4135 Q4136
Limitations for added procedure codes: Procedure codes Q4131, Q4134, Q4135, and Q4136 may be reimbursed to NP, CNS, PA, physician, dentist, and podiatrist providers for services rendered in the office setting and to hospital providers for services rendered in the outpatient hospital setting.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Medical and Nursing Specialists, Physicians, and Physician Assistants Handbook, subsection 8.2.80.1.4, “Dressings and Metabolically Active Skin Equivalents” for more information.
Texas Medicaid Special Bulletin, No. 592013 HCPCS Special Bulletin
Medicaid FeeForService/Managed Care Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
Behavioral health ServiceS ProviderS
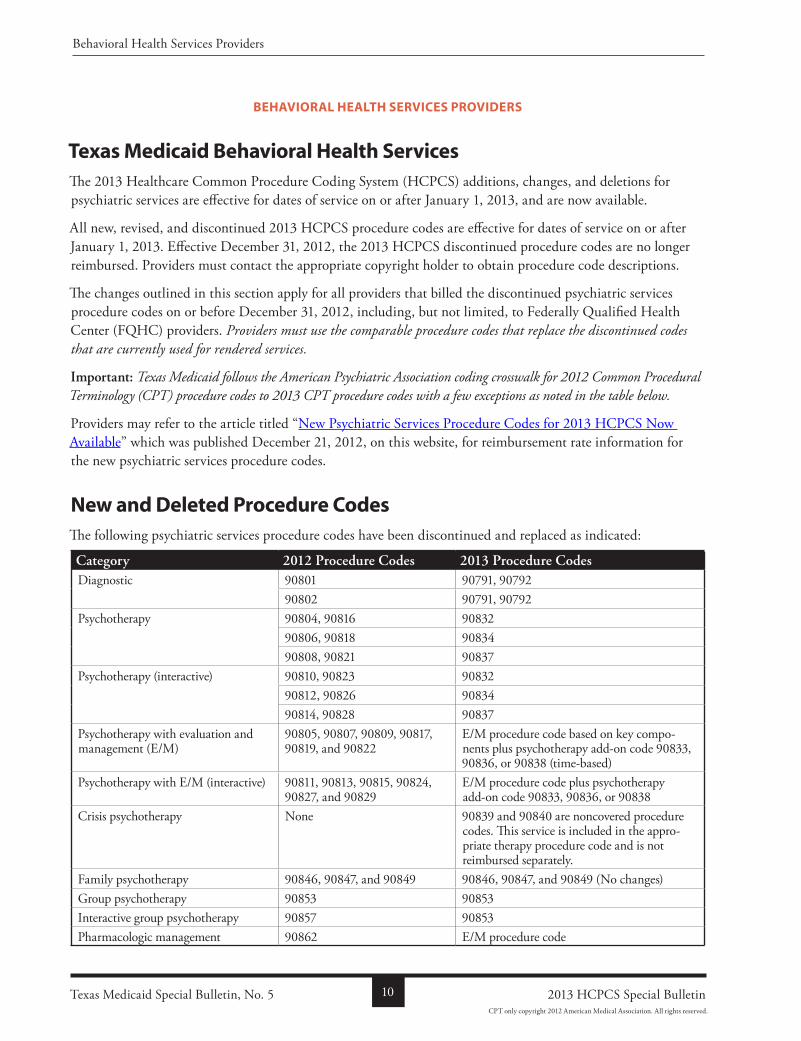
Texas Medicaid Behavioral Health ServicesThe 2013 Healthcare Common Procedure Coding System (HCPCS) additions, changes, and deletions for psychiatric services are effective for dates of service on or after January 1, 2013, and are now available.
All new, revised, and discontinued 2013 HCPCS procedure codes are effective for dates of service on or after January 1, 2013. Effective December 31, 2012, the 2013 HCPCS discontinued procedure codes are no longer reimbursed. Providers must contact the appropriate copyright holder to obtain procedure code descriptions.
The changes outlined in this section apply for all providers that billed the discontinued psychiatric services procedure codes on or before December 31, 2012, including, but not limited, to Federally Qualified Health Center (FQHC) providers. Providers must use the comparable procedure codes that replace the discontinued codes that are currently used for rendered services.
Important: Texas Medicaid follows the American Psychiatric Association coding crosswalk for 2012 Common Procedural Terminology (CPT) procedure codes to 2013 CPT procedure codes with a few exceptions as noted in the table below.
Providers may refer to the article titled “New Psychiatric Services Procedure Codes for 2013 HCPCS Now Available” which was published December 21, 2012, on this website, for reimbursement rate information for the new psychiatric services procedure codes.
New and Deleted Procedure CodesThe following psychiatric services procedure codes have been discontinued and replaced as indicated:
Category 2012 Procedure Codes 2013 Procedure CodesDiagnostic 90801 90791, 90792
90802 90791, 90792Psychotherapy 90804, 90816 90832
90806, 90818 9083490808, 90821 90837
Psychotherapy (interactive) 90810, 90823 9083290812, 90826 9083490814, 90828 90837
Psychotherapy with evaluation and management (E/M)
90805, 90807, 90809, 90817, 90819, and 90822
E/M procedure code based on key components plus psychotherapy addon code 90833, 90836, or 90838 (timebased)
Psychotherapy with E/M (interactive) 90811, 90813, 90815, 90824, 90827, and 90829
E/M procedure code plus psychotherapy addon code 90833, 90836, or 90838
Crisis psychotherapy None 90839 and 90840 are noncovered procedure codes. This service is included in the appropriate therapy procedure code and is not reimbursed separately.
Family psychotherapy 90846, 90847, and 90849 90846, 90847, and 90849 (No changes)Group psychotherapy 90853 90853Interactive group psychotherapy 90857 90853Pharmacologic management 90862 E/M procedure code
Texas Medicaid Special Bulletin, No. 5 10 2013 HCPCS Special Bulletin
Behavioral Health Services Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
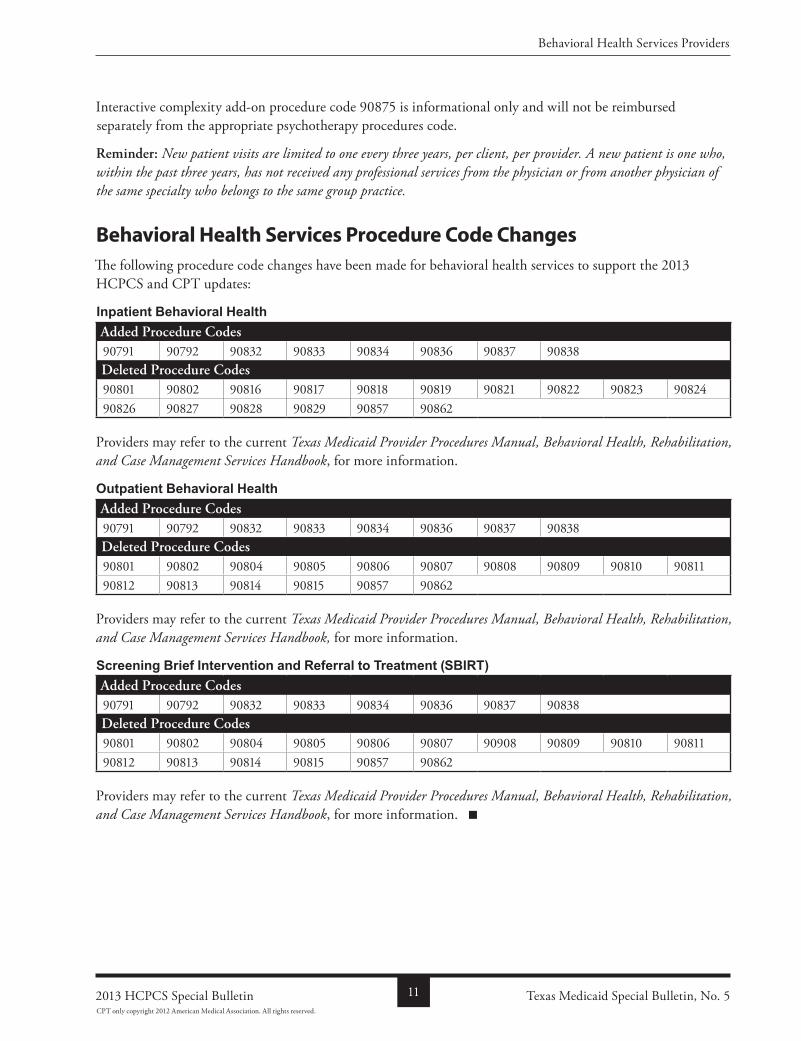
Interactive complexity addon procedure code 90875 is informational only and will not be reimbursed separately from the appropriate psychotherapy procedures code.
reminder: New patient visits are limited to one every three years, per client, per provider. A new patient is one who, within the past three years, has not received any professional services from the physician or from another physician of the same specialty who belongs to the same group practice.
Behavioral Health Services Procedure Code ChangesThe following procedure code changes have been made for behavioral health services to support the 2013 HCPCS and CPT updates:
Inpatient Behavioral Healthadded Procedure Codes90791 90792 90832 90833 90834 90836 90837 90838Deleted Procedure Codes90801 90802 90816 90817 90818 90819 90821 90822 90823 9082490826 90827 90828 90829 90857 90862
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Behavioral Health, Rehabilitation, and Case Management Services Handbook, for more information.
Outpatient Behavioral Healthadded Procedure Codes90791 90792 90832 90833 90834 90836 90837 90838Deleted Procedure Codes90801 90802 90804 90805 90806 90807 90808 90809 90810 9081190812 90813 90814 90815 90857 90862
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Behavioral Health, Rehabilitation, and Case Management Services Handbook, for more information.
Screening Brief Intervention and Referral to Treatment (SBIRT)added Procedure Codes90791 90792 90832 90833 90834 90836 90837 90838Deleted Procedure Codes90801 90802 90804 90805 90806 90807 90908 90809 90810 9081190812 90813 90814 90815 90857 90862
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Behavioral Health, Rehabilitation, and Case Management Services Handbook, for more information.
Texas Medicaid Special Bulletin, No. 5112013 HCPCS Special Bulletin
Behavioral Health Services Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
dShS FaMily Planning ProviderS
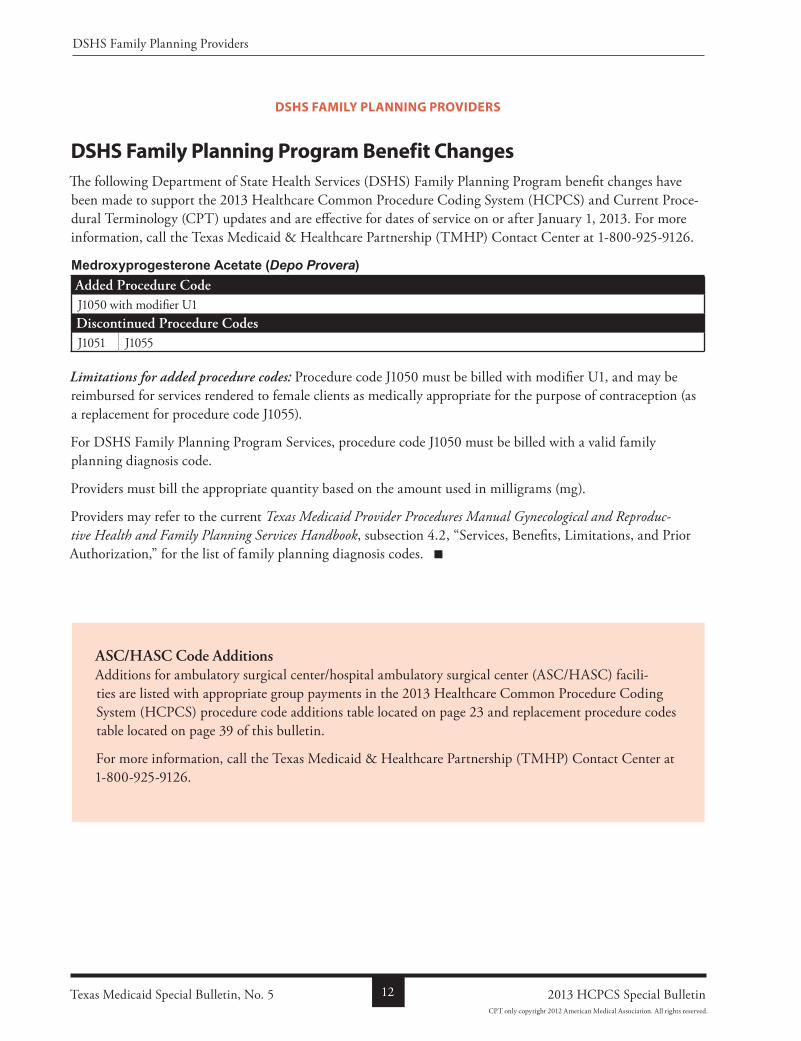
DSHS Family Planning Program Benefit ChangesThe following Department of State Health Services (DSHS) Family Planning Program benefit changes have been made to support the 2013 Healthcare Common Procedure Coding System (HCPCS) and Current Procedural Terminology (CPT) updates and are effective for dates of service on or after January 1, 2013. For more information, call the Texas Medicaid & Healthcare Partnership (TMHP) Contact Center at 18009259126.
Medroxyprogesterone Acetate (Depo Provera)added Procedure CodeJ1050 with modifier U1Discontinued Procedure CodesJ1051 J1055
Limitations for added procedure codes: Procedure code J1050 must be billed with modifier U1, and may be reimbursed for services rendered to female clients as medically appropriate for the purpose of contraception (as a replacement for procedure code J1055).
For DSHS Family Planning Program Services, procedure code J1050 must be billed with a valid family planning diagnosis code.
Providers must bill the appropriate quantity based on the amount used in milligrams (mg).
Providers may refer to the current Texas Medicaid Provider Procedures Manual Gynecological and Reproduc-tive Health and Family Planning Services Handbook, subsection 4.2, “Services, Benefits, Limitations, and Prior Authorization,” for the list of family planning diagnosis codes.
aSC/HaSC Code additionsAdditions for ambulatory surgical center/hospital ambulatory surgical center (ASC/HASC) facilities are listed with appropriate group payments in the 2013 Healthcare Common Procedure Coding System (HCPCS) procedure code additions table located on page 23 and replacement procedure codes table located on page 39 of this bulletin.
For more information, call the Texas Medicaid & Healthcare Partnership (TMHP) Contact Center at 18009259126.
Texas Medicaid Special Bulletin, No. 5 12 2013 HCPCS Special Bulletin
DSHS Family Planning Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
hoMe health and coMPrehenSive care PrograM ProviderS
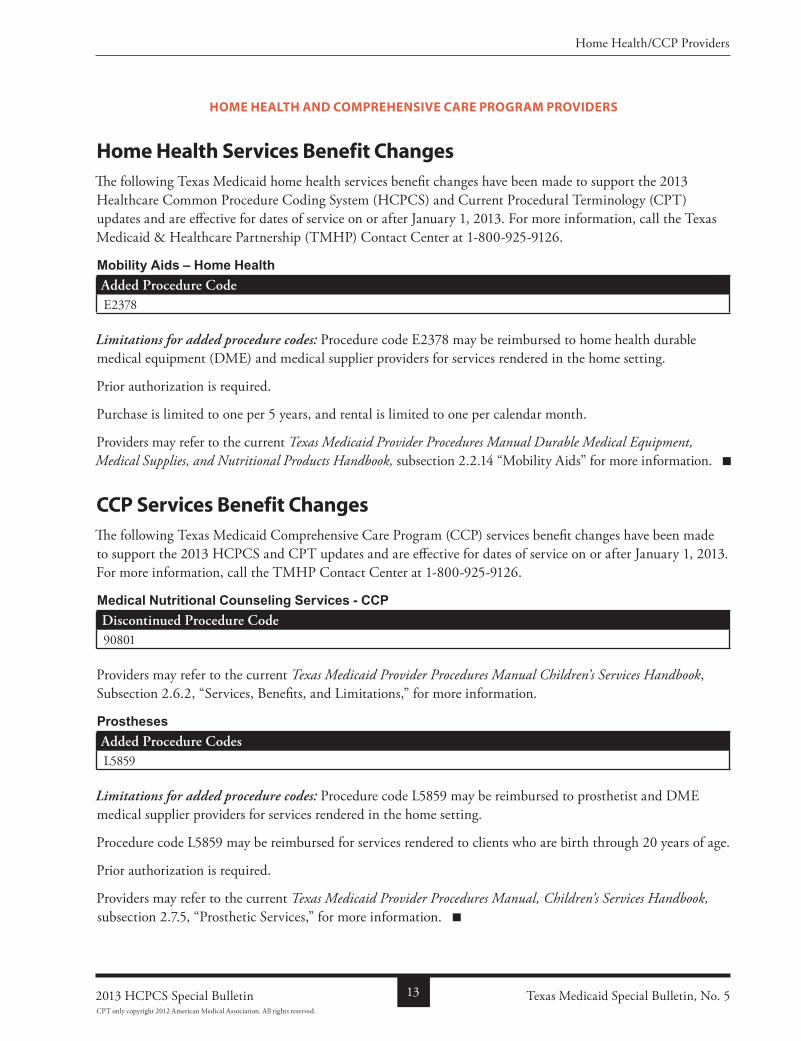
Home Health Services Benefit ChangesThe following Texas Medicaid home health services benefit changes have been made to support the 2013 Healthcare Common Procedure Coding System (HCPCS) and Current Procedural Terminology (CPT) updates and are effective for dates of service on or after January 1, 2013. For more information, call the Texas Medicaid & Healthcare Partnership (TMHP) Contact Center at 18009259126.
