Embed Size (px)
Citation preview
DOI: 10.1542/peds.2009-1162B 2009;124;S265Pediatrics
Darren A. DeWalt and Ashley HinkLiterature
Health Literacy and Child Health Outcomes: A Systematic Review of the
http://pediatrics.aappublications.org/content/124/Supplement_3/S265.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from

Health Literacy and Child Health Outcomes: ASystematic Review of the Literature
abstractOBJECTIVES: To review the relationship between parent and child lit-eracy and child health outcomes and interventions designed to im-prove child health outcomes for children or parents with low literacyskills.
METHODS: We searched Medline and the Cumulative Index to Nursingand Allied Health Literature (CINAHL) for articles published from 1980through 2008 and included studies that reported original data, mea-sured literacy and�1 health outcome, and assessed the relationshipbetween literacy and health outcomes. Health outcomes includedhealth knowledge, health behaviors, use of health care resources, in-termediatemarkers of disease status, andmeasures of morbidity. Twoabstractors reviewed each study for inclusion. Included studies wereabstracted into evidence tables andwere assessed by using an 11-itemquality scale.
RESULTS: We reviewed 4182 new titles and abstracts published since2003. Fifty-eight articles were retained for full review, and 13 met theinclusion criteria. Eleven articles from the systematic review from 1980to 2003 met the inclusion criteria, giving us a total of 24 articles. Chil-dren with low literacy generally had worse health behaviors. Parentswith low literacy had less health knowledge and had behaviors thatwere less advantageous for their children’s health compared with par-ents with higher literacy. Children whose parents had low literacyoften had worse health outcomes, but we found mixed results for therelationship of literacy to the use of health care services. Interventionsfound that improving written materials can increase health knowl-edge, and combining good written materials with brief counseling canimprove behaviors including adherence. The average quality of thestudies was fair to good.
CONCLUSIONS: Child and parent literacy seems associated with im-portant health outcomes. Future research can help us understandunder what circumstances this relationship is causal, how literacy andhealth outcomes are related in noncausal pathways, the relative im-portance of parent and child literacy, and what interventions effec-tively reduce health literacy–related disparities. Pediatrics 2009;124:S265–S274
AUTHORS: Darren A. DeWalt, MD, MPH and Ashley Hink,MPH
Program on Health Literacy, Cecil G. Sheps Center for HealthServices Research, University of North Carolina, Chapel Hill,North Carolina
KEY WORDShealth literacy, literacy, health disparities, child healthoutcomes
ABBREVIATIONSREALM—Rapid Estimate of Adult Literacy in MedicineTOFHLA—Test of Functional Health Literacy in AdultsCINAHL—Cumulative Index to Nursing and Allied HealthLiterature
The views presented in this article are those of the authors, notthe organizations with which they are affiliated.
www.pediatrics.org/cgi/doi/10.1542/peds.2009-1162B
doi:10.1542/peds.2009-1162B
Accepted for publication Jul 20, 2009
Address correspondence to Darren A. DeWalt, MD, MPH, Cecil G.Sheps Center for Health Services Research, Program on HealthLiteracy, 5039 Old Clinic Building, CB 7110, Chapel Hill, NC 27599.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 3, November 2009 S265 by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from

Health literacy is recognized by the In-stitute of Medicine as a critical compo-nent of high-quality health care.1
Researchers have documented the re-lationship between low literacy skillsand worse health outcomes.2 Becauseof the strength of this relationship, andbecause large segments of most soci-eties have low literacy skills,3,4 manyprograms, including Healthy People2010,5 address the role of literacy orhealth literacy for improving popula-tion health. Research that assessesthe relationship between literacy andhealth outcomes and testing interven-tions to mitigate the effects of lowhealth literacy is becomingmuchmorecommon in the medical and publichealth literature.
In health care policy and research, theterm “health literacy” is often appliedto a set of skills that are required tofunction well in the health care or pub-lic health setting. Although a usefulconstruct, our ability to measurehealth literacy as a single variable islimited. Rather, research to date hasfocused mostly on reading ability as aproxy measure for health literacy.1,6–8
Some measures of reading ability usehealth care words or paragraphs thatcontain health-related content to as-sess research participants, but suchinstruments (such as the Rapid Esti-mate of Adult Literacy in Medicine[REALM] and Test of Functional HealthLiteracy in Adults [TOFHLA]) are highlycorrelated with generic reading testsand still focus on the skill of reading orinterpreting information rather than abroader set of functional skills.2 Thefull TOFHLA has some items related tomath skills, but they are few and arenot used in most studies. As such, thebody of research to date has reportedthe evaluation of the relationship be-tween reading ability and health. We donot raise this issue as a limitation ofcurrent research but, rather, to clarifyour understanding of health literacy.
To remind the reader that researchhas focused on reading ability, we willrefer to the exposure variable as liter-acy rather than the broader constructof health literacy.
The role of literacy in health care hasbeen less extensively studied for childhealth comparedwith adult health. In asystematic review of the literaturefrom 1980 to 2003, we found 44 articlesthat addressed the relationship be-tween literacy and health outcomesand 10 that addressed the effects onchild health outcomes.2 Most of thosestudies examined parental knowledgeas the outcome of interest. More re-cently, the authors of 2 review articlesdiscussed the role of health literacyin pediatric health care and pointedto the need for further developmentand understanding of this field ofresearch.9,10
In this article, we summarize the cur-rent evidence of the relationship be-tween literacy and child health out-comes, review interventions designedto mitigate the effects of low literacyon child health outcomes, and exposeareas of needed research.
METHODS
This systematic review is an extensionof the systematic reviewwe performedfor the Agency for Healthcare Re-search and Quality in 2004.8 For thisreview, we included articles pub-lished through September 2008 andfocused our attention on studies thatevaluated the role of child or parentliteracy and child health outcomes.
In this systematic review, we examinethe following key questions:
1. Are caregiver or child literacy skillsrelated to health outcomes?
2. What interventions have been stud-ied to improve health outcomes forchildren who have low literacy orwho have parents with low literacy,or to reduce disparities in health
outcomes associated with lowliteracy?
Inclusion and Exclusion Criteria
On the basis of the key questions, wegenerated a list of inclusion and exclu-sion criteria, which have been listed inprevious publications.2,11 Briefly, welimited studies to those with outcomesrelated to health and health servicesand that measured literacy skills witha valid instrument. We defined a validinstrument as one that had previouslybeen used in a published study or onethat compared with other publishedinstruments. Studies were not system-atically excluded if they measuredother aspects of literacy (writing or lis-tening). In contrast to our previous re-view, we only included studies thatevaluated child health outcomes.
To be included, studies had to (1) beconducted in a developed country (de-fined as the United States, Canada,Western Europe, Japan, Australia, orNew Zealand), (2) be published from1980 to 2008, (3) be written in English,(4) study �10 subjects, (5) measureliteracy directly among participants,(6) measure a child health outcome orcaregiver behavior directly related tochild health, and, if an intervention, (7)use a controlled or uncontrolled ex-perimental design and (8) measurethe effect of an intervention on at least1 health outcome. We defined eligiblehealth outcomes to be:
● health knowledge, assessed by anobjective scale;
● health behaviors;
● biochemical or biometric healthoutcomes with recognized rela-tionships to illnesses or healthconditions;
● measures of disease incidence, prev-alence, morbidity, and mortality;
● self-reported general health status;
● utilization of health services; and
● cost of care.
