Embed Size (px)
Citation preview
Jackie L. Clark
School of Behavioral & BrainSciences, University of Texas atDallas, Callier Center, Dallas, USAUniversity of the Witwatersrand,Johannesburg, South Africa
Key WordsMozambique
Developing countries
Hearing loss
Demographics
Philanthropy
Hearing screening program
Transient otoacoustic emissions
Pure tone audiometry
AbbreviationsEAC: External auditory canal
OME: Otitis media with effusion
TEOAE: Transient evoked
otoacoustic emission
Original Article
International Journal of Audiology 2008; 47 (Suppl. 1):S49�S56
Hearing loss in Mozambique: Current data
from Inhambane Province
AbstractMozambique is a developing African country recuperat-ing from a lengthy civil war. As a result, documenting theincidence of hearing loss has remained a low priority.This paper provides results from work being carried outby the Mozambique Audiology Program (MAP), which isa philanthropic effort established in 1997 to introduceaudiology services and identify auditory disorders in thecountry. Some decades before the MAP, another programreported extremely high incidence rates of otitis media in1000 primary school students in the capital city ofMaputo. This paper presents the MAP results frommass hearing screenings conducted over a two year periodon a cohort group of 2685 students ranging in age from3�18 years at a preschool and primary school in Chicuqueand Maxixe, Mozambique. This current study showed aprevalence of 5% of the total 2685 students across ageswith varying degrees of hearing loss resulting frommultiple etiologies. External auditory canal obstructionwas the greatest otoscopic abnormality (regardless ofage), followed by severely limited tympanic membranemobility (i.e. flat tympanogram) in the absence of EACobstruction in those students identified with hearing loss.Of the 145 student identified with hearing loss, there were27 found to have active drainage. Some of the benefits ofconducting mass hearing screening in this population arediscussed.
SumarioMozambique es un paıs africano en desarrollo que estarecuperandose de una prolongada guerra civil. Comoresultado, la documentacion de la incidencia de lasperdidas auditivas ha constituido una baja prioridad.Este trabajo aporta resultados de una labor llevada a cabopor el Programa de Audiologıa de Mozambique (MAP),que es un esfuerzo filantropico establecido en 1997 paraintroducir servicios audiologicos e identificar trastornosauditivos en el paıs. Algunas decadas antes del MAP, otroprograma reporto tasas extremadamente altas de otitismedia en 1000 estudiantes de escuela primaria, en laciudad capital: Maputo. Este trabajo presenta los resulta-dos del MAP a partir del tamiz auditivo masivo conducidodurante un perıodo de dos anos con una cohorte de 2.685estudiantes, con edades entre 3�18 anos, en un centroescolar y pre-escolar en Chicuque y Maxixe, Mozambique.Este estudio mostro una prevalencia de 5% en un total de2.685 estudiantes, de todas las edades y con gradosvariables de hipoacusia, como resultado de multiplesetiologıas. La obstruccion del conducto auditivo externofue la anormalidad otoscopica mayor (sin importar laedad), seguida de movilidades timpanicas severamentelimitadas (p.e., timpanogramas planos) en ausencia deobstruccion del CAE, en aquellos estudiantes identifica-dos con hipoacusia. De los 145 estudiantes identificadoscon hipoacusia, se encontro que 27 tenıa supuracionactiva. Se discuten algunos de los beneficios de conducirprogramas masivos de identificacion auditiva.
There is a paucity of quality data describing the epidemiology of
hearing impairment in African countries, especially in children.
Oftentimes children in this population are identified as ‘deaf’
when they exhibit great difficulty understanding speech or when
they begin school. According to 2005 estimates by the World
Health Organization (WHO), 278 million people worldwide have
moderate to profound hearing loss in both ears, with an
estimated 80% of those deaf and hearing-impaired people living
in developing and medium developing countries. Out of the
718 000� annual new live births worldwide, it is estimated that
approximately 90% are born in developing countries (Olusanya
& Newton, 2007). Preventable hearing loss continues to be an
important public health consideration, especially in the devel-
oping countries, with chronic middle-ear infection frequently
cited as the cause of much of the mild to moderate reversible
hearing impairment in children (Okeowo, 1985). With the
growing global population coupled with longer life expectancies,
the number of people worldwide with all levels of hearing
impairment is on the rise. In comparison to other parts of the
world, the available data about incidence of hearing loss in
African countries is severely limited (WHO, 1995).
A workshop organized in 1995 by the WHO Regional Office
for Africa was conducted to review available data on the
magnitude and main causes of hearing impairment in 15 African
countries and to consider appropriate strategies for the preven-
tion of hearing impairment. It was estimated that the population
of Africa is 12% of the world, and consequently at the time of
the workshop, there were probably 14.4 million people with
disabling hearing impairment in Africa. The first known reports
detailing the incidence of hearing loss in many African countries
were presented at the WHO workshop which took place in
Nairobi, Kenya. All country representatives, including those
from Mozambique indicated that chronic otitis media and
ototoxicity were considered the two most prevalent causes of
hearing impairment in their population. Results of hearing
evaluation in the capital city of Maputo from 1000 primary
school aged children (5�16 years old) in 1995 were reported at
the conference. Of the 1000 children evaluated, 18.6% presented
with otitis media, and a total of 5% of the children exhibited
otitis media and hearing impairment. Unfortunately, the report
provided neither information on the cut-off values by audio-
metric intensity nor the type of hearing impairment observed.