Mobility Aids – Home Healthadded Procedure CodeE2378
Limitations for added procedure codes: Procedure code E2378 may be reimbursed to home health durable medical equipment (DME) and medical supplier providers for services rendered in the home setting.
Prior authorization is required.
Purchase is limited to one per 5 years, and rental is limited to one per calendar month.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Durable Medical Equipment, Medical Supplies, and Nutritional Products Handbook, subsection 2.2.14 “Mobility Aids” for more information.
CCP Services Benefit ChangesThe following Texas Medicaid Comprehensive Care Program (CCP) services benefit changes have been made to support the 2013 HCPCS and CPT updates and are effective for dates of service on or after January 1, 2013. For more information, call the TMHP Contact Center at 18009259126.
Medical Nutritional Counseling Services - CCPDiscontinued Procedure Code90801
Providers may refer to the current Texas Medicaid Provider Procedures Manual Children’s Services Handbook, Subsection 2.6.2, “Services, Benefits, and Limitations,” for more information.
Prosthesesadded Procedure CodesL5859
Limitations for added procedure codes: Procedure code L5859 may be reimbursed to prosthetist and DME medical supplier providers for services rendered in the home setting.
Procedure code L5859 may be reimbursed for services rendered to clients who are birth through 20 years of age.
Prior authorization is required.
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Children’s Services Handbook, subsection 2.7.5, “Prosthetic Services,” for more information.
Texas Medicaid Special Bulletin, No. 5132013 HCPCS Special Bulletin
Home Health/CCP Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
texaS health StePS dental ProviderS
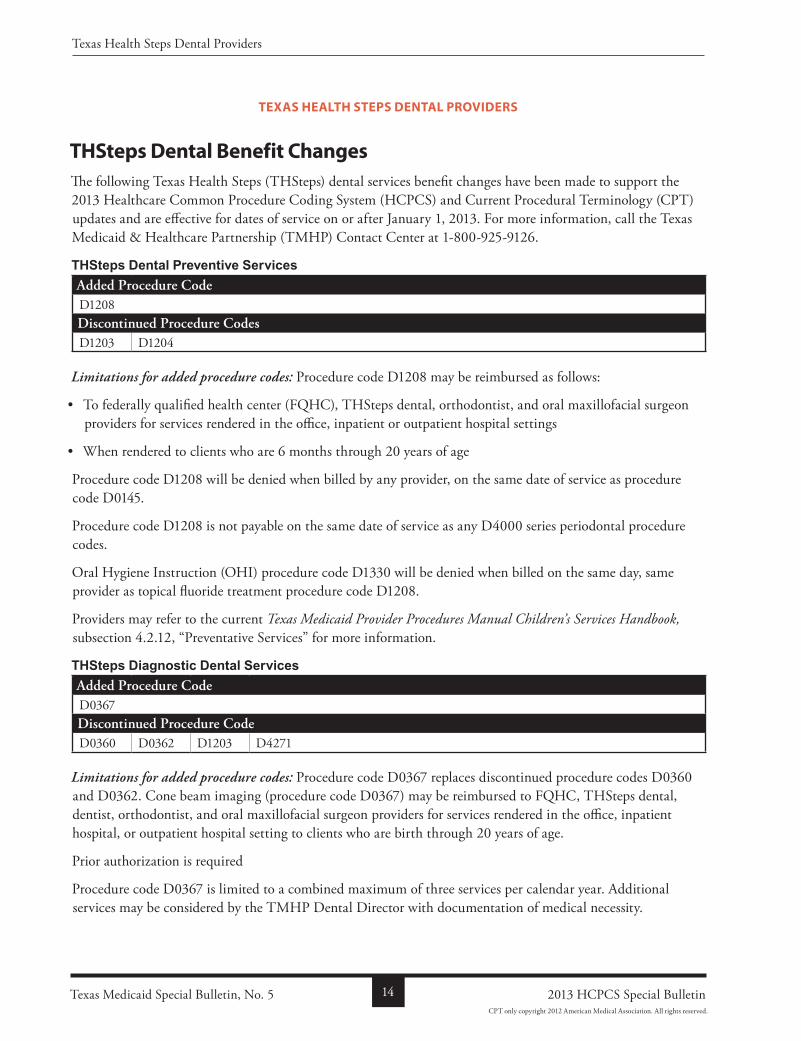
THSteps Dental Benefit ChangesThe following Texas Health Steps (THSteps) dental services benefit changes have been made to support the 2013 Healthcare Common Procedure Coding System (HCPCS) and Current Procedural Terminology (CPT) updates and are effective for dates of service on or after January 1, 2013. For more information, call the Texas Medicaid & Healthcare Partnership (TMHP) Contact Center at 18009259126.
THSteps Dental Preventive Servicesadded Procedure CodeD1208Discontinued Procedure CodesD1203 D1204
Limitations for added procedure codes: Procedure code D1208 may be reimbursed as follows:
• To federally qualified health center (FQHC), THSteps dental, orthodontist, and oral maxillofacial surgeon providers for services rendered in the office, inpatient or outpatient hospital settings
• When rendered to clients who are 6 months through 20 years of age
Procedure code D1208 will be denied when billed by any provider, on the same date of service as procedure code D0145.
Procedure code D1208 is not payable on the same date of service as any D4000 series periodontal procedure codes.
Oral Hygiene Instruction (OHI) procedure code D1330 will be denied when billed on the same day, same provider as topical fluoride treatment procedure code D1208.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Children’s Services Handbook, subsection 4.2.12, “Preventative Services” for more information.
THSteps Diagnostic Dental Servicesadded Procedure CodeD0367Discontinued Procedure CodeD0360 D0362 D1203 D4271
Limitations for added procedure codes: Procedure code D0367 replaces discontinued procedure codes D0360 and D0362. Cone beam imaging (procedure code D0367) may be reimbursed to FQHC, THSteps dental, dentist, orthodontist, and oral maxillofacial surgeon providers for services rendered in the office, inpatient hospital, or outpatient hospital setting to clients who are birth through 20 years of age.
Prior authorization is required
Procedure code D0367 is limited to a combined maximum of three services per calendar year. Additional services may be considered by the TMHP Dental Director with documentation of medical necessity.
Texas Medicaid Special Bulletin, No. 5 14 2013 HCPCS Special Bulletin
Texas Health Steps Dental Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
Providers may refer to the current Texas Medicaid Provider Procedures Manual Children’s Services Handbook, subsection 4.2.29.1, “Cone Beam Imaging” for more information.
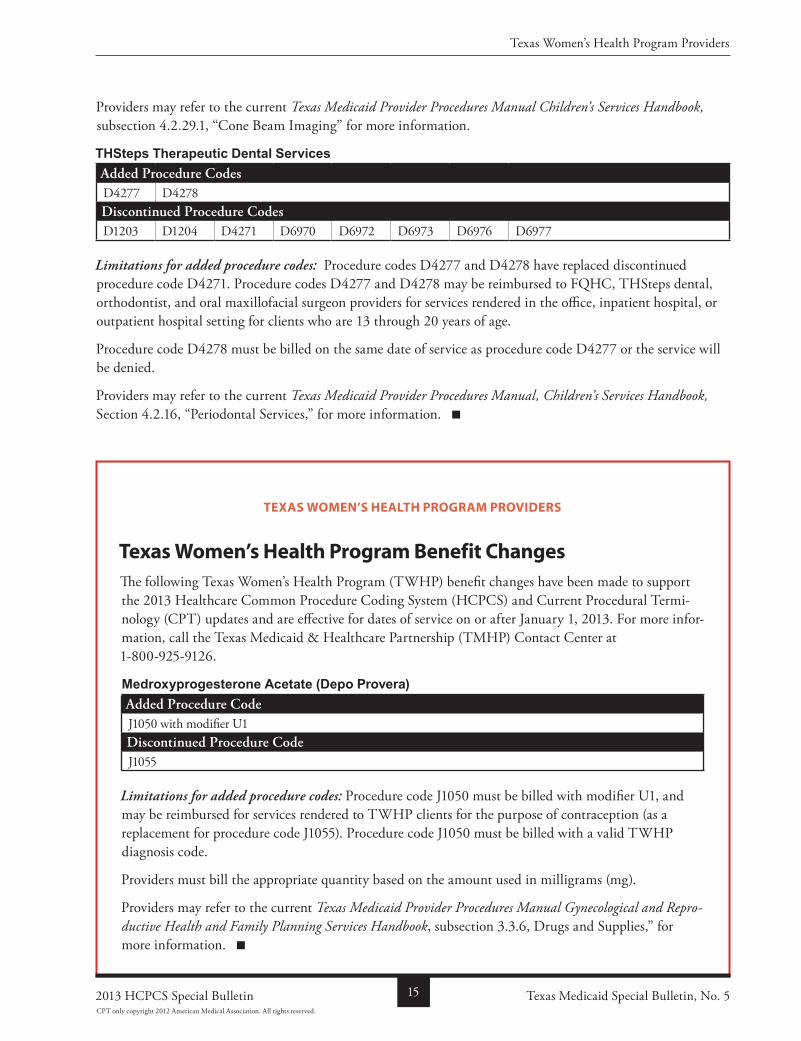
THSteps Therapeutic Dental Servicesadded Procedure CodesD4277 D4278Discontinued Procedure CodesD1203 D1204 D4271 D6970 D6972 D6973 D6976 D6977
Limitations for added procedure codes: Procedure codes D4277 and D4278 have replaced discontinued procedure code D4271. Procedure codes D4277 and D4278 may be reimbursed to FQHC, THSteps dental, orthodontist, and oral maxillofacial surgeon providers for services rendered in the office, inpatient hospital, or outpatient hospital setting for clients who are 13 through 20 years of age.
Procedure code D4278 must be billed on the same date of service as procedure code D4277 or the service will be denied.
Providers may refer to the current Texas Medicaid Provider Procedures Manual, Children’s Services Handbook, Section 4.2.16, “Periodontal Services,” for more information.
texaS WoMen’S health PrograM ProviderS
Texas Women’s Health Program Benefit ChangesThe following Texas Women’s Health Program (TWHP) benefit changes have been made to support the 2013 Healthcare Common Procedure Coding System (HCPCS) and Current Procedural Terminology (CPT) updates and are effective for dates of service on or after January 1, 2013. For more information, call the Texas Medicaid & Healthcare Partnership (TMHP) Contact Center at 18009259126.
Medroxyprogesterone Acetate (Depo Provera)added Procedure CodeJ1050 with modifier U1Discontinued Procedure CodeJ1055
Limitations for added procedure codes: Procedure code J1050 must be billed with modifier U1, and may be reimbursed for services rendered to TWHP clients for the purpose of contraception (as a replacement for procedure code J1055). Procedure code J1050 must be billed with a valid TWHP diagnosis code.
Providers must bill the appropriate quantity based on the amount used in milligrams (mg).
Providers may refer to the current Texas Medicaid Provider Procedures Manual Gynecological and Repro-ductive Health and Family Planning Services Handbook, subsection 3.3.6, Drugs and Supplies,” for more information.
Texas Medicaid Special Bulletin, No. 5152013 HCPCS Special Bulletin
Texas Women’s Health Program Providers
CPT only copyright 2012 American Medical Association. All rights reserved.

children With SPecial health care needS (cShcn) ServiceS PrograM ProviderS
CSHCN Services Program UpdatesThe 2013 Healthcare Common Procedure Coding System (HCPCS) updates including authorization and prior authorization updates for the CSHCN Services Program are included in the HCPCS tables in the “All Code Changes” section of this bulletin beginning on page 23. The 2013 HCPCS deletions and replacements are effective January 1, 2013, for dates of service on or after January 1, 2013, for the CSHCN Services Program. Providers may refer to the “General Information” section for more information.
authorization and Prior authorization update reminderEffective January 1, 2013, the 2013 HCPCS deleted procedure codes are no longer reimbursed by the CSHCN Services Program. Unless otherwise indicated on page 23 of this bulletin, providers who have received authorizations or prior authorizations for dates of service that occur on, after, or encompass January 1, 2013, must submit a written request on the appropriate, completed CSHCN Services Program authorization or prior authorization request form in order to update the HCPCS procedure codes authorized for those services.
Providers may refer to the section of this bulletin titled, “Services That Require Authorization or Prior Authorization,” for information about obtaining authorization or prior authorization.
For more information, call the Texas Medicaid & Healthcare Partnership (TMHP)CSHCN Services Program Contact Center 18005682413.
CSHCN Services Program Benefit ChangesThe following CSHCN Services Program benefit changes have been made to support the 2013 HCPCS and Current Procedural Terminology (CPT) updates and are effective for dates of service on or after January 1, 2013. For more information, call the TMHPCSHCN Services Program Contact Center at 18009259126.
The policy articles below contain the following information:
• Revised: The description has been revised for these procedure codes. Providers may refer to the appropriate copyright holder for the revised descriptions.
• Discontinued: Discontinued procedure codes are no longer reimbursed after December 31, 2012.
• Added: Added procedure codes are new procedure codes added by the Centers for Medicare & Medicaid Services (CMS). Procedure codes noted with an asterisk (*) require a rate hearing for pricing.
• Limitations: Additional benefit and limitation information for the added procedure codes.
• Replacement: Replacement procedure codes directly replace the indicated discontinued procedure code. The discontinued procedure codes are no longer reimbursed after December 31, 2012, and the replacement procedure codes are effective for dates of service on or after January 1, 2013. Not all discontinued procedure codes have direct replacements.
Note: For the purposes of this section for CSHCN Services Program benefit changes, “advanced practice registered nurse (APRN)” includes nurse practitioner (NP) and clinical nurse specialist (CNS) providers only.
Texas Medicaid Special Bulletin, No. 5 16 2013 HCPCS Special Bulletin
CSHCN Services Program Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
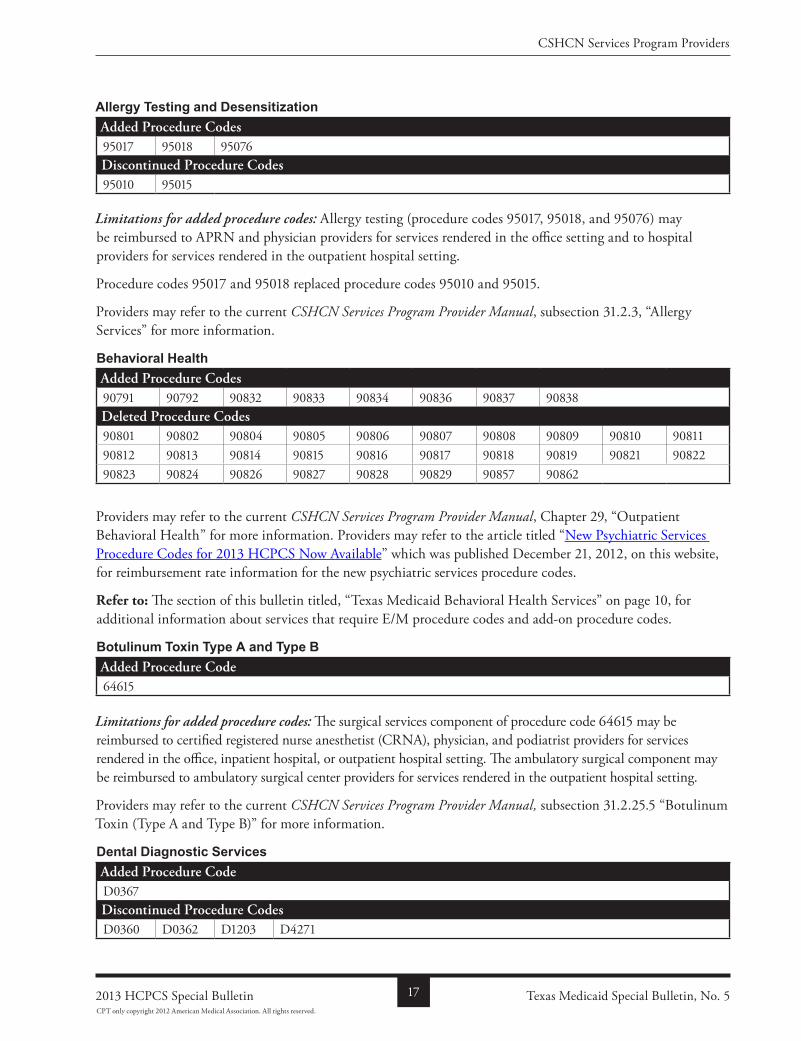
Allergy Testing and Desensitizationadded Procedure Codes95017 95018 95076Discontinued Procedure Codes95010 95015
Limitations for added procedure codes: Allergy testing (procedure codes 95017, 95018, and 95076) may be reimbursed to APRN and physician providers for services rendered in the office setting and to hospital providers for services rendered in the outpatient hospital setting.