S266 DeWALT and HINK by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from
Literature Search
We used the articles identified in ourprevious systematic review, and the lit-erature search was well described inprevious publications.2,11 To update theliterature search to 2008, we per-formed a search for pediatrics articles(children aged 0–18 in PubMed) pub-lished from 2003 through 2008. For theupdated search, we searched for thekey words “literacy,” “WRAT,” “REALM,”“TOFHLA,” “numeracy,” “reading ability,”“reading skill,” “wide range achieve-ment,” “rapid estimate of adult,” and“test of functional health” in the titlesand abstracts of articles. We per-formed the search by using PubMedand the Cumulative Index to Nursingand Allied Health (CINAHL), becausethose databases identified 98% of thearticles for our previous systematicreview.2 A PubMed search was firstconducted by using each key word. Wedid not exclude duplicate referenceswith each key-word search. However,only unique articles were retainedfor full review for each search. Then,a CINAHL search excluding PubMedreferences was performed to find ad-ditional unique articles.
Article Selection and Review
One reviewer initially evaluated titlesand abstracts and excluded articlesthat did not measure literacy or ahealth outcome. All other articles wentto a full review by both authors. Dis-agreements were reconciled by dis-cussion. A reviewer (Ms Hink) entereddata from included articles into an ev-idence table, and the second re-viewer (Dr DeWalt) then examinedthe articles and edited the table en-tries for accuracy.
Evaluation of Quality and Strengthof Evidence
We graded each study according to theadequacy of study population, compa-rability of subjects across comparison
groups, validity and reliability of the lit-eracy measurement, maintenance ofcomparable groups, appropriatenessof the outcome measurement, appro-priateness of statistical analysis, andadequacy of control of confounding.8
We converted our quality ratings foreach item into numeric values (0 �poor, 1� fair, and 2� good) and cre-ated a composite rating for each study,giving each item equal weight; we ex-cluded items that were judged not ap-plicable on the basis of study design.We totaled the score for each evalua-tor and then averaged the results forapplicable elements.8 Although ourrating scale is based on previouslyused quality assessments, it should beinterpreted with caution because ithas not been validated.
RESULTS
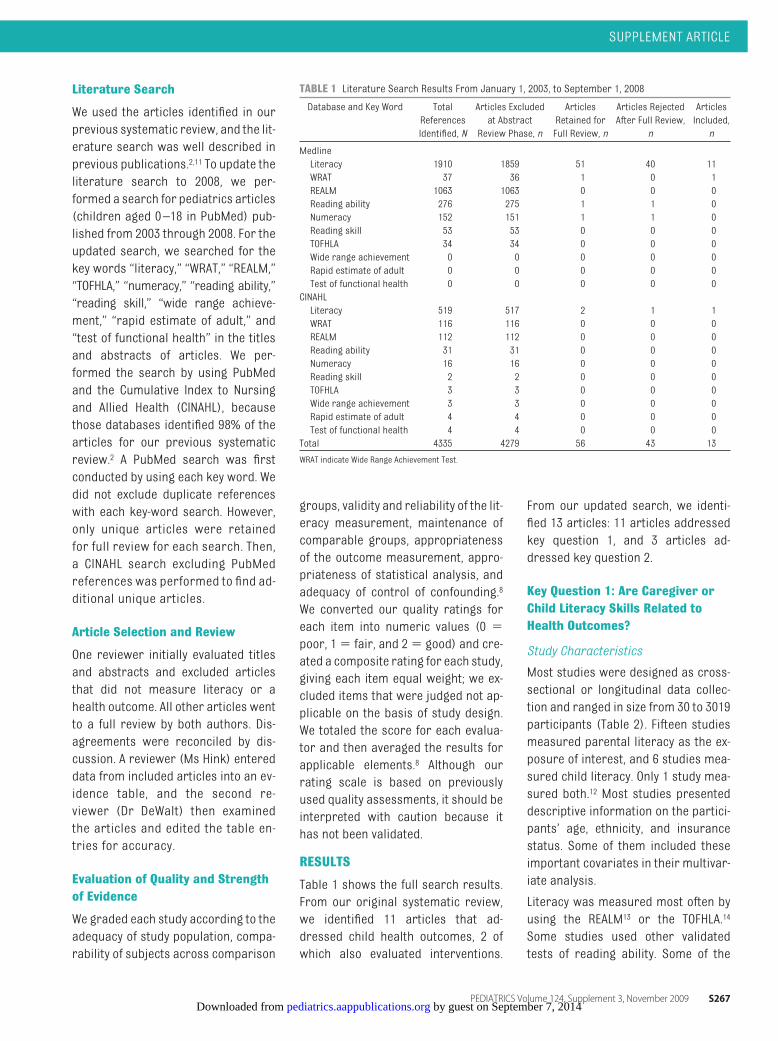
Table 1 shows the full search results.From our original systematic review,we identified 11 articles that ad-dressed child health outcomes, 2 ofwhich also evaluated interventions.
From our updated search, we identi-fied 13 articles: 11 articles addressedkey question 1, and 3 articles ad-dressed key question 2.
Key Question 1: Are Caregiver orChild Literacy Skills Related toHealth Outcomes?
Study Characteristics
Most studies were designed as cross-sectional or longitudinal data collec-tion and ranged in size from 30 to 3019participants (Table 2). Fifteen studiesmeasured parental literacy as the ex-posure of interest, and 6 studies mea-sured child literacy. Only 1 study mea-sured both.12 Most studies presenteddescriptive information on the partici-pants’ age, ethnicity, and insurancestatus. Some of them included theseimportant covariates in their multivar-iate analysis.
