Embed Size (px)
Citation preview
www.elsevier.com/locate/braindev
Brain & Development 29 (2007) 109–111
Case report
Hemiconvulsion–hemiplegia–epilepsy syndrome: Early magneticresonance imaging findings and neuroradiological follow-up
I. Toldo a, M. Calderone b, C. Boniver a, Ch. Dravet c, R. Guerrini c,d, A.M. Laverda a,*
a Pediatrics Department, University of Padova, 35128 Padova, Italyb Division of Neuroradiology, Padova, Italy
c Department of Child Neurology and Psychiatry, IRCCS Fondazione Stella Maris, Pisa, Italyd Department of Child Neurology and Psychiatry, University of Pisa, Italy
Received 10 February 2006; received in revised form 15 June 2006; accepted 23 June 2006
Abstract
We describe a case of hemiconvulsion–hemiplegia–epilepsy (HHE) syndrome documented by longitudinal magnetic reso-nance imaging (MRI). A two-year and nine-month-old boy had a prolonged hemiconvulsion during fever followed by righthemiparesis. Seven days later the imaging abnormality on T2 and diffusion-weighted images (DWI) was limited to the whitematter of the left hemisphere. One month later severe gliosis and unilateral brain atrophy were already evident. MRI isuseful in the early stages of prolonged seizures and T2 and DWI abnormalities appear to be well correlated with paren-chymal damage that results from sustained ictal activity. The neuroradiological findings in our case and in the few HHEpatients reported in the literature seem to be very characteristic and, if confirmed in larger series, could permit an earlydiagnosis.� 2006 Elsevier B.V. All rights reserved.
Keywords: Hemiconvulsion–hemiplegia–epilepsy syndrome; Status epilepticus; Unilateral brain atrophy
1. Introduction
HHE syndrome is characterized by prolonged unilat-eral convulsions during fever in children under 4 yearsof age, who subsequently develop a transient or defini-tive hemiplegia. Later partial epilepsy is often observed.An extensive atrophy of the involved hemisphere is alsodocumented by neuroimaging.
Longitudinal MRI studies are rare and the pathogen-esis of the abnormalities observed in the early and in thelater stages is still poorly understood [1–3].
0387-7604/$ - see front matter � 2006 Elsevier B.V. All rights reserved.