ISSN 1499-2027 print/ISSN 1708-8186 onlineDOI: 10.1080/14992020802291723# 2008 British Society of Audiology, InternationalSociety of Audiology, and Nordic Audiological Society
Jackie L. ClarkSchool of Behavioral & Brain Sciences, University of Texas at Dallas; Callier Center,1966 Inwood Road, Dallas, TX 75235, USA.E-mail: [email protected]
Received:June 3, 2008Accepted:June 23, 2008
Int J
Aud
iol 2
008.
47:S
49-S
56.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
thea
ster
n U
nive
rsity
on
10/2
6/14
. For
per
sona
l use
onl
y.
Located just east of Swaziland and South Africa, the Republic
of Mozambique is a country bordered by the Indian Ocean to
the east, Tanzania to the north, and Malawi and Zambia to the
northeast. As a developing country that is still recuperating from
decades-long civil war and a population of almost 21 million
that increases 2.4% annually, the World Health Organization
2008 statistics show Mozambique currently has a life expectancy
of 40 years, 38.7% adult literacy, with a 70�80% net primary
school enrollment; a little more than one third of the population
exists on less than $1/day. Not surprisingly, determination of the
incidence of hearing loss has remained a low priority in
Mozambique. Currently there is 1 physician per 10 000 popula-
tion and 1659 associated health-care workers in the entire
country of Mozambique.
Beginning in 1997, the Mozambique Audiology Program
(MAP) was established to introduce audiology services into
Mozambique. Prior to some of the MAP training, social action
workers would be directed by word of mouth to children in the
community who exhibited hearing difficulties, whereupon a
battery of various noise makers (i.e. keys jangling, pots banging,
etc) were utilized to identify and refer candidates to attend the
provincial classroom (Maxixe Primary School) that was
equipped with a teacher trained in Mozambique and Portuguese
sign language. Since then, MAP has initiated and maintained
multiple focuses that included instructing a number of hospital
based Medical ‘Technicals’ (as termed by the Health Ministry)
regarding aspects such as: anatomy and physiology of the
hearing mechanism; efficacy of hearing evaluations; training to
conduct hearing and immittance screenings; training to conduct
diagnostic audiology with immittance measures; and training to
evaluate the electroacoustic status of hearing aids. Additionally,
the program initiated a free hearing clinic in which the local
Medical Technicals might participate in a large scale community
hearing screening, encompassing diagnostic audiometric evalua-
tion and hearing aid dispensing or medical referral as needed. In
preparation for the eventual large scale hearing screening
program, an otoscopic survey was conducted in 2004 on 1518
primary school student’s ears (ages 8�14 years) by trained
individuals. The findings of the initial survey suggested at least
39% of the ears viewed had significant occlusion, and as a
consequence appropriate preparation for the subsequent large
scale hearing screening could be made with cerumen manage-
ment and medical referrals plans.
With the limited information available, there are still a number
of questions about the incidence of hearing loss in Mozambique.
The purpose of this report is to present results on the prevalence
of hearing loss and otologic conditions and in a sample
population of primary school children many hundreds of miles
north of the urban capital of Maputo.
Methodology
All 1st, 3rd, and 5th grade students (ranging in ages 6�20 years
old) at one of two primary schools in Maxixe, and children at
one preschool (0�5 years old) in Chicuque, Mozambique were
invited to be tested during an eight-day period in the winter
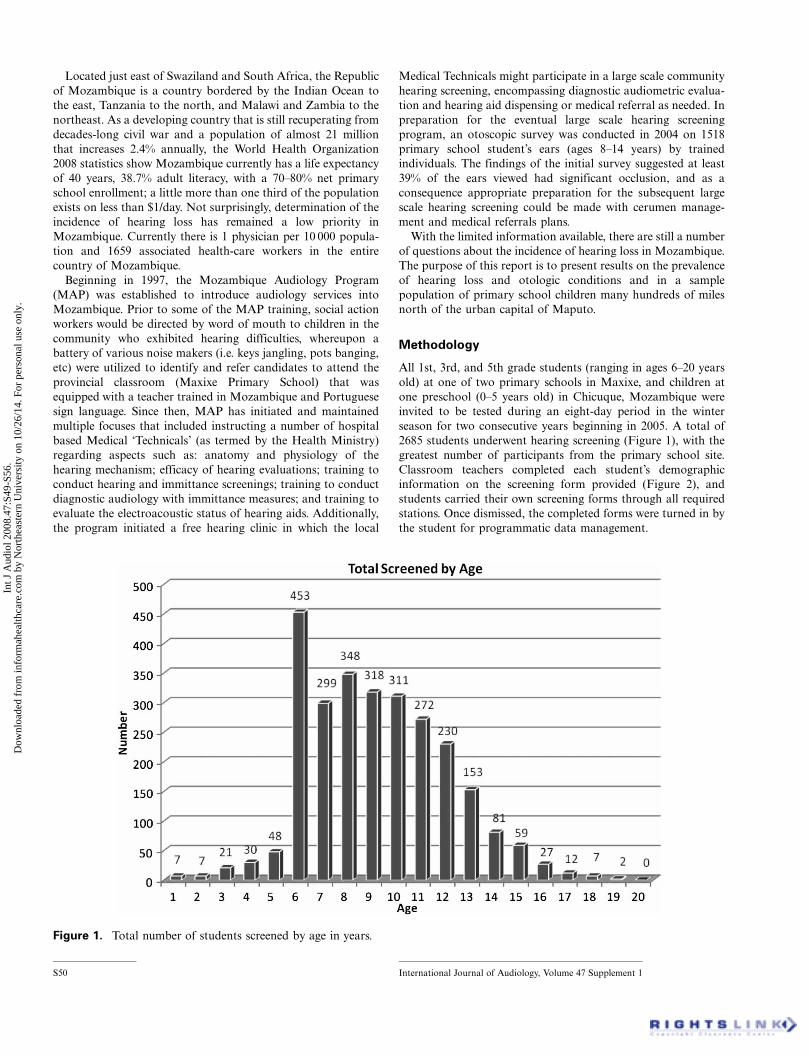
season for two consecutive years beginning in 2005. A total of
2685 students underwent hearing screening (Figure 1), with the
greatest number of participants from the primary school site.