Literacy was measured most often byusing the REALM13 or the TOFHLA.14
Some studies used other validatedtests of reading ability. Some of the
TABLE 1 Literature Search Results From January 1, 2003, to September 1, 2008
Database and Key Word TotalReferencesIdentified, N
Articles Excludedat AbstractReview Phase, n
ArticlesRetained forFull Review, n
Articles RejectedAfter Full Review,
n
ArticlesIncluded,n
MedlineLiteracy 1910 1859 51 40 11WRAT 37 36 1 0 1REALM 1063 1063 0 0 0Reading ability 276 275 1 1 0Numeracy 152 151 1 1 0Reading skill 53 53 0 0 0TOFHLA 34 34 0 0 0Wide range achievement 0 0 0 0 0Rapid estimate of adult 0 0 0 0 0Test of functional health 0 0 0 0 0CINAHLLiteracy 519 517 2 1 1WRAT 116 116 0 0 0REALM 112 112 0 0 0Reading ability 31 31 0 0 0Numeracy 16 16 0 0 0Reading skill 2 2 0 0 0TOFHLA 3 3 0 0 0Wide range achievement 3 3 0 0 0Rapid estimate of adult 4 4 0 0 0Test of functional health 4 4 0 0 0Total 4335 4279 56 43 13
WRAT indicate Wide Range Achievement Test.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 3, November 2009 S267 by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from
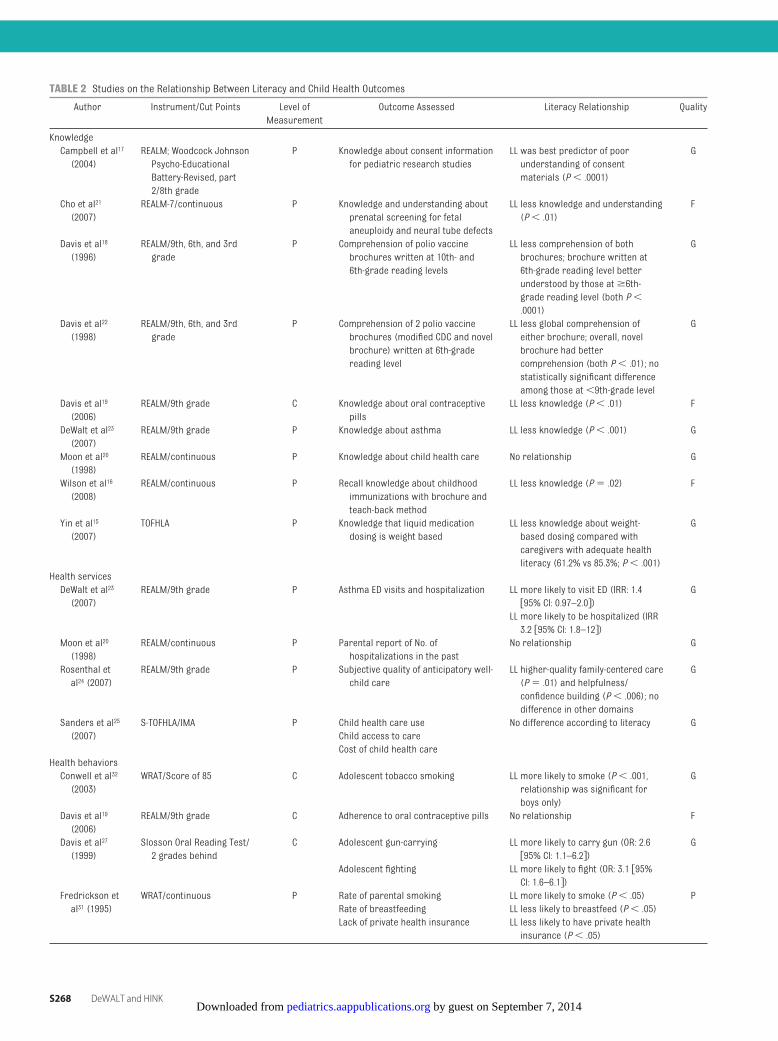
TABLE 2 Studies on the Relationship Between Literacy and Child Health Outcomes
Author Instrument/Cut Points Level ofMeasurement
Outcome Assessed Literacy Relationship Quality
KnowledgeCampbell et al17
(2004)REALM; Woodcock JohnsonPsycho-EducationalBattery-Revised, part2/8th grade
P Knowledge about consent informationfor pediatric research studies
LL was best predictor of poorunderstanding of consentmaterials (P� .0001)
G
Cho et al21
(2007)REALM-7/continuous P Knowledge and understanding about
prenatal screening for fetalaneuploidy and neural tube defects
LL less knowledge and understanding(P� .01)
F
Davis et al18
(1996)REALM/9th, 6th, and 3rdgrade
P Comprehension of polio vaccinebrochures written at 10th- and6th-grade reading levels
LL less comprehension of bothbrochures; brochure written at6th-grade reading level betterunderstood by those at�6th-grade reading level (both P�.0001)
G
Davis et al22
(1998)REALM/9th, 6th, and 3rdgrade
P Comprehension of 2 polio vaccinebrochures (modified CDC and novelbrochure) written at 6th-gradereading level
LL less global comprehension ofeither brochure; overall, novelbrochure had bettercomprehension (both P� .01); nostatistically significant differenceamong those at�9th-grade level
G
Davis et al19
(2006)REALM/9th grade C Knowledge about oral contraceptive
pillsLL less knowledge (P� .01) F
DeWalt et al23
(2007)REALM/9th grade P Knowledge about asthma LL less knowledge (P� .001) G
Moon et al20
(1998)REALM/continuous P Knowledge about child health care No relationship G
Wilson et al16
(2008)REALM/continuous P Recall knowledge about childhood
immunizations with brochure andteach-back method
LL less knowledge (P� .02) F
Yin et al15
(2007)TOFHLA P Knowledge that liquid medication
dosing is weight basedLL less knowledge about weight-based dosing compared withcaregivers with adequate healthliteracy (61.2% vs 85.3%; P� .001)
G
Health servicesDeWalt et al23
(2007)REALM/9th grade P Asthma ED visits and hospitalization LL more likely to visit ED (IRR: 1.4
�95% CI: 0.97–2.0�)G
LL more likely to be hospitalized (IRR3.2 �95% CI: 1.8–12�)
Moon et al20
(1998)REALM/continuous P Parental report of No. of
hospitalizations in the pastNo relationship G
Rosenthal etal24 (2007)
REALM/9th grade P Subjective quality of anticipatory well-child care
LL higher-quality family-centered care(P� .01) and helpfulness/confidence building (P� .006); nodifference in other domains
G
Sanders et al25
(2007)S-TOFHLA/IMA P Child health care use No difference according to literacy G
Child access to careCost of child health care
Health behaviorsConwell et al32
(2003)WRAT/Score of 85 C Adolescent tobacco smoking LL more likely to smoke (P� .001,
relationship was significant forboys only)
G
Davis et al19
(2006)REALM/9th grade C Adherence to oral contraceptive pills No relationship F
Davis et al27
(1999)Slosson Oral Reading Test/2 grades behind
C Adolescent gun-carrying LL more likely to carry gun (OR: 2.6�95% CI: 1.1–6.2�)
G
Adolescent fighting LL more likely to fight (OR: 3.1 �95%CI: 1.6–6.1�)
Fredrickson etal31 (1995)
WRAT/continuous P Rate of parental smoking LL more likely to smoke (P� .05) PRate of breastfeeding LL less likely to breastfeed (P� .05)Lack of private health insurance LL less likely to have private health
insurance (P� .05)
S268 DeWALT and HINK by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from
tests were based on health care wordsor phrases, and others were genericreading tests.
Relationship Between Literacy andKnowledge Outcomes
Nine studies measured the relationshipbetween literacy and knowledge regard-ing health outcomes, behaviors, or ser-vices (Table 2).15–23 Eight of these studiesexamined parental literacy as the expo-sure of interest, and all but one20 re-vealed that people with lower literacyhad less knowledge about health out-comes, behaviors, and health services.
Relationship Between Literacy andUse of Health Care Services
Four studies evaluated the relation-ship between literacy and use of health
care services.20,23–25 All studies were ofyoung children, and parental literacywas the exposure of interest. Onestudy showed that asthmatic childrenof parents with low literacy havehigher rates of hospitalizations andemergency department visits even af-ter controlling for potential confound-ing variables.23 The study by Sanders etal,25 which was not limited to 1 disease,did not find statistically significant re-lationships between literacy and pre-ventive care, emergency or hospitalcare, or cost. Moon et al20 did not find arelationship between literacy and pre-vious hospitalizations or number ofchronic diseases. In a qualitatively dif-ferent study of health services,Rosenthal et al24 found that parents
with low literacy were more likely thanthose with higher literacy to reportfamily-centered care, helpfulness, andconfidence building after an appoint-ment with a physician.
