Embed Size (px)
Citation preview

Disorders of Disorders of coagulation and coagulation and anticoagulantsanticoagulants
Dr.Somit jainDr.Somit jain
Department of PeriodonticsDepartment of Periodontics

ContentsContents
IntroductionIntroduction HemostasisHemostasis Clotting factorsClotting factors Cascade of clottingCascade of clotting Disorders of bleeding and clottingDisorders of bleeding and clotting Laboratory investigationsLaboratory investigations AnticoagulantsAnticoagulants Periodontal considerationsPeriodontal considerations References References

IntroductionIntroduction
Vertebrates have evolved complex Vertebrates have evolved complex mechanisms to stem hemorrhage mechanisms to stem hemorrhage after injury.after injury.
Failure of the hemostatic Failure of the hemostatic mechanisms may lead to fatal mechanisms may lead to fatal exsanguination. exsanguination.
Any surgical procedure presents a Any surgical procedure presents a severe challenge to the body’s severe challenge to the body’s hemostatic mechanism. hemostatic mechanism.

HEMOSTASISHEMOSTASIS
Normal hemostasis results from well Normal hemostasis results from well regulated processes that maintain regulated processes that maintain blood in a fluid,clot free state in blood in a fluid,clot free state in normal vessels while inducing the normal vessels while inducing the rapid formation of hemostatic plug at rapid formation of hemostatic plug at the site of vascular injury.the site of vascular injury.
Dependent on the vascular Dependent on the vascular wall,platelets and the coagulation wall,platelets and the coagulation cascade. cascade.

NORMAL HEMOSTASISNORMAL HEMOSTASISHemostasis, a complex process, can be divided Hemostasis, a complex process, can be divided
intointo Four important steps: Four important steps:
1. 1. Vasoconstriction due to local myogenic spasm, local Vasoconstriction due to local myogenic spasm, local neural response, and release of endothelin from the neural response, and release of endothelin from the endotheliumendothelium
2.2.Primary hemostatic plug: due to platelet adhesion, Primary hemostatic plug: due to platelet adhesion, activation, RELEASE REACTION or degranulation (ADP, activation, RELEASE REACTION or degranulation (ADP, TXA2) and recruitment of other plateletsTXA2) and recruitment of other platelets
3.3.Secondary hemostasis due to activation of coagulation Secondary hemostasis due to activation of coagulation cascade by tissue factor and phospholipid via extrinsic cascade by tissue factor and phospholipid via extrinsic pathway- the end result being fibrin which traps the cells in pathway- the end result being fibrin which traps the cells in the blood forming a clotthe blood forming a clot
4. Clot organization/ Clot retractions4. Clot organization/ Clot retractions

Vascular phaseVascular phase
Vasoconstriction in area of injuryVasoconstriction in area of injuryBegins immediately after injuryBegins immediately after injury


Primary hemostasisPrimary hemostasis
Platelet adhesionPlatelet adhesion
Platelet aggregationPlatelet aggregation
Platelet plug formationPlatelet plug formation


Secondary haemostasisSecondary haemostasis(Coagulation of Blood)(Coagulation of Blood)
Involves activation of clotting process in plasma, Involves activation of clotting process in plasma, resulting in fibrin formationresulting in fibrin formation
Important to stop bleeding from large vessels. Important to stop bleeding from large vessels.
It comprises three separate though related systems It comprises three separate though related systems
Coagulation systemCoagulation system The coagulation inhibitory systemThe coagulation inhibitory system Fibrinolytic systemFibrinolytic system
Pathological disturbances may occur in any or Pathological disturbances may occur in any or more of these systems and lead to bleeding more of these systems and lead to bleeding tendency or intravascular coagulationtendency or intravascular coagulation



MECHNISM OF BLOOD MECHNISM OF BLOOD COAGULATIONCOAGULATION
In the blood stream anticoagulants In the blood stream anticoagulants normally predominate, so that the normally predominate, so that the blood does not coagulate while it is blood does not coagulate while it is circulating in the blood vesselscirculating in the blood vessels
When the blood vessel is ruptured, When the blood vessel is ruptured, procoagulants from the area of procoagulants from the area of tissue damage become activated tissue damage become activated and override the anticoagulants and and override the anticoagulants and then clot does developthen clot does develop