Classroom teachers completed each student’s demographic
information on the screening form provided (Figure 2), and
students carried their own screening forms through all required
stations. Once dismissed, the completed forms were turned in by
the student for programmatic data management.
Figure 1. Total number of students screened by age in years.
S50 International Journal of Audiology, Volume 47 Supplement 1
Int J
Aud
iol 2
008.
47:S
49-S
56.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
thea
ster
n U
nive
rsity
on
10/2
6/14
. For
per
sona
l use
onl
y.
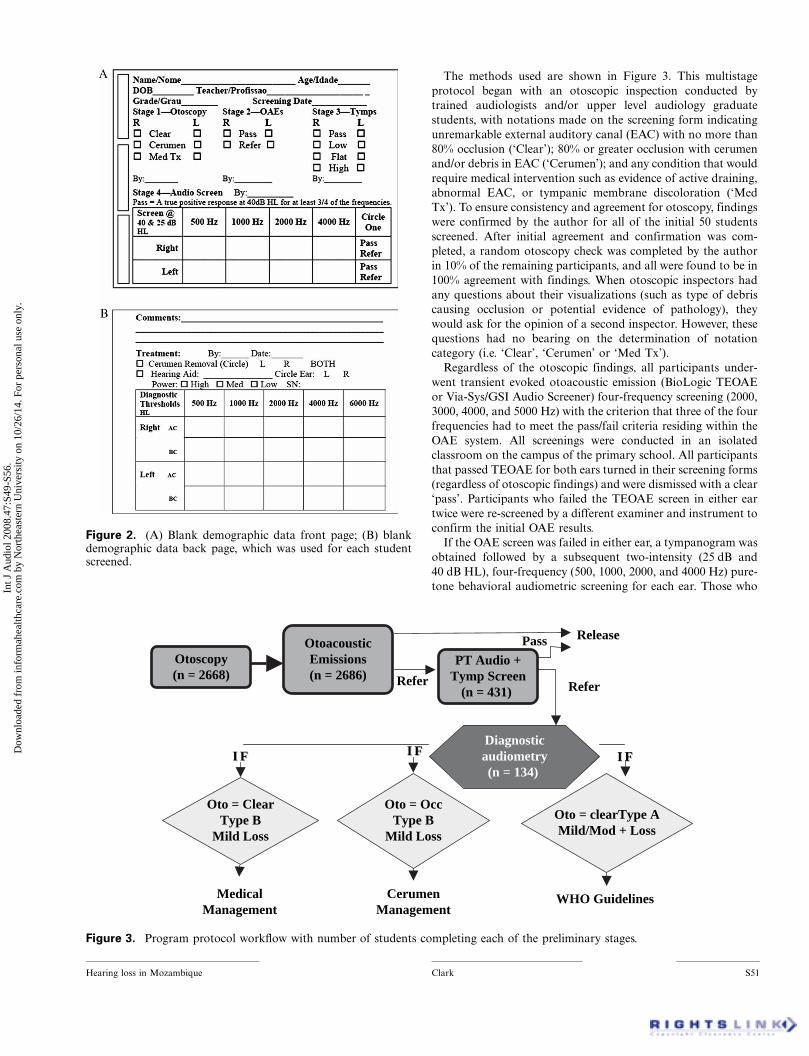
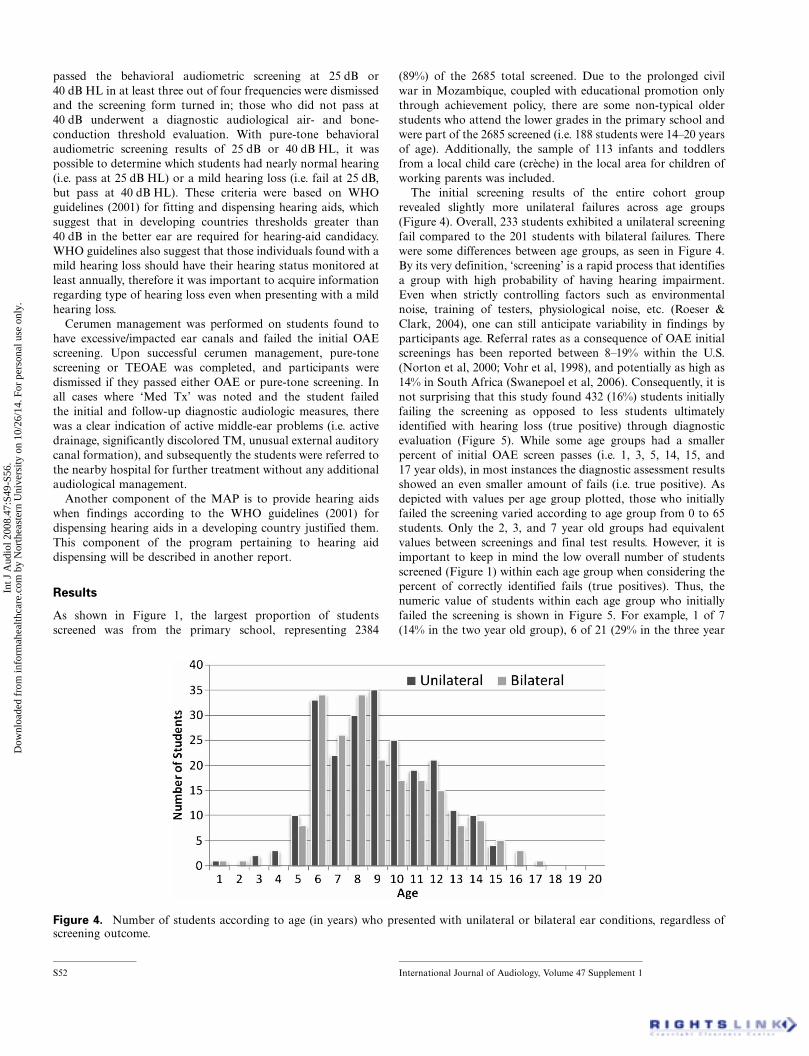
The methods used are shown in Figure 3. This multistage
protocol began with an otoscopic inspection conducted by
trained audiologists and/or upper level audiology graduate
students, with notations made on the screening form indicating
unremarkable external auditory canal (EAC) with no more than
80% occlusion (‘Clear’); 80% or greater occlusion with cerumen
and/or debris in EAC (‘Cerumen’); and any condition that would
require medical intervention such as evidence of active draining,
abnormal EAC, or tympanic membrane discoloration (‘Med
Tx’). To ensure consistency and agreement for otoscopy, findings
were confirmed by the author for all of the initial 50 students
screened. After initial agreement and confirmation was com-
pleted, a random otoscopy check was completed by the author
in 10% of the remaining participants, and all were found to be in
100% agreement with findings. When otoscopic inspectors had
any questions about their visualizations (such as type of debris
causing occlusion or potential evidence of pathology), they
would ask for the opinion of a second inspector. However, these
questions had no bearing on the determination of notation
category (i.e. ‘Clear’, ‘Cerumen’ or ‘Med Tx’).
Regardless of the otoscopic findings, all participants under-
went transient evoked otoacoustic emission (BioLogic TEOAE
or Via-Sys/GSI Audio Screener) four-frequency screening (2000,
3000, 4000, and 5000 Hz) with the criterion that three of the four
frequencies had to meet the pass/fail criteria residing within the
OAE system. All screenings were conducted in an isolated
classroom on the campus of the primary school. All participants
that passed TEOAE for both ears turned in their screening forms
(regardless of otoscopic findings) and were dismissed with a clear
‘pass’. Participants who failed the TEOAE screen in either ear
twice were re-screened by a different examiner and instrument to
confirm the initial OAE results.
If the OAE screen was failed in either ear, a tympanogram was
obtained followed by a subsequent two-intensity (25 dB and
40 dB HL), four-frequency (500, 1000, 2000, and 4000 Hz) pure-
tone behavioral audiometric screening for each ear. Those who
Figure 2. (A) Blank demographic data front page; (B) blankdemographic data back page, which was used for each studentscreened.
Diagnosticaudiometry(n = 134)
II FF II FF II FF
CerumenManagement
WHO Guidelines MedicalManagement