Relationship Between Literacy andHealth Behaviors
Nine studies evaluated the relationshipbetween literacy and health behav-iors.15,19,26–32 All studies analyzed behav-ior of the person whose literacy wasmeasured, and5 studiesmeasuredchildliteracy. Davis et al27 and Stanton et al30
both evaluated adolescent literacy andproblem behaviors including fightingand gun-carrying. After controlling forrace, gender, and age, Davis et al foundthat adolescents with lower literacy
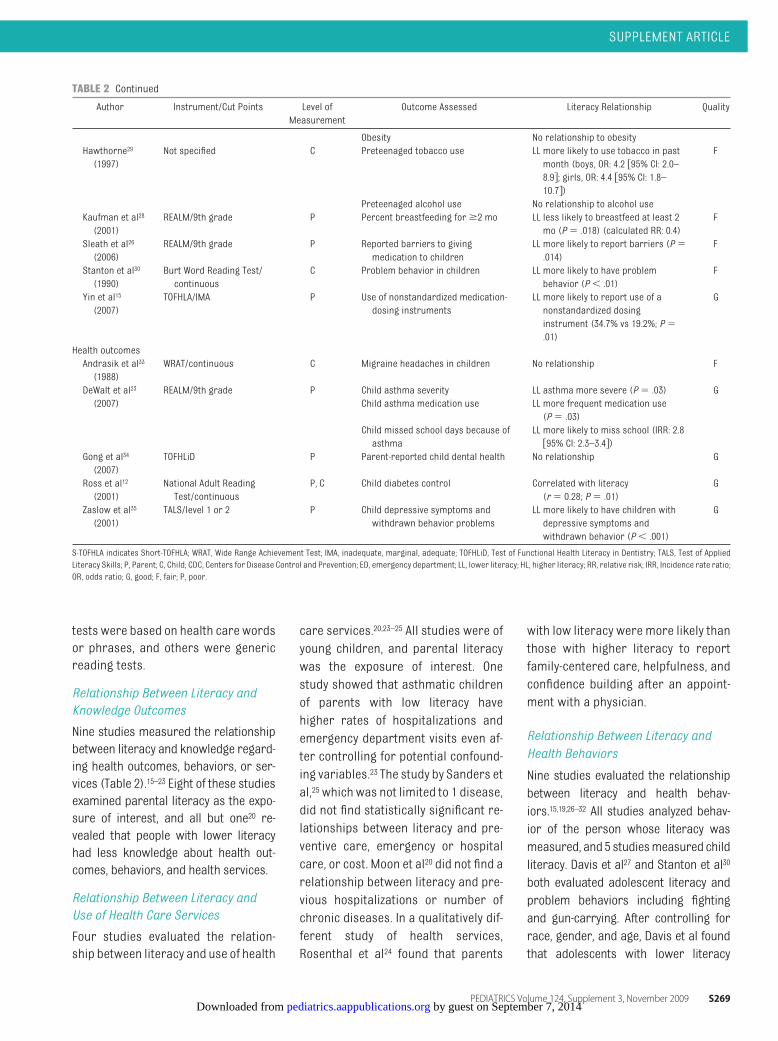
TABLE 2 Continued
Author Instrument/Cut Points Level ofMeasurement
Outcome Assessed Literacy Relationship Quality
Obesity No relationship to obesityHawthorne29
(1997)Not specified C Preteenaged tobacco use LL more likely to use tobacco in past
month (boys, OR: 4.2 �95% CI: 2.0–8.9�; girls, OR: 4.4 �95% CI: 1.8–10.7�)
F
Preteenaged alcohol use No relationship to alcohol useKaufman et al28
(2001)REALM/9th grade P Percent breastfeeding for�2 mo LL less likely to breastfeed at least 2
mo (P� .018) (calculated RR: 0.4)F
Sleath et al26
(2006)REALM/9th grade P Reported barriers to giving
medication to childrenLL more likely to report barriers (P�.014)
F
Stanton et al30
(1990)Burt Word Reading Test/continuous
C Problem behavior in children LL more likely to have problembehavior (P� .01)
F
Yin et al15
(2007)TOFHLA/IMA P Use of nonstandardized medication-
dosing instrumentsLL more likely to report use of anonstandardized dosinginstrument (34.7% vs 19.2%; P�.01)
G
Health outcomesAndrasik et al33
(1988)WRAT/continuous C Migraine headaches in children No relationship F
DeWalt et al23
(2007)REALM/9th grade P Child asthma severity LL asthma more severe (P� .03) G
Child asthma medication use LL more frequent medication use(P� .03)
Child missed school days because ofasthma
LL more likely to miss school (IRR: 2.8�95% CI: 2.3–3.4�)
Gong et al34
(2007)TOFHLiD P Parent-reported child dental health No relationship G
Ross et al12
(2001)National Adult ReadingTest/continuous
P, C Child diabetes control Correlated with literacy(r� 0.28; P� .01)
G
Zaslow et al35
(2001)TALS/level 1 or 2 P Child depressive symptoms and
withdrawn behavior problemsLL more likely to have children withdepressive symptoms andwithdrawn behavior (P� .001)
G
S-TOFHLA indicates Short-TOFHLA; WRAT, Wide Range Achievement Test; IMA, inadequate, marginal, adequate; TOFHLiD, Test of Functional Health Literacy in Dentistry; TALS, Test of AppliedLiteracy Skills; P, Parent; C, Child; CDC, Centers for Disease Control and Prevention; ED, emergency department; LL, lower literacy; HL, higher literacy; RR, relative risk; IRR, Incidence rate ratio;OR, odds ratio; G, good; F, fair; P, poor.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 3, November 2009 S269 by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from

were more likely to fight and carry gunsthan those with higher literacy. Stantonet al assessed regression models thatincluded variables for family adversity,early problem behavior, and school-ageIQ and found that literacy was most cor-related with problem behavior. Haw-thorne29 found that adolescents withlower literacy were more likely to usealcohol and tobacco than those withhigher literacy. Conwell et al32 found that14-year-olds with lower literacy weremore likely to smoke tobacco than thosewith higher literacy, although this find-ing was only significant among boys.Davis et al19 evaluated adherence to oralcontraceptive pills and found that onethird of the sample had missed 1 or 2pills in the previous 2weeks, butmissingthe pill was not related to literacy.
Four studies measured literacy andbehavior among parents or caregiv-ers.15,26,28,31 Yin et al15 found that caregiv-ers with low literacy were more likely touse a nonstandard dosing instrumentwhen administering liquidmedication toinfants. Kaufman et al28 found that moth-ers with low literacy were less likely tocontinue breastfeeding for �2 months.Sleath et al26 found that homelesswomen with low literacy were morelikely to report barriers for giving medi-cations to their children than homelesswomen with higher literacy.
Relationship Between Literacy andHealth Outcomes
Five studies attempted to examine therelationship between literacy andhealth outcomes.12,23,33–35 Two studiesmeasured child literacy and the out-come of interest.12,33 Andrasik et al33
found no relationship between literacyamong children and migraine head-aches. Ross et al12 found no relation-ship between child literacy and glyce-mic control among children aged 5 to17 years with diabetes, but it is inter-esting to note that they did find a rela-
tionship between maternal literacyand the child’s glycemic control.