Procedure codes 95017 and 95018 replaced procedure codes 95010 and 95015.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 31.2.3, “Allergy Services” for more information.
Behavioral Healthadded Procedure Codes90791 90792 90832 90833 90834 90836 90837 90838Deleted Procedure Codes90801 90802 90804 90805 90806 90807 90808 90809 90810 9081190812 90813 90814 90815 90816 90817 90818 90819 90821 9082290823 90824 90826 90827 90828 90829 90857 90862
Providers may refer to the current CSHCN Services Program Provider Manual, Chapter 29, “Outpatient Behavioral Health” for more information. Providers may refer to the article titled “New Psychiatric Services Procedure Codes for 2013 HCPCS Now Available” which was published December 21, 2012, on this website, for reimbursement rate information for the new psychiatric services procedure codes.
Refer to: The section of this bulletin titled, “Texas Medicaid Behavioral Health Services” on page 10, for additional information about services that require E/M procedure codes and addon procedure codes.
Botulinum Toxin Type A and Type Badded Procedure Code64615
Limitations for added procedure codes: The surgical services component of procedure code 64615 may be reimbursed to certified registered nurse anesthetist (CRNA), physician, and podiatrist providers for services rendered in the office, inpatient hospital, or outpatient hospital setting. The ambulatory surgical component may be reimbursed to ambulatory surgical center providers for services rendered in the outpatient hospital setting.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 31.2.25.5 “Botulinum Toxin (Type A and Type B)” for more information.
Dental Diagnostic Servicesadded Procedure CodeD0367Discontinued Procedure CodesD0360 D0362 D1203 D4271
Texas Medicaid Special Bulletin, No. 5172013 HCPCS Special Bulletin
CSHCN Services Program Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
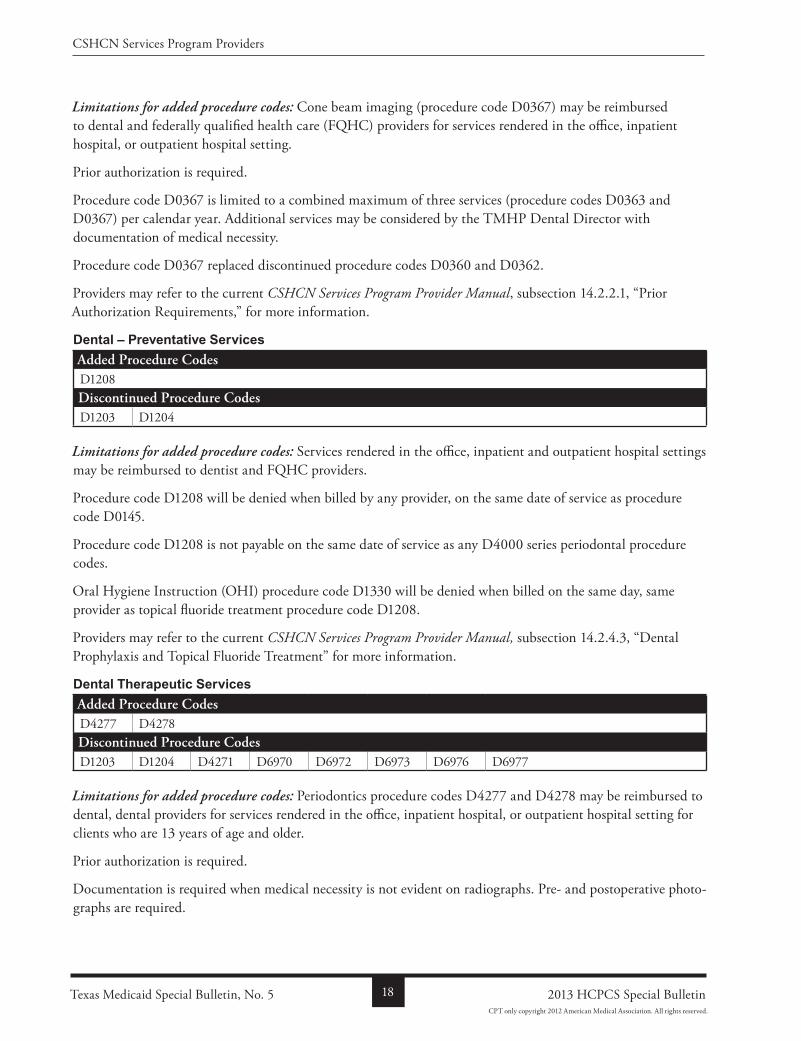
Limitations for added procedure codes: Cone beam imaging (procedure code D0367) may be reimbursed to dental and federally qualified health care (FQHC) providers for services rendered in the office, inpatient hospital, or outpatient hospital setting.
Prior authorization is required.
Procedure code D0367 is limited to a combined maximum of three services (procedure codes D0363 and D0367) per calendar year. Additional services may be considered by the TMHP Dental Director with documentation of medical necessity.
Procedure code D0367 replaced discontinued procedure codes D0360 and D0362.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 14.2.2.1, “Prior Authorization Requirements,” for more information.
Dental – Preventative Servicesadded Procedure CodesD1208Discontinued Procedure CodesD1203 D1204
Limitations for added procedure codes: Services rendered in the office, inpatient and outpatient hospital settings may be reimbursed to dentist and FQHC providers.
Procedure code D1208 will be denied when billed by any provider, on the same date of service as procedure code D0145.
Procedure code D1208 is not payable on the same date of service as any D4000 series periodontal procedure codes.
Oral Hygiene Instruction (OHI) procedure code D1330 will be denied when billed on the same day, same provider as topical fluoride treatment procedure code D1208.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 14.2.4.3, “Dental Prophylaxis and Topical Fluoride Treatment” for more information.
Dental Therapeutic Servicesadded Procedure CodesD4277 D4278Discontinued Procedure CodesD1203 D1204 D4271 D6970 D6972 D6973 D6976 D6977
Limitations for added procedure codes: Periodontics procedure codes D4277 and D4278 may be reimbursed to dental, dental providers for services rendered in the office, inpatient hospital, or outpatient hospital setting for clients who are 13 years of age and older.
Prior authorization is required.
Documentation is required when medical necessity is not evident on radiographs. Pre and postoperative photographs are required.
Texas Medicaid Special Bulletin, No. 5 18 2013 HCPCS Special Bulletin
CSHCN Services Program Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
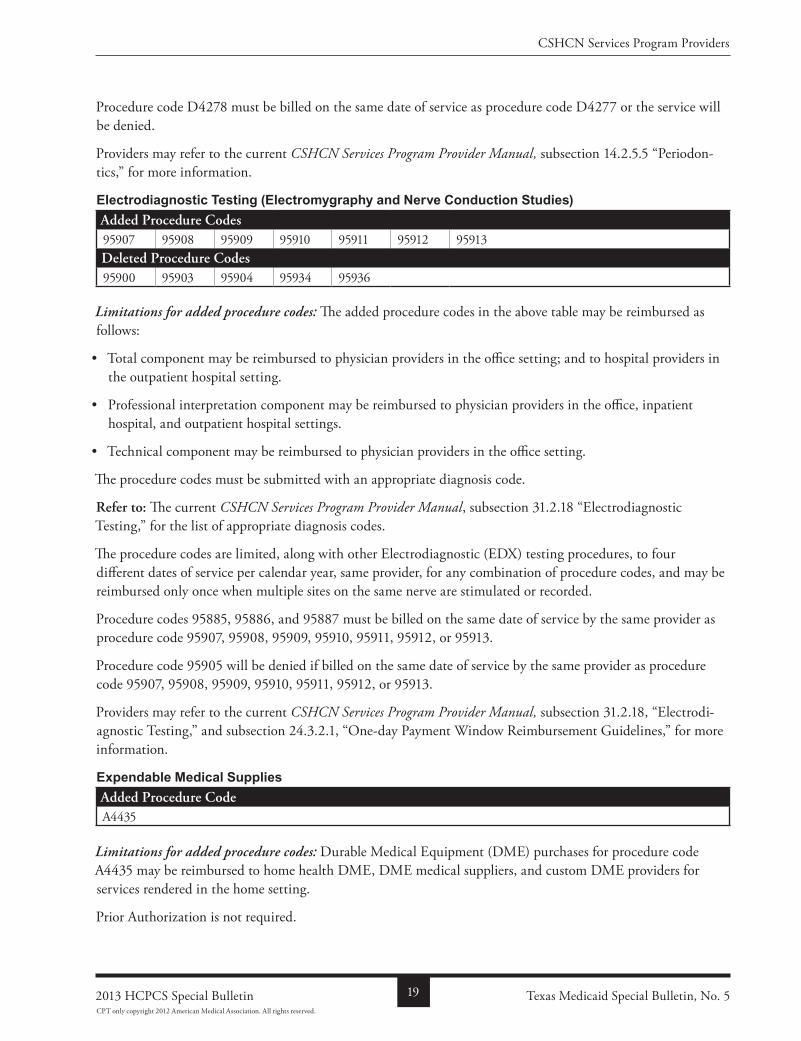
Procedure code D4278 must be billed on the same date of service as procedure code D4277 or the service will be denied.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 14.2.5.5 “Periodontics,” for more information.
Electrodiagnostic Testing (Electromygraphy and Nerve Conduction Studies)added Procedure Codes95907 95908 95909 95910 95911 95912 95913Deleted Procedure Codes95900 95903 95904 95934 95936
Limitations for added procedure codes: The added procedure codes in the above table may be reimbursed as follows:
• Total component may be reimbursed to physician providers in the office setting; and to hospital providers in the outpatient hospital setting.
• Professional interpretation component may be reimbursed to physician providers in the office, inpatient hospital, and outpatient hospital settings.
• Technical component may be reimbursed to physician providers in the office setting.
The procedure codes must be submitted with an appropriate diagnosis code.
refer to: The current CSHCN Services Program Provider Manual, subsection 31.2.18 “Electrodiagnostic Testing,” for the list of appropriate diagnosis codes.
The procedure codes are limited, along with other Electrodiagnostic (EDX) testing procedures, to four different dates of service per calendar year, same provider, for any combination of procedure codes, and may be reimbursed only once when multiple sites on the same nerve are stimulated or recorded.
Procedure codes 95885, 95886, and 95887 must be billed on the same date of service by the same provider as procedure code 95907, 95908, 95909, 95910, 95911, 95912, or 95913.
Procedure code 95905 will be denied if billed on the same date of service by the same provider as procedure code 95907, 95908, 95909, 95910, 95911, 95912, or 95913.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 31.2.18, “Electrodiagnostic Testing,” and subsection 24.3.2.1, “Oneday Payment Window Reimbursement Guidelines,” for more information.
Expendable Medical Suppliesadded Procedure CodeA4435
Limitations for added procedure codes: Durable Medical Equipment (DME) purchases for procedure code A4435 may be reimbursed to home health DME, DME medical suppliers, and custom DME providers for services rendered in the home setting.
Prior Authorization is not required.
Texas Medicaid Special Bulletin, No. 5192013 HCPCS Special Bulletin
CSHCN Services Program Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
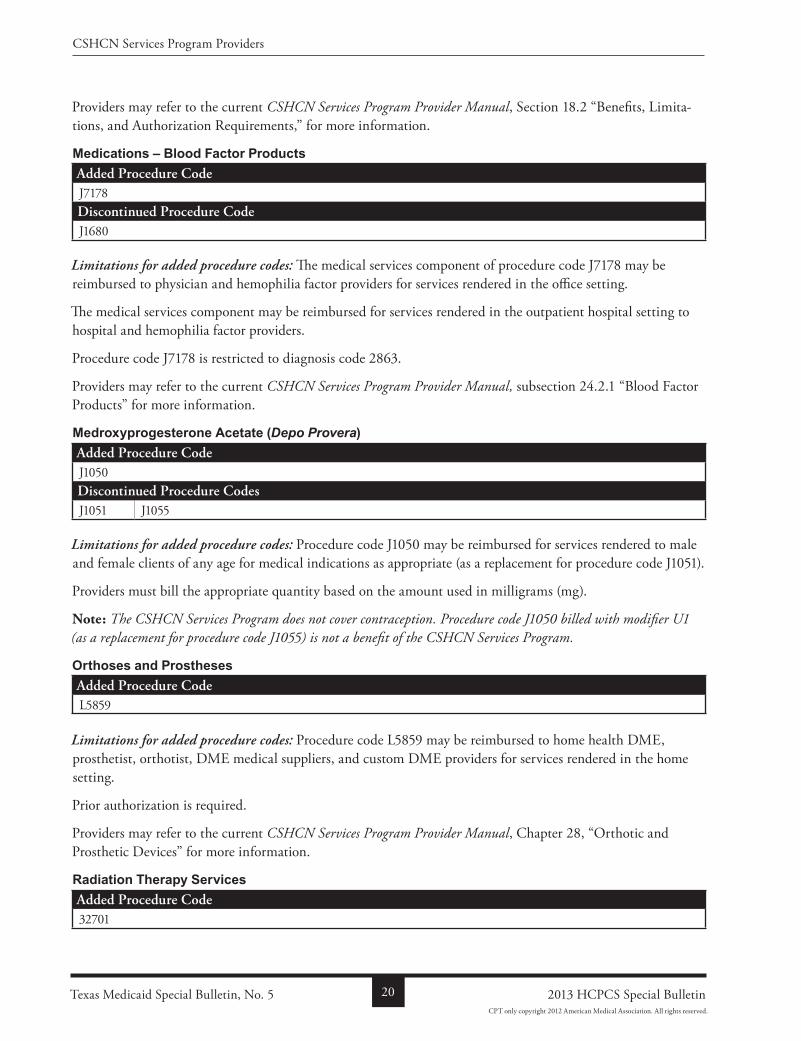
Providers may refer to the current CSHCN Services Program Provider Manual, Section 18.2 “Benefits, Limitations, and Authorization Requirements,” for more information.
Medications – Blood Factor Productsadded Procedure CodeJ7178Discontinued Procedure CodeJ1680
Limitations for added procedure codes: The medical services component of procedure code J7178 may be reimbursed to physician and hemophilia factor providers for services rendered in the office setting.
The medical services component may be reimbursed for services rendered in the outpatient hospital setting to hospital and hemophilia factor providers.
Procedure code J7178 is restricted to diagnosis code 2863.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 24.2.1 “Blood Factor Products” for more information.
Medroxyprogesterone Acetate (Depo Provera)added Procedure CodeJ1050Discontinued Procedure CodesJ1051 J1055
Limitations for added procedure codes: Procedure code J1050 may be reimbursed for services rendered to male and female clients of any age for medical indications as appropriate (as a replacement for procedure code J1051).
Providers must bill the appropriate quantity based on the amount used in milligrams (mg).
Note: The CSHCN Services Program does not cover contraception. Procedure code J1050 billed with modifier U1 (as a replacement for procedure code J1055) is not a benefit of the CSHCN Services Program.
Orthoses and Prosthesesadded Procedure CodeL5859
Limitations for added procedure codes: Procedure code L5859 may be reimbursed to home health DME, prosthetist, orthotist, DME medical suppliers, and custom DME providers for services rendered in the home setting.
Prior authorization is required.
Providers may refer to the current CSHCN Services Program Provider Manual, Chapter 28, “Orthotic and Prosthetic Devices” for more information.
Radiation Therapy Servicesadded Procedure Code32701
Texas Medicaid Special Bulletin, No. 5 20 2013 HCPCS Special Bulletin
CSHCN Services Program Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
Limitations for added procedure codes: Radiation therapy procedure code 32701 may be reimbursed to physicians and radiation treatment center providers for services rendered in the office setting; and to physicians and radiation treatment center providers for services rendered in the outpatient hospital setting.
Prior Authorization is required.
One procedure code may be reimbursed per day. If an additional procedure is medically necessary, a second procedure code may be reimbursed the same day when it is billed with modifier 76.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 33.2.8 “Stereotactic Radiosurgery,” for more information.
Sleep Studiesadded Procedure Codes95782 95783
Limitations for added procedure codes: The following benefit limitation applies for polysomnography (procedure codes 95782 and 95783):
• The total laboratory component may be reimbursed to physician, portable Xray supplier, radiological laboratory, and physiological laboratory providers for services rendered in the office setting; and to hospital providers for services rendered in the outpatient hospital setting.
