Embed Size (px)
Citation preview
Page 1 of 15
DISCLAIMER
This Molina Clinical Policy (MCP) is intended to facilitate the Utilization Management process. It expresses
Molina's determination as to whether certain services or supplies are medically necessary, experimental,
investigational, or cosmetic for purposes of determining appropriateness of payment. The conclusion that a
particular service or supply is medically necessary does not constitute a representation or warranty that this
service or supply is covered (i.e., will be paid for by Molina) for a particular member. The member's benefit
plan determines coverage. Each benefit plan defines which services are covered, which are excluded, and
which are subject to dollar caps or other limits. Members and their providers will need to consult the member's
benefit plan to determine if there are any exclusion(s) or other benefit limitations applicable to this service or
supply. If there is a discrepancy between this policy and a member's plan of benefits, the benefits plan will
govern. In addition, coverage may be mandated by applicable legal requirements of a State, the Federal
government or CMS for Medicare and Medicaid members. CMS's Coverage Database can be found on the CMS
website. The coverage directive(s) and criteria from an existing National Coverage Determination (NCD) or
Local Coverage Determination (LCD) will supersede the contents of this Molina Clinical Policy (MCP)
document and provide the directive for all Medicare members.1
DESCRIPTION OF PROCEDURE/SERVICE/PHARMACEUTICAL 26 27
Acute Myelogenous Leukemia
Acute leukemia’s comprise a heterogeneous group of neoplastic disorders that arise from malignant
transformation of blood-forming, or hematopoietic, stem cells. Malignant transformation typically involves
chromosomal rearrangements (translocations), deletions, or additions, which disturb the normal control of cell
division, allowing affected cells to multiply without restraint. Clones, or leukemic cells, arising from such
transformation particularly influence the development of white blood cells (WBCs), or leukocytes, and rapidly
proliferate in the bone marrow, ultimately replacing normal cells and causing anemia, thrombocytopenia, and
granulocytopenia. After release into the blood stream, leukemic cells can infiltrate any organ or site and often
spread to the liver, spleen, lymph nodes, central nervous system (CNS), and gonads, where they continue to
grow and divide, resulting in small tumors, inflammation, and/or organ damage and failure. Acute myeloid
leukemia (AML) also called acute myeloblastic leukemia, acute myelogenous leukemia, and acute
nonlymphocytic leukemia (ANLL) is an aggressive disease in which too many myeloblasts or immature white
blood cells that are not lymphoblasts are found in the bone marrow and blood. Two methods are commonly
used to classify AML. The French-American-British (FAB) Cooperative Group classification is based on
morphological-histochemical cell characteristics and identifies eight subtypes of AML, categorized as M0-M7.
The newer, World Health Organization Classification System incorporates clinical, morphologic,
immunophenotypic, cytogenetic and molecular markers that can be used to direct treatment that include 5 major
subcategories of AML: 1) AML with recurrent genetic abnormalities; 2) AML with multilineage dysplasia; 3)
therapy-related AML and myelodysplasia (MDS); 4) AML not otherwise categorized; and 5) acute leukemia of
Subject: Hematopoietic Stem Cell Transplantation for Acute Myelogenous
Leukemia (AML)
Original Effective Date:
10/31/12
Policy Number:
MCP-119
Revision Date(s): 9/1/2015
Review Date: 12/16/15, 12/14/16
Page 2 of 15
ambiguous lineage. Certain gene and cytogenetic abnormalities have been identified as high-risk for a poor
prognosis with chemotherapy. These include internal tandem duplication of the FLT3 gene, deletions of the
long arms or monosomies of chromosomes 5 or 7; translocations or inversions of chromosome 3, t(6;9), t(9;22)
and abnormalities of chromosome 11q23, t(10;11) translocation, t(1;22)(p13;q13) translocation, trisomy 8, and
certain antigens/gycoproteins.
Most children and adults with newly diagnosed AML undergo systemic multiagent chemotherapy designed to
induce disease remission (induction therapy). These aggressive treatment approaches produce severe bone
marrow aplasia and suppression of the hematopoietic system, which may lead to morbidity and mortality from
infection or hemorrhage. Therefore, therapy is combined with appropriate supportive care involving early
recognition and treatment of infection and, when necessary, red blood cell and platelet transfusions. With
effective anticancer agents and appropriate supportive care, complete remission (CR) occurs in 75% to 90% of
the children and 60% to 70% of the adults with AML. Even with treatment most patients relapse and ultimately
die from leukemia. Among those who achieve first CR (CR1), disease-free survival has averaged only 40% at 5
years in children and overall survival with or without disease has averaged only 25% at ≥ 3 years in adults.
Since undetected minimal residual disease is a major cause of relapse, patients in CR usually undergo a second
phase and, often, a third phase of multiagent chemotherapy known as consolidation therapy and intensification
therapy, respectively, which frequently employ different agents and/or higher doses than used in induction
therapy in an attempt to eradicate residual disease. High-dose chemotherapy may be administered for this
purpose but also ablates normal marrow (myeloablation), thereby destroying the hematopoietic system.
Stem Cell Transplantation
Stem-cell transplantation refers to transplantation of hematopoietic stem cells (HSCs) from a donor into a
patient. HSCs are immature cells that can develop into any of the three types of blood cells (red cells, white
cells or platelets). HSCs are created in the bone marrow and are found in the bone marrow and peripheral blood.
There is also a high concentration of HSCs in umbilical-cord blood. Hematopoietic stem-cell transplantation
(HSCT) can be either autologous (using the person’s own stem cells) or allogeneic (using stem cells from a
donor). In allogeneic HSCT, it is preferable for donors to have a human leukocyte antigen (HLA) type that is
identical to the recipient. Matching is performed on the basis of variability at three of more loci of the HLA
gene (e.g., HLA-A, HLA-B, HLA-DRB1). As HLA variability increases, transplant-related morbidity and
mortality, including graft rejection and graft-versus-host disease, also increase.