Otoscopy(n = 2668)
OtoacousticEmissions(n = 2686)
Pass Release
Refer
Oto = clearType AMild/Mod + Loss
Oto = OccType B
Mild Loss
Oto = ClearType B
Mild Loss
PT Audio +Tymp Screen
(n = 431) Refer
Figure 3. Program protocol workflow with number of students completing each of the preliminary stages.
Hearing loss in Mozambique Clark S51
Int J
Aud
iol 2
008.
47:S
49-S
56.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
thea
ster
n U
nive
rsity
on
10/2
6/14
. For
per
sona
l use
onl
y.
passed the behavioral audiometric screening at 25 dB or
40 dB HL in at least three out of four frequencies were dismissed
and the screening form turned in; those who did not pass at
40 dB underwent a diagnostic audiological air- and bone-
conduction threshold evaluation. With pure-tone behavioral
audiometric screening results of 25 dB or 40 dB HL, it was
possible to determine which students had nearly normal hearing
(i.e. pass at 25 dB HL) or a mild hearing loss (i.e. fail at 25 dB,
but pass at 40 dB HL). These criteria were based on WHO
guidelines (2001) for fitting and dispensing hearing aids, which
suggest that in developing countries thresholds greater than
40 dB in the better ear are required for hearing-aid candidacy.
WHO guidelines also suggest that those individuals found with a
mild hearing loss should have their hearing status monitored at
least annually, therefore it was important to acquire information
regarding type of hearing loss even when presenting with a mild
hearing loss.
Cerumen management was performed on students found to
have excessive/impacted ear canals and failed the initial OAE
screening. Upon successful cerumen management, pure-tone
screening or TEOAE was completed, and participants were
dismissed if they passed either OAE or pure-tone screening. In
all cases where ‘Med Tx’ was noted and the student failed
the initial and follow-up diagnostic audiologic measures, there
was a clear indication of active middle-ear problems (i.e. active
drainage, significantly discolored TM, unusual external auditory
canal formation), and subsequently the students were referred to
the nearby hospital for further treatment without any additional
audiological management.
Another component of the MAP is to provide hearing aids
when findings according to the WHO guidelines (2001) for
dispensing hearing aids in a developing country justified them.
This component of the program pertaining to hearing aid
dispensing will be described in another report.
Results
As shown in Figure 1, the largest proportion of students
screened was from the primary school, representing 2384
(89%) of the 2685 total screened. Due to the prolonged civil
war in Mozambique, coupled with educational promotion only
through achievement policy, there are some non-typical older
students who attend the lower grades in the primary school and
were part of the 2685 screened (i.e. 188 students were 14�20 years
of age). Additionally, the sample of 113 infants and toddlers
from a local child care (creche) in the local area for children of
working parents was included.