• The professional component may be reimbursed to physician providers in the office, inpatient hospital, and outpatient hospital setting.
• The technical component may be reimbursed to portable Xray supplier, radiological laboratory, and physiological laboratory providers for services rendered in the office setting.
Procedure codes 95782 and 95783 may be reimbursed for services rendered to clients who are birth through 5 years of age, and must be submitted with an appropriate diagnosis code.
refer to: The CSHCN Services Program Provider Manual subsection 31.2.36.1, “Polysomnography” for the list of appropriate diagnosis codes.
Procedure code 95782 and 95783 is limited to one per day any provider.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 31.2.36.1, “Sleep Studies” for more information.
Telemedicine Servicesadded Procedure Codes90791 90792 90832 90833 90834 90836 90837 90838Discontinued Procedure Codes90801 90802 90804 90805 90806 90807 90808 90809 90862
Limitations for added procedure codes: Procedure code 90791, 90792, 90832, 90833, 90834, 90836, 90837, and 90838) may be reimbursed to distantsite providers when billed with the GT modifier.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 31.2.38, “Telemedicine Services.”
Texas Medicaid Special Bulletin, No. 5212013 HCPCS Special Bulletin
CSHCN Services Program Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
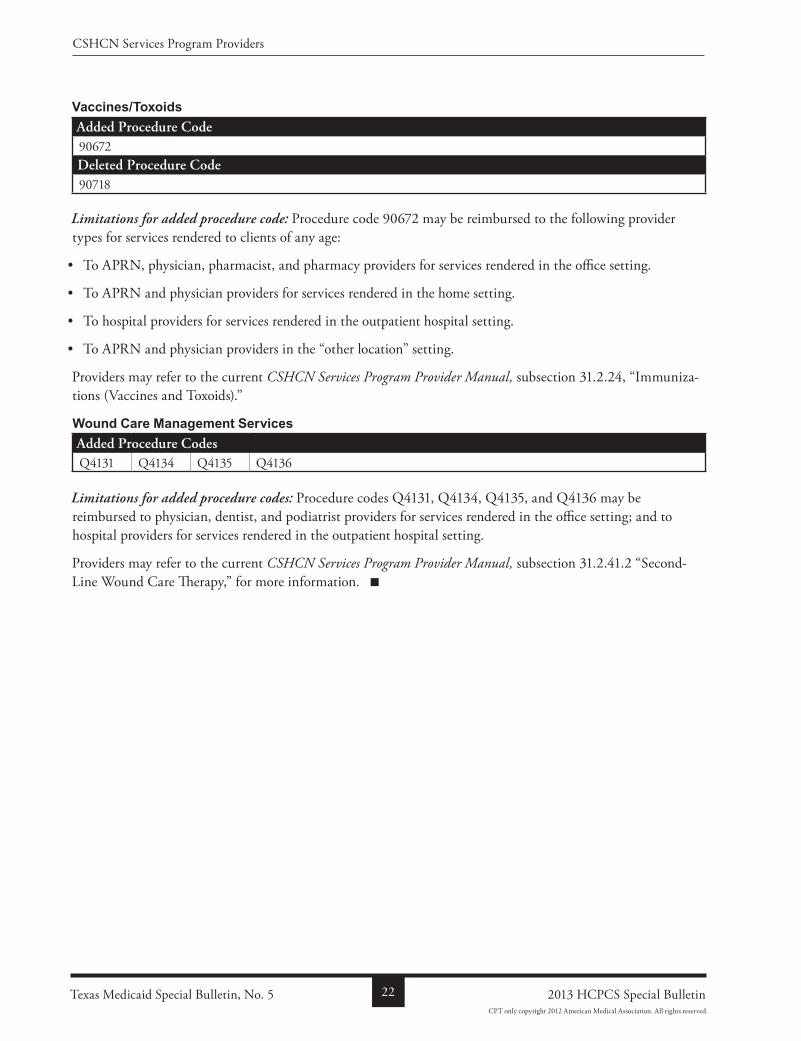
Vaccines/Toxoidsadded Procedure Code90672Deleted Procedure Code90718
Limitations for added procedure code: Procedure code 90672 may be reimbursed to the following provider types for services rendered to clients of any age:
• To APRN, physician, pharmacist, and pharmacy providers for services rendered in the office setting.
• To APRN and physician providers for services rendered in the home setting.
• To hospital providers for services rendered in the outpatient hospital setting.
• To APRN and physician providers in the “other location” setting.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 31.2.24, “Immunizations (Vaccines and Toxoids).”
Wound Care Management Servicesadded Procedure CodesQ4131 Q4134 Q4135 Q4136
Limitations for added procedure codes: Procedure codes Q4131, Q4134, Q4135, and Q4136 may be reimbursed to physician, dentist, and podiatrist providers for services rendered in the office setting; and to hospital providers for services rendered in the outpatient hospital setting.
Providers may refer to the current CSHCN Services Program Provider Manual, subsection 31.2.41.2 “SecondLine Wound Care Therapy,” for more information.
Texas Medicaid Special Bulletin, No. 5 22 2013 HCPCS Special Bulletin
CSHCN Services Program Providers
CPT only copyright 2012 American Medical Association. All rights reserved.
all code changeS: added, reviSed, rePlaceMent, and diScontinued
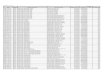
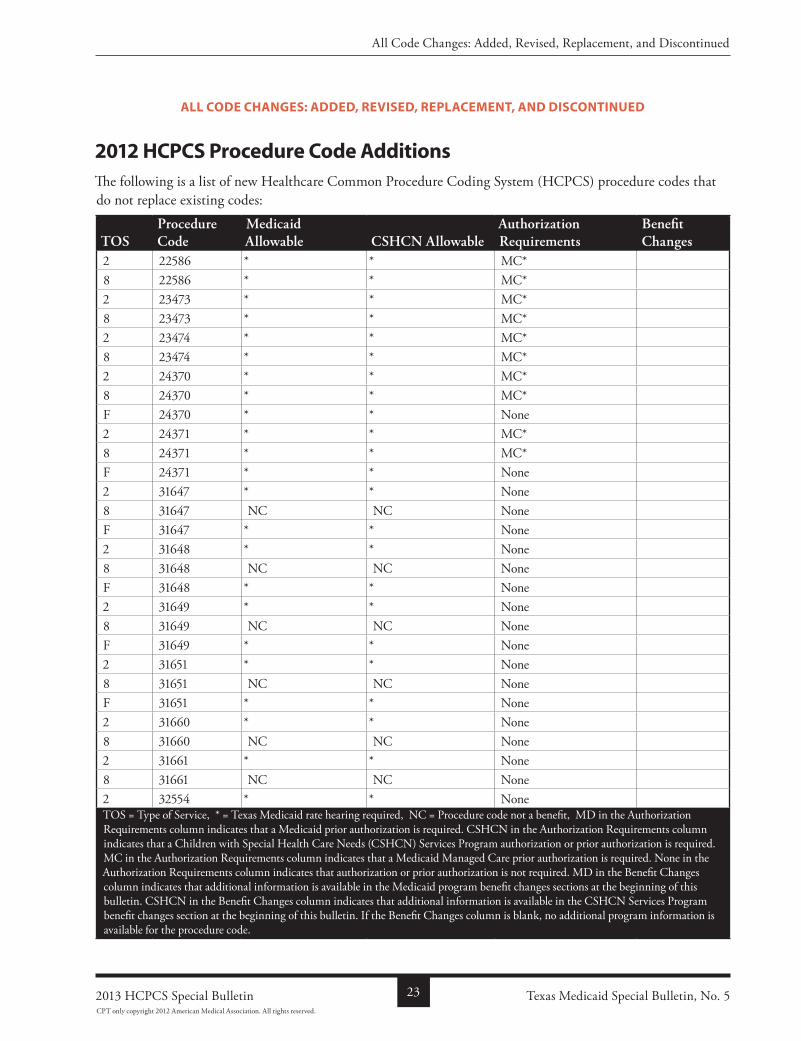
2012 HCPCS Procedure Code AdditionsThe following is a list of new Healthcare Common Procedure Coding System (HCPCS) procedure codes that do not replace existing codes:
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
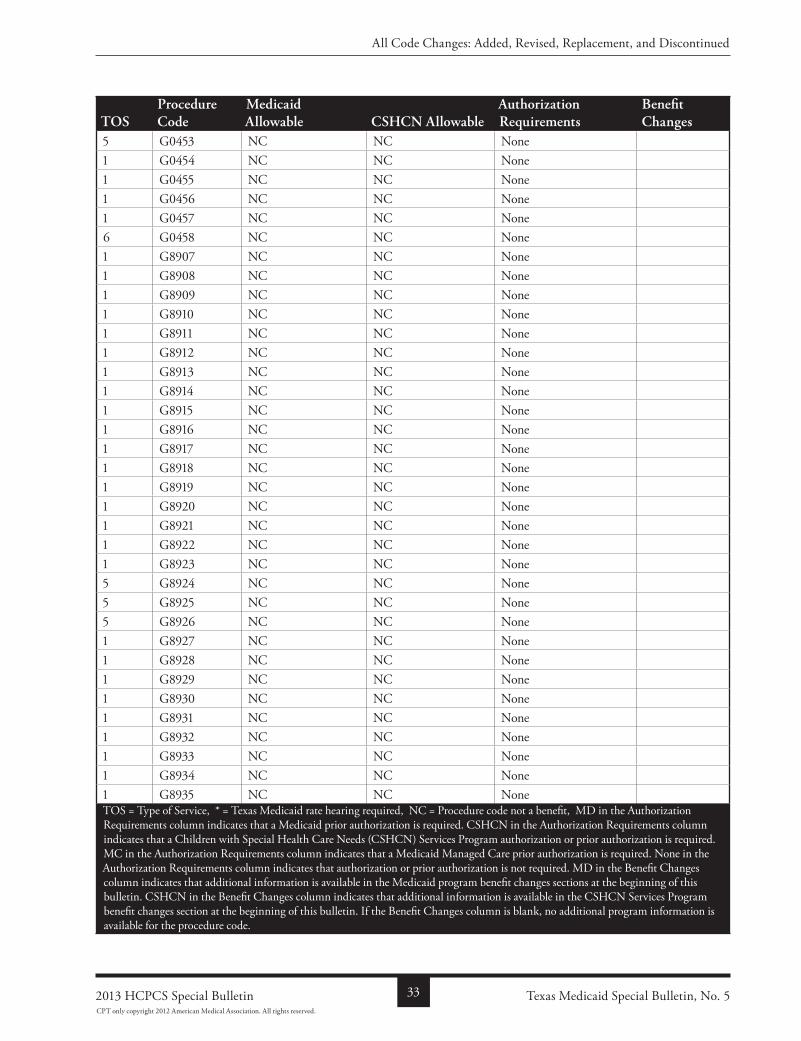
2 22586 * * MC*8 22586 * * MC*2 23473 * * MC*8 23473 * * MC*2 23474 * * MC*8 23474 * * MC*2 24370 * * MC*8 24370 * * MC*F 24370 * * None2 24371 * * MC*8 24371 * * MC*F 24371 * * None2 31647 * * None8 31647 NC NC NoneF 31647 * * None2 31648 * * None8 31648 NC NC NoneF 31648 * * None2 31649 * * None8 31649 NC NC NoneF 31649 * * None2 31651 * * None8 31651 NC NC NoneF 31651 * * None2 31660 * * None8 31660 NC NC None2 31661 * * None8 31661 NC NC None2 32554 * * NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5232013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
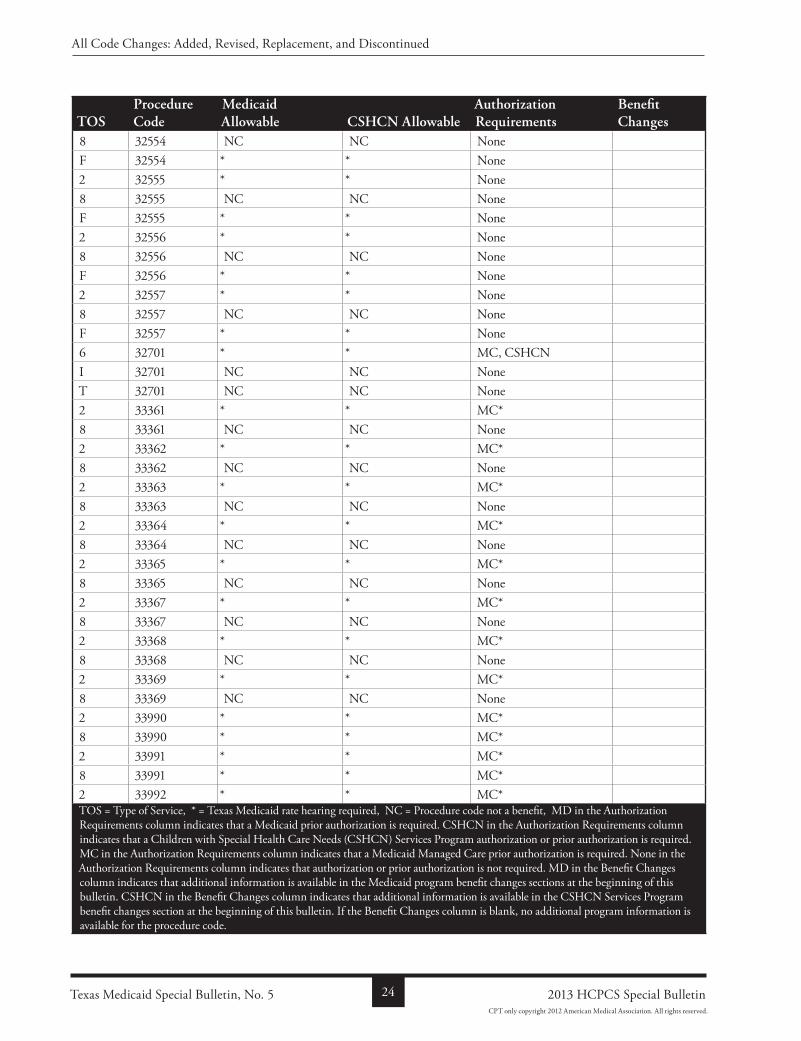
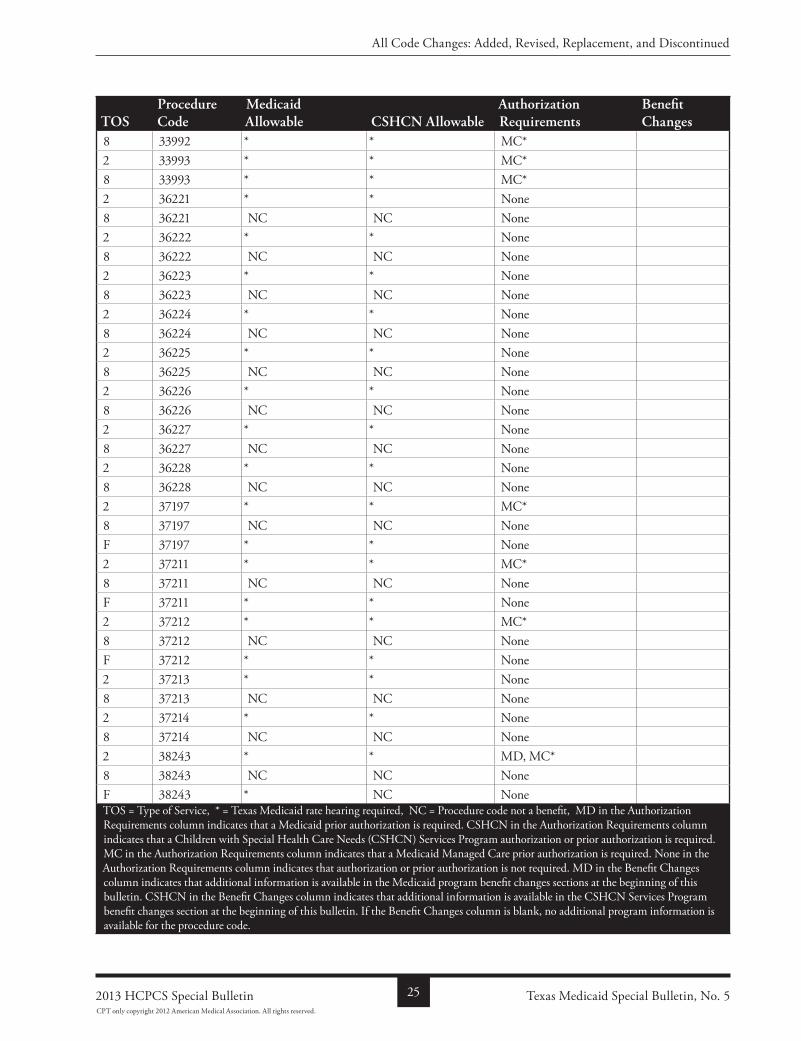
8 32554 NC NC NoneF 32554 * * None2 32555 * * None8 32555 NC NC NoneF 32555 * * None2 32556 * * None8 32556 NC NC NoneF 32556 * * None2 32557 * * None8 32557 NC NC NoneF 32557 * * None6 32701 * * MC, CSHCNI 32701 NC NC NoneT 32701 NC NC None2 33361 * * MC*8 33361 NC NC None2 33362 * * MC*8 33362 NC NC None2 33363 * * MC*8 33363 NC NC None2 33364 * * MC*8 33364 NC NC None2 33365 * * MC*8 33365 NC NC None2 33367 * * MC*8 33367 NC NC None2 33368 * * MC*8 33368 NC NC None2 33369 * * MC*8 33369 NC NC None2 33990 * * MC*8 33990 * * MC*2 33991 * * MC*8 33991 * * MC*2 33992 * * MC*TOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5 24 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