RECOMMENDATION 3-36
All transplants require prior authorization from the Corporate Transplant Department. Solid organ
transplant requests will be reviewed by the Corporate Senior Medical Director or qualified clinical
designee. All other transplants will be by the Corporate Senior Medical Director or covering Medical
Director. If the criteria are met using appropriate NCD and/or LCD guidelines, state regulations and/or
MCP policies the Corporate Senior Medical Director’s designee can approve the requested transplant.
Members must meet UNOS guidelines for transplantation and the diagnosis must be made by a Specialist
in the Disease and or Transplant Surgeon.
Page 3 of 15
Pre-Transplant Evaluation: 25 32 34
Criteria for transplant evaluation include all of the following:
History and physical examination
Psychosocial evaluation and clearance:
No behavioral health disorder by history or psychosocial issues:
if history of behavioral health disorder, no severe psychosis or personality disorder
mood/anxiety disorder must be excluded or treated
member has understanding of surgical risk and post procedure compliance and
follow-up required
Adequate family and social support
EKG
Chest x-ray
Cardiac clearance in the presence of any of the following:
o chronic smokers
o > 50 years age
o those with a clinical or family history of heart disease or diabetes
Pulmonary clearance if evidence of pulmonary artery hypertension (PAH) or chronic pulmonary
disease
Neurological exam and clearance for transplant: [ONE]
o Normal exam by H&P
o Abnormal neurological exam with positive findings: [ONE]
Lumbar puncture normal cytology
Lumbar puncture with cytological exam abnormal: CNS disease treated prior to
clearance
Performance Status : [ONE]
o Karnofsky score 70-100%; or
o Eastern Cooperative Oncology Group (ECOG) grade 0-2
Lab studies:
o *Complete blood count, Kidney profile (blood urea nitrogen, creatinine), electrolytes,
calcium, phosphorous, albumin, liver function tests, Coagulation profile (prothrombin time,
and partial thromboplastin time)
o *Serologic screening for HIV, Epstein Barr virus (EBV), Hepatitis virus B (HBV), and
Hepatitis C(HCV), cytomegalovirus (CMV), RPR and/or FTA:
If HIV positive all of the following are met:
CD4 count >200 cells/mm-3 for >6 months
HIV-1 RNA undetectable
On stable anti-retroviral therapy >3 months
No other complications from AIDS (e.g., opportunistic infection, including
aspergillus, tuberculosis, coccidioides mycosis, resistant fungal infections, Kaposi’s
sarcoma, or other neoplasm)
If abnormal serology need physician plan to address and/or treatment as indicated
o UDS (urine drug screen) if patient is current or gives a history of past drug abuse
Page 4 of 15
*Colonoscopy (if indicated or if patient is 50 > older should have had an initial screening
colonoscopy, after initial negative screening requires follow up colonoscopy every ten years) with
complete workup and treatment of abnormal results as indicated
*GYN examination with Pap smear for women > 21 to < 65 years of age or indicated (not indicated
in women who have had a TAH or TVH) with in the last three year with complete workup and
treatment of abnormal results as indicated
Within the last 12 months:
Dental examination or oral exam showing good dentition and oral care or no abnormality on panorex
or plan for treatment of problems pre or post-transplant
*Mammogram (if indicated or > age 40) with complete workup and treatment of abnormal results as
indicated
*PSA if history of prostate cancer or previously elevated PSA with complete workup and treatment
of abnormal results as indicated
*Participating Centers of Excellence may waive these criteria
Criteria for Hematopoietic Allogeneic Stem Cell transplantation (HSCT) Transplantation:
1. Hematopoietic Allogeneic stem-cell transplantation (HSCT) ablative or non-myeloablative from a
human leukocyte antigen (HLA)-matched donor (i.e., at least six out of eight match of the HLA-A,
HLA-B, HLA-C and HLA-DRB1 markers) or from cord blood when there are no matched sibling or
unrelated donors (i.e. at least four out of six match of the HLA-A, HLA-B and HLA-DRB-1 markers)
may be authorized in adults and children for the treatment of acute myelogenous leukemia (AML) when
ANY of the following criteria are met:
All pre-transplant criteria are met; and
In adults who are > age 18 with any of the following:
o history of myelodysplastic syndrome (MDS)
o failed induction therapy: presence of leukemia blasts in the blood, bone marrow or any
extramedullary site after 4-6 weeks of chemotherapy
o high white blood cell count (WBC) > 100,000 at diagnosis
o AML after first relapse
o extramedullary disease outside the bone marrow especially affecting central nervous system
o requiring > one cycle to achieve remission
o Complete first remission (CR-1)* and poor to intermediate risk stratification 28 defined by
abnormal molecular and cytogenetic factors that include any of the following:
Intermediate:
Normal +8 only, t(9;11) only
c-KIT mutation in patients with t(8;21), inv(16) or t(16;16)
Poor:
Abnormalities of chromosome 11q23
Complex chromosome dislocations (3 or more abnormalities) that include -5, -7, 5q-,
7q-, +8, Inv3, t(3;3), t(6;9), t(9;22), 11q23
Normal cytogenetics with isolated FLT3-ITD mutations
*Note: Complete first remission (CR-1) is defined by bone marrow biopsy as:
Page 5 of 15
bone marrow is normocellular with no more than 5% blasts
no signs or symptoms of the disease
In children who are < age 18 with any of the following:
o in children who are < 2 years at diagnosis
o failed induction therapy: presence of leukemia blasts in the blood, bone marrow or any
extramedullary site after 4-6 weeks of chemotherapy
o high white blood cell count (WBC) > 100,000 at diagnosis
o AML after first relapse
o extramedullary disease outside the bone marrow especially affecting central nervous system
o requiring > one cycle to achieve remission
o Abnormality of chromosome 5 or 7
o Complete first remission (CR-1)* with HLA-matched sibling donor
