Embed Size (px)
Citation preview
ORIGINAL CONTRIBUTION cardiopulmonary resuscitation, complication; gastric tear, from CPR; gastrointestinal bleeding, from CPR
Hemorrhage from Gastric Mucosal Tears Complicating Cardiopulmonary Resuscitation
We observed at autopsy two patients in whom clinically significant gastroin- testinal bleeding occurred from gastric mucosal tears following closed chest cardiac massage. Review of autopsy files showed that, when the Mallory- Weiss syndrome is excluded, linear mucosal tears along the lesser curvature of the stomach occur in about 2% of patients given cardiopulmonary resus- citation; similar lesions have not been observed in patients not subjected to resuscitation. The localization of the tears along the lesser curvature of the stomach is probably the consequence of the catenoidal configuration of thai region. The importance of the mucosal tears lies in their propensity to hem- orrhage if resuscitation is successful. [McDonnell PJ, Hutchins GM, Hruban RH, Brown CG: Hemorrhage from gastric mucosal tears complicating car- diopulmonary resuscitation. Ann Emerg Med April 1984;13:230-233.]
INTRODUCTION Since the introduction of mouth-to-mouth resuscitation by Safar in 1958,1
and dosed chest cardiac massage by Kouwenhoven et al in 1960, 2 these tech- niques have to a great extent replaced thoracotomy and open chest cardiac massage in the management of sudden circulatory arrest. Findings at autopsy that have been interpreted as complications of closed chest massage include rib and stemal fractures, hemothorax, hemopericardium, ruptured liver and spleen, and bone marrow emboli.a Tears or lacerations of the gastric mucosa also have been reported.4, s
We recently observed at autopsy two patients in whom clinically signifi- cant gastrointestinal hemorrhage originated from gastric tears. We examined the frequency and specificity of thiS complication of closed chest massage, and we suggest a mechanism for its development.
NATERIALS A N D M E T H O D S The autopsy files of The Johns Hopkins Hospital were reviewed to identify
patients found at autopsy to have tears or lacerations of the gastric mucosa. The clinical summaries and gross and microscopic findings were reviewed. Patients were excluded if they had a history of alcohol abuse and/or vomiting that might put them at risk for development of Mallory-Weiss tears. To as- sess the frequency of this lesion, we reviewed 125 consecutive autopsies per- formed during 1960 and 1961 in which the patient had undergone cardiopul- monary resuscitation (CPR), and compared them with 125 consecutive autopsies performed during 1980 and 1981 in which an attempt had been made to resuscitate the patient. To assess the specificity of gastric mucosal tears for resuscitation-related trauma, we reviewed the anatomical findings of 10,000 consecutive autopsies performed prior to 1960 (the advent of closed chest CPR).
RESULTS Patient Profile
We identified 20 patients who had one or more linear mucosal tears along the lesser curvature of the stomach. In every instance the patient had been subjected to closed chest cardiac massage. The patients ranged in age from 32 to 79 years {average, 61); seven were women. The underlying illness in six patients was myocardial irdarction; pulmonary emboli, pulmonary edema,
Peter J McDonnell, MD* Grover M Hutchins, MD* Ralph H Hruban* Charles G Brown, MDt Baltimore, Maryland
From the Departments of Pathology* and Emergency Medicine,l The Johns Hopkins Medical Institutions, Baltimore, Maryland.
Received for publication August 22, 1983. Revision received December 5, 1983. Accepted for publication December 20, 1983.
Supported by NIH Grants HL-17655 from The National Heart, Lung and Blood Institute and LM-03651 from The National Library of Medicine.
Address for reprints: Grover M Hutchins, MD, Department of Pathology, The Johns Hopkins Hospital, 600 North Wolfe Street, Baltimore, Maryland 21205.