8 33992 * * MC*2 33993 * * MC*8 33993 * * MC*2 36221 * * None8 36221 NC NC None2 36222 * * None8 36222 NC NC None2 36223 * * None8 36223 NC NC None2 36224 * * None8 36224 NC NC None2 36225 * * None8 36225 NC NC None2 36226 * * None8 36226 NC NC None2 36227 * * None8 36227 NC NC None2 36228 * * None8 36228 NC NC None2 37197 * * MC*8 37197 NC NC NoneF 37197 * * None2 37211 * * MC*8 37211 NC NC NoneF 37211 * * None2 37212 * * MC*8 37212 NC NC NoneF 37212 * * None2 37213 * * None8 37213 NC NC None2 37214 * * None8 37214 NC NC None2 38243 * * MD, MC*8 38243 NC NC NoneF 38243 * NC NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5252013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
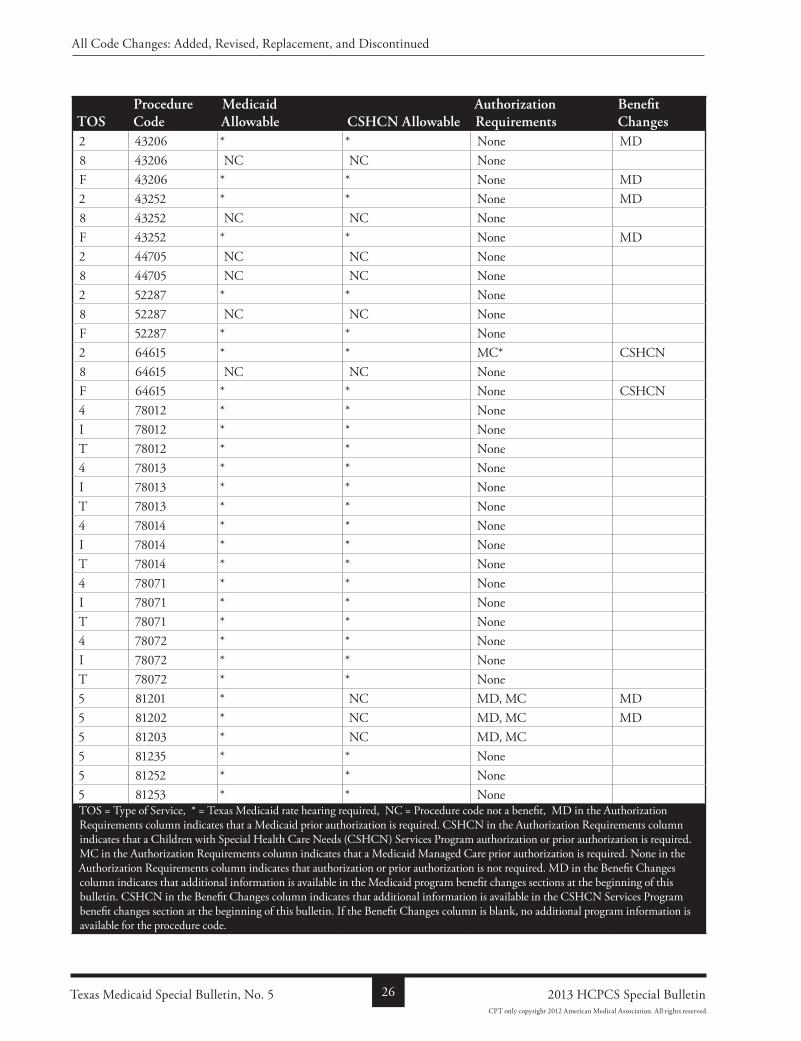
2 43206 * * None MD8 43206 NC NC NoneF 43206 * * None MD2 43252 * * None MD8 43252 NC NC NoneF 43252 * * None MD2 44705 NC NC None8 44705 NC NC None2 52287 * * None8 52287 NC NC NoneF 52287 * * None2 64615 * * MC* CSHCN8 64615 NC NC NoneF 64615 * * None CSHCN4 78012 * * NoneI 78012 * * NoneT 78012 * * None4 78013 * * NoneI 78013 * * NoneT 78013 * * None4 78014 * * NoneI 78014 * * NoneT 78014 * * None4 78071 * * NoneI 78071 * * NoneT 78071 * * None4 78072 * * NoneI 78072 * * NoneT 78072 * * None5 81201 * NC MD, MC MD5 81202 * NC MD, MC MD5 81203 * NC MD, MC5 81235 * * None5 81252 * * None5 81253 * * NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5 26 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
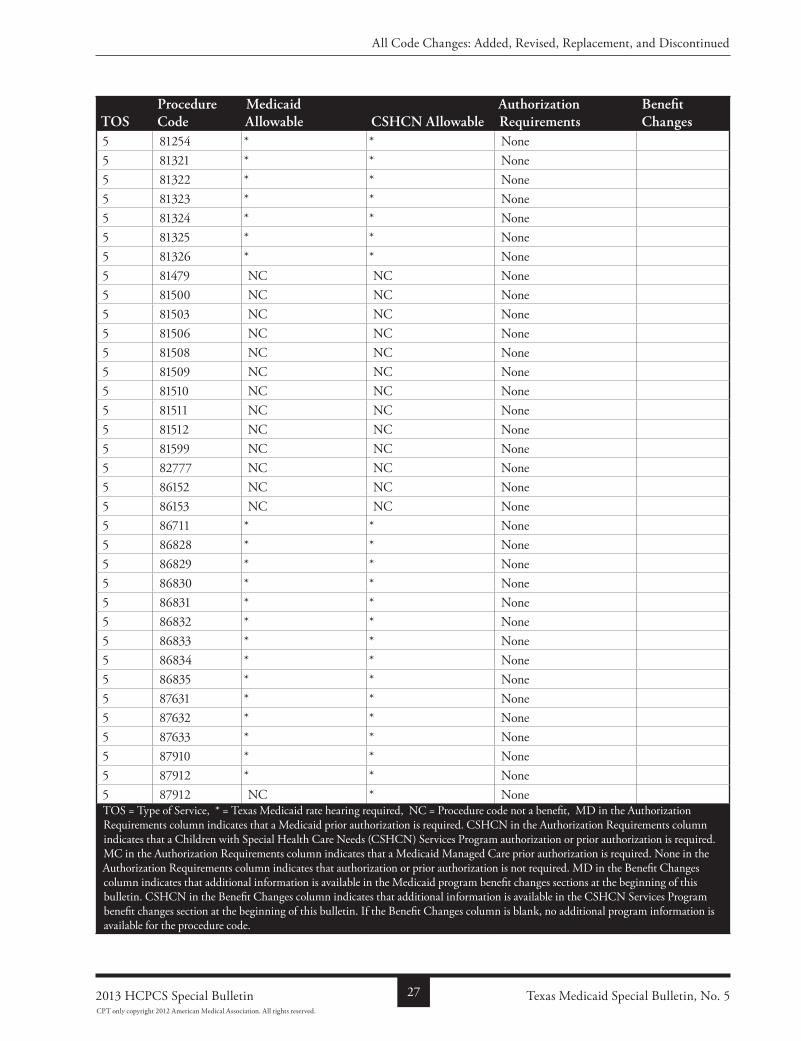
5 81254 * * None5 81321 * * None5 81322 * * None5 81323 * * None5 81324 * * None5 81325 * * None5 81326 * * None5 81479 NC NC None5 81500 NC NC None5 81503 NC NC None5 81506 NC NC None5 81508 NC NC None5 81509 NC NC None5 81510 NC NC None5 81511 NC NC None5 81512 NC NC None5 81599 NC NC None5 82777 NC NC None5 86152 NC NC None5 86153 NC NC None5 86711 * * None5 86828 * * None5 86829 * * None5 86830 * * None5 86831 * * None5 86832 * * None5 86833 * * None5 86834 * * None5 86835 * * None5 87631 * * None5 87632 * * None5 87633 * * None5 87910 * * None5 87912 * * None5 87912 NC * NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5272013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
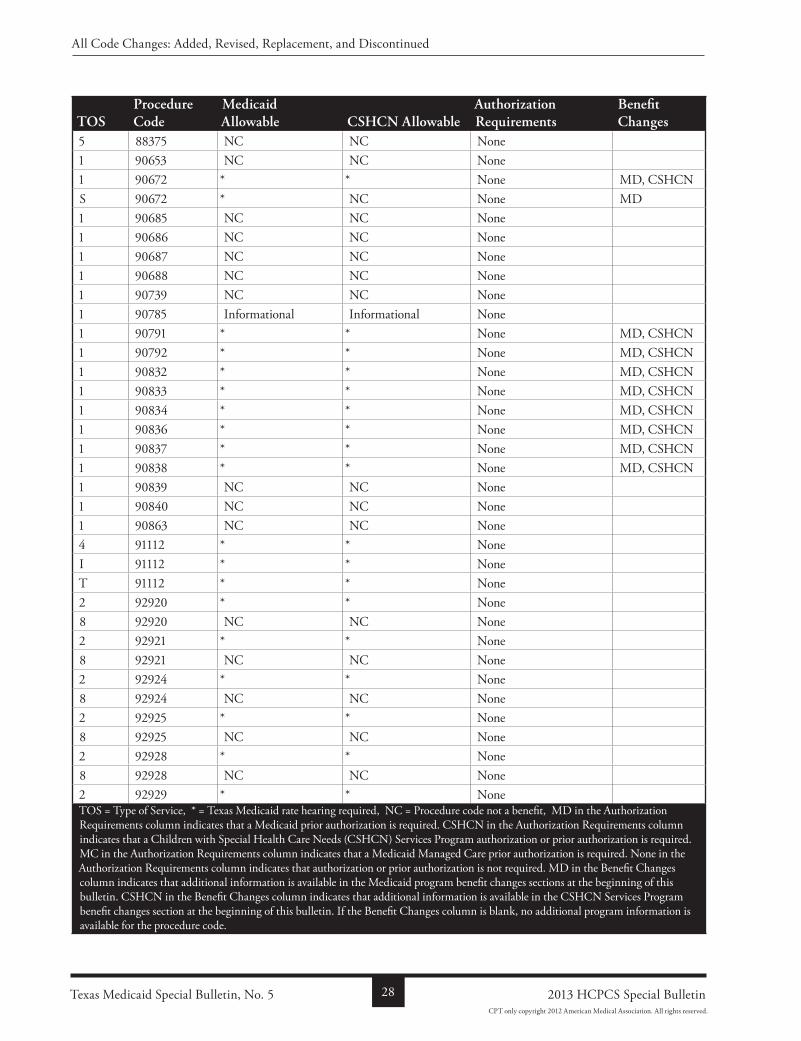
5 88375 NC NC None1 90653 NC NC None1 90672 * * None MD, CSHCNS 90672 * NC None MD1 90685 NC NC None1 90686 NC NC None1 90687 NC NC None1 90688 NC NC None1 90739 NC NC None1 90785 Informational Informational None1 90791 * * None MD, CSHCN1 90792 * * None MD, CSHCN1 90832 * * None MD, CSHCN1 90833 * * None MD, CSHCN1 90834 * * None MD, CSHCN1 90836 * * None MD, CSHCN1 90837 * * None MD, CSHCN1 90838 * * None MD, CSHCN1 90839 NC NC None1 90840 NC NC None1 90863 NC NC None4 91112 * * NoneI 91112 * * NoneT 91112 * * None2 92920 * * None8 92920 NC NC None2 92921 * * None8 92921 NC NC None2 92924 * * None8 92924 NC NC None2 92925 * * None8 92925 NC NC None2 92928 * * None8 92928 NC NC None2 92929 * * NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5 28 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
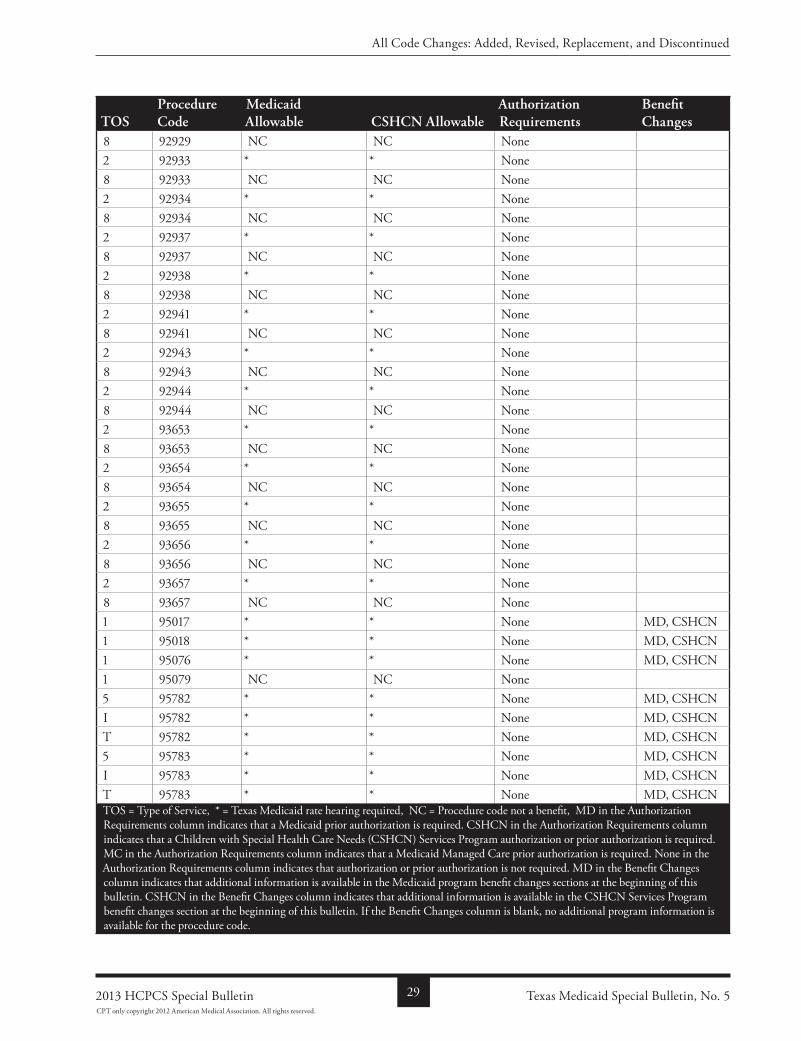
8 92929 NC NC None2 92933 * * None8 92933 NC NC None2 92934 * * None8 92934 NC NC None2 92937 * * None8 92937 NC NC None2 92938 * * None8 92938 NC NC None2 92941 * * None8 92941 NC NC None2 92943 * * None8 92943 NC NC None2 92944 * * None8 92944 NC NC None2 93653 * * None8 93653 NC NC None2 93654 * * None8 93654 NC NC None2 93655 * * None8 93655 NC NC None2 93656 * * None8 93656 NC NC None2 93657 * * None8 93657 NC NC None1 95017 * * None MD, CSHCN1 95018 * * None MD, CSHCN1 95076 * * None MD, CSHCN1 95079 NC NC None5 95782 * * None MD, CSHCNI 95782 * * None MD, CSHCNT 95782 * * None MD, CSHCN5 95783 * * None MD, CSHCNI 95783 * * None MD, CSHCNT 95783 * * None MD, CSHCNTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5292013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
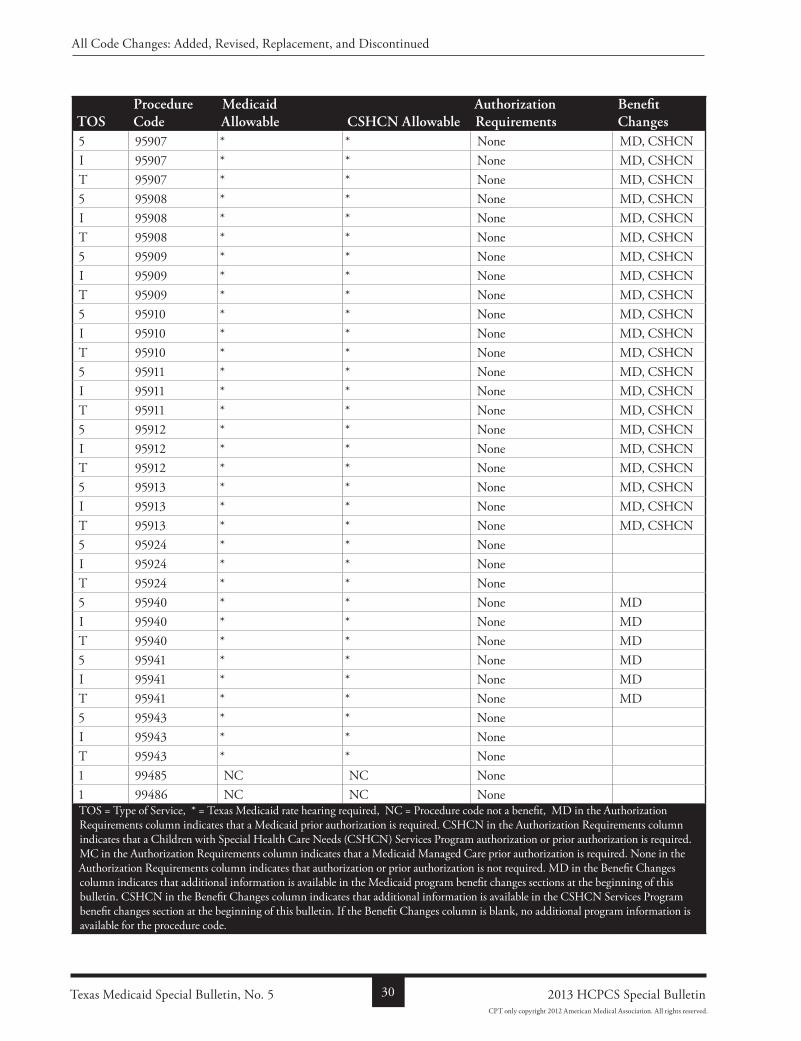
5 95907 * * None MD, CSHCNI 95907 * * None MD, CSHCNT 95907 * * None MD, CSHCN5 95908 * * None MD, CSHCNI 95908 * * None MD, CSHCNT 95908 * * None MD, CSHCN5 95909 * * None MD, CSHCNI 95909 * * None MD, CSHCNT 95909 * * None MD, CSHCN5 95910 * * None MD, CSHCNI 95910 * * None MD, CSHCNT 95910 * * None MD, CSHCN5 95911 * * None MD, CSHCNI 95911 * * None MD, CSHCNT 95911 * * None MD, CSHCN5 95912 * * None MD, CSHCNI 95912 * * None MD, CSHCNT 95912 * * None MD, CSHCN5 95913 * * None MD, CSHCNI 95913 * * None MD, CSHCNT 95913 * * None MD, CSHCN5 95924 * * NoneI 95924 * * NoneT 95924 * * None5 95940 * * None MDI 95940 * * None MDT 95940 * * None MD5 95941 * * None MDI 95941 * * None MDT 95941 * * None MD5 95943 * * NoneI 95943 * * NoneT 95943 * * None1 99485 NC NC None1 99486 NC NC NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5 30 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
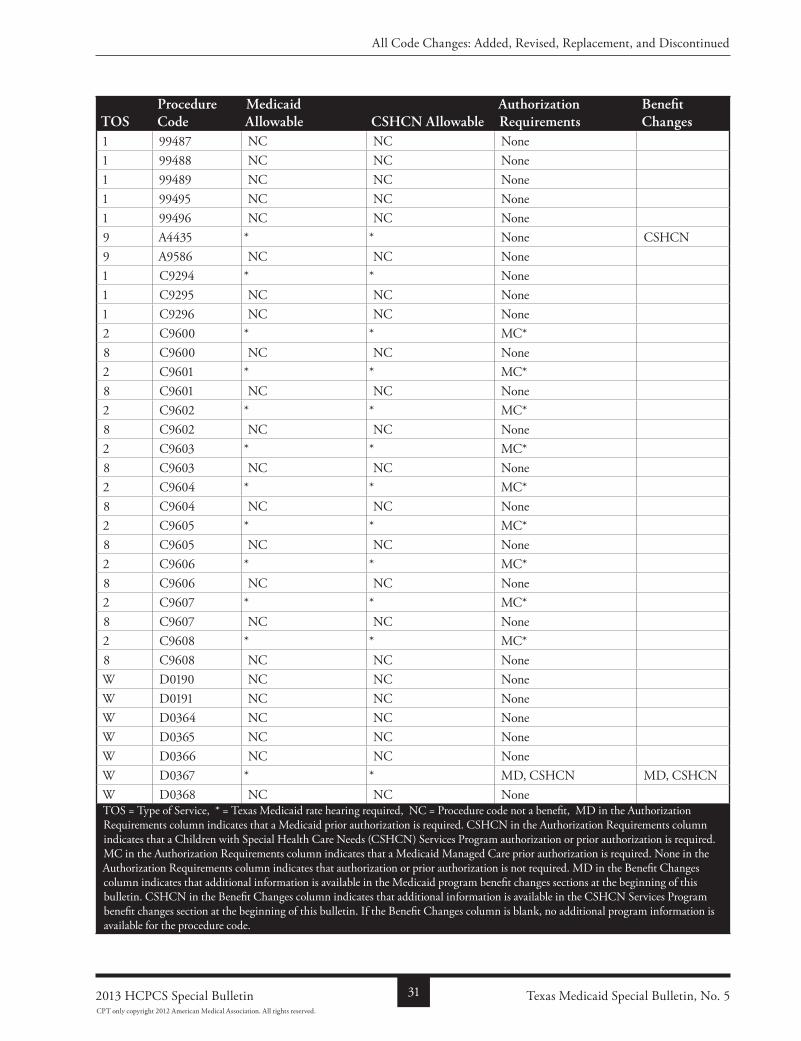