doi:10.1016/j.braindev.2006.06.005
* Corresponding author. Tel.: +39 049 8218094; fax: +39 0498213509.
E-mail address: [email protected] (A.M. Laverda).
We describe a two-year and nine-month-old childwith HHE syndrome with a neuroradiological and clin-ical follow-up of 8 months.
2. Case report
A two-year and nine-month-old boy was admitted fora prolonged right sided partial motor seizure (45 min)during fever (body temperature 39 �C). Two days afterthe admission he had two similar though shorter convul-sions followed by right hemiparesis. EEG was character-ized by slow and low amplitude electrical activity on theleft hemisphere. Cranial computed tomography (CT)(third day) showed signs of unilateral cerebral edema.A MRI of 7 days later showed on T2-weighted imagesa diffuse swelling of the left cerebral hemisphere and
110 I. Toldo et al. / Brain & Development 29 (2007) 109–111
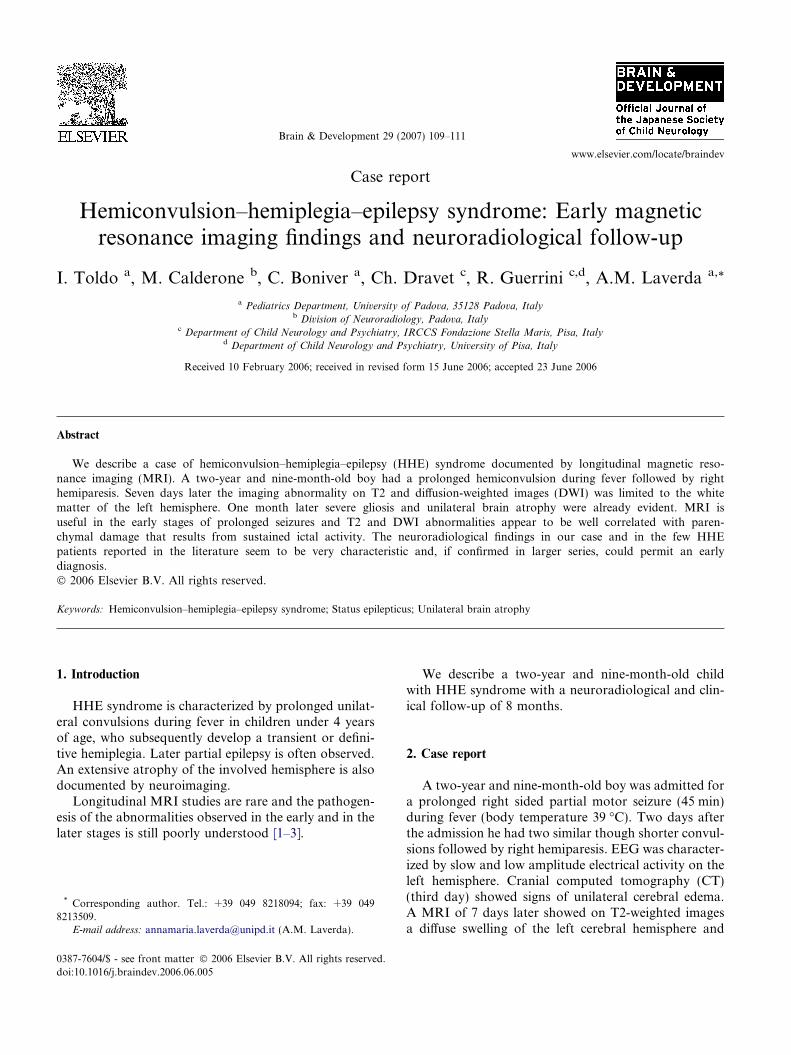
signal hyperintensity of the whole left cerebral hemi-sphere predominantly involving the subcortical U-fibersboth on T2 and DWI (Figs. 1 and 2) with reduction ofthe apparent diffusion coefficient (ADC). MRI-angiog-raphy (MRA) was normal. Urinary organic acid, plas-ma amino acids, blood lactate and ammoniaconcentrations were normal. CSF analysis revealed nor-mal protein, glucose and lactate levels. No infectiousagent was isolated after extensive investigation. Onemonth later T2 hyperintensity was increased and severegliosis and unilateral brain atrophy were already evident(Fig. 3). After 8 months the child is seizure-free undermedication (Carbamazepine) and has a slight righthemiparesis. MRI shows a marked left cerebral atrophypredominantly involving the temporal-parietal-occipital white matter; signal hyperintensity on DWIdisappeared.
Fig. 2. Axial DWI (7 days from the onset): hyperintensity of the whitematter of the left hemisphere predominantly involving the subcorticalU-fibers.
3. Discussion
MRI findings in the few HHE patients reported in theliterature seem to be very peculiar. Early stages are char-acterised by T2 and DWI hyperintensity and reducedADC involving predominantly the subcortical whitematter of the affected hemisphere.