o Poor to intermediate risk stratification 28 defined by abnormal molecular and cytogenetic
factors that include any of the following:
Intermediate:
Normal +8 only, t(9;11) only
c-KIT mutation in patients with t(8;21), inv(16) or t(16;16)
Poor:
Abnormalities of chromosome 11q23
Complex chromosome dislocations (3 or more abnormalities) that include -5, -7, 5q-,
7q-, +8, Inv3, t(3;3), t(6;9), t(9;22), 11q23
Normal cytogenetics with isolated FLT3-ITD mutations
*Note: Complete first remission (CR-1) is defined by bone marrow biopsy as [BOTH]: 26 27
bone marrow is normocellular with no more than 5% blasts; and
no signs or symptoms of the disease
OR
Second or subsequent complete remission (CR-2) following complete first remission (CR-1)
defined by bone marrow biopsy as [BOTH]:
o bone marrow is normocellular with no more than 5% blasts; and
o no signs or symptoms of the disease
AND
The requesting transplant recipient should not have any of the following absolute
contraindications:
o Cardiac, pulmonary, and nervous system disease that cannot be corrected and is a prohibitive
risk for surgery
o Malignant neoplasm with a high risk for reoccurrence, non-curable malignancy (excluding
localized skin cancer)
o Systemic and/or uncontrolled infection
o AIDS (CD4 count < 200cells/mm3)
Page 6 of 15
o Unwilling or unable to follow post-transplant regimen
Documented history of non-compliance
Inability to follow through with medication adherence or office follow-up
o Chronic illness with one year or less life expectancy
o Limited, irreversible rehabilitation potential
o Active untreated substance abuse issues, requires documentation supporting free from
addiction for minimally 6 months if previous addiction was present
o No adequate social/family support
The requesting transplant recipient should be evaluated carefully and potentially treated if the
following relative contraindications are present:
o Irreversible lung disease patients require consultation and clearance by a Pulmonologist prior
to consideration of transplantation, this includes the following:
o Smoking, documentation supporting free from smoking for 6 months
o Active peptic ulcer disease
o Active gastroesophageal reflux disease
o CVA with long term impairment that is not amendable to rehabilitation or a patient with
CVA/transient ischemic attack within past 6 months
o Obesity with body mass index of >30 kg/m2 may increase surgical risk
o Chronic liver disease such as Hepatitis B/C/D, or cirrhosis which increases the risk of death
from sepsis and hepatic failure requires consultation by a gastroenterologist or hepatologist
o Gall bladder disease requires ultrasound of the gall bladder with treatment prior to
transplantation
Criteria for Hematopoietic Autologous Stem Cell Transplantation:
2. Hematopoietic Autologous stem cell transplantation may be authorized only if the member has AML
in complete first remission (CR-1) and: [ALL]
All pre-transplant criteria are met; and
Does not have an allogeneic donor or has medical contraindications to an allogeneic
transplantation procedure; and
Is in complete morphologic and cytogenetic complete remission (CR) at the time of stem cell
harvest; and
Does not have myelodysplastic syndrome (MDS)
Should not have any of the absolute contraindications and should be evaluated for any relative
contraindications listed above
Criteria for Subsequent Hematopoietic Stem Cell Transplantation:
3. Hematopoietic Allogeneic stem cell transplantation (ablative or non-myeloablative) after the first
autologous stem cell transplantation has occurred may be authorized only one time for members with
AML who meet all of the above criteria for transplant and have any of the following:
bone marrow relapse: defined as the reappearance of leukemia cells in the bone marrow or
peripheral blood after a complete remission as indicated by a peripheral blast count of 5,000 or
greater ; or
Page 7 of 15
primary graft failure indicated by no signs of engraftment* by 42 days after the transplant; or
failure to engraft*; AND
a suitable allogeneic donor has been identified
4. A second or repeat Hematopoietic Autologous or Allogeneic stem cell transplantation (ablative or non-
myeloablative) may be authorized only one time for members with AML who meet all of the above
criteria for transplant and have any of the following: [ONE]
primary graft failure indicated by no signs of engraftment* by 42 days after the transplant; or
failure to engraft*
*Note: Engraftment is defined as the first 3 consecutive days on which the absolute neutrophil count
(ANC) exceeds 5 x 109/L or > ANC500 at any time after transplantation.15
CONTINUATION OF THERAPY
When extension of a previously approved transplant authorization is requested, review using updated clinical
information is appropriate.
If Molina Healthcare has authorized prior requests for transplantation, the following information is
required for medical review: [ALL]
o Presence of no absolute contraindication as listed above;
o History and physical within the last 12 months;
o Kidney profile within the last 12 months;
o Cardiac update if history of cardiac disease within two years (> 50 years of age);
o Psychosocial evaluation or update within the last 12 months;
o Per initial and updated history and physical, any other clinically indicated tests and/or scans as
determined by transplant center physician or Molina Medical Director.
If authorized prior requests for transplantation were obtained from another insurer, the following
information is required for medical review: [ALL]
o Authorization letter/documentation from previous insurer;
o Presence of no absolute contraindication as listed above;
o History and physical within the last 12 months;
o Cardiac update if history of cardiac disease within two years (> 50 years of age);
o Psychosocial evaluation or update within the last 12 months;
o Per initial and updated history and physical, any other clinically indicated tests and/or scans as
determined by transplant center physician or Molina Medical Director.