1 99487 NC NC None1 99488 NC NC None1 99489 NC NC None1 99495 NC NC None1 99496 NC NC None9 A4435 * * None CSHCN9 A9586 NC NC None1 C9294 * * None1 C9295 NC NC None1 C9296 NC NC None2 C9600 * * MC*8 C9600 NC NC None2 C9601 * * MC*8 C9601 NC NC None2 C9602 * * MC*8 C9602 NC NC None2 C9603 * * MC*8 C9603 NC NC None2 C9604 * * MC*8 C9604 NC NC None2 C9605 * * MC*8 C9605 NC NC None2 C9606 * * MC*8 C9606 NC NC None2 C9607 * * MC*8 C9607 NC NC None2 C9608 * * MC*8 C9608 NC NC NoneW D0190 NC NC NoneW D0191 NC NC NoneW D0364 NC NC NoneW D0365 NC NC NoneW D0366 NC NC NoneW D0367 * * MD, CSHCN MD, CSHCNW D0368 NC NC NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5312013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
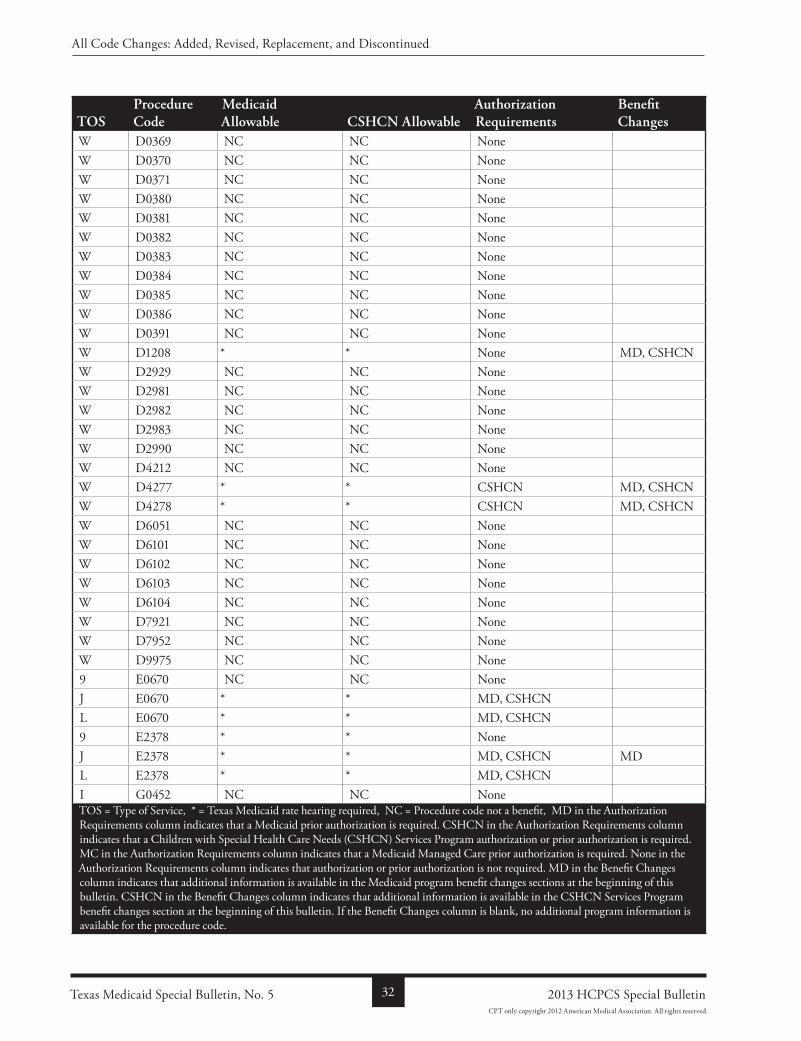
W D0369 NC NC NoneW D0370 NC NC NoneW D0371 NC NC NoneW D0380 NC NC NoneW D0381 NC NC NoneW D0382 NC NC NoneW D0383 NC NC NoneW D0384 NC NC NoneW D0385 NC NC NoneW D0386 NC NC NoneW D0391 NC NC NoneW D1208 * * None MD, CSHCNW D2929 NC NC NoneW D2981 NC NC NoneW D2982 NC NC NoneW D2983 NC NC NoneW D2990 NC NC NoneW D4212 NC NC NoneW D4277 * * CSHCN MD, CSHCNW D4278 * * CSHCN MD, CSHCNW D6051 NC NC NoneW D6101 NC NC NoneW D6102 NC NC NoneW D6103 NC NC NoneW D6104 NC NC NoneW D7921 NC NC NoneW D7952 NC NC NoneW D9975 NC NC None9 E0670 NC NC NoneJ E0670 * * MD, CSHCNL E0670 * * MD, CSHCN9 E2378 * * NoneJ E2378 * * MD, CSHCN MDL E2378 * * MD, CSHCNI G0452 NC NC NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5 32 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
5 G0453 NC NC None1 G0454 NC NC None1 G0455 NC NC None1 G0456 NC NC None1 G0457 NC NC None6 G0458 NC NC None1 G8907 NC NC None1 G8908 NC NC None1 G8909 NC NC None1 G8910 NC NC None1 G8911 NC NC None1 G8912 NC NC None1 G8913 NC NC None1 G8914 NC NC None1 G8915 NC NC None1 G8916 NC NC None1 G8917 NC NC None1 G8918 NC NC None1 G8919 NC NC None1 G8920 NC NC None1 G8921 NC NC None1 G8922 NC NC None1 G8923 NC NC None5 G8924 NC NC None5 G8925 NC NC None5 G8926 NC NC None1 G8927 NC NC None1 G8928 NC NC None1 G8929 NC NC None1 G8930 NC NC None1 G8931 NC NC None1 G8932 NC NC None1 G8933 NC NC None1 G8934 NC NC None1 G8935 NC NC NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5332013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
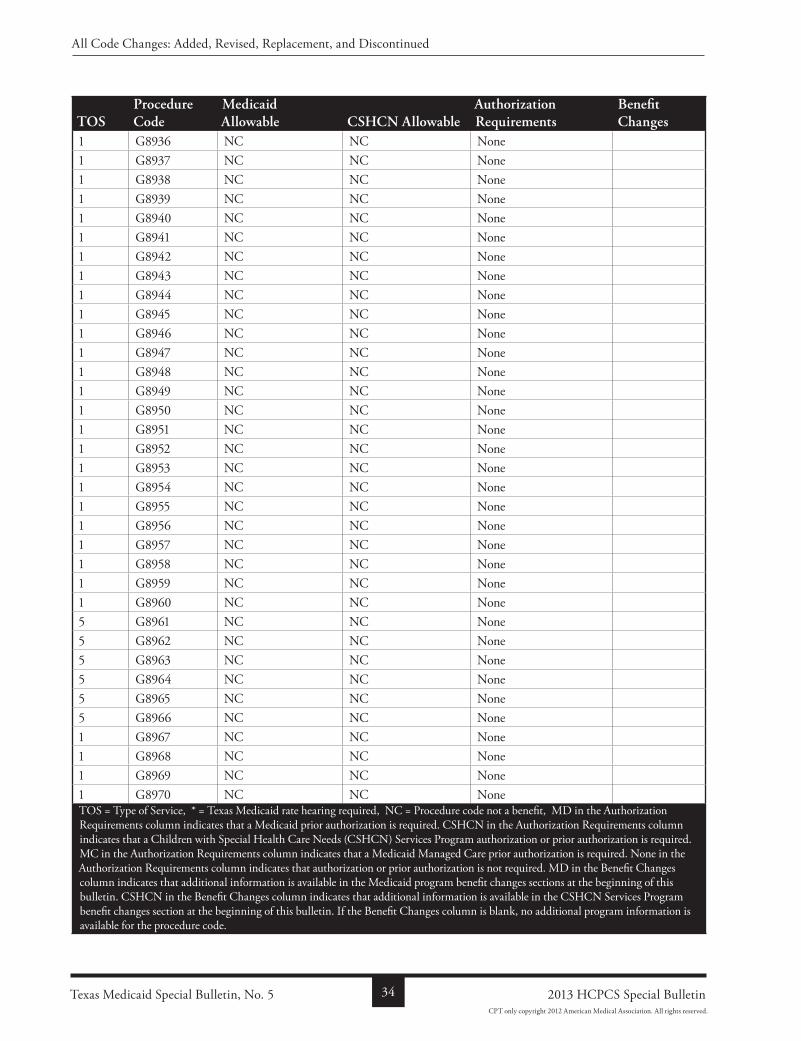
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
1 G8936 NC NC None1 G8937 NC NC None1 G8938 NC NC None1 G8939 NC NC None1 G8940 NC NC None1 G8941 NC NC None1 G8942 NC NC None1 G8943 NC NC None1 G8944 NC NC None1 G8945 NC NC None1 G8946 NC NC None1 G8947 NC NC None1 G8948 NC NC None1 G8949 NC NC None1 G8950 NC NC None1 G8951 NC NC None1 G8952 NC NC None1 G8953 NC NC None1 G8954 NC NC None1 G8955 NC NC None1 G8956 NC NC None1 G8957 NC NC None1 G8958 NC NC None1 G8959 NC NC None1 G8960 NC NC None5 G8961 NC NC None5 G8962 NC NC None5 G8963 NC NC None5 G8964 NC NC None5 G8965 NC NC None5 G8966 NC NC None1 G8967 NC NC None1 G8968 NC NC None1 G8969 NC NC None1 G8970 NC NC NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5 34 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
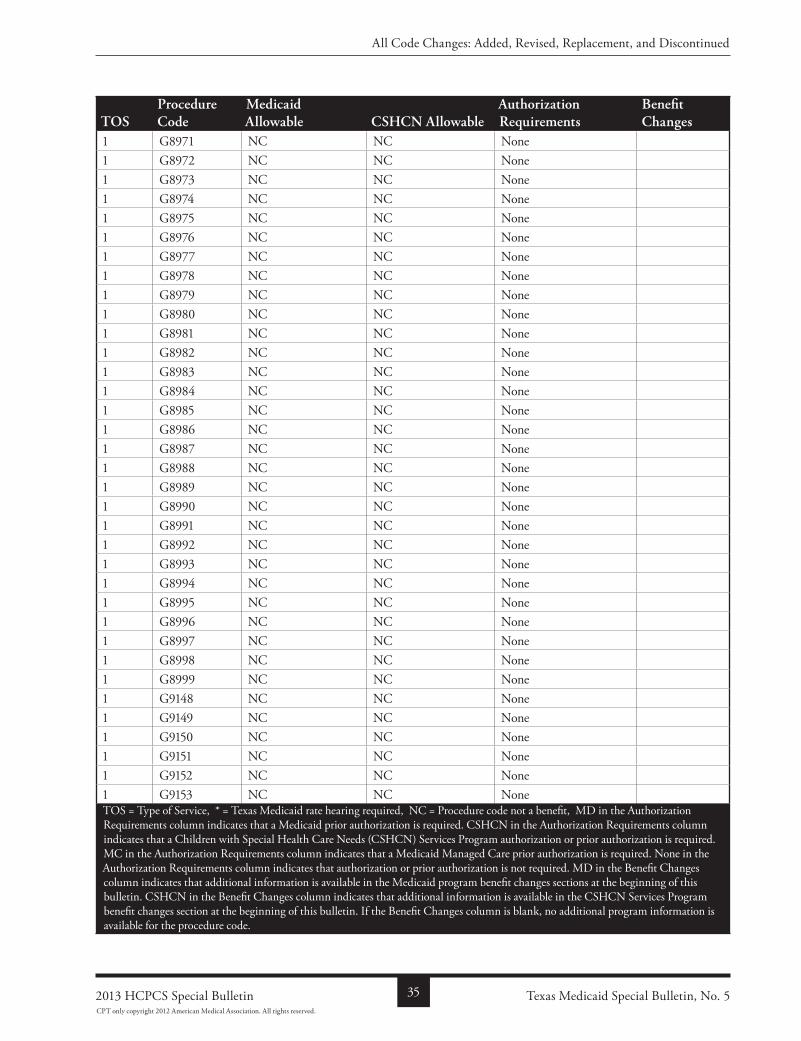
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
1 G8971 NC NC None1 G8972 NC NC None1 G8973 NC NC None1 G8974 NC NC None1 G8975 NC NC None1 G8976 NC NC None1 G8977 NC NC None1 G8978 NC NC None1 G8979 NC NC None1 G8980 NC NC None1 G8981 NC NC None1 G8982 NC NC None1 G8983 NC NC None1 G8984 NC NC None1 G8985 NC NC None1 G8986 NC NC None1 G8987 NC NC None1 G8988 NC NC None1 G8989 NC NC None1 G8990 NC NC None1 G8991 NC NC None1 G8992 NC NC None1 G8993 NC NC None1 G8994 NC NC None1 G8995 NC NC None1 G8996 NC NC None1 G8997 NC NC None1 G8998 NC NC None1 G8999 NC NC None1 G9148 NC NC None1 G9149 NC NC None1 G9150 NC NC None1 G9151 NC NC None1 G9152 NC NC None1 G9153 NC NC NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5352013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
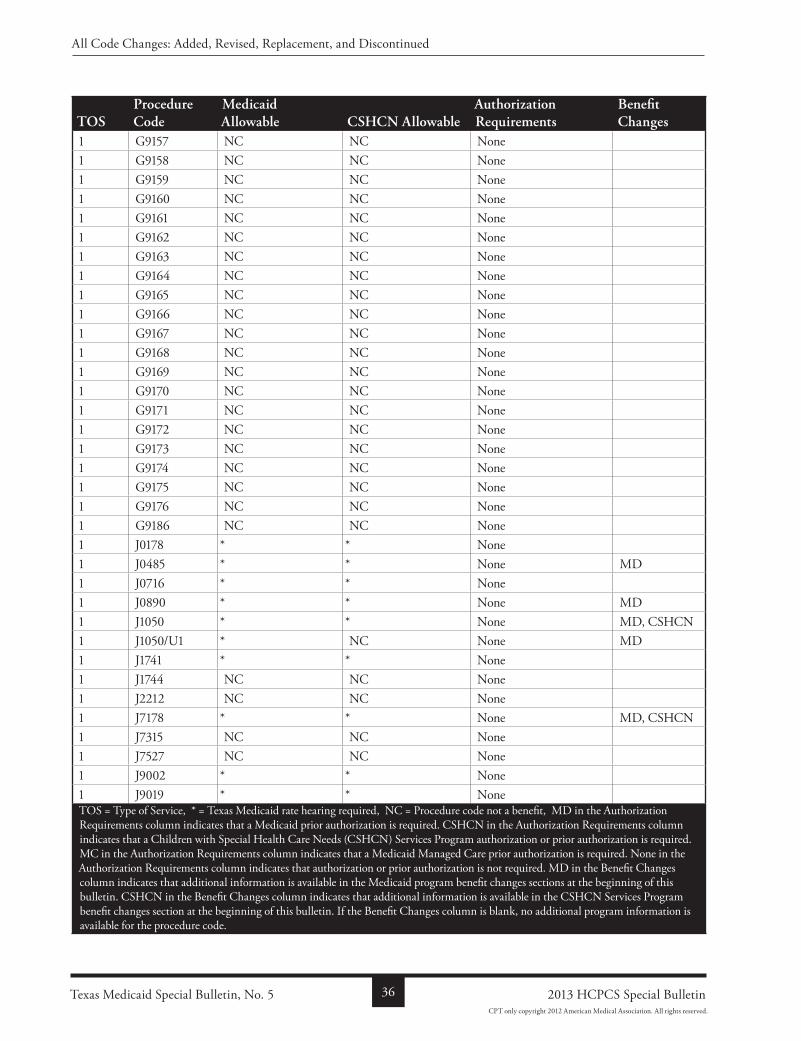
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
1 G9157 NC NC None1 G9158 NC NC None1 G9159 NC NC None1 G9160 NC NC None1 G9161 NC NC None1 G9162 NC NC None1 G9163 NC NC None1 G9164 NC NC None1 G9165 NC NC None1 G9166 NC NC None1 G9167 NC NC None1 G9168 NC NC None1 G9169 NC NC None1 G9170 NC NC None1 G9171 NC NC None1 G9172 NC NC None1 G9173 NC NC None1 G9174 NC NC None1 G9175 NC NC None1 G9176 NC NC None1 G9186 NC NC None1 J0178 * * None1 J0485 * * None MD1 J0716 * * None1 J0890 * * None MD1 J1050 * * None MD, CSHCN1 J1050/U1 * NC None MD1 J1741 * * None1 J1744 NC NC None1 J2212 NC NC None1 J7178 * * None MD, CSHCN1 J7315 NC NC None1 J7527 NC NC None1 J9002 * * None1 J9019 * * NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Texas Medicaid Special Bulletin, No. 5 36 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
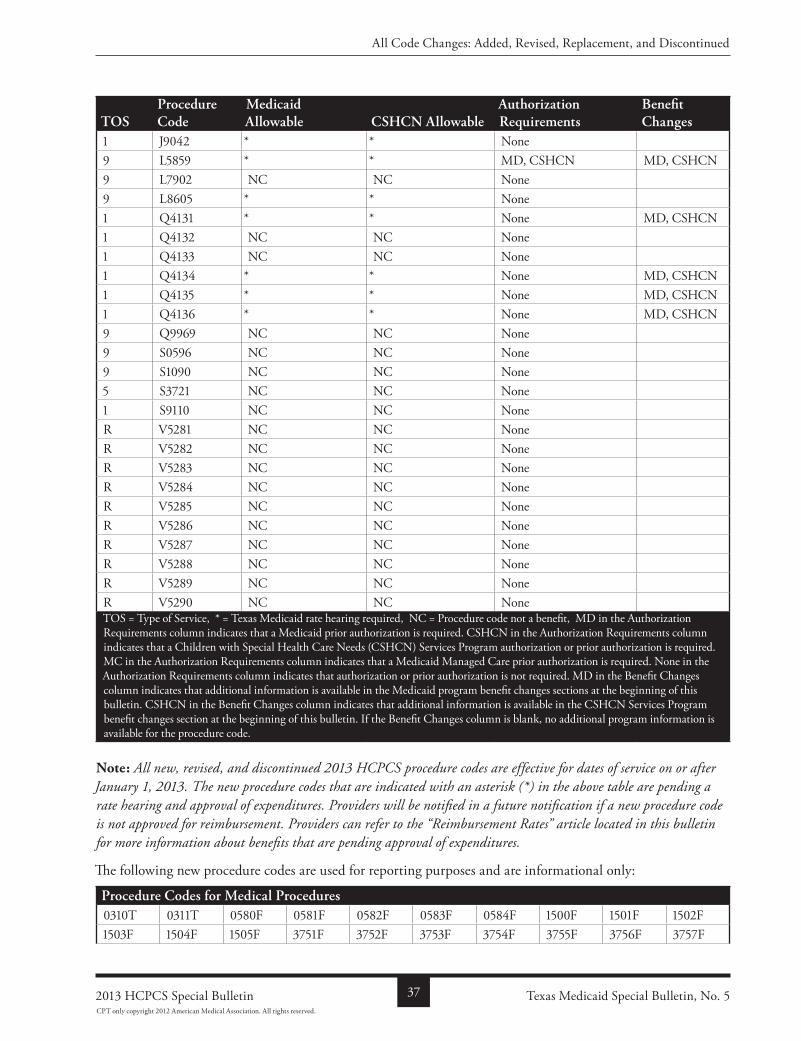
ToSProcedure Code
Medicaid allowable CSHCn allowable
authorization requirements
Benefit Changes