GENERAL MECHANISM
Clotting takes place in 3 essential steps-
1. Formation of prothrombin activator 2. Conversion of Prothrombin to thrombin 3. Conversion of Fibrinogen to fibrin

Formation of prothrombin Formation of prothrombin activatoractivator
The mechanism sets in to play byThe mechanism sets in to play by
1.1.Trauma to the vascular wall & adjacent tissueTrauma to the vascular wall & adjacent tissue
2.2.Trauma to the blood Trauma to the blood
3.3.Contact of the blood with the damaged Contact of the blood with the damaged endothelial cells or with collagen & other tissue endothelial cells or with collagen & other tissue elements outside the blood vesselelements outside the blood vessel
Each instance leads to the formation of Each instance leads to the formation of prothrombin activatorprothrombin activator

Prothrombin Activator generally formed in Prothrombin Activator generally formed in two ways & interact constantly with each two ways & interact constantly with each
other.other.Both the pathways occur simultaneouslyBoth the pathways occur simultaneously
EXTRINSIC PATHWAYEXTRINSIC PATHWAY ExplosiveExplosive With severe trauma With severe trauma
clotting occurs in 15 clotting occurs in 15 secsec
Begins with trauma to Begins with trauma to the vascular wall and the vascular wall and surrounding tissuesurrounding tissue
INTRINSIC PATHWAYINTRINSIC PATHWAY Much slowerMuch slower Clotting occurs inClotting occurs in
1- 6min1- 6min
Begins in the blood Begins in the blood itself or exposure of itself or exposure of the blood to the the blood to the collagen from the collagen from the traumatised blood traumatised blood vessel wallvessel wall

Extrinsic pathwayExtrinsic pathwayThe release of Tissue Factor or Tissue The release of Tissue Factor or Tissue
Thromboplastin (Composed of Thromboplastin (Composed of Phospholipid from the membrane of Phospholipid from the membrane of the tissue plus lipoprotien complex)the tissue plus lipoprotien complex)
Activation of factor X.Activation of factor X.Effect of activated factor X to form Effect of activated factor X to form
Prothrombin activatorProthrombin activator

EXTRINSIC PATHWAYEXTRINSIC PATHWAY

INTRINSIC PATHWAYINTRINSIC PATHWAY Activation of factor XII Activation of factor XII
1.Trauma 1.Trauma
Release of plateletRelease of platelet
PhospholipidPhospholipid
2.Activation of factor XI2.Activation of factor XI
3.Activation factor IX - by activated factor 3.Activation factor IX - by activated factor XIXI
4.Activation factor X – Role of factor VIII4.Activation factor X – Role of factor VIII
5. Activation of activated X to form 5. Activation of activated X to form Prothrombin activator – Role of factor VProthrombin activator – Role of factor V

INTRINSIC PATHWAYINTRINSIC PATHWAY

COMMON PATHWAYCOMMON PATHWAY


CLOT RETRACTIONCLOT RETRACTION
Once the fibrin meshwork has appeared, RBCs & platelets stick to the fibrin strands.
The platelets then contract and the clot undergoes clot retraction which:Pulls the torn edges of the vessel closer
together, reducing residual bleeding and stabilizing the injury site
Reduces the size of the injured area, making it easier for fibroblasts, smooth muscle cells, and endothelial cells to complete repairs

Fibrinolytic systemFibrinolytic system

Principles underlying coagulation tests Test Principle Causes of abnormality
Blood clotting time Contact activation by glass tube
Deficiency of intrinsic pathway
Partial thromboplastin time
Intrinsic pathway activated by kaolin
Deficiency of factors-XII,IX,XI,X,V,VIII
Prothrombin time Extrinsic pathway activated by brain tissue.
Deficiency of factors-VII,X,V,
Thrombin time Fibrinogen is converted to fibrin by added thrombin
Deficiency of fibrinogen or high level of FDPs
Bleeding time Duration of bleeding from skin puncture is timed
Defect in platelets