COVERAGE EXCLUSIONS
1. Allogeneic (ablative or non-myeloablative) stem cell transplantation or autologous stem cell
transplantation when the above criteria are not met.
Page 8 of 15
2. A second or repeat autologous or allogeneic (ablative or non-myeloablative) transplant due to persistent,
progressive or relapsed disease.
3. Hematopoietic stem cell collection, storage and freezing for a future unplanned transplant
SUMMARY OF MEDICAL EVIDENCE 4-21
The published medical evidence and outcomes for hematopoietic stem cell transplantation for acute
myelogenous leukemia (AML) in children and adults in the United States consists of registry data obtained from
transplant centers that perform adult and pediatric transplantation and is available from the United Network for
Organ Sharing (UNOS) database. Registry data demonstrates graft survival rates and outcomes for stem cell
transplantation based on demographic and clinical information.
Adults:
A systematic review and meta-analysis of allogeneic stem cell transplantation for individuals with AML in first
complete remission was conducted by Koreth and colleagues in 2009. Twenty-four prospective trials with 6,007
assigned participants were analyzed for relapse-free survival (RFS) and overall survival (OS) stratified by good,
intermediate, and poor-risk AML. Compared to non-allogeneic treatment modalities (e.g., consolidation
chemotherapy, autologous stem cell transplantation (SCT) or both) for AML in first CR, good-risk AML had a
combined hazard ratio (HR) of 1.06 (95% confidence interval [CI], 0.80-1.42) indicating a lack of RFS benefit
(P=.68). Intermediate-risk AML had a combined HR of 0.76 (95% CI, 0.68-0.85) with a significant RFS benefit
(P<.01) with allogeneic SCT. Similarly, poor-risk AML had a combined HR of 0.69 (95% CI, 0.57 – 0.84) with
a significant RFS with allogeneic SCT (P<.01). The authors concluded that SCT does not provide significant
benefit for good-risk AML in CR1 and that allogeneic SCT offers significant RFS and overall survival benefits
for intermediate- and poor-risk AML in CR1. 14
Another meta-analysis of allogeneic HSCT in patients with AML in first complete remission (CR1) pooled data
from 5 studies that included a total of 3,100 patients. Among those patients, 1,151 received allogeneic HSCT,
and 1,949 were given alternative therapies including chemotherapy and autologous HSCT. All of the studies
employed natural randomization based on donor availability, and an intention-to-treat analysis, with overall
survival (OS) and disease-free survival (DFS) as outcomes of interest. This analysis showed a significant
advantage of allogeneic HSCT in terms of OS for the entire cohort (fixed-effects model HR=1.17 95% CI: 1.06-
1.30; p=0.003; random-effects model HR=1.15, 95% CI: 1.01–1.32; p=0.037) even though none of the
individual studies did so. Meta-regression analysis showed that the effect of allogeneic HSCT on OS differed
depending on the cytogenetic risk groups of patients, suggesting significant benefit for poor-risk patients (HR=
1.39, 95% CI not reported), indeterminate benefit for intermediate-risk cases, and no benefit in better-risk
patients compared to alternative approaches. 13
The Dutch-Belgian Hemato-Oncology Cooperative Group and the Swiss Group for Clinical Cancer Research
(HOVON SAKK) collaborative study group evaluated outcome of patients with acute myeloid leukemia (AML)
in first remission (CR1) entered in 3 consecutive studies according to a donor versus no-donor comparison.
Between 1987 and 2004, 2287 pts were entered in these studies: 1032 pts (45%) without FAB M3 or t(15;17)
were in CR1 after 2 cycles of chemotherapy, received consolidation treatment, and were younger than 55 years

Page 9 of 15
of age and therefore eligible for allogeneic hematopoietic stem cell transplantation (allo-SCT). An HLA-
identical sibling donor was available for 326 pts (32%), and 599 pts (58%) lacked such a donor, information
was not available in 107 pts. Compliance with allo-SCT was 82% (268 of 326). Cumulative incidences of
relapse were, respectively, 32% versus 59% for pts with versus those without a donor. Despite more treatment
related mortality (TRM) in the donor group disease-free survival (DFS) appeared significantly better in the
donor group. Following risk-group analysis, DFS was significantly better for pts with a donor and an
intermediate or poor-risk profile and also better in pts younger than 40 years of age. The authors concluded that
the results were evaluated in a meta-analysis which revealed a significant benefit of 12% in overall survival
(OS) by donor availability for all patients with AML in CR1 without a favorable cytogenetic profile. 11
Reduced Intensity Conditioning Regimen (RIC)
Outcomes of 315 reduced intensity conditioning regimen (RIC) were compared with 407 myeloablative (MA)
HSCT recipients to study the results of (RIC) in the HLA identical haematopoietic stem cell transplantation
(HSCT) compared to those after (MA) regimen HSCT in patients with acute myeloblastic leukaemia (AML)
over 50 years of age. The majority of RIC was fludarabine-based regimen associated to busulphan (BU) (53%)
or low-dose total body irradiation (24%). Multivariate analyses of outcomes were used adjusting for differences
between both groups. The median follow-up was 13 months. Cytogenetics, FAB classification, WBC count at
diagnosis and status of the disease at transplant were not statistically different between the two groups.