13:4 April 1984 Annals of Emergency Medicine 230/29
GASTRIC MUCOSAL TEARS McDonnell et al
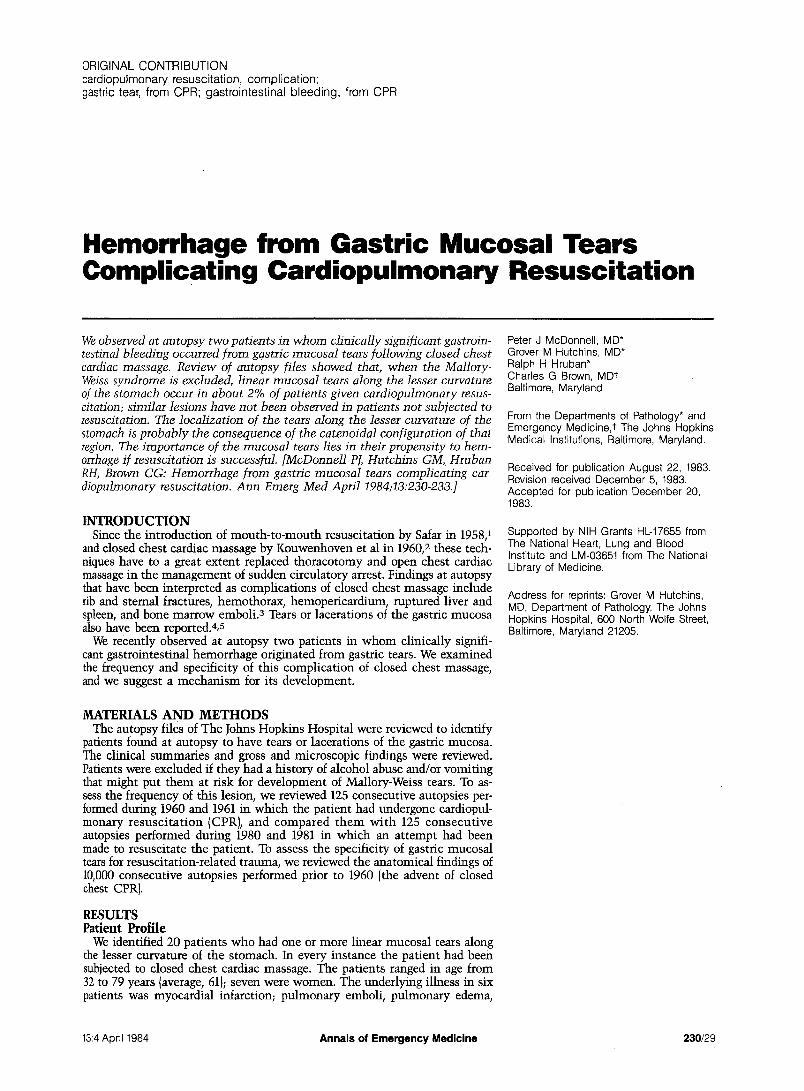
Fig. 1. A. Linear gastric mucosal tears along the lesser curvature of the stom- ach. The esophagus is above and the pyloric area is below. B and C. Trans- verse sections of linear gastric tears along the lesser curvature of the stom- ach. The lacerations ex tend only through the mucosa and are associ- ated with variable amounts of hemor- rhage (both hematoxylin and eosin, x 2o).
