Embed Size (px)
Citation preview

LETTERS TO THE EDITOR
Hemispherectomy for Intractable Seizures
SIR-Hemispherectomy has been advocated recently for the control of intractable epilepsy associated with hemimegalencephaly', '. However, it is not clear whether surgery should be performed early, to prevent adverse development of the normal hemisphere, or delayed, to ensure that the sole source of seizures is the abnormal hemisphere. We describe a patient with hemimegalencephaly and intractable seizures, the youngest yet reported to benefit from hemispherectomy.
A boy was born at term, after a normal pregnancy and labour, weighing 3300g. Antenatal cranial ultrasonography at 22 weeks had shown dilatation of the left lateral ventricle, which was confirmed by a repeat ultrasound scan on day one of life. His head circumference lay just above the 98th centile, but physical examination was otherwise normal. A t two days of age he developed frequent, generalised, tonic-clonic seizures, lasting bet ween one and five minutes. Metabolic and TORCH studies (including fresh urine for cytomegalovirus) and cerebrospinal fluid analysis were normal or negative. EEG revealed virtually continuous seizure activity arising from the left hemisphere. CT head scan demonstrated left hemimegalencephaly, left frontal cortical thickening with pachygyria,
prominence of the cortical sulci and dilatation of the left lateral venticle. Between three weeks and four months of age the child continued to have very frequent seizures (generalised tonic- clonic, myoclonic and right-sided clonic), which recurred every 15 to 30 minutes and lasted between one and five minutes.
The following anticonvulsants, used either singly or in combination, had no significant or sustained effect on either the frequency of pattern of the seizures:
carbamazepine, sodium valproate, N
clonazepam, diazepam, chlormethiazole, t-
ACTH, prednisone, vigabatrin (up to a m rn maximum daily dose of 125mgIkg) and
intravenous immunoglobulins. Only m Q' vigabatrin seemed to be of some d 9 benefit. Throughout this three-month
period the patient would bottle- feed e 9 intermittently, but was otherwise
unresponsive; he was profoundly P .- hypotonic, with signs of a mild right 2 hemiparesis. Head growth continued
just above and parallel to the 98th centile. .-
&2 Repeat, prolonged EEG at four s months showed no independent epileptiform activity arising from the right hemisphere. Repeat, non-contrast
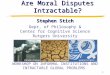
9" head CT was unchanged (Fig. I ) .
B
pyridoxine, phenobarbitone, phenytoin, \o t-
m N
-
-x 0
u
- ... E
A left hemispherectomy was performed at z 4% months of age, leaving intact the basal ganglia. Three myoclonic seizures were observed in the 48 hours following 2 73

Fig. I . Non-contrast CT at 4% months, showing left hemimegalencephaly with frontal cortical thickening, pachygyria and dilatation of left lateral ventricle.
surgery, but none thereafter. The hemiparesis resolved after the operation. Four months post-hemispherectomy he is seizure-free, and is receiving vigabatrin (7Smg/kg/day) and phenobarbitone. He feeds normally, moves all four limbs symmetrically, smiles to voices and is beginning to f ix and follow visual cues. Head growth remains parallel to the 98th centile.
Macroscopically, only the temporal lobe showed gyri and an obvious sulcal pattern. Microscopic examination demonstrated a grossly abnormal neocortex with an almost complete lack of normal neuronal architecture. There was a distinct superficial cortical layer, containing grossly abnormal and giant neurons.
Hemimegalencephaly is characterised clinically by severe epilepsy, psychomotor retardation and hemipare~is‘.~. Our patient developed frequent drug- resistant seizures from the first week of lge, and made no developmental progress. Investigations indicated that the right hemisphere was ‘normal’ and exluded the presence of seizures originating from that hemisphere. A left hemispherectomy was performed to treat intractable epilepsy, and also in the hope of allowing development of higher cortical functions in the right 2 74
hemisphere. Seizures may yet develop in the right hemisphere2; however, the child is currently seizure-free and has made some developmental progress. While it is right to strive for medical control of seizures4, we feel that delaying surgery for too long may limit, or even prevent, psychomotor development.
RICHARD APPLETON* DAVID GARDNER-MEDWIN
DAVID MENDELOW Departments of Paediatrics (Neurology),
Newcastle General Hospital, Westgate Road, Newcastle upon Tyne NE4 6BE. *Child Development Centre, Royal Liverpool Children’s Hospital, Alder Hey, Liverpool L I2 2AP.
and Neurosurgery,
References 1. King, M., Stephenson, J. B. P., Ziervogel, M.,
Doyle, D., Galbraith, S. (1985) ‘Hemimegalen- cephaly-a case for hemispherectomy?’ i euro- pediatrics, 16, 46-55.
2. Vigevano, F., Bertini, E., Boldrini, R., Bosman, C., Claps, D., di Capua, M., di Rocco, C., Rossi, G. F. (1989) ‘Hemimegalencephaly and intractable epilepsy: benefits of hemispher- ectomy.’ Epilepsia, 30, 833-843.
3. Tjiam, A. T., Stefanko, S., Schenk, V. W. D., de Vlieger, M. (1978) ‘Infantile spasms associated with hemihypsarrhythmia and hemimegalen- cephaly.’ Developmental Medicine and Child Neurology, 20, 779-789.
4. Trounce, J. Q., Rutter, N., Mellor, D. H. (1991) ‘Hemimegalencephaly: diagnosis and treatment .’ Developmental Medicine and Child Neurology, 33, 261-266.
How Idiopathic is Idiopathic External Hydrocephalus?
SIR- The report by Cundall et a1 . ’ on identical twins with idiopathic external hydrocephalus and their proposal of a monogenic inheritance of the trait is of particular interest, because it induces refection about the possible pathogenic mechanisms of this clearly hetero- geneous condition. We would like to recount our own observations, with data from the literature relevant to idiopathic external hydrocephalus.
with hypodense subarachnoid fluid collections, we found that only 12 had an uneventful delivery (Table I). In three a primary neonatal subarachnoid
In a series of 3 I macrocephalic infants