However, RIC patients were older, transplanted more recently, and more frequently with peripheral blood
allogeneic stem cells as compared to MA recipients. In multivariate analysis, acute GVHD (II–IV) and
transplant-related mortality were significantly decreased and relapse incidence was significantly higher after
RIC transplantation. Leukaemia-free survival was not statistically different between the two groups. The
authors concluded that these results may set the grounds for prospective trials comparing RIC with other
strategies of treatment in elderly AML. 10
Children:
A retrospective review by Ravindranath et al. (2005) showed the results of a total of 1823 children with AML
enrolled in four consecutive Pediatric Oncology Group (POG) clinical trials from the years 1981 to 2000. Of
these four trials one labeled POG 8821 compared the efficacy of autologous HSCT with that of intensive
consolidation chemotherapy. Intent-to-treat analysis revealed similar five-year event-free survival (EFS)
estimates for the autologous HSCT (36%) and intensive chemotherapy (35%) groups. There was a high rate of
treatment-related mortality in the autologous HSCT group. The study also demonstrated superior results of
allogeneic BMT for patients with histocompatible related donors. The 5-year event free survival estimate was
64% for allogeneic BMT. 12
A prospective multi-center AML-BFM 98 study evaluated the impact of allogeneic stem cell transplantation in
children with high-risk acute myeloid leukemia in first complete remission. 247 HLA-typed children and
adolescents (ages 0 to 18 years) with high-risk acute myeloid leukemia, who achieved first complete remission
were included in this analysis. All patients received double induction and consolidation. Based on the
availability of a matched-sibling donor, 61 patients were allocated by genetic chance to allogeneic stem cell
transplantation and 186 patients received chemotherapy-only (i.e. intensification and maintenance therapy).
Intention-to-treat analysis did not show a significantly different 5-year disease-free survival (49±6% vs 45±4%),
or overall survival (68±6% vs 57±4%,) between the matched-sibling donor and no-matched-sibling donor
Page 10 of 15
groups, whereas late adverse effects occurred more frequently after allogeneic stem cell transplantation (72.5%
vs 31.8%). These results were confirmed by as-treated analysis corrected for the time until transplantation (5-
year overall survival: 72±8% vs 60±4%). Subgroup analysis demonstrated improved survival rates for patients
with 11q23 aberrations allocated to allogeneic stem cell transplantation (5-year overall survival: 94±6% vs
52±7%) in contrast to patients without 11q23 aberrations (5-year overall survival: 58±8% vs 55±5%. The
authors concluded that In conclusion, the advantage of allogeneic SCT in the post-remission management of
pediatric high-risk AML with 11q23 aberrations compared to chemotherapy only. However, the specific 11q23
cytogenetic subgroups which might benefit from early allogeneic SCT have to be defined by future studies. In
contrast, the remaining patients demonstrated no advantage from allogeneic SCT in first complete remission. 22
Autologous vs. Allogeneic Stem Cell Transplant:
A systematic overview of the best available evidence on the clinical effectiveness and cost-effectiveness of SCT
in the treatment of acute leukemia was conducted. Electronic databases, including MEDLINE, EMBASE and
the Cochrane Library, were searched from inception to December 2008 to identify published systematic reviews
and meta-analyses. reviews and meta-analyses were critically appraised and data extracted and narratively
presented. Included randomized controlled trials (RCTs) and donor versus no donor (DvND) studies were
mapped to the evidence covered in existing systematic reviews and meta-analyses according to a framework of
12 decision problems (DPs): DP1 related to SCT in adults with AML in first complete remission (CR1); DP2 to
adults with AML in second or subsequent remission or with refractory disease (CR2+); DP3 to children with
AML in CR1; DP4 to children with AML in CR2+; DP5 to adults with ALL in CR1; DP6 to adults with ALL in
CR2+; DP7 to children with ALL in CR1; DP8 to children with ALL in CR2+; DP9 to comparison of different
sources of stem cells in transplantation; DP10 to different conditioning regimens; DP11 to the use of purging in
autologous SCT; and DP12 to the use of T-cell depletion in allogeneic SCT. Fifteen systematic reviews/meta-
analyses met the inclusion criteria for the review of clinical effectiveness, thirteen of which were published
from 2004 onwards. The best available evidence for effectiveness of allogeneic SCT using stem cells from
matched sibling donors came from DvND studies: there was sufficient evidence to support the use of allogeneic
SCT in DP1 (except in good-risk patients), DP3 (role of risk stratification unclear) and DP5 (role of risk
stratification unclear). There was conflicting evidence in DP7 and a paucity of evidence from DvND studies for
all decision problems concerning patient groups in CR2+. The best available evidence for effectiveness of
autologous SCT came from RCTs: overall, evidence suggested that autologous SCT was either similar to or less
effective than chemotherapy. There was a paucity of evidence from published reviews of RCTs for DPs 9-12.
Nineteen studies met the inclusion criteria in the cost-effectiveness review, most reporting only cost information
and only one incorporating an economic model. Although there is a wealth of information on costs and some
information on cost-effectiveness of allogeneic SCT in adults with AML (DPs 1 and 2), there is very limited
evidence on relative costs and cost-effectiveness for other DPs. The authors concluded that existing evidence
suggests that sibling donor allogeneic SCT may be more effective than chemotherapy in adult AML (except in
good-risk patients) in CR1, childhood AML in CR1 and adult ALL in CR1, and that autologous SCT is equal to
or less effective than chemotherapy. 4
Another meta-analysis published by Wang and colleagues in 2010 evaluated autologous HSCT versus further
chemotherapy or no further treatment for AML in CR1. A total of 9 randomized trials involving 1,104 adults
who underwent autologous HSCT and 1,118 who received additional chemotherapy or no additional treatment
Page 11 of 15
were identified. The analyses suggest that autologous HSCT in CR1 was associated with statistically significant
reduction of relapse risk (RR = 0.56, 95% CI = 0.44, 0.71, p = 0.0004) and significant improvement in DFS
(HR = 0.89, 95% CI = 0.80, 0.98), but at the cost of significantly increased NRM (RR = 1.90, 95% CI = 0.72.