1 J9042 * * None9 L5859 * * MD, CSHCN MD, CSHCN9 L7902 NC NC None9 L8605 * * None1 Q4131 * * None MD, CSHCN1 Q4132 NC NC None1 Q4133 NC NC None1 Q4134 * * None MD, CSHCN1 Q4135 * * None MD, CSHCN1 Q4136 * * None MD, CSHCN9 Q9969 NC NC None9 S0596 NC NC None9 S1090 NC NC None5 S3721 NC NC None1 S9110 NC NC NoneR V5281 NC NC NoneR V5282 NC NC NoneR V5283 NC NC NoneR V5284 NC NC NoneR V5285 NC NC NoneR V5286 NC NC NoneR V5287 NC NC NoneR V5288 NC NC NoneR V5289 NC NC NoneR V5290 NC NC NoneTOS = Type of Service, * = Texas Medicaid rate hearing required, NC = Procedure code not a benefit, MD in the Authorization Requirements column indicates that a Medicaid prior authorization is required. CSHCN in the Authorization Requirements column indicates that a Children with Special Health Care Needs (CSHCN) Services Program authorization or prior authorization is required. MC in the Authorization Requirements column indicates that a Medicaid Managed Care prior authorization is required. None in the Authorization Requirements column indicates that authorization or prior authorization is not required. MD in the Benefit Changes column indicates that additional information is available in the Medicaid program benefit changes sections at the beginning of this bulletin. CSHCN in the Benefit Changes column indicates that additional information is available in the CSHCN Services Program benefit changes section at the beginning of this bulletin. If the Benefit Changes column is blank, no additional program information is available for the procedure code.
Note: All new, revised, and discontinued 2013 HCPCS procedure codes are effective for dates of service on or after January 1, 2013. The new procedure codes that are indicated with an asterisk (*) in the above table are pending a rate hearing and approval of expenditures. Providers will be notified in a future notification if a new procedure code is not approved for reimbursement. Providers can refer to the “Reimbursement Rates” article located in this bulletin for more information about benefits that are pending approval of expenditures.
The following new procedure codes are used for reporting purposes and are informational only:
Procedure Codes for Medical Procedures0310T 0311T 0580F 0581F 0582F 0583F 0584F 1500F 1501F 1502F1503F 1504F 1505F 3751F 3752F 3753F 3754F 3755F 3756F 3757F
Texas Medicaid Special Bulletin, No. 5372013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
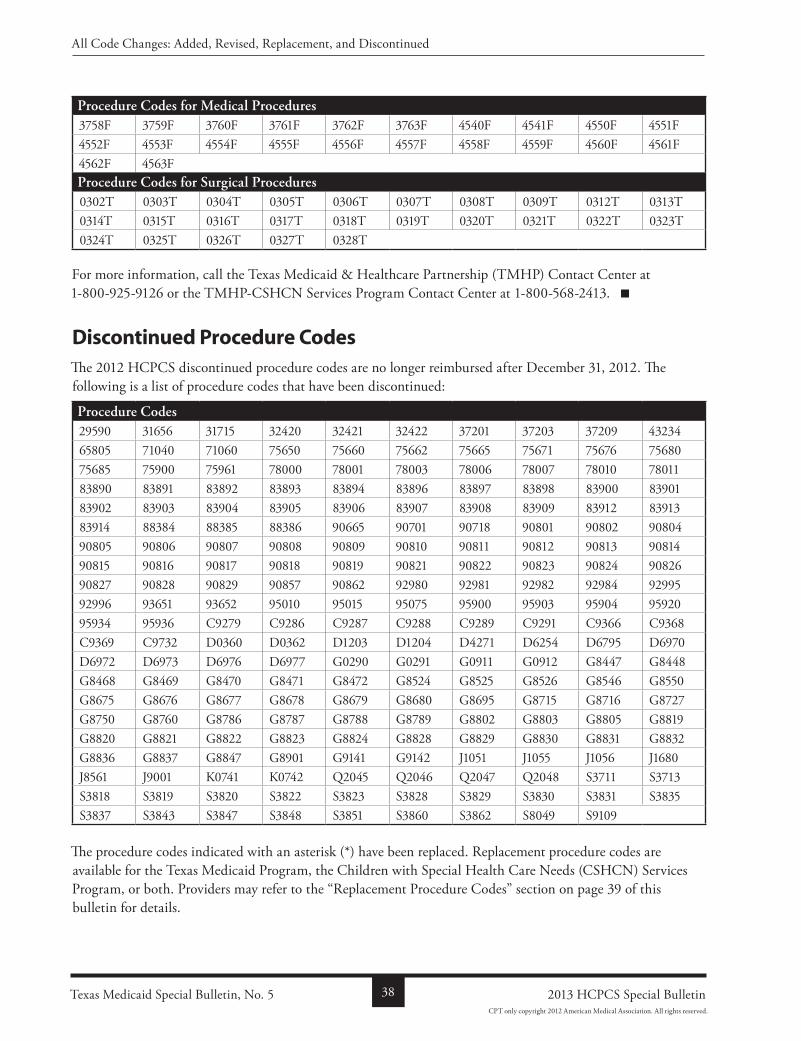
Procedure Codes for Medical Procedures3758F 3759F 3760F 3761F 3762F 3763F 4540F 4541F 4550F 4551F4552F 4553F 4554F 4555F 4556F 4557F 4558F 4559F 4560F 4561F4562F 4563FProcedure Codes for Surgical Procedures0302T 0303T 0304T 0305T 0306T 0307T 0308T 0309T 0312T 0313T0314T 0315T 0316T 0317T 0318T 0319T 0320T 0321T 0322T 0323T0324T 0325T 0326T 0327T 0328T
For more information, call the Texas Medicaid & Healthcare Partnership (TMHP) Contact Center at 18009259126 or the TMHPCSHCN Services Program Contact Center at 18005682413.
Discontinued Procedure CodesThe 2012 HCPCS discontinued procedure codes are no longer reimbursed after December 31, 2012. The following is a list of procedure codes that have been discontinued:
Procedure Codes29590 31656 31715 32420 32421 32422 37201 37203 37209 4323465805 71040 71060 75650 75660 75662 75665 75671 75676 7568075685 75900 75961 78000 78001 78003 78006 78007 78010 7801183890 83891 83892 83893 83894 83896 83897 83898 83900 8390183902 83903 83904 83905 83906 83907 83908 83909 83912 8391383914 88384 88385 88386 90665 90701 90718 90801 90802 9080490805 90806 90807 90808 90809 90810 90811 90812 90813 9081490815 90816 90817 90818 90819 90821 90822 90823 90824 9082690827 90828 90829 90857 90862 92980 92981 92982 92984 9299592996 93651 93652 95010 95015 95075 95900 95903 95904 9592095934 95936 C9279 C9286 C9287 C9288 C9289 C9291 C9366 C9368C9369 C9732 D0360 D0362 D1203 D1204 D4271 D6254 D6795 D6970D6972 D6973 D6976 D6977 G0290 G0291 G0911 G0912 G8447 G8448G8468 G8469 G8470 G8471 G8472 G8524 G8525 G8526 G8546 G8550G8675 G8676 G8677 G8678 G8679 G8680 G8695 G8715 G8716 G8727G8750 G8760 G8786 G8787 G8788 G8789 G8802 G8803 G8805 G8819G8820 G8821 G8822 G8823 G8824 G8828 G8829 G8830 G8831 G8832G8836 G8837 G8847 G8901 G9141 G9142 J1051 J1055 J1056 J1680J8561 J9001 K0741 K0742 Q2045 Q2046 Q2047 Q2048 S3711 S3713S3818 S3819 S3820 S3822 S3823 S3828 S3829 S3830 S3831 S3835S3837 S3843 S3847 S3848 S3851 S3860 S3862 S8049 S9109
The procedure codes indicated with an asterisk (*) have been replaced. Replacement procedure codes are available for the Texas Medicaid Program, the Children with Special Health Care Needs (CSHCN) Services Program, or both. Providers may refer to the “Replacement Procedure Codes” section on page 39 of this bulletin for details.