The initial screening results of the entire cohort group
revealed slightly more unilateral failures across age groups
(Figure 4). Overall, 233 students exhibited a unilateral screening
fail compared to the 201 students with bilateral failures. There
were some differences between age groups, as seen in Figure 4.
By its very definition, ‘screening’ is a rapid process that identifies
a group with high probability of having hearing impairment.
Even when strictly controlling factors such as environmental
noise, training of testers, physiological noise, etc. (Roeser &
Clark, 2004), one can still anticipate variability in findings by
participants age. Referral rates as a consequence of OAE initial
screenings has been reported between 8�19% within the U.S.
(Norton et al, 2000; Vohr et al, 1998), and potentially as high as
14% in South Africa (Swanepoel et al, 2006). Consequently, it is
not surprising that this study found 432 (16%) students initially
failing the screening as opposed to less students ultimately
identified with hearing loss (true positive) through diagnostic
evaluation (Figure 5). While some age groups had a smaller
percent of initial OAE screen passes (i.e. 1, 3, 5, 14, 15, and
17 year olds), in most instances the diagnostic assessment results
showed an even smaller amount of fails (i.e. true positive). As
depicted with values per age group plotted, those who initially
failed the screening varied according to age group from 0 to 65
students. Only the 2, 3, and 7 year old groups had equivalent
values between screenings and final test results. However, it is
important to keep in mind the low overall number of students
screened (Figure 1) within each age group when considering the
percent of correctly identified fails (true positives). Thus, the
numeric value of students within each age group who initially
failed the screening is shown in Figure 5. For example, 1 of 7
(14% in the two year old group), 6 of 21 (29% in the three year
Figure 4. Number of students according to age (in years) who presented with unilateral or bilateral ear conditions, regardless ofscreening outcome.
S52 International Journal of Audiology, Volume 47 Supplement 1
Int J
Aud
iol 2
008.
47:S
49-S
56.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
thea
ster
n U
nive
rsity
on
10/2
6/14
. For
per
sona
l use
onl
y.
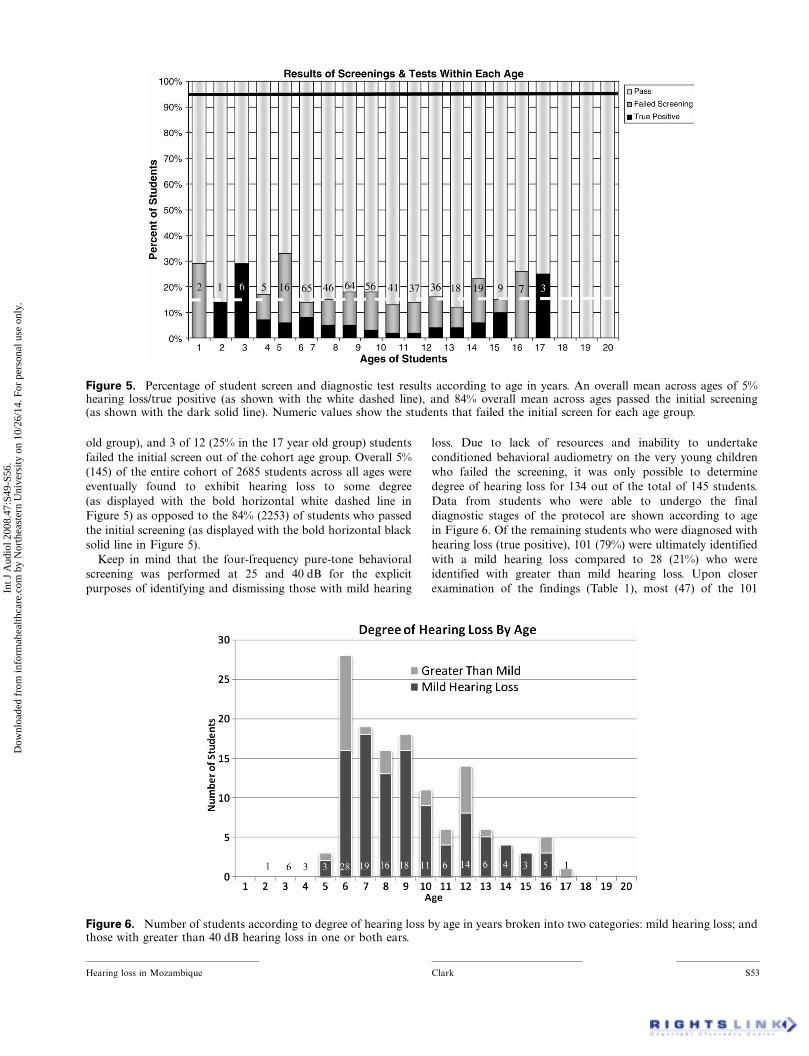
old group), and 3 of 12 (25% in the 17 year old group) students
failed the initial screen out of the cohort age group. Overall 5%
(145) of the entire cohort of 2685 students across all ages were
eventually found to exhibit hearing loss to some degree
(as displayed with the bold horizontal white dashed line in
Figure 5) as opposed to the 84% (2253) of students who passed
the initial screening (as displayed with the bold horizontal black
solid line in Figure 5).
Keep in mind that the four-frequency pure-tone behavioral
screening was performed at 25 and 40 dB for the explicit
purposes of identifying and dismissing those with mild hearing
loss. Due to lack of resources and inability to undertake
conditioned behavioral audiometry on the very young children
who failed the screening, it was only possible to determine
degree of hearing loss for 134 out of the total of 145 students.