0.87, p = 0.0002). There were more deaths during the first remission among patients assigned to autologous
HSCT than among the chemotherapy recipients or further untreated patients. As a consequence of increased
NRM, no statistical difference in OS (HR = 1.05, 95% CI = 0.91, 1.21) was associated with the use of
autologous HSCT compared to further chemotherapy or no further therapy. 19
Professional Society Guidelines: Several professional society organizations have recommended that
Allogeneic SCT is the preferred method of treatment for individuals in first complete remission (CR1) with
HLA matched sibling donor, AML after relapse, and second complete remission (CR2). 22-28
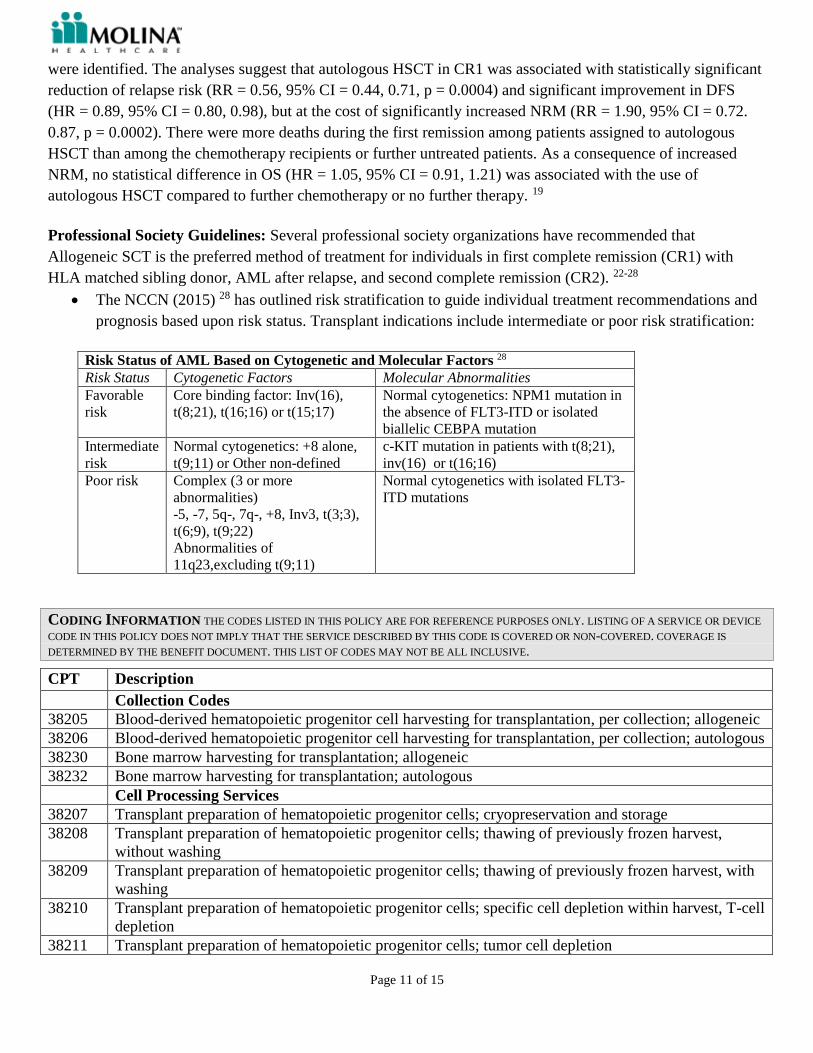
The NCCN (2015) 28 has outlined risk stratification to guide individual treatment recommendations and
prognosis based upon risk status. Transplant indications include intermediate or poor risk stratification:
Risk Status of AML Based on Cytogenetic and Molecular Factors 28
Risk Status Cytogenetic Factors Molecular Abnormalities
Favorable
risk
Core binding factor: Inv(16),
t(8;21), t(16;16) or t(15;17)
Normal cytogenetics: NPM1 mutation in
the absence of FLT3-ITD or isolated
biallelic CEBPA mutation
Intermediate
risk
Normal cytogenetics: +8 alone,
t(9;11) or Other non-defined
c-KIT mutation in patients with t(8;21),
inv(16) or t(16;16)
Poor risk Complex (3 or more
abnormalities)
-5, -7, 5q-, 7q-, +8, Inv3, t(3;3),
t(6;9), t(9;22)
Abnormalities of
11q23,excluding t(9;11)
Normal cytogenetics with isolated FLT3-
ITD mutations
CODING INFORMATION THE CODES LISTED IN THIS POLICY ARE FOR REFERENCE PURPOSES ONLY. LISTING OF A SERVICE OR DEVICE
CODE IN THIS POLICY DOES NOT IMPLY THAT THE SERVICE DESCRIBED BY THIS CODE IS COVERED OR NON-COVERED. COVERAGE IS
DETERMINED BY THE BENEFIT DOCUMENT. THIS LIST OF CODES MAY NOT BE ALL INCLUSIVE.