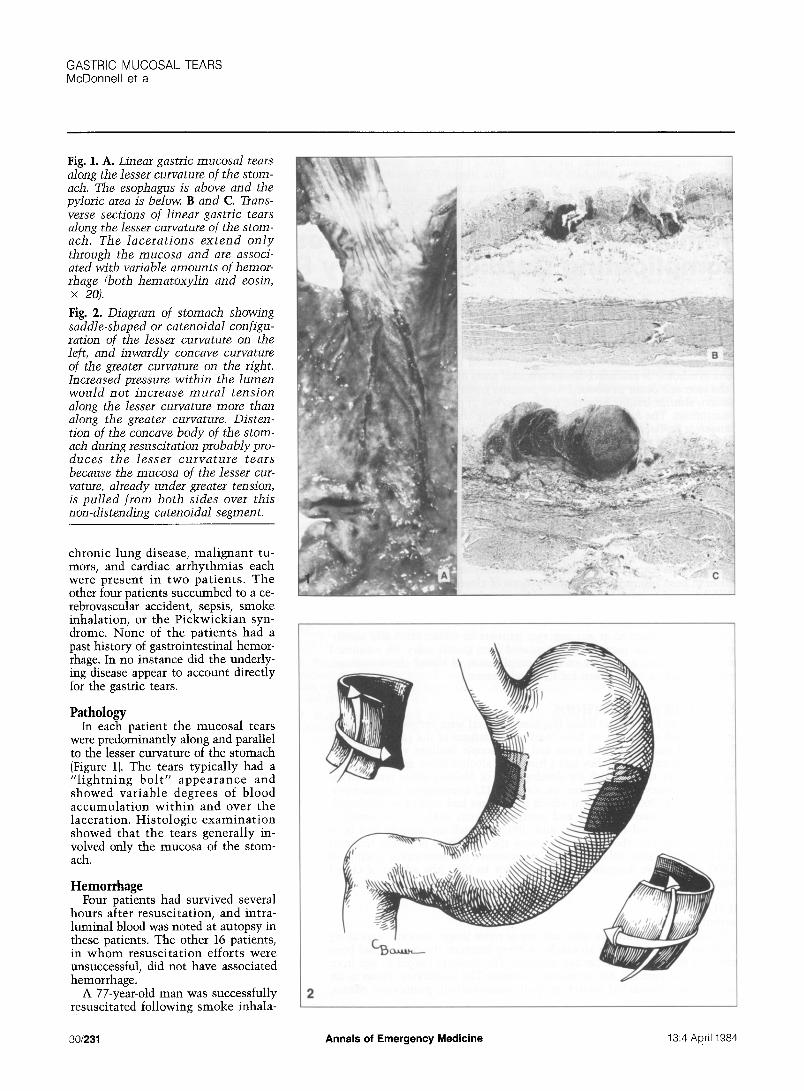
Fig. 2. Diagram of stomach showing saddle-shaped or catenoidal configu- ration of the lesser curvature on the left, and inwardly concave curvature of the greater curvature on the right. Increased pressure within the lumen would not increase mural tension along the lesser curvature more than along the greater curvature. Disten- tion of the concave body of the stom- ach during resuscitation probably pro- duces the lesser curvature tears because the mucosa of the lesser cur- vature, already under greater tension, is pulled from both sides over this non-ddstending catenoidal segment.
chronic lung disease, malignant tu- mors, and cardiac arrhythmias each were present in two patients . The other four patients succumbed to a ce- rebrovascular accident, sepsis, smoke inhalation, or the Pickwickian syn- drome. None of the patients had a past history of gastrointestinal hemor- rhage. In no instance did the underly- ing disease appear to account directly for the gastric tears.
Pathology In each patient the mucosal tears
were predominantly along and parallel to the lesser curvature of the stomach (Figure 1). The tears typically had a " l ightn ing bo l t " appearance and showed variable degrees of blood accumulat ion wi th in and over the laceration. Histologic examina t ion showed that the tears generally in- volved only the mucosa of the stom- ach.
Hemorrhage Four patients had survived several
hours after resuscitation, and intra- luminal blood was noted at autopsy in these patients. The other 16 patients, in whom resuscitation efforts were unsuccessful, did not have associated hemorrhage.
A 77-year-old man was successfully resuscitated following smoke inhala-
30/231 Annals of Emergency Medicine 13:4 April 1984

tion. Several hours later, a marked drop in hematocrit was noted and the patient died from complications of up- per gastrointestinal hemorrhage. At autopsy' he was found to have bled from a tear in the mucosa of the stom- ach.
Another patient seen here recently was successfully resuscitated and two days later underwent esophagogastro- duodenoscopy for evaluation of per- sistent upper gastrointestinal hemor- rhage. The endoscopist described a large mass on the lesser curvature of the stomach and diagnosed a probable fungating gastric carcinoma. Repeat endoscopy one week later, however, showed only a small organizing clot. The patient died of a cardiac arrhyth- mia one week later. At autopsy the le- sion had healed almost completely. In retrospect, awareness of the occur- rence of gastric mucosal tears follow- ing resuscitation would have allowed the endoscopist to suspect the correct diagnosis initially.
