Embed Size (px)
DESCRIPTION
algoritm diagnostic hemoragia pulmonara
Citation preview

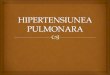
DEFINIŢIE: lichid HEMORAGIC în trahee / hemoragie masivă cu alterarea stării generale(MASIV ≥ 2 lobi)
HEMORAGIA PULMONARĂ
FACTORI DE RISC
IUGR Prematuri PCA VAP SDR Sepsis BHNN Coagulopatii Asfixie severă
SEMNE CLINICE:
debut în ziua 2-4 de viaţă tahicardie apnee, DR ↓SaO2 hTA
DIAGNOSTIC
LABORATOR
AGS: hipoxie, hipercarbie, acidoza respiratorie /mixtăHLG: Hb↓,Ht↓COAGULARE: alterarea factorilor de coagulare
IMAGISTIC
Pulmon OPAC (în totalitate dacă HP estemasivă)
MANAGEMENT DE URGENŢĂ
IOT-VAP PIP>25,PEEP=6-12,TI=0.4-0.5’’
ASPIRARE sânge pe sonda endotraheală (în caz deobstrucţie!)
Adm. ADRENALINA (1/10000)-0.1ml/kgc+0.5ml SF
Transfuzie SÂNGE/PLASMĂ10 ml/kgc
Dacă există hTA/şoc – VOLUM
EXPANDER 10-20 ml/kgc
Vit K CTbPPC
CorectiaACIDOZEI
Autori: Prof. Dr. Maria STAMATIN, Data elaborarii:2010, dupa „Manual de urgente neonatale”, Chisinau 2009

Prescurtari:IUGR – întârziere în creşterea intrauterinăPCA – persistenţa canalului arterialVAP – ventilaţia artificială a pulmonilorSDR – sindrom de detresă respiratorieBHNN – boala hemolitică a nou-născutuluiSaO2 – saturaţia hemoglobinei în oxigenhTA – hipotensiune arterialăAGS – analiza gazelor sanguineHLG – hemoleucogramăPIP – presiune inspiratorie pozitivăPEEP – presiune pozitivă la sfârşitul expiruluiTI – timp inspiratorPPC – plasmă proaspătă congelată
Bibliografie
1. Kaneko M, Watanabe J, Ueno E. Surfactant lavage and replacement in meconium aspirationsyndrome with pulmonary hemorrhage. J Perinat Med 2001;29:351-6
2. Mikawa K, Maekawa N, Nishina K, et al. Improvement of gas exchange following endobronchialinstillation of an exogenous surfactant in an infant with respiratory failure by postoperativepulmonary haemorrhage. Intensive Care Med 1994;20:58-60
3. Pandit PB, Dunn MS, Colucci EA. Surfactant therapy in neonates with respiratory deterioration dueto pulmonary hemorrhage. Pediatrics 1995;95:32-6
4. Raju TN, Langenberg P. Pulmonary hemorrhage and exogenous surfactant therapy: a metaanalysis. JPediatr 1993;123:603-10
5. Al Kharfy TM. High-frequency ventilation in the management of very-low-birth-weight infants withpulmonary hemorrhage. Am J Perinatol 2004;21:19-26 Bhandari V, Gagnon C, Rosenkrantz T, et al.Pulmonary hemorrhage in neonates of early and late gestation. J Perinat Med 1999;369-75
6. Dearborn DG, Smith PG, Dahms BB, et al. Clinical profile of 30 infants with acute pulmonaryhemorrhage in Cleveland. Pediatrics 2002;110:627-37
7. Ko, SY, Chang YS, Park WS. Massive pulmonary hemorrhage in newborn infants successfullytreated with high frequency oscillatory ventilation. J Korean Med Sci 1998;13:495-9
8. Pappas MD, Sarnaik AP, Meert KL, et al. Idiopathic pulmonary hemorrhage in infancy: clinicalfeatures and management with high frequency ventilation. Chest 1996;110:553-5
9. Trompeter R, Yu VY, Aynsley-Green A, Roberton NR. Massive pulmonary haemorrhage in thenewborn infant. Arch Dis Child 1975;50:123-7
10. Bland RD. Edema formation in the newborn lung. Clin Perinatol, 1982;9:593-61111. Greenough A, Roberton NR. Acute respiratory disease in the newborn. In: Rennie JM, Roberton NR
(eds). Textbook of neonatology, 3rd
ed. Edinburgh: Churchill Livingstone, 1999. p55212. Pandit PB, O’Brien K, Asztalos E, et al. Outcome following pulmonary haemorrhage in very low
birthweight neonates treated with surfactant. Arch Dis Child Fetal Neonatal Ed 1999;81:F40-413. Soll RF. Prophylactic synthetic surfactant for preventing morbidity and mortality in preterm infants.
The Cochrane Database of Systematic Reviews 1998, Issue 2. Art. No.: CD001079