CPT Description
Collection Codes
38205 Blood-derived hematopoietic progenitor cell harvesting for transplantation, per collection; allogeneic
38206 Blood-derived hematopoietic progenitor cell harvesting for transplantation, per collection; autologous
38230 Bone marrow harvesting for transplantation; allogeneic
38232 Bone marrow harvesting for transplantation; autologous
Cell Processing Services
38207 Transplant preparation of hematopoietic progenitor cells; cryopreservation and storage
38208 Transplant preparation of hematopoietic progenitor cells; thawing of previously frozen harvest,
without washing
38209 Transplant preparation of hematopoietic progenitor cells; thawing of previously frozen harvest, with
washing
38210 Transplant preparation of hematopoietic progenitor cells; specific cell depletion within harvest, T-cell
depletion
38211 Transplant preparation of hematopoietic progenitor cells; tumor cell depletion
Page 12 of 15
38212 Transplant preparation of hematopoietic progenitor cells; red blood cell removal
38213 Transplant preparation of hematopoietic progenitor cells; platelet depletion
38214 Transplant preparation of hematopoietic progenitor cells; plasma (volume) depletion
38215 Transplant preparation of hematopoietic progenitor cells; cell concentration in plasma, mononuclear,
or buffy coat layer
Cell infusion codes
38240 Bone marrow or blood-derived peripheral stem cell transplantation; allogeneic
38241 Bone marrow or blood-derived peripheral stem cell transplantation; autologous
38242 Bone marrow or blood-derived peripheral stem cell transplantation; allogeneic donor lymphocyte
infusions
HCPCS Description
S2140 Cord blood harvesting for transplantation, allogeneic
S2142 Cord blood derived stem-cell transplantation, allogeneic
S2150 Bone marrow or blood-derived stem cells (peripheral or umbilical), allogeneic or autologous,
harvesting, transplantation, and related complications; including pheresis and cell
preparation/storage; marrow ablative therapy; drugs; supplies; hospitalization with outpatient follow-
up; medical/surgical, diagnostic, emergency, and rehabilitative services; and the number of days of
pre-and post-transplant care in the global definition
ICD-9 Description: [For dates of service prior to 10/01/2015]
205.00-
205.02
Acute myeloid leukemia
ICD-10 Description: [For dates of service on or after 10/01/2015]
C92.0-
C95.0
Acute myeloid leukemia
RESOURCE REFERENCES
Government Agency
1. Centers for Medicare & Medicaid Services. NCD for Stem Cell Transplantation (110.8.1). 2010.
Accessed at: http://www.cms.gov/medicare-coverage-database/
2. National Marrow Donor Program. AML Transplant Outcomes. Accessed at:
http://marrow.org/Physicians/When_to_Transplant/Outcomes_by_Disease.aspx
3. National Bone Marrow Donor Program HLA Matching Requirements. Accessed at:
http://marrow.org/Patient/Transplant_Process/Search_Process/HLA_Matching__Finding_the_Best_Don
or_or_Cord_Blood_Unit.aspx
Peer Reviewed Publications
4. Ashfaq K, Yahaya I et al. Clinical effectiveness and cost-effectiveness of stem cell transplantation in the
management of acute leukaemia: a systematic review. Health Technol Assess. 2010 Dec;14(54):iii-iv,
ix-xi, 1-141.
Page 13 of 15
5. Imrie K, Rumble RB, Crump M, Advisory Panel on Bone Marrow and Stem Cell Transplantation,
Hematology Disease Site Group. Stem cell transplantation in adults: recommendations. Toronto (ON):
Cancer Care Ontario Program in Evidence-based Care; 2009 Jan 30. 78 p. Accessed at:
https://www.cancercare.on.ca/common/pages/UserFile.aspx?serverId=6&path=/File%20Database/CCO
%20Files/PEBC/pebc_stemcell.pdf
6. C Mackall, T Fry, R Gress, K Peggs, J Storek and A Toubert. Background to hematopoietic cell
transplantation, including post-transplant immune recovery. Bone Marrow Transplant 44: 457-462;
doi:10.1038/bmt.2009.255 Accessed at:
http://www.nature.com/bmt/journal/v44/n8/full/bmt2009255a.html
7. Eastern Cooperative Oncology Group (ECOG) Performance Status. Accessed at:
http://www.ecog.org/general/perf_stat.html
8. Collins RH, Goldstein S, Giralt S, et al. Donor leukocyte infusions in acute lymphocytic leukemia. Bone
Marrow Transplant. 2000; 26(5): 511-516. Accessed at:
http://www.nature.com/bmt/journal/v26/n5/full/1702555a.html
9. Mackinnon S. American Society of clinical Oncology (ASCO). Donor Lymphocyte Infusion after
Allogeneic Stem Cell Transplantation. 2008. Accessed at:
http://www.asco.org/ascov2/Education+&+Training/Educational+Book?&vmview=edbk_detail_view&
confID=55&abstractID=54
10. Aoudjhane M, Labopin M et al. Comparative outcome of reduced intensity and myeloablative
conditioning regimen in HLA identical sibling allogeneic haematopoietic stem cell transplantation for
patients older than 50 years of age with acute myeloblastic leukaemia: a retrospective survey from the
Acute Leukemia Working Party (ALWP) of the European group for Blood and Marrow transplantation
(EBMT). Leukemia. 2005 Dec;19(12): 2304-12. Accessed at:
http://www.medicine.ufl.edu/hemonc/fellowship/Reading_List/2006
2007%20BMT%20ARTICLES/Mini-Transplants/Aoudjhane.pdf
11. Cornelisson JJ, van Putten WL et al. Results of a HOVON/SAKK donor versus no-donor analysis of
myeloablative HLA-identical sibling stem cell transplantation in first remission acute myeloid leukemia
in young and middle-aged adults: benefits for whom? Blood. 2007 May 1;109(9):3658-66. Epub 2007
Jan 9. Accessed at: http://bloodjournal.hematologylibrary.org/content/109/9/3658.full.pdf
12. Ravindranath Y, Chang M. et al. Pediatric Oncology Group (POG) studies of acute myeloid leukemia
(AML): a review of four consecutive childhood AML trials conducted between 1981 and 2000.
Leukemia. 2005 Dec; 19(12):2101-16. Accessed at:
http://www.nature.com/leu/journal/v19/n12/full/2403927a.html
13. Yanada, M, Matsuo, K, Emi, N, Naoe, T. Efficacy of allogeneic hematopoietic stem cell transplantation
depends on cytogenetic risk for acute myeloid leukemia in first disease remission: a meta analysis.