Frequency To determine whether the frequen-
cy of gastric mucosal tears as a corn* plication of resuscitation has changed over the years, we reviewed groups of patients resuscitated when the pro- cedure was first developed and com- pared them to current experience. Among the 125 patients receiving closed chest cardiac massage in 1960 or 1961, three (2.4%) had l inear mucosal tears along the lesser curva- ture of the stomach. Similarly among 125 consecutive autopsies performed during 1980 or 1981, two patients (1.6%) had the lesion. Thus these le- sions were seen, albeit infrequently, both at the time of origin of closed chest cardiac resuscitation and cur- rently. It appears reasonable to expect that approximately one patient in 50 will develop gastric tears and be at risk for hemorrhage following success- ful resuscitation.
Specificity The autopsy index revealed no pa-
tients in whom gastric mucosal tears were not associated with closed chest cardiac massage. However, excluded were four patients in whom the clini- cal and autopsy findings were charac- teristic of the Mallory-Weiss syn- drome. In each of these four patients there was a history of alcoholism and vomiting, and at autopsy there were lacerations at the gastroesophageal junction. Our review included more
than 25,000 patients autopsied be- tween 1943 and 1983.
DISCUSSION We concluded that linear tears of
the gastric mucosa along the lesser curvature represent a consequence of trauma related to closed chest cardio- pulmonary resuscitation. Autopsy re- vealed the lesion to be present in ap- proximately 2% of patients who had undergone CPR. Not one example of this lesion could be found among pa- tients not subjected to closed chest cardiac massage.
Gastric rupture occurring during ex- ternal cardiac resuscitation was first described by Demos and Poticha in 1964. 6 In 1967 Lundberg7 first reported the occurrence of gastric lacerations with associated gastrointestinal bleed- ing in patients not surviving CPR. Since these initial reports, several cases of gastric rupture or laceration have been described. 8-1z Anthony lz and Lundberg 7 found the incidence of gastric mucosal lacerations at autopsy to be 10% to 12% in patients not sur- viving cardiopulmonary resuscitation. The potentially fatal nature of these lacerations was demonstrated by Ag- uilarlO when he described a patient who died from gastric hemorrhage secondary to gastric mucosal lacera- tions caused by CPR.
If the trachea is not intubated, mouth-to-mouth resuscitation may lead to inflation of the stomach. Safari demonstrated that gastric distention of one to two liters can occur during mouth-to-mouth breathing. He noted that improper support of the jaw and excessively high inflation pressures contributed to the production of gas- tric distention. Gastric distention can, in turn, produce gastric mucosal lac- erations. Lion-Cacheg 3 produced gas- tric mucosa l tears by dis tending cadaver stomachs with water. At- kinson 14 distended cadaver stomachs with air and found gastric tears in one of five distended at 100 mm Hg and in all six distended at 150 mm Hg. The combination of forceful mouth-to- mouth breathing and chest compres- sion could generate pressures suffi- cient to cause gastric mucosal tears.
The pathogenesis of these lesions and their constant location apparently reflect a susceptibility of the gastric mucosa of the lesser curvature to the trauma of resuscitation. One possible explanation relates to the catenoidal configuration of the stomach at this site (Figure 2). A catenoid is a saddle-
shaped surface with the property that every point has mutually perpendicu- lar curvatures that are equal and op- posite, ie, each point has a net zero curvature. The effect of such a config- uration of the stomach, with slight net curvature in terms of the Laplace equation (pressure equals tension times curvature) would be that an in- traluminal pressure increase would produce a marked effect on mural ten- sion. In contrast, the remainder of the stomach body is inwardly concave. Smaller increases in mural tension and stretching of these concave re- gions would be produced by increased luminal pressure. Presumably stretch- ing of the mucosa over the non-chang- ing lesser curvature by the expansion of the body of the stomach produces the mucosal tears.