Three studies measured only parentalliteracy and evaluated the child’shealth outcome. Zaslow et al35 evalu-ated maternal literacy, maternal de-pression, and children’s scores ondepressive/withdrawn measurementscales. Children of mothers with moredepressive symptoms had more de-pressive/withdrawn symptoms onlyin the presence of low maternal liter-acy. The positive interaction betweenmaternal literacy and depression onchild depressive symptoms indicatesthat literacy may be a mediating va-riable between parental and childhealth outcomes. Gong et al34 foundno relationship between parentalliteracy and parents’ reports of theirchild’s oral health. DeWalt et al23
found that children with parents whohave low literacy are more likely to havemoderate or severe persistent asthmaand miss more school days because ofasthma compared with children whoseparents have higher literacy.
Key Question 2: What InterventionsHave Been Studied to ImproveHealth Outcomes for Children WhoHave Low Literacy or Who HaveParents With Low Literacy, or toReduce Disparities in HealthOutcomes Associated With LowLiteracy?
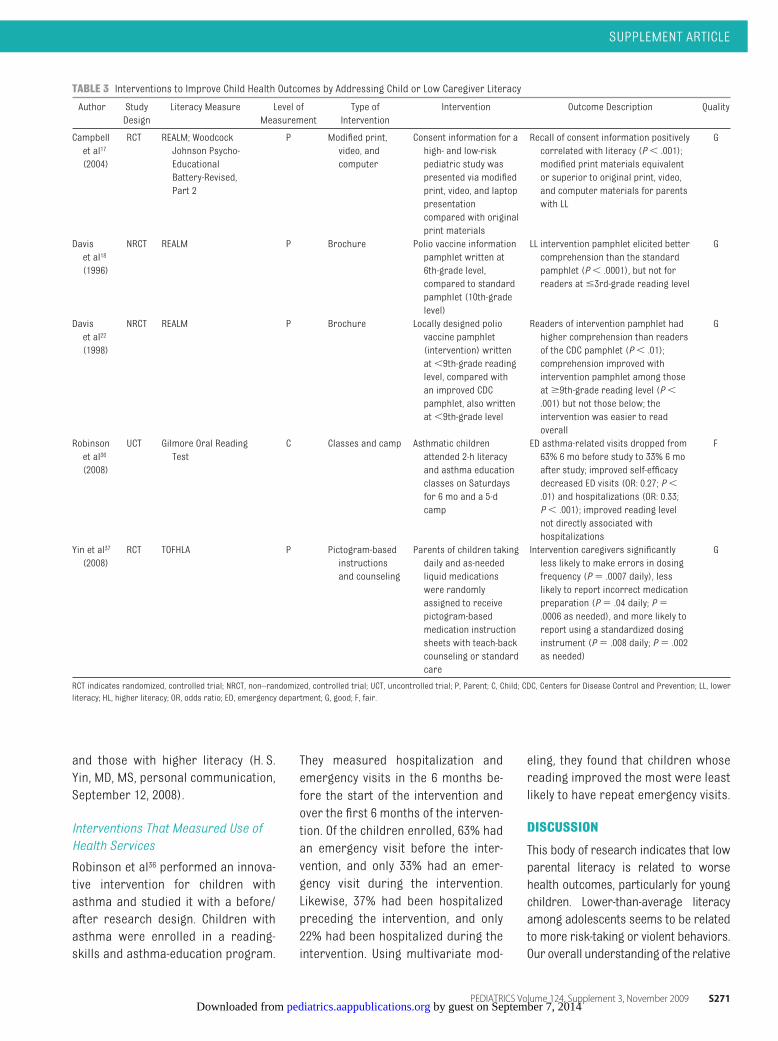
We identified 5 studies thatmeasured lit-eracy in the child or the parent and stud-ied the effect of an intervention onhealthoutcomes (Table 3).17,18,22,36,37 The inter-vention for4studieswas targeted for theparents, and all 4 studies were in thecontext of children younger than 5years.17,18,22,37 All 4 of those studies werecontrolled clinical trials,17,18,22,37 and 3stratified their results according toliteracy level.17,18,22One uncontrolledstudy targeted the intervention for thechildren (aged 6 to 14 years) them-selves.36
Interventions to ImproveHealth-Related Knowledge
Four studies measured knowledge as1 of the outcomes.17,18,22,37 Two studiesby Davis et al18,22 demonstrated thatwell-designed written materials canimprove comprehension across thecontinuum of reading ability, but thedisparity in comprehension betweengood and poor readers remainedabout the same.
Campbell et al17 evaluated the under-standing of informed consent by using4 different strategies for delivering in-formation: (1) original consent form;(2) enhanced easy-to-read consentform; (3) computer-based presenta-tion; and (4) video. Of the 4 methods,they found that the enhanced writtenmaterials were as effective as thevideo and computer-based materialsfor the total sample. In the subgroup ofparents who read below the 9th-gradelevel, the enhanced written materialswere generally superior to all othermethods.
Yin et al37 tested a pictogram-basedmedication-instruction sheet com-bined with brief counseling and teach-back sessions. Parents who receivedthe intervention had more knowledgeabout the medication and dose fre-quency compared with those in ausual-care control group.
Interventions to Improve HealthBehaviors
One study measured actual healthbehaviors; Yin et al37 measured parent-reported medication dosing and ob-served parents preparing a medica-tion dose. Parents in the interventiongroup were more likely to use the cor-rect dose. They also found that the par-ents in the intervention group hadgreater self-reported adherence to theprescribed medication regimen. Al-though not stated in the article, the au-thor confirmed that effect sizes weresimilar for parents with low literacy
S270 DeWALT and HINK by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from
and those with higher literacy (H. S.Yin, MD, MS, personal communication,September 12, 2008).
Interventions That Measured Use ofHealth Services
Robinson et al36 performed an innova-tive intervention for children withasthma and studied it with a before/after research design. Children withasthma were enrolled in a reading-skills and asthma-education program.
They measured hospitalization andemergency visits in the 6 months be-fore the start of the intervention andover the first 6 months of the interven-tion. Of the children enrolled, 63% hadan emergency visit before the inter-vention, and only 33% had an emer-gency visit during the intervention.Likewise, 37% had been hospitalizedpreceding the intervention, and only22% had been hospitalized during theintervention. Using multivariate mod-
eling, they found that children whosereading improved the most were leastlikely to have repeat emergency visits.