These alterations, that usually disappear in about 1month [1–3], correlate with the neuropathological find-
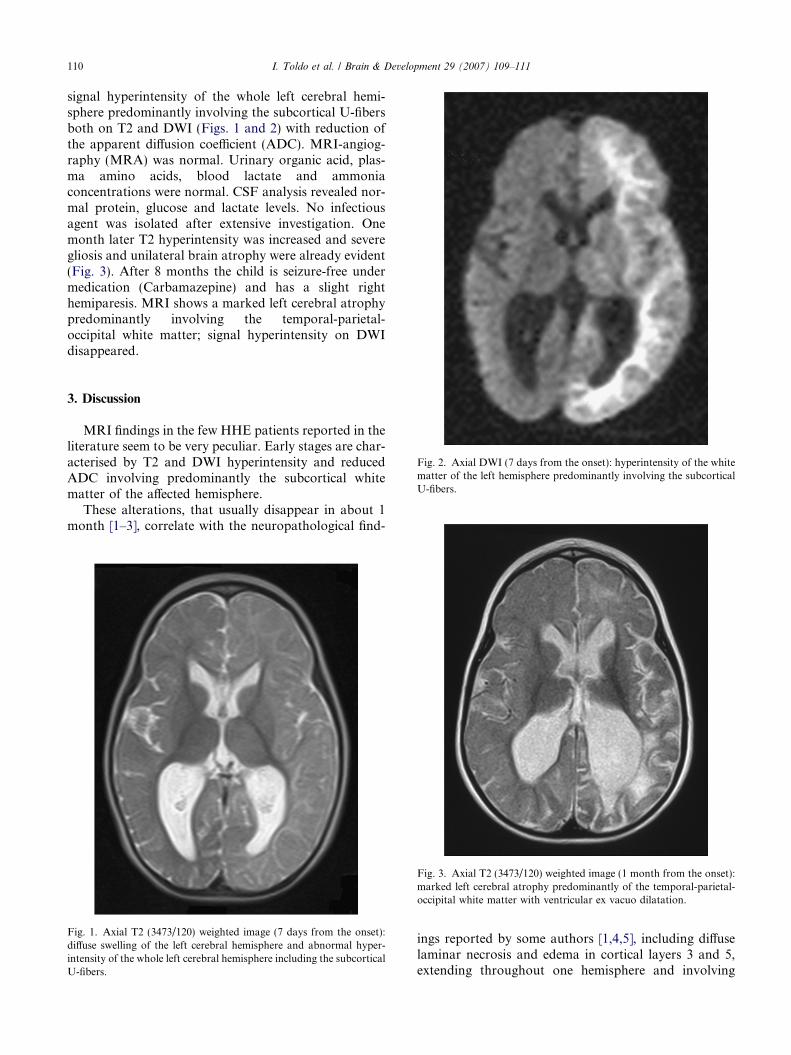
Fig. 1. Axial T2 (3473/120) weighted image (7 days from the onset):diffuse swelling of the left cerebral hemisphere and abnormal hyper-intensity of the whole left cerebral hemisphere including the subcorticalU-fibers.
Fig. 3. Axial T2 (3473/120) weighted image (1 month from the onset):marked left cerebral atrophy predominantly of the temporal-parietal-occipital white matter with ventricular ex vacuo dilatation.
ings reported by some authors [1,4,5], including diffuselaminar necrosis and edema in cortical layers 3 and 5,extending throughout one hemisphere and involving

I. Toldo et al. / Brain & Development 29 (2007) 109–111 111
the hippocampus. The evolution is towards a diffuse uni-lateral cortical and subcortical atrophy [1–3,5–9].
These neuroradiological features differ from thoseobserved in the acute phase of partial status epilepticus,in which T2 and DWI hyperintensity is more localized,unilateral or bilateral and disappears after a few days[10]. In some cases, transient edema can be followedby neuropathological findings of neuronal loss and glio-sis. The neuroimaging of HHE differs also from local-ized atrophies observed in ischemic lesions of vascularorigin. In our case a normal MRA ruled out a vascularaetiology.
Four HHE patients with longitudinal MRI investiga-tions have previously been described [1–3]. Furthermoretwo cases, reported by Morimoto [8] and Hisano [9] asepileptic status, showed, in fact, clinical and neuroradio-logical findings consistent with a diagnosis of HHEsyndrome.
Pathogenesis of HHE is still controversial. Someauthors suggest that a primary viral infection couldcause, directly or by proinflammatory cytokines, a cere-brovascular disorder leading to an ischemic lesion,responsible for the hemiconvulsions, the hemiplegiaand the cytotoxic edema [2,3,6]. Other authors [1,8,9]believe that the lesions could be a direct consequenceof the prolonged ictal activity. More convincing hypoth-esis is that iterative seizures can produce brain damageby impairing the neuronal energy metabolism. Someauthors emphasized the role of excitatory aminoacidneurotransmitter toxicity, as demonstrated in experi-mental animal models of status epilepticus (in particularthose triggered by kainic acid) [5].