The importance of this lesion re- lates to the possibility of significant gastrointestinal hemorrhage after suc- cessful resuscitation. The following techniques have been suggested to minimize the incidence of gastric mucosal laceration during cardiopul- monary resuscitation:ha,is 1) early tra- cheal intubation, 2) gastric decompres- sion by nasogastric suction, 3) lower insufflation pressures, 4) proper posi- tioning of the patient's head, and 5) not pressing the patient's upper abdo- men. It may be expected that abdomi- nal binding, if performed at or near the onset of resuscitation, could mini- mize gastric distention by maintain- ing constant intra-abdominal pressure.
In a study conducted at our institu- tion} 6 no abdominal visceral injury was found at autopsy i n six patients who had undergone abdominal bind- ing as part of cardiopulmonary resus- citation. Binder pressure was limited to 110 cm HzO and the number of pa- tients was small. We hope that autop- sies on such patients in the future will establish whether abdominal binding affects the development of gastric mucosal tears.
REFERENCES 1. Safar P: Ventilatory efficacy of mouth- to-mouth artificial respiration. JAMA 1958;167:335-341.
2. Kouwenhoven WB, Jude JR. Knicker- bocker GG: Closed-chest cardiac mas- sage. JAMA 1960~173:1064-1067.
3. Baringer JR, Salzman EW, Jones WA, et ah External cardiac massage. N Engl J Med I961;265:62-65.
4. Clark DT: Complications following closed chest cardiac massage. JAMA 1962;18h337-338.
13:4 April 1984 Annals of Emergency Medicine 232/31

GASTRIC MUCOSAL TEARS McDonnell et al
5. Morgan RR: Laceration of the liver from closed-chest cardiac massage. N Engl J Med 1961;265:82-83.
6. Demos NJ, Poticha SM: Gastric rup- ture occurring during external cardiac re- suscitation. Surgery 1964;55:364-366.
7. Lundberg GD, Mattei IR, Davis CJ, et al: Hemorrhage from gastroesophageal lacerations following closed-chest cardiac massage. JAMA 1967;202:123-126.
8. McGrath RB: Gastroesophageal lacera- tions. A fatal complication of closed chest cardiopulmonary resusci tat ion. Chest 1983;83:571-572.
9. Matikainen M: Rupture of the stom- ach: A rare complication of resuscitation. Acta Chir Scand 1978;144:61-62.
10. Aguilar JC: Fatal gastric hemorrhage: A complication of cardiorespiratory resus- citation. J Trauma 1981;21:573-575.
11. Darke SG, Bloomfield E: Case of com- plete gastric rupture complicating resusci- tation. Br Med J 1975;3:414-415.
12. Anthony PP, Tattersfield AE: Gastric mucosal lacerations after cardiac resusci- tation. Br Heart J 1969;31:72-75.
13. Lion-Cachet J: Gastric fundal mucosal
tears. Br J Surgery 1963;50:985-986.
14. Atkinson M, Bottrill MB, Edwards AT, et al: Mucosal tears at the oesophagogas- tric junction (the Mallory-Weiss syn- drome). Gut 1961;2:1-11.
15. Valtonen EJ, Hakola N: Rupture of the normal stomach during mouth-to-mouth resuscitation. Report of a case. Acta Chit Scand 1964;127:427-431.
16. Chandra N, Snyder LD, Weisfeldt ML: Abdominal binding during cardiopulmo- nary resuscitation in man. JAMA 1981; 246:351-353.
American Board of Emergency Medicine Notice On June 30, 1988, the practice option will terminate for those physicians wishing to meet the credential requirements of the American Board of Emergency Medicine's certification examination. Practice, teaching, or CME accumulated after the above date may not be used to satisfy the practice requirements. Questions should be directed to ABEM, 200 Woodland Pass, Suite D, East Lansing, MI 48823; 517/332-4800.
Application materials for the 1984 cycle of the American Board of Emergency Medicine certifying examinat ion will be distributed in April 1984. Applications for the 1984 cycle will be accepted wi th postmark dates of May 1 through July 15, 1984. For further information, contact ABEM.
32/233 Annals of Emergency Medicine 13:4 April-1984





