DISCUSSION
This body of research indicates that lowparental literacy is related to worsehealth outcomes, particularly for youngchildren. Lower-than-average literacyamong adolescents seems to be relatedto more risk-taking or violent behaviors.Our overall understanding of the relative
TABLE 3 Interventions to Improve Child Health Outcomes by Addressing Child or Low Caregiver Literacy
Author StudyDesign
Literacy Measure Level ofMeasurement
Type ofIntervention
Intervention Outcome Description Quality
Campbellet al17
(2004)
RCT REALM; WoodcockJohnson Psycho-EducationalBattery-Revised,Part 2
P Modified print,video, andcomputer
Consent information for ahigh- and low-riskpediatric study waspresented via modifiedprint, video, and laptoppresentationcompared with originalprint materials
Recall of consent information positivelycorrelated with literacy (P� .001);modified print materials equivalentor superior to original print, video,and computer materials for parentswith LL
G
Daviset al18
(1996)
NRCT REALM P Brochure Polio vaccine informationpamphlet written at6th-grade level,compared to standardpamphlet (10th-gradelevel)
LL intervention pamphlet elicited bettercomprehension than the standardpamphlet (P� .0001), but not forreaders at�3rd-grade reading level
G
Daviset al22
(1998)
NRCT REALM P Brochure Locally designed poliovaccine pamphlet(intervention) writtenat�9th-grade readinglevel, compared withan improved CDCpamphlet, also writtenat�9th-grade level
Readers of intervention pamphlet hadhigher comprehension than readersof the CDC pamphlet (P� .01);comprehension improved withintervention pamphlet among thoseat�9th-grade reading level (P�.001) but not those below; theintervention was easier to readoverall
G
Robinsonet al36
(2008)
UCT Gilmore Oral ReadingTest
C Classes and camp Asthmatic childrenattended 2-h literacyand asthma educationclasses on Saturdaysfor 6 mo and a 5-dcamp
ED asthma-related visits dropped from63% 6 mo before study to 33% 6 moafter study; improved self-efficacydecreased ED visits (OR: 0.27; P�.01) and hospitalizations (OR: 0.33;P� .001); improved reading levelnot directly associated withhospitalizations
F
Yin et al37
(2008)RCT TOFHLA P Pictogram-based
instructionsand counseling
Parents of children takingdaily and as-neededliquid medicationswere randomlyassigned to receivepictogram-basedmedication instructionsheets with teach-backcounseling or standardcare
Intervention caregivers significantlyless likely to make errors in dosingfrequency (P� .0007 daily), lesslikely to report incorrect medicationpreparation (P� .04 daily; P�.0006 as needed), and more likely toreport using a standardized dosinginstrument (P� .008 daily; P� .002as needed)
G
RCT indicates randomized, controlled trial; NRCT, non–randomized, controlled trial; UCT, uncontrolled trial; P, Parent; C, Child; CDC, Centers for Disease Control and Prevention; LL, lowerliteracy; HL, higher literacy; OR, odds ratio; ED, emergency department; G, good; F, fair.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 3, November 2009 S271 by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from

importanceofparental andchild literacyover the continuum of development isweak.
As observed in our previous systematicreview, health-related knowledge is al-most always associated with literacy. Al-thoughknowledge is oftennot closely as-sociated with health outcomes, health-behavior experts assert that all health-behavior theories assume adequateknowledge.38 As such, it is important tonot ignore this meaningful relationship.
Few studies have examined the impactof knowledge-related interventionsstratified according to literacy level.The studies that have done so have hadmixed results.11 In some cases, im-proved written materials were betterfor everyone but did not reduce thegap in knowledge between those withhigher literacy and those with lowerliteracy.18,22 The study by Campbell etal17 showed a greater effect of the en-hancedwrittenmaterials among thosewith the lowest literacy. Future studiesshould focus on the health informationthat is most closely related to behav-iors and outcomes when they evaluatechanges in knowledge from interven-tion. We often refer to this as the “needto know and need to do.”39 As in thestudy by Yin et al,37 measuring behav-iors closely related to knowledge is an-other advance in this type of research.
We did find that low literacy is associ-ated with a variety of adverse healthbehaviors among parents and adoles-cents. Many of the behaviors, such assmoking, violence, and lack of breast-feeding, are likely to have other soci-etal influences related to but not causedby low literacy. However, some behav-iors such as adherence, correct dosing,and ability to getmedicines could have amore direct link to the ability to read andunderstand health care–related instruc-tions. These relationships are still quiteunclear given the numerous studies thathave not found a relationship betweenliteracy and adherence.19,40 We may con-
clude that understanding what oneneeds to do is necessary, but not suffi-cient, for adherence to medical recom-mendations.
Fewer studies have evaluated the rela-tionship between caregiver or child liter-acy and health service use or health out-comes. Although most studies haveshown a relationship between parentalliteracyandchildhealthoutcomes, somehave presented negative findings, whichprevents us from drawing firm conclu-sions. Although DeWalt et al23 found thatchildren with asthma who have parentswith low literacy skills had higher inci-dence of emergency department visits,hospitalizations, and missed schooldays, Sanders et al,25 who studied abroader sample of children, did not finda relationship between parental literacyand children’s health service. Moon etal20 also did not find more hospitaliza-tions or chronic illnesses for childrenwhose parents had lower literacy. Thesefindings suggest that not all situationslead to health literacy–related dispari-ties, and research is needed to enhanceour understanding of those situationsthatmay respond to literacy-sensitive in-terventions.
One of the most challenging aspects ofstudying the role of literacy or healthliteracy for children’s health is takinginto account the relative responsibilityof the parent and the child for thechild’s health outcome. Maturationalcognitive abilities may affect a child’sability to understand and implementself-care.41 Moreover, children dem-onstrate variations in their ability toengage in self-care within the sameage group, and parents use differentcues to determine the child’s readi-ness to assume self-care.42–44 Childma-turity, initiation of self-care activities,self-concept, family support and orga-nization, shared decision-making withmedical providers, maternal self-efficacy, duration of disease, the per-ceived disease knowledge of the child,
child academic achievement, and par-ticipation in outside activities havebeen found to influence the transfer ofmedical care activities from parent tochild.45–49 Parents of children withchronic medical needs often transferself-care responsibilities when theirchild is between the ages of 11 and 15years.49,50 Oftentimes adolescents donot implement the necessary level ofself-care activities when the transferof care occurs, which results in poorerhealth outcomes.45,51 Parent or child lit-eracy may also influence the transferof care. We suggest that studies exam-ining the role of literacy in childhoodhealth outcomes focus on parental liter-acy among children younger than 7years and child literacy for children intheir late teenage years. When studyingchildren between those ages, it would beworthwhile to measure both parent andchild literacy to determine their degreeof association tohealthoutcomesduringthe “transition” years. Of course, theseages are approximate and will vary onthebasisof thehealthbehaviorsandout-comes under study.
We found relatively few studies of in-terventions to improve child healthoutcomes for children or parents withlow literacy. Most studies have demon-strated improving knowledge. One studyimproved important health behaviors(giving the correct medication dose andcompleting the regimen).37 The studiesby Yin et al37 and Davis et al18,22 demon-strated improvement across all levels ofliteracy but not a reduction in the dispar-ity between parents with low and higherliteracy.Weareparticularly interested inthose that could narrow the gap in out-comes between low and higher literacy,but fewstudies in adult health havedem-onstrated such effects,52,53 and no stud-ies in child health have done so thus far.
From this relatively small number ofstudies, it is difficult to draw conclu-sions about the cause-and-effect rela-tionship between literacy and child
S272 DeWALT and HINK by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from

health outcomes. Although there is astrong relationship between literacyand the measured outcome, particu-larly knowledge, the nonexperimentalnature of the study designs leaves uswondering whether important otherfactors explain the relationship be-tween literacy and the outcome. Manystudies attempted to adjust for age, so-cioeconomic status, race/ethnicity,and insurance status, but such statis-tical adjustment does not ensure de-tection of a causal relationship. Inter-vention studies that target the effectsof low literacy and find a reduction inthe relationship between literacy andthe outcome could help to increase ourconfidence that the literacy-outcomerelationship is causal.