Cancer. 2005 Apr 15;103(8):1652-8. PMID: 15742336
14. Koreth, J, Schlenk, R, Kopecky, KJ, et al. Allogeneic stem cell transplantation for acute myeloid
leukemia in first complete remission: systematic review and meta-analysis of prospective clinical trials.
JAMA. 2009 Jun 10;301(22):2349-61. PMID: 19509382
15. National Bone Marrow Donor Program. Measuring Engraftment. Accessed at:
http://marrow.org/Patient/Transplant_Process/Days_0-30/Measuring_Engraftment.aspx
16. Thakar MS, Forman SJ. ASH evidence-based guidelines: is there a role for second allogeneic transplant
after relapse? Hematology Am Soc Hematol Educ Program. 2009:414-8. Accessed at:
http://asheducationbook.hematologylibrary.org/content/2009/1/414.long
17. Blau IW, Basara N et al. Second allogeneic hematopoietic stem cell transplantation as treatment for
leukemia relapsing following a first transplant. Bone Marrow Transplant. 2000 Jan; 25(1):41-5.
18. Michallet M, Tanguy ML et al. Second allogeneic haematopoietic stem cell transplantation in relapsed
acute and chronic leukaemias for patients who underwent a first allogeneic bone marrow transplantation:
Page 14 of 15
a survey of the Société Française de Greffe de moelle (SFGM). Bone Marrow Transplant. 2000
Jan;25(1):41-5.
19. Wang, J, Ouyang, J, Zhou et al. Autologous hematopoietic stem cell transplantation for acute myeloid
leukemia in first complete remission: a meta-analysis of randomized trials. Acta Haematol.
2010;124(2):61-71. PMID: 20616541
20. Klusmann JH, Reinhardt D, Zimmermann M et al. The role of matched sibling donor allogeneic stem
cell transplantation in pediatric high-risk acute myeloid leukemia: results from the AML-BFM 98 study.
Haematologica. 2012 Jan; 97(1):21-9. Epub 2011 Sep 20.
21. Bejanyan N, Weisdorf DJ, Logan BR, et al. Survival of patients with acute myeloid leukemia relapsing
after allogeneic hematopoietic cell transplantation: a center for international blood and marrow
transplant research study. Biol Blood Marrow Transplant. 2015; 21(3):454-459.
Professional Society Guidelines
22. National Marrow Donor Program® (NMDP) and the American Society for Blood and Marrow
Transplantation (ASBMT) 2015 referral guidelines: Recommended Timing for Transplant Consultation.
Accessed at: https://bethematchclinical.org/Transplant-Indications-and-Outcomes/Referral-Timing-
Guidelines/
23. The American Society for Blood and Marrow Transplantation (ASBMT). The Role of Cytotoxic
Therapy with Hematopoietic Stem Cell Transplantation in the Therapy of Adult Acute Myeloid
Leukemia in Adults: Biol Blood Marrow Transplant. 2008; 14:135-136. Accessed at:
http://www.asbmt.org/?page=GuidelineStatements
24. The American Society for Blood and Marrow Transplantation (ASBMT). The Role of Cytotoxic
Therapy with Hematopoietic Stem Cell Transplantation in the Therapy of Acute Myeloid Leukemia in
Children. Biology of Blood and Marrow Transplantation 2007;13:500-501. Accessed at:
http://www.asbmt.org/?page=GuidelineStatements
25. National Marrow Donor Program® (NMDP). Patient Eligibility for HCT. Accessed at:
https://bethematchclinical.org/Transplant-Indications-and-Outcomes/Eligibility/
26. National Cancer Institute. Adult Acute Myeloid Leukemia PDQ 2015. Accessed at:
http://www.cancer.gov/types/leukemia/patient/adult-aml-treatment-pdq
27. National Cancer Institute. Childhood Acute Myeloid Leukemia PDQ 2015. Accessed at:
http://www.cancer.gov/types/leukemia/patient/adult-aml-treatment-pdq
28. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology Acute
Myeloid Leukemia. Version 1.2015. Accessed at:
http://www.nccn.org/professionals/physician_gls/f_guidelines.asp
Other Resources
29. McKesson InterQual Criteria for Procedures: Adult 2015 InterQual Transplantation, Allogeneic Stem
Cell, Autologous Stem Cell; 2015.
30. DynaMed LLC [website]. Acute Myeloid Leukemia. 2015
31. UpToDate. Larson R. Treatment of relapsed or refractory acute myeloid leukemia. 2015.
32. UpToDate: Holmberg L, Deeg H, Sandmaier B. Determining eligibility for autologous hematopoietic
cell transplantation. 2015.
33. UpToDate. Larson R. Post Remission Therapy for Acute Myeloid Leukemia in Younger Adults. 2015.
34. UpToDate. Deeg H, Sandmaier B. Determining eligibility for allogeneic hematopoietic cell
transplantation. 2015.
35. UpToDate: Chao NG. Selection of an umbilical cord blood graft for hematopoietic cell transplantation.
2015.

Page 15 of 15
36. Advanced Medical Review (AMR): Policy reviewed by MD board certified in Internal Medicine,
Oncology, Hematology. October 19, 2012

![Germline Met Mutations in Mice Reveal Mutation- and ...€¦ · myelogenous leukemias (AML) and other hematological malig-nancies [3]. These studies and numerous others have demonstrat-](https://img.pdfslide.net/doc/110x75/5fd5e90e6848df0f7457757f/germline-met-mutations-in-mice-reveal-mutation-and-myelogenous-leukemias-aml.jpg)
























![[Ghiduri][Cancer]Chronic Myelogenous Leukemia](https://img.pdfslide.net/doc/110x75/577cc6ea1a28aba7119f80de/ghiduricancerchronic-myelogenous-leukemia.jpg)