Data from students who were able to undergo the final
diagnostic stages of the protocol are shown according to age
in Figure 6. Of the remaining students who were diagnosed with
hearing loss (true positive), 101 (79%) were ultimately identified
with a mild hearing loss compared to 28 (21%) who were
identified with greater than mild hearing loss. Upon closer
examination of the findings (Table 1), most (47) of the 101
Figure 6. Number of students according to degree of hearing loss by age in years broken into two categories: mild hearing loss; andthose with greater than 40 dB hearing loss in one or both ears.
Figure 5. Percentage of student screen and diagnostic test results according to age in years. An overall mean across ages of 5%hearing loss/true positive (as shown with the white dashed line), and 84% overall mean across ages passed the initial screening(as shown with the dark solid line). Numeric values show the students that failed the initial screen for each age group.
Hearing loss in Mozambique Clark S53
Int J
Aud
iol 2
008.
47:S
49-S
56.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
thea
ster
n U
nive
rsity
on
10/2
6/14
. For
per
sona
l use
onl
y.
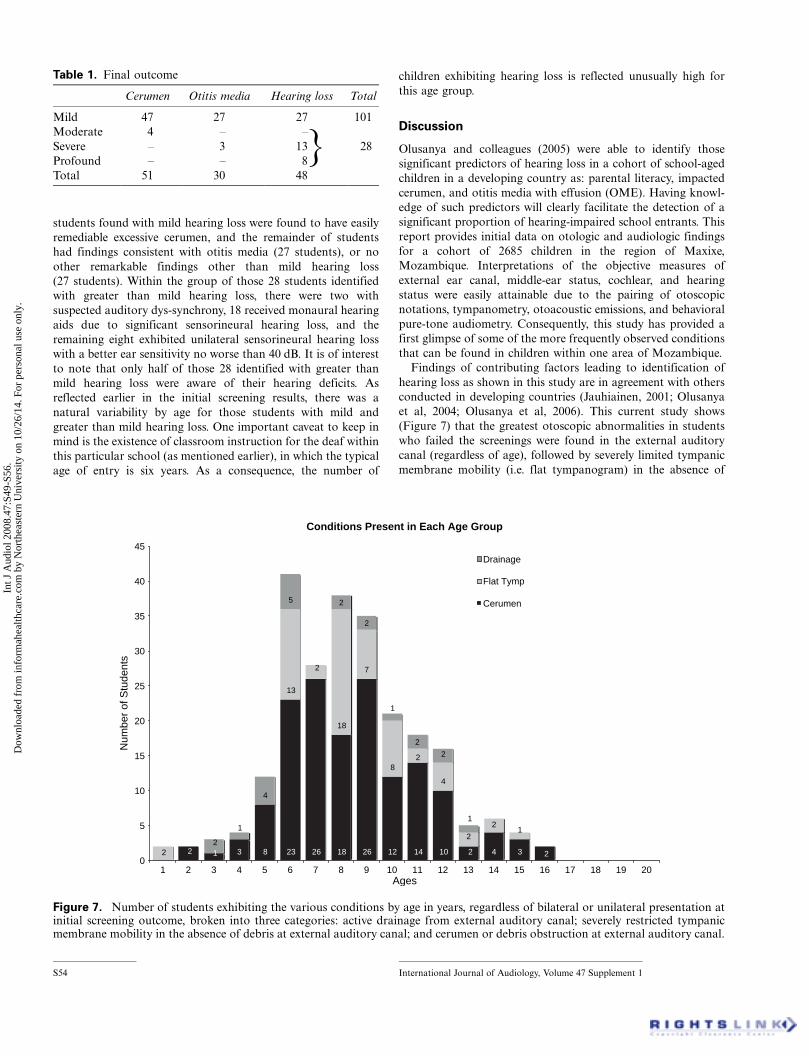
students found with mild hearing loss were found to have easily
remediable excessive cerumen, and the remainder of students
had findings consistent with otitis media (27 students), or no
other remarkable findings other than mild hearing loss
(27 students). Within the group of those 28 students identified
with greater than mild hearing loss, there were two with
suspected auditory dys-synchrony, 18 received monaural hearing
aids due to significant sensorineural hearing loss, and the
remaining eight exhibited unilateral sensorineural hearing loss
with a better ear sensitivity no worse than 40 dB. It is of interest
to note that only half of those 28 identified with greater than
mild hearing loss were aware of their hearing deficits. As
reflected earlier in the initial screening results, there was a
natural variability by age for those students with mild and
greater than mild hearing loss. One important caveat to keep in
mind is the existence of classroom instruction for the deaf within
this particular school (as mentioned earlier), in which the typical
age of entry is six years. As a consequence, the number of
children exhibiting hearing loss is reflected unusually high for
this age group.
Discussion
Olusanya and colleagues (2005) were able to identify those
significant predictors of hearing loss in a cohort of school-aged
children in a developing country as: parental literacy, impacted
cerumen, and otitis media with effusion (OME). Having knowl-
edge of such predictors will clearly facilitate the detection of a
significant proportion of hearing-impaired school entrants. This
report provides initial data on otologic and audiologic findings
for a cohort of 2685 children in the region of Maxixe,
Mozambique. Interpretations of the objective measures of
external ear canal, middle-ear status, cochlear, and hearing
status were easily attainable due to the pairing of otoscopic
notations, tympanometry, otoacoustic emissions, and behavioral
pure-tone audiometry. Consequently, this study has provided a
first glimpse of some of the more frequently observed conditions
that can be found in children within one area of Mozambique.