Our findings reflect the quality of thepublished literature. Most studieswere cross-sectional design, andmanydid not control for important covari-ates in the analysis. By limiting our in-clusion to the published English-language literature and to studies thathave measured literacy in the popula-tion of interest, we may have excludedsome interventions that could be effec-tive for patients or caregivers with lowliteracy skills. However, exclusion ofthose studies was necessary, because
literacy measurement was required toanswer questions about the role of lit-eracy. Our ratings of quality are ap-proximate and meant to address theability of the study to answer our ques-tions of interest. Some studies mayhave been focused on other questionsfor which they are “good” but had“fair” data related to the relationshipbetween literacy and health. Finally, itis important to recognize that the cur-rent research literature documents therelationship between reading ability andhealth outcomes rather than thebroader construct of health literacy.
Some view the fact that health literacymeasures do not address every possi-ble facet of health literacy as a limita-tion, but we do not hold that opinion.This body of research has identified animportant measured variable that pre-dicts disparities in health outcomes.This variable, mostly reading ability forprose and documents, may lend itselfvery well as a target for interventions,as demonstrated in this review and re-search in adults.11,52–54 Efforts to mea-sure health literacy broadly may iden-tify other areas to target forintervention, but that should not pre-vent us from pursuing interventionsthat mitigate this important disparity.
This review has important implica-tions for researchers and practitio-ners who are interested in childhealth. Practitioners should considerthe role of literacy and use interven-tions such as those described by Yin etal,37 Robinson et al,36 Campbell et al,17
and Davis et al,18,22 which can improvehealth behaviors and health outcomes.
CONCLUSIONS
Researchers should seize on theemerging recognition of the impor-tance of literacy for child health out-comes. We need to expand our under-standing of the relative roles ofcaregiver and child literacy. Studies toidentify the key health literacy skillsneeded by children as they transitionto self-management can lead to bettercurricula for clinician training and pri-mary and secondary schools. We needa better understanding of the relation-ship between knowledge and behav-iors so that our interventions can af-fect behaviors that are most closelyassociated with positive health out-comes. Finally, interventions shouldimprove outcomes for all patients butalso narrow the gap in outcomes be-tween people with low and higherliteracy.
REFERENCES
1. Nielsen-Bohlman L, Panzer AM, Kindig DA;Committee onHealth Literacy.Health Literacy:A Prescription to End Confusion. Washington,DC: National Academies Press; 2004
2. DeWalt DA, BerkmanND, Sheridan SL, Lohr KN,Pignone M. Literacy and health outcomes: asystematic review of the literature. J Gen In-tern Med. 2004;19(12):1228–1239
3. Kirsch I. The International Adult Literacy Sur-vey (IALS): Understanding What Was Mea-sured. Princeton, NJ: Educational TestingServices; 2001
4. Kutner M, Greenberg E, Baer J. A First Look atthe Literacy of America’s Adults in the 21stCentury. Baltimore, MD: US Department ofEducation; 2005. NCES report No. 2006–470
5. US Department of Health and Human Ser-vices.Healthy People 2010. 2nd ed. Washing-ton, DC: Government Printing Office; 2000
6. DeWalt DA, Pignone MP. Reading is funda-mental: the relationship between literacy andhealth. Arch Intern Med. 2005;165(17):1943–1944
7. Schwartzberg JG, VanGeest JB, Wang CC, eds.Understanding Health Literacy: Implicationsfor Medicine and Public Health. Chicago, IL:AMA Press; 2005
8. Berkman ND, DeWalt DA, Pignone MP, et al.Literacy and Health Outcomes. Rockville, MD:RTI International-University of North CarolinaEvidence-Based Practice Center; 2004
9. Sanders LM, Federico S, Klass P, AbramsMA, Dreyer B. Literacy and child health: asystematic review. Arch Pediatr AdolescMed. 2009;163(2):131–140
10. Yin HS, Forbis SG, Dreyer BP. Health literacyand pediatric health. Curr Probl Pediatr Ado-lesc Health Care. 2007;37(7):258–286
11. Pignone M, DeWalt DA, Sheridan S, BerkmanN, Lohr KN. Interventions to improve healthoutcomes for patients with low literacy: asystematic review. J Gen Intern Med. 2005;20(2):185–192
12. Ross LA, Frier BM, Kelnar CJ, Deary IJ. Childand parental mental ability and glycaemiccontrol in children with type 1 diabetes. Dia-bet Med. 2001;18(5):364–369
13. Davis TC, Long SW, Jackson RH, et al. RapidEstimate of Adult Literacy in Medicine: ashortened screening instrument. Fam Med.1993;25(6):391–395
14. Parker RM, Baker DW, Williams MV, NurssJR. The Test of Functional Health Literacy inAdults: a new instrument for measuring pa-tients’ literacy skills. J Gen InternMed. 1995;10(10):537–541
15. Yin HS, Dreyer BP, Foltin G, van Schaick L,
SUPPLEMENT ARTICLE
PEDIATRICS Volume 124, Supplement 3, November 2009 S273 by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from

Mendelsohn AL. Association of low care-giver health literacy with reported use ofnonstandardized dosing instruments andlack of knowledge of weight-based dosing.Ambul Pediatr. 2007;7(4):292–298
16. Wilson FL, Baker LM, Nordstrom CK, Leg-wand C. Using the teach-back and Orem’sSelf-care Deficit Nursing theory to increasechildhood immunization communicationamong low-income mothers. Issues ComprPediatr Nurs. 2008;31(1):7–22
17. Campbell FA, Goldman BD, Boccia ML, Skin-ner M. The effect of format modificationsand reading comprehension on recall of in-formed consent information by low-incomeparents: a comparison of print, video, andcomputer-based presentations. PatientEduc Couns. 2004;53(2):205–216
18. Davis TC, Bocchini JA Jr, Fredrickson D, et al.Parent comprehension of polio vaccine in-formation pamphlets. Pediatrics. 1996;97(6pt 1):804–810
19. Davis TC, Fredrickson DD, Potter L, et al. Pa-tient understanding and use of oral contra-ceptive pills in a southern public healthfamily planning clinic. South Med J. 2006;99(7):713–718
20. Moon RY, Cheng TL, Patel KM, Baumhaft K,Scheidt PC. Parental literacy level and un-derstanding of medical information. Pediat-rics. 1998;102(2). Available at: www.pediatrics.org/cgi/content/full/102/2/e25
21. Cho RN, Plunkett BA, Wolf MS, Simon CE,GrobmanWA. Health literacy and patient un-derstanding of screening tests for aneu-ploidy and neural tube defects. PrenatDiagn. 2007;27(5):463–467