LABORATORY TEST FOR ASSESSING LABORATORY TEST FOR ASSESSING HEMOSTASISHEMOSTASIS
TEST Normal RangeTEST Normal Range Platelet count 150,000 to 450,000/mm3Platelet count 150,000 to 450,000/mm3 Bleeding time < 7 min (by simplate); 1–6 min (modifiedBleeding time < 7 min (by simplate); 1–6 min (modified
Ivy’s test)Ivy’s test) Prothrombin time/international Control ± 1 s (eg, PT: 11–Prothrombin time/international Control ± 1 s (eg, PT: 11–
13 13
normalized ratio s/INR 1.0normalized ratio s/INR 1.0 Activated partial thromboplastin time Comparable to Activated partial thromboplastin time Comparable to
control control
( eg 15-35 s )( eg 15-35 s ) Thrombin time Control ± 3 s (eg, 9–13 s)Thrombin time Control ± 3 s (eg, 9–13 s) Fibrin degradation products < 10 Fibrin degradation products < 10 μμg/dLg/dL Fibrinogen assay 200–400 mg/dLFibrinogen assay 200–400 mg/dL von Willebrand’s antigen 60–150% vWF activityvon Willebrand’s antigen 60–150% vWF activity Coagulation factor assays 60-100% F VIII (eg Coagulation factor assays 60-100% F VIII (eg
F VIII assay) activityF VIII assay) activity

ASSESSMENT OF A PATIENT WITHASSESSMENT OF A PATIENT WITHPOSSIBLE BLEEDING DISORDERPOSSIBLE BLEEDING DISORDER
· Clinical history· Clinical history
· Physical examination· Physical examination
· Lab investigations· Lab investigations

PRE-OPERATIVE EVALUATIONPRE-OPERATIVE EVALUATION
HISTORYHISTORY Prolonged bleeding after trauma/dental Prolonged bleeding after trauma/dental
extractionextraction MedicationsMedications Bruises without apparent injuryBruises without apparent injury Excessive menstrual bleedingExcessive menstrual bleeding Relatives with bleeding problemsRelatives with bleeding problems Bleeding problems associated with Bleeding problems associated with
major/minor surgerymajor/minor surgery

CLASSIFICATION OF BLEEDING CLASSIFICATION OF BLEEDING DISORDERSDISORDERS
1. VASCULAR DISORDERS1. VASCULAR DISORDERS
CongenitalCongenital Heriditary hemorrhagic telangiectasiaHeriditary hemorrhagic telangiectasia Ehler – Danlos syndromeEhler – Danlos syndrome
AcquiredAcquired
Henoch schonein purpuraHenoch schonein purpura Easy bruishing purpuraEasy bruishing purpura Senile purpura Senile purpura Factitial purpuraFactitial purpura ScurvyScurvy Severe infectionSevere infection Drugs Drugs

QUALITATIVE DISORDERS OF QUALITATIVE DISORDERS OF PLATELETSPLATELETS
1) Disorders of “adhesion”1) Disorders of “adhesion” Congenital - Bernard soulier syndrome Congenital - Bernard soulier syndrome Acquired - Uremia Acquired - Uremia
2) Disorders of “aggregation”2) Disorders of “aggregation” Congenital - Thrombasthenia Congenital - Thrombasthenia Acquired - Drugs Acquired - Drugs
- Para proteinemia - Para proteinemia
3) Disorders of platelet secretion3) Disorders of platelet secretion Congenital - Storage pool disease Congenital - Storage pool disease Acquired - Myeloproliferative disorder Acquired - Myeloproliferative disorder

Quantitative Disorders Of PlateletsQuantitative Disorders Of PlateletsTHROMBOCYTOPENIAS THROMBOCYTOPENIAS
1) Production of platelets1) Production of platelets HypoplasiaHypoplasia - Idiopathic- Idiopathic
- Drugs- DrugsInfiltrationInfiltration - Carcinoma- Carcinoma - Leukemia- Leukemia - Myeloma- Myeloma - Myelofibrosis- MyelofibrosisNutritional deficiencyNutritional deficiency - Iron- Iron - B12 / Folate - B12 / Folate

2) Consumption of platelets2) Consumption of platelets Immune Immune
- ITP- ITP- Sec.immune - Sec.immune
thrombocytopenia thrombocytopenia- Post transfusion purpura- Post transfusion purpura
CoagulationCoagulation- DIC- DIC- Gram – ve septicemia - Gram – ve septicemia
3) Sequestration of platelets3) Sequestration of platelets - Hypersplenism- Hypersplenism
4) Loss of platelets4) Loss of platelets- Hemorrhage- Hemorrhage- Massive transfusion - Massive transfusion
of stored blood of stored blood- Hemodialysis- Hemodialysis