Findings of contributing factors leading to identification of
hearing loss as shown in this study are in agreement with others
conducted in developing countries (Jauhiainen, 2001; Olusanya
et al, 2004; Olusanya et al, 2006). This current study shows
(Figure 7) that the greatest otoscopic abnormalities in students
who failed the screenings were found in the external auditory
canal (regardless of age), followed by severely limited tympanic
membrane mobility (i.e. flat tympanogram) in the absence of
Table 1. Final outcome
Cerumen Otitis media Hearing loss Total
Mild 47 27 27 101
Moderate 4 � �Severe � 3 13 28
Profound � � 8
Total 51 30 48
}
Conditions Present in Each Age Group
3 8 23 26 18 26 12 14 10 4 3
13
18
7
8
4
4
5
2212
12
2
2
2
2
1
2
2
1
2
2
1
2
0
5
10
15
20
25
30
35
40
45
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20Ages
Num
ber
of S
tude
nts
Drainage
Flat Tymp
Cerumen
Figure 7. Number of students exhibiting the various conditions by age in years, regardless of bilateral or unilateral presentation atinitial screening outcome, broken into three categories: active drainage from external auditory canal; severely restricted tympanicmembrane mobility in the absence of debris at external auditory canal; and cerumen or debris obstruction at external auditory canal.
S54 International Journal of Audiology, Volume 47 Supplement 1
Int J
Aud
iol 2
008.
47:S
49-S
56.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
thea
ster
n U
nive
rsity
on
10/2
6/14
. For
per
sona
l use
onl
y.

EAC obstruction, and finally a smaller number of students with
active drainage condition. All of these conditions are indis-
criminant yet remediable health problems in many populations
around the world, but are found to more chronically impact
citizens residing in developing countries (Olusanya & Newton,
2007; WHO/CIBA, 1996).
A similar mass screening study conducted in Nigeria
(Olusanya, 2001), with 359 randomly chosen school-aged
children who attended various schools in the urban inner-city
of Lagos, showed 13.9% of school-aged children found with
hearing loss and 3.3% with sensorineural hearing loss. Despite
the difference in number of students assessed and the mean age
of participants, there was good agreement in findings between
the current study and the Olusanya study. This current study
showed an overall average of 5% of the total 2685 students
(regardless of age) were documented with varying degrees of
hearing loss of varying etiologies, with findings ranging more
greatly according to age. Olusanya (2001) also reported findings
that 50% of those children in Nigeria having hearing loss were in
fact experiencing a mild hearing loss. However, this current
study documented a larger percentage of children identified with
mild hearing loss (79%) within the group of children exhibiting
hearing loss. Since the current study conducted screenings
during two consecutive winter seasons, this could account for
the higher incidence of mild hearing loss than seen in the
Nigerian study. It is also important to take note that those
students, in the current program, who passed the initial OAE
screening could potentially have silent episodes of otitis media,
but the screening protocol would not facilitate identifying the
pathology since tympanometry was conducted only if there was
an OAE fail.
Six population studies (WHO, 1995) conducted in normal
schools in southern Africa, Angola, and Kenya found the
prevalence of mild or worse hearing impairment ranged from
0.5% in South Africa (defined with 35 dB cut-off) to 5.6% in
Kenya (defined with 30 dB cut-off) to 9% in a poorer area of
South Africa (defined with 30 dB cut-off). Yet, data from this
study are not in complete agreement with those reported by
Mozambique health representatives in 1995 (WHO). The 1995
report showed an overall mean of 18.6% incidence of otitis
media only, and an overall mean of 5% had hearing loss
accompanied with otitis media, in a group of 1000 primary
school (5�16 year old) students in the capital of Mozambique
(Maputo). They showed some variability according to age, with
the 11�13 year old students exhibiting a greater incidence for
both conditions (i.e. 21% with otitis media only; 9.8% of otitis
media accompanied with hearing loss). Clearly, the confound
findings had to do with percentage of students found with otitis
media as well as the age group most affected when comparing
the current findings with those reported in 1995. Unfortunately,
the 1995 WHO data was not accompanied with methodological
procedures and details about the cut-off audiometric intensities
for normal hearing, nor whether there were seasonal influences
for their findings. In addition, it is not known if the 1995 WHO
Mozambique audiometric data were collected with additional
information such as otoscopy, parental report, tympanometry,
etc.
Some of the benefits of conducting population studies about
hearing and hearing loss include raising community awareness:
to encourage avoidance of those behaviors that lead to impacted
cerumen (i.e. cleaning ear canals with sticks and rags); of signs
and symptoms of otitis media, as well as the critical importance
of seeking medical assistance at the onset of fever and/or
drainage; and of educational opportunities for aural rehabilita-
tion/habilitation. When there is very little infrastructure or only
limited audiological/otolaryngological services within a country,
it is not unusual to find higher than expected complication rates
from acute infections. One specific report suggests that compli-
cation rates from acute infections within developing countries
can be as high as 60 per 1000 cases in comparison to as few as
1 per 1000 cases in a developed country (WHO/PBD/PDH/00.1,
1998). Because the key to prevention of hearing loss is knowl-
edge of accurate epidemiological information on prevalence, risk
factors, and costs of hearing loss in the population, there is an
ongoing need for establishing national hearing health-care
programs within Mozambique that can be integrated with
primary health care. None the least of which would promote
good health practices, hearing conservation, as well as commu-
nity education and awareness.
WHO guidelines (2001) suggest that one of the purposes of
any hearing health project should be to increase community
awareness about hearing loss and hearing health. Interestingly,
none of those students identified with unilateral or mild hearing
loss, or their parents or teachers were aware of the student’s
hearing status. Of those students identified with greater than
mild hearing loss, only half were aware of their hearing status.