Neuroradiological studies in HHE patients haveestablished a sequential relation between early repetitiveseizures, brain edema and cortical-subcortical atrophy[5]. However there is no convincing explanation aboutthe mechanisms which determine the early and diffuseinvolvement of the white matter and the unilateralityof the damage observed in HHE syndrome.
Several factors might contribute to the pathogenesisof HHE:
(1) onset of seizures in the first years of life: at thisage, child brain seems to be very prone to theintrahemispheric diffusion of the ictal dischargewhich could explain the T2 and DWI hyperinten-sity of the whole hemisphere and the unilateralityof the damage [5];
(2) convulsions of long duration that may passunnoticed;
(3) impairment of neuronal energy metabolism due tosustained ictal activity;
(4) genetic factors predisposing to prolonged febrileseizures [5];
(5) systemic factors such as hypoxia, hypoglicemia,arterial hypotension and hyperthermia [5].
In our case, among the known risk factors for thedevelopment of HHE, there were young age at presenta-tion and prolonged febrile status epilepticus. The findingof early DWI abnormalities indicating cytotoxic edemaof the epileptic hemisphere supports the idea that pro-longed focal febrile seizures produce or contribute tothe development of brain damage. In fact, unilateralbrain atrophy rapidly develops about 4 weeks after theseizures as documented in our and in the other HHEcases reported in the literature.
Finally, we underline the importance of MRI in chil-dren who experience prolonged seizures, in whom hemi-spheric atrophy underlying HHE can be diagnosedearly. In particular, T2 and DWI abnormalities appearto be well correlated with parenchymal damage thatresults from sustained ictal activity. MRI findings inour case and in the few HHE patients reported in liter-ature seem to be very peculiar and, if confirmed in largerseries, could suggest an early diagnosis.
References
[1] Freeman JL, Coleman LT, Smith LJ, Shield LK. Hemiconvul-sion–hemiplegia–epilepsy syndrome: characteristic early magneticresonance imaging findings. J Child Neurol 2002;17(1):10–6.
[2] Kawada J, Kimura H, Yoshikawa T, Ihira M, Okumura A,Morishima T, et al. Hemiconvulsion–hemiplegia–epilepsy syn-drome and primary human herpesvirus 7 infection. Brain Dev2004;26:412–4.
[3] Wakamoto H, Ohta M, Nakano N. Hypercytokinemia inhemiconvulsion–hemiplegia–epilepsy syndrome associated withdual infection with Varicella zoster virus and Epstein-Barr virus.Neuropediatrics 2002;33:262–5.
[4] Soffer D, Melamed E, Assaf Y, Cotev S. Hemispheric braindamage in unilateral status epilepticus. Ann Neurol1986;20:737–40.
[5] Chauvel P, Dravet Ch. The HHE syndrome. In: Roger J, et al,editors. Epileptic syndromes in infancy, childhood and adoles-cence. 3rd ed. John Libbey; pp. 247–60. [Chapter 17].
[6] Kimura M, Tasaka M, Sejima H, Takusa Y, Ichiyama T,Yamaguchi S. Hemiconvulsion–hemiplegia–epilepsy syndromeand elevated interleukin-6: case report. J Child Neurol2002;17:705–7.
[7] Salih MAM, Kabiraj M, Al-Jarallah AS, Othman S, Palkar V.Hemiconvulsion–hemiplegia–epilepsy syndrome: a clinical, elec-troencephalographic and neuroradiological study. Childs NervSyst 1997;13:257–63.
[8] Morimoto T, Mitsumasa F, Suzuki Y, Kusu M, Kida K.Sequential changes of brain CT and MRI after febrile statusepilepticus in a 6-year-old-girl. Brain Dev 2002;24:190–3.
[9] Hisano T, Ohno M, Egawa T, Takano T, Shimada M. Changes indiffusion-weighted MRI after status epilepticus. Pediatr Neurol2000;22:327–9.
[10] Cole AJ. Status epilepticus and periictal imaging. Epilepsia2004;45:72–7.