COAGULATION DISORDERSCOAGULATION DISORDERS
Classification of Coagulation Classification of Coagulation Disorders:Disorders:
• • Acquired – Usually multiple factors Acquired – Usually multiple factors are involvedare involved
• • Hereditary – Usually single factor is Hereditary – Usually single factor is involvedinvolved

Acquired Coagulation Disorders:The followings disorders are associated with acquired coagulation disorders:1. Vitamin K deficiency a. Obstructive jaundice b. Coeliac disease c. Liver disease i. Defective synthesis of coagulation factors (I, II, V, VII, IV and X) ii. Increased fibrinolytic activity iii. Intravascular coagulation2. Anticoagulant drugs3. Disseminated intravascular coagulation4. Active fibrinolysis5. Massive transfusion of stored blood6. Circulating inhibitors of coagulation

Common Hereditary Coagulation Disorders:
1. Hemophilia a. Hemophilia A – Factor VIII deficiency b. Hemophilia B – factor IX deficiency
2. Von-Willebrand disease
3. Other congenital deficiency disorders a. Fibrinogen deficiency b. Factor V deficiency c. Factor XIII

HEMOPHLIA AHEMOPHLIA A X-linked recessive disorder resulting from deficiency of X-linked recessive disorder resulting from deficiency of
factor VIIIfactor VIII Body fails to synthesize this essential globulin due to the Body fails to synthesize this essential globulin due to the
absence of the specific enzyme which is controlled by the absence of the specific enzyme which is controlled by the mutant genemutant gene
Affects males.Affects males. Sons of carriers have 50:50 chance developing hemophilia.Sons of carriers have 50:50 chance developing hemophilia. Daughters of carriers have 50:50 chance of being carriersDaughters of carriers have 50:50 chance of being carriers All daughters of an affected males are carriers but sons are All daughters of an affected males are carriers but sons are
normalnormal Carriers rarely have bleeding tendencyCarriers rarely have bleeding tendency Prevalence of 5 per 100000 of populationPrevalence of 5 per 100000 of population 10 times more common than hemophilia B10 times more common than hemophilia B

The hemophilia gene is carried on the The hemophilia gene is carried on the X X chromosome chromosome in males who lack a normal allele, in males who lack a normal allele,
the defect is manifested by clinical haemophilia. the defect is manifested by clinical haemophilia. Women may be carriersWomen may be carriers

HemophiliaHemophiliaClinical manifestations (hemophilia A & B are
indistinguishable)
Hemarthrosis (most common)Fixed joints
Soft tissue hematomas (e.g., muscle)Muscle atrophyShortened tendons
Other sites of bleedingUrinary tractCNS, neck (may be life-threatening)
Prolonged bleeding after surgery or dental extractions

ORAL MANIFESTATIONSORAL MANIFESTATIONS Hemorrhage from many sites in oral cavity.Hemorrhage from many sites in oral cavity. Gingival bleeding massive and prolonged.Gingival bleeding massive and prolonged. Tooth eruption and exfoliation with severe Tooth eruption and exfoliation with severe
prolonged hemorrhageprolonged hemorrhage Subperiosteal bleeding with reactive new bone Subperiosteal bleeding with reactive new bone
formation causing tumor like expansion of bone formation causing tumor like expansion of bone (MANDIBULAR PSEUDOTUMOR)(MANDIBULAR PSEUDOTUMOR)
Uncontrolled or delayed hemorrhage may result Uncontrolled or delayed hemorrhage may result from SURGICAL EXCISION,DENTAL EXTRACTION, from SURGICAL EXCISION,DENTAL EXTRACTION, PERIODONTAL CURETTAGE.PERIODONTAL CURETTAGE.
Slight trauma may lead to HEMATOMA formation in Slight trauma may lead to HEMATOMA formation in tongue, lip and palate.tongue, lip and palate.
Oropharyngeal bleeding(severe Oropharyngeal bleeding(severe complication)complication)

Haemarthrosis in elderly hemophiliac has Haemarthrosis in elderly hemophiliac has caused crippling arthritiscaused crippling arthritis


Haemophilia – B
(Christmas Disease)Christmas disease is a congenital sex-linked hemorrhagic disorder due to absence, reduction or functional abnormality of factor IX
Incidence
1 per 50,000 male
Clinical features are same as Hemophilia – A
Pathophysiology
Factor IX coagulation activities is reduced or absent.