Texas Medicaid Special Bulletin, No. 5 38 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
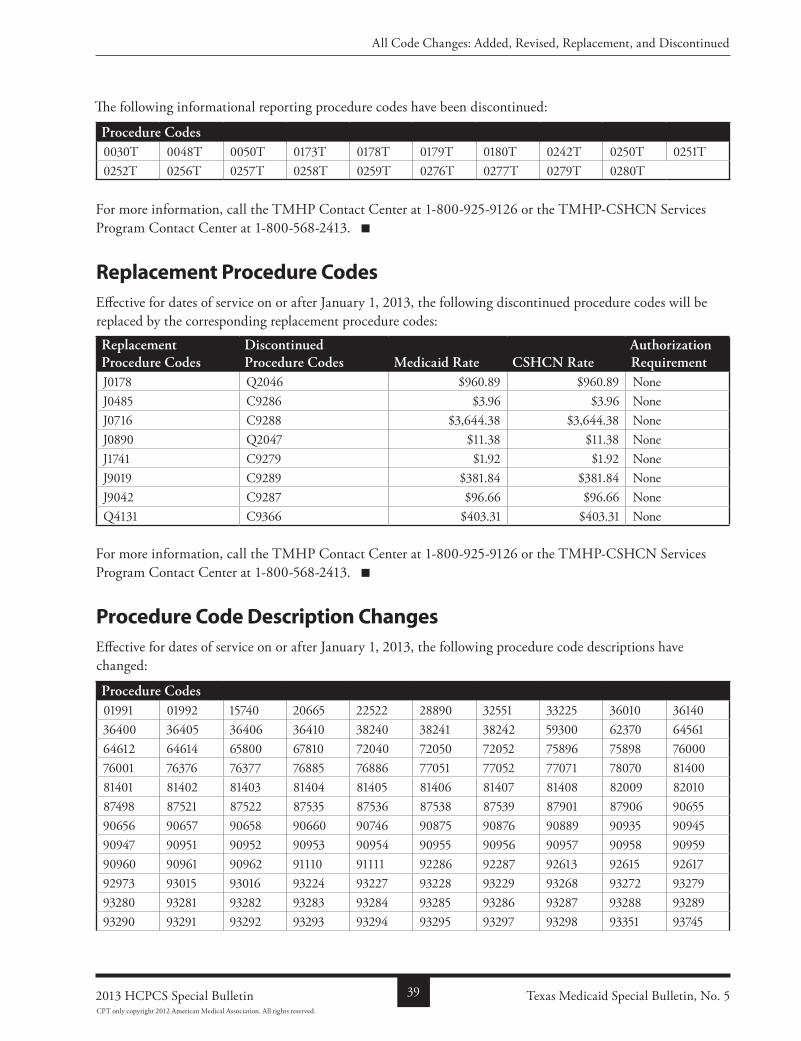
The following informational reporting procedure codes have been discontinued:
Procedure Codes0030T 0048T 0050T 0173T 0178T 0179T 0180T 0242T 0250T 0251T0252T 0256T 0257T 0258T 0259T 0276T 0277T 0279T 0280T
For more information, call the TMHP Contact Center at 18009259126 or the TMHPCSHCN Services Program Contact Center at 18005682413.
Replacement Procedure CodesEffective for dates of service on or after January 1, 2013, the following discontinued procedure codes will be replaced by the corresponding replacement procedure codes:
replacement Procedure Codes
Discontinued Procedure Codes Medicaid rate CSHCn rate
authorization requirement
J0178 Q2046 $960.89 $960.89 NoneJ0485 C9286 $3.96 $3.96 NoneJ0716 C9288 $3,644.38 $3,644.38 NoneJ0890 Q2047 $11.38 $11.38 NoneJ1741 C9279 $1.92 $1.92 NoneJ9019 C9289 $381.84 $381.84 NoneJ9042 C9287 $96.66 $96.66 NoneQ4131 C9366 $403.31 $403.31 None
For more information, call the TMHP Contact Center at 18009259126 or the TMHPCSHCN Services Program Contact Center at 18005682413.
Procedure Code Description ChangesEffective for dates of service on or after January 1, 2013, the following procedure code descriptions have changed:
Procedure Codes01991 01992 15740 20665 22522 28890 32551 33225 36010 3614036400 36405 36406 36410 38240 38241 38242 59300 62370 6456164612 64614 65800 67810 72040 72050 72052 75896 75898 7600076001 76376 76377 76885 76886 77051 77052 77071 78070 8140081401 81402 81403 81404 81405 81406 81407 81408 82009 8201087498 87521 87522 87535 87536 87538 87539 87901 87906 9065590656 90657 90658 90660 90746 90875 90876 90889 90935 9094590947 90951 90952 90953 90954 90955 90956 90957 90958 9095990960 90961 90962 91110 91111 92286 92287 92613 92615 9261792973 93015 93016 93224 93227 93228 93229 93268 93272 9327993280 93281 93282 93283 93284 93285 93286 93287 93288 9328993290 93291 93292 93293 93294 93295 93297 93298 93351 93745
Texas Medicaid Special Bulletin, No. 5392013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
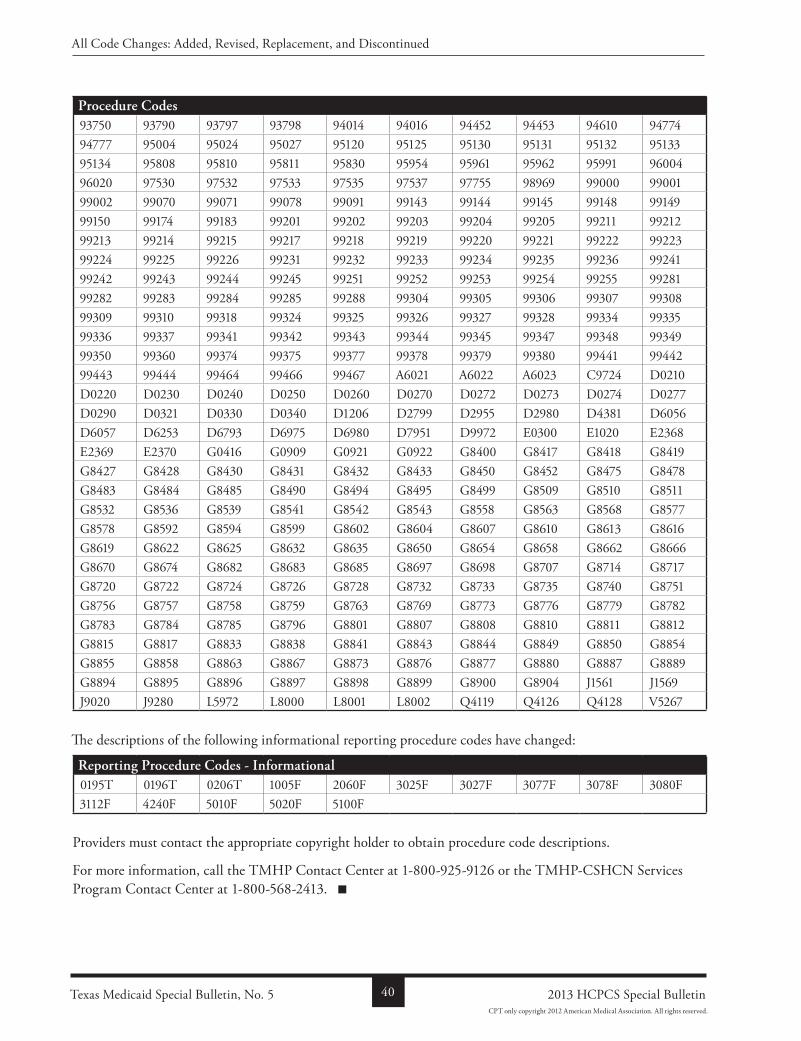
Procedure Codes93750 93790 93797 93798 94014 94016 94452 94453 94610 9477494777 95004 95024 95027 95120 95125 95130 95131 95132 9513395134 95808 95810 95811 95830 95954 95961 95962 95991 9600496020 97530 97532 97533 97535 97537 97755 98969 99000 9900199002 99070 99071 99078 99091 99143 99144 99145 99148 9914999150 99174 99183 99201 99202 99203 99204 99205 99211 9921299213 99214 99215 99217 99218 99219 99220 99221 99222 9922399224 99225 99226 99231 99232 99233 99234 99235 99236 9924199242 99243 99244 99245 99251 99252 99253 99254 99255 9928199282 99283 99284 99285 99288 99304 99305 99306 99307 9930899309 99310 99318 99324 99325 99326 99327 99328 99334 9933599336 99337 99341 99342 99343 99344 99345 99347 99348 9934999350 99360 99374 99375 99377 99378 99379 99380 99441 9944299443 99444 99464 99466 99467 A6021 A6022 A6023 C9724 D0210D0220 D0230 D0240 D0250 D0260 D0270 D0272 D0273 D0274 D0277D0290 D0321 D0330 D0340 D1206 D2799 D2955 D2980 D4381 D6056D6057 D6253 D6793 D6975 D6980 D7951 D9972 E0300 E1020 E2368E2369 E2370 G0416 G0909 G0921 G0922 G8400 G8417 G8418 G8419G8427 G8428 G8430 G8431 G8432 G8433 G8450 G8452 G8475 G8478G8483 G8484 G8485 G8490 G8494 G8495 G8499 G8509 G8510 G8511G8532 G8536 G8539 G8541 G8542 G8543 G8558 G8563 G8568 G8577G8578 G8592 G8594 G8599 G8602 G8604 G8607 G8610 G8613 G8616G8619 G8622 G8625 G8632 G8635 G8650 G8654 G8658 G8662 G8666G8670 G8674 G8682 G8683 G8685 G8697 G8698 G8707 G8714 G8717G8720 G8722 G8724 G8726 G8728 G8732 G8733 G8735 G8740 G8751G8756 G8757 G8758 G8759 G8763 G8769 G8773 G8776 G8779 G8782G8783 G8784 G8785 G8796 G8801 G8807 G8808 G8810 G8811 G8812G8815 G8817 G8833 G8838 G8841 G8843 G8844 G8849 G8850 G8854G8855 G8858 G8863 G8867 G8873 G8876 G8877 G8880 G8887 G8889G8894 G8895 G8896 G8897 G8898 G8899 G8900 G8904 J1561 J1569J9020 J9280 L5972 L8000 L8001 L8002 Q4119 Q4126 Q4128 V5267
The descriptions of the following informational reporting procedure codes have changed:
reporting Procedure Codes - Informational0195T 0196T 0206T 1005F 2060F 3025F 3027F 3077F 3078F 3080F3112F 4240F 5010F 5020F 5100F
Providers must contact the appropriate copyright holder to obtain procedure code descriptions.
For more information, call the TMHP Contact Center at 18009259126 or the TMHPCSHCN Services Program Contact Center at 18005682413.
Texas Medicaid Special Bulletin, No. 5 40 2013 HCPCS Special Bulletin
All Code Changes: Added, Revised, Replacement, and Discontinued
CPT only copyright 2012 American Medical Association. All rights reserved.
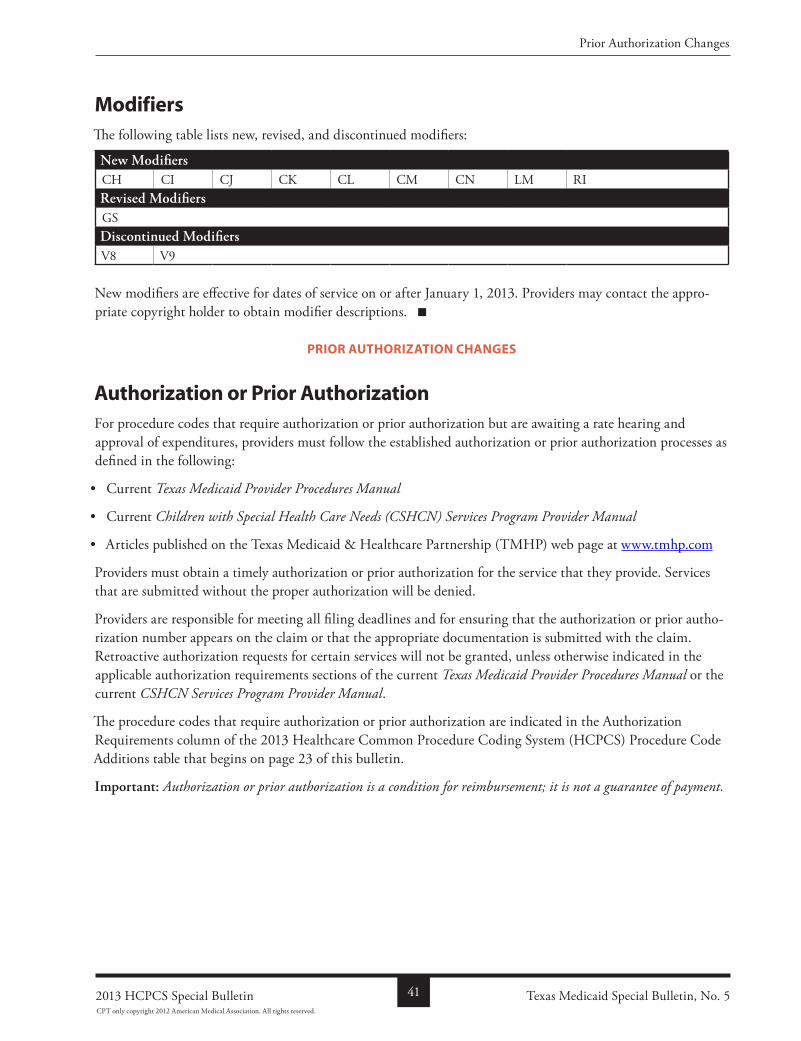
ModifiersThe following table lists new, revised, and discontinued modifiers:
new ModifiersCH CI CJ CK CL CM CN LM RIrevised ModifiersGSDiscontinued ModifiersV8 V9
New modifiers are effective for dates of service on or after January 1, 2013. Providers may contact the appropriate copyright holder to obtain modifier descriptions.
Prior authorization changeS
Authorization or Prior AuthorizationFor procedure codes that require authorization or prior authorization but are awaiting a rate hearing and approval of expenditures, providers must follow the established authorization or prior authorization processes as defined in the following:
• Current Texas Medicaid Provider Procedures Manual
• Current Children with Special Health Care Needs (CSHCN) Services Program Provider Manual
• Articles published on the Texas Medicaid & Healthcare Partnership (TMHP) web page at www.tmhp.com
Providers must obtain a timely authorization or prior authorization for the service that they provide. Services that are submitted without the proper authorization will be denied.
Providers are responsible for meeting all filing deadlines and for ensuring that the authorization or prior authorization number appears on the claim or that the appropriate documentation is submitted with the claim. Retroactive authorization requests for certain services will not be granted, unless otherwise indicated in the applicable authorization requirements sections of the current Texas Medicaid Provider Procedures Manual or the current CSHCN Services Program Provider Manual.
The procedure codes that require authorization or prior authorization are indicated in the Authorization Requirements column of the 2013 Healthcare Common Procedure Coding System (HCPCS) Procedure Code Additions table that begins on page 23 of this bulletin.
Important: Authorization or prior authorization is a condition for reimbursement; it is not a guarantee of payment.
Texas Medicaid Special Bulletin, No. 5412013 HCPCS Special Bulletin
Prior Authorization Changes
CPT only copyright 2012 American Medical Association. All rights reserved.
Texas Medicaid No. 5
Texas Medicaid 2013 Healthcare Common Procedure Coding System (HCPCS) Special Bulletin
Prior authorization updateProviders who have received prior authorization for any of the following 2013 HCPCS discontinued procedure codes for dates of service that occur on, after, or encompass January 1, 2013, must contact the TMHP Prior Authorization Department to update the procedure codes that are prior authorized for those services:
Discontinued Procedure Codes Prior authorization requirements37209 MC92982 CSHCN92984 CSHCND0360 MD, MC, CSHCND0362 MD, MC, CSHCND4271 CSHCHD6970 MD, MC, CSHCND6972 MD, MC, CSHCND6973 MD, MC, CSHCND6976 MD, MC, CSHCND6977 MD, MC, CSHCNG0291 MCS3820 MD, MCS3822 MD, MCS3823 MD, MCS3828 MD, MCS3829 MD, MCS3830 MD, MCS3831 MD, MCS3835 MD, MCMD = Prior authorization required for Texas Medicaid, MC = Managed care prior authorization required, CSHCN = Prior authorization required for the CSHCN Services Program.
For a list of Prior Authorization Department telephone numbers, providers may refer to the “TMHP Telephone and Address Guide” in the current Texas Medicaid Provider Procedures Manual, Vol. 1, (General Informa-tion), and TMHPCSHCN Services Program Contact Information” in the current CSHCN Services Program Provider Manual.