With an estimated almost 21 million population that increases
2.4% annually (WHO, 2008), it would appear that a silent
disability, such as hearing loss, is robbing Mozambique of an
underutilized natural resource in the manner of citizens who
could potentially be more productive and provide positive
contributions to their communities. As suggested by WHO
(1996), there is a need to gather prevalence data on conditions
such as otitis media, etc. in order to determine the burden of
disease and set priorities on a national level for prevention and
management. There continues to be an urgent need for more
accurate data in Mozambique and other developing countries
for a number of reasons: prevalence and cause may differ
between and within countries; national governments need
accurate information to prioritize health programs and select/
monitor preventive strategies; and compiling regional databases.
Currently, audiology as a profession is only provided as a
voluntary philanthropic program and any prevalence and
incidence of hearing loss investigations exist through this unique
program. Sadly, the Minister of Health for Mozambique has
made the decision to disallow medical teams to provide
professional service within the country. As a consequence there
is a cessation of any philanthropic audiology programs for the
foreseeable future.
Acknowledgements
Without the cooperation of the Mozambique Minister of Health
and Chicuque Rural Hospital, none of the work would have
been completed, and much is owed to the facilitation from both
administrations over the years. Tremendous gratitude goes to
Drs. Ross Roeser, DeWet Swanepoel, and Emily Tobey, whose
valued input has clearly improved the readability of this
manuscript. Thanks also to Ms. Rachel Wood and Dr.
Stephanie Cox for their notable diligence in accurately and
Hearing loss in Mozambique Clark S55
Int J
Aud
iol 2
008.
47:S
49-S
56.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
thea
ster
n U
nive
rsity
on
10/2
6/14
. For
per
sona
l use
onl
y.

methodically organizing these data. Those 1999�2004 Mozam-
bique Audiology Team members provided an invaluable base
that allowed us to set the stage for this ongoing demographic
study. Thanks also to 2005 and 2006 Mozambique Audiology
Team members for their ‘can do’ attitude while working on-site
in ‘interesting and challenging conditions’. Many thanks are
also owed to academic and industry supporters: UTDallas/
Callier Center; University Witwatersrand; Oak-Tree Products;
Widex; Hal-Hen Company; BioLogic Corporation; GSI Viasys
Healthcare; Siemens; Phonak; Starkey Foundation; Insta-Mold
Products; Kessler Renata Batteries.
References
Clark J.L. 2008. A two-year study on factors contributing to hearing lossin Mozambique. Community Ear and Hearing, 5.
Jauhiainen T. 2001. Hearing impaired children in developing countries.Scand Audiol, 30 (Suppl): 83�84.
Okeowo, P.A. 1985. Observation on the incidence of secretory otitismedia in Nigerian children. J Trop Pediatr, 31, 295�298.
Norton S.J., Gorga M.P., Widen J.E., Folsom R.C., Sinninger Y.S. et al,2000. Identification of neonatal hearing impairment: Summary andrecommendations. Ear Hear, 21, 529�535.
Olusanya, B.O. 2001. Early detection of hearing impairment in adeveloping country: What options? Audiology, 40, 141�147.
Olusanya, B.O. & Newton, V.E. 2007. Global burden of childhoodhearing impairment and disease control priorities for developingcountries. Lancet, 369, 1314�1317.
Olusanya, B.O., Okolo, A.A. & Aderemi, A.A. 2005. Predictors ofhearing loss in school entrants in a developing country. J Postgrad
Med, 50, 173�178.Olusanya, B.O., Luxon, L.M. & Wirz, S.L. 2004. Benefits and challenges
of newborn hearing screening for developing countries. Int J
Pediatric Otorhinolaryngol, 68, 287�305.Olusanya, B.O., Luxon, L.M. & Wirz, S.L. 2005. Childhood deafness
poses problems in developing countries. BMJ, 330, 480�481.Roeser, R.J. & Clark, J.L. 2004. Screening audiometry. In R. Roeser &
M. Downs (eds.) Auditory Disorders in School Children. New York:Thieme.
Swanepoel, D., Hugo, R. & Louw, B. 2006. Infant hearing screenings atimmunization clinics in South Africa. Int J Pediatric Otorhinolar-
yngol, 70, 1241�1249.Vohr, B.R., Carty, L.M., Moore, P.E. & Letourneau, K. 1998. The
Rhode Island hearing assessment program: Experience with state-wide hearing screening (1993�1996). J Pediatri, 133, 353�357.
World Health Organization (WHO) Prevention of Hearing Impairmentin Africa (1995). WHO/PDH/96.3/AFR/NCD/96.1: Report of aWorkshop, Nairobi, Kenya, 24�27 October.
WHO/World Health Statistics. 2008. http://www.who.int/whosis/whostat/2008/en/index.html
WHO/CIBA. 1996. Prevention of Hearing Impairment from ChronicOtitis Media; Report of a WHO/CIBA Foundation Workshop,London.
WHO/PBD/PDH/01.1. 2001. Guidelines for hearing aids and services fordeveloping countries. Report of a WHO/CBM Workshop; Germany.
WHO/PBD/PDH/00.10. 1998. Report of the International Primary Earand Hearing Care; Cape Town, South Africa; World HealthOrganization.
S56 International Journal of Audiology, Volume 47 Supplement 1
Int J
Aud
iol 2
008.
47:S
49-S
56.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nor
thea
ster
n U
nive
rsity
on
10/2
6/14
. For
per
sona
l use
onl
y.