22. Davis TC, Fredrickson DD, Arnold C, MurphyPW, Herbst M, Bocchini JA. A polio immuni-zation pamphlet with increased appeal andsimplified language does not improve com-prehension to an acceptable level. PatientEduc Couns. 1998;33(1):25–37
23. DeWalt DA, Dilling MH, Rosenthal MS, Pig-none MP. Low parental literacy is associ-ated with worse asthma care measures inchildren. Ambul Pediatr. 2007;7(1):25–31
24. Rosenthal MS, Socolar RR, DeWalt DA, Pig-noneM, Garrett J, Margolis PA. Parents withlow literacy report higher quality of parent-provider relationships in a residency clinic.Ambul Pediatr. 2007;7(1):51–55
25. Sanders LM, Thompson VT, Wilkinson JD.Caregiver health literacy and the use ofchild health services. Pediatrics. 2007;119(1). Available at: www.pediatrics.org/cgi/content/full/119/1/e86
26. SleathBL, JacksonE, ThomasKC, et al. Literacyand perceived barriers to medication taking
among homeless mothers and their children.Am J Health Syst Pharm. 2006;63(4):346–351
27. Davis TC, Byrd RS, Arnold CL, Auinger P, Boc-chini JAJ. Low literacy and violence amongad-olescents inasummersportsprogram.JAdo-lesc Health. 1999;24(6):403–411
28. Kaufman H, Skipper B, Small L, Terry T,McGrewM. Effect of literacy on breast-feedingoutcomes. South Med J. 2001;94(3):293–296
29. Hawthorne G. Preteenage drug use inAustralia: the key predictors and school-based drug education. J Adolesc Health. 1997;20(5):384–395
30. Stanton WR, Feehan M, McGee R, Silva PA. Therelative value of reading ability and IQ as pre-dictors of teacher-reported behavior prob-lems. J Learn Disabil. 1990;23(8):514–517
31. FredricksonDD,WashingtonRL, PhamN, Jack-son T, Wiltshire J, Jecha LD. Reading gradelevels andhealth behaviors of parents at childclinics. Kans Med. 1995;96(3):127–129
32. Conwell LS, O’Callaghan MJ, Andersen MJ,Bor W, Najman JM, Williams GM. Early ado-lescent smoking and a web of personal andsocial disadvantage. J Paediatr ChildHealth. 2003;39(8):580–585
33. Andrasik F, Kabela E, Quinn S, Attanasio V,Blanchard EB, Rosenblum EL. Psychologicalfunctioning of children who have recurrentmigraine. Pain. 1988;34(1):43–52
34. Gong DA, Lee JY, Rozier RG, Pahel BT, Rich-man JA, Vann WF Jr. Development and test-ing of the Test of Functional Health Literacyin Dentistry (TOFHLiD). J Public Health Dent.2007;67(2):105–112
35. Zaslow MJ, Hair EC, Dion MR, Ahluwalia SK,Sargent J. Maternal depressive symptomsand low literacy as potential barriers to em-ployment in a sample of families receivingwelfare: are there two-generational implica-tions?Women Health. 2001;32(3):211–251
36. Robinson LD Jr, Calmes DP, Bazargan M. Theimpact of literacy enhancement on asthma-related outcomes among underserved chil-dren. J Natl Med Assoc. 2008;100(8):892–896
37. Yin HS, Dreyer BP, van Schaick L, Foltin GL, Din-glas C, Mendelsohn AL. Randomized con-trolled trial of a pictogram-based interventionto reduce liquidmedicationdosingerrorsandimprove adherence among caregivers ofyoung children. Arch Pediatr Adolesc Med.2008;162(9):814–822
38. Bandura A. Self-efficacy: The Exercise of Con-trol. NewYork, NY:WH FreemanandCompany;1997
39. Seligman HK, Wallace AS, DeWalt DA, et al. De-veloping low-literacy patient educational ma-terials to facilitate behavior change. Am JHealth Behav. 2007;31(suppl 1):S69–S78
40. Pignone MP, DeWalt DA. Literacy and healthoutcomes: is adherence the missing link?J Gen Intern Med. 2006;21(8):896–897
41. Piaget J. The Origins of Intelligence in Chil-dren. New York, NY: International Universi-ties Press, Inc; 1952
42. Saucier CP. Self concept and self-care man-agement in school-age children with diabe-tes. Pediatr Nurs. 1984;10(2):135–138
43. Moore JB. Predictors of children’s self-careperformance: testing the theory of self-caredeficit.Sch InqNurs Pract. 1993;7(3):199–212;discussion 213–217
44. Moore JB, Mosher RB. Adjustment responsesof children and their mothers to cancer: self-care and anxiety. Oncol Nurs Forum. 1997;24(3):519–525
45. Ingersoll GM, Orr DP, Herrold AJ, Golden MP.Cognitive maturity and self-managementamongadolescentswith insulin-dependentdi-abetes mellitus. J Pediatr. 1986;108(4):620–623
46. Buford TA. Transfer of asthmamanagementresponsibility from parents to their school-age children. J Pediatr Nurs. 2004;19(1):3–12
47. Faulkner MS. Family responses to childrenwith diabetes and their influence on self-care. J Pediatr Nurs. 1996;11(2):82–93
48. Follansbee DS. Assuming responsibility fordiabetes management: what age? Whatprice? Diabetes Educ. 1989;15(4):347–353
49. Giordano BP, Petrila A, Banion CR, Neuen-kirchen G. The challenge of transferring re-sponsibility for diabetes management fromparent to child. J Pediatr Health Care. 1992;6(5 pt 1):235–239
50. Schilling LS, Knafl KA, Grey M. Changing pat-terns of self-management in youth with typeI diabetes. J Pediatr Nurs. 2006;21(6):412–424
51. Wysocki T, Taylor A, Hough BS, Linscheid TR,Yeates KO, Naglieri JA. Deviation from devel-opmenta l l y appropr ia te se l f - careautonomy: association with diabetes out-comes. Diabetes Care. 1996;19(2):119–125
52. Rothman R, DeWalt DA, Malone R, et al. Theinfluence of patient literacy on the effective-ness of a primary-care based diabetes dis-ease management program. JAMA. 2004;292(14):1711–1716
53. Paasche-Orlow MK, Riekert KA, BilderbackA, et al. Tailored education may reducehealth literacy disparities in asthma self-management. Am J Respir Crit Care Med.2005;172(8):980–986
54. Dewalt DA, Malone RM, Bryant ME, et al. Aheart failure self-management program forpatients of all literacy levels: a randomized,controlled trial [ISRCTN11535170]. BMCHealth Serv Res. 2006;6(1):30
S274 DeWALT and HINK by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2009-1162B 2009;124;S265Pediatrics
Darren A. DeWalt and Ashley HinkLiterature
Health Literacy and Child Health Outcomes: A Systematic Review of the
ServicesUpdated Information &
_3/S265.full.htmlhttp://pediatrics.aappublications.org/content/124/Supplementincluding high resolution figures, can be found at:
References
_3/S265.full.html#ref-list-1http://pediatrics.aappublications.org/content/124/Supplementat:This article cites 44 articles, 5 of which can be accessed free
Citations
_3/S265.full.html#related-urlshttp://pediatrics.aappublications.org/content/124/SupplementThis article has been cited by 18 HighWire-hosted articles:
Subspecialty Collections
y_pediatrics_subhttp://pediatrics.aappublications.org/cgi/collection/communitCommunity Pediatricsthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on September 7, 2014pediatrics.aappublications.orgDownloaded from