Level of factor VIIIc activityLevel of factor VIIIc activity Severity of clinical SymptomsSeverity of clinical Symptoms
Normal activity: 50-200%Normal activity: 50-200%
(0.5-2 µg/ml)(0.5-2 µg/ml)
Mild activity : 5-25%Mild activity : 5-25%
(0.05-0.25 µg/ml)(0.05-0.25 µg/ml)
Moderate activity : 1-5%Moderate activity : 1-5%
(0.01-0.05 µg/ml)(0.01-0.05 µg/ml)
Severe activity : <1%Severe activity : <1%
(0.01 µg/ml)(0.01 µg/ml)
Hemorrhage secondary to trauma, Hemorrhage secondary to trauma, surgery and dental extraction.surgery and dental extraction.
Occasional spontaneous bleeding, Occasional spontaneous bleeding, hemarthrosis, musculoskeletal hemarthrosis, musculoskeletal bleeding.bleeding.
Severe spontaneous bleeding since Severe spontaneous bleeding since childhood. Intracranial bleeding, childhood. Intracranial bleeding, bleeding into tongue and frenum, bleeding into tongue and frenum, Bleeding in facial spaces of the neck. Bleeding in facial spaces of the neck.

Replacement therapyReplacement therapy
Infusion of plasma products enriched Infusion of plasma products enriched with factor VIII with factor VIII cryoprecipitate,partially purified cryoprecipitate,partially purified factor VIII concentrate- Lyophilized factor VIII concentrate- Lyophilized powderpowder
Each unit of Factor VIII infused Each unit of Factor VIII infused increases plasma level of recipient increases plasma level of recipient by 2% per Kg of body weight.by 2% per Kg of body weight.

Source of Factor VIIISource of Factor VIII
Fresh whole bloodFresh whole bloodFresh frozen plasmaFresh frozen plasmaCryoprecipitate prepared from Cryoprecipitate prepared from
human plasmahuman plasmaFreeze-dried animal AHGFreeze-dried animal AHGFreeze-dried human AHG Freeze-dried human AHG

PrecautionsPrecautions
Nerve Blocks - avoid if not on replacement Nerve Blocks - avoid if not on replacement therapytherapy
For infiltration no need for cover of antibioticsFor infiltration no need for cover of antibiotics Tranexamic acid Prophylaxis - 10 ml of 4.8% Tranexamic acid Prophylaxis - 10 ml of 4.8%
aqueous solution, QID for 1 week should be aqueous solution, QID for 1 week should be prescribed for patients undergoing regional prescribed for patients undergoing regional blocksblocks
Preventive dental care:Preventive dental care: Use of fluoridesUse of fluorides Fissure sealantsFissure sealants Dietary adviceDietary advice Regular dental checkupsRegular dental checkups

Simple tooth extractionSimple tooth extraction::
Regime IRegime I Regime IIRegime II
1.1. Factor VIII of Factor VIII of between 50-75% between 50-75% is required.is required.
2. Preoperative 2. Preoperative factor VIII, i.vfactor VIII, i.v
3. Tranexamic acid 3. Tranexamic acid 1g (30mg/kg) 1g (30mg/kg) QID start 24 hrs QID start 24 hrs preoperativepreoperative
1. Epsilon Amino 1. Epsilon Amino caproic acid 5-6 caproic acid 5-6 grams every 6grams every 6thth hrly.hrly.
2. Tranexamic acid 2. Tranexamic acid 1gr QID for 10 1gr QID for 10 days.days.
3. If bleeding occurs 3. If bleeding occurs
during this time, a during this time, a
dose of factor VIIIdose of factor VIII
Surgical procedureSurgical procedure

Desmopressin TherapyDesmopressin Therapy
0.3 – 0.5µg/kg i.v just before the surgery, 0.3 – 0.5µg/kg i.v just before the surgery, repeat 12 hrly if necessary for upto 4 days.repeat 12 hrly if necessary for upto 4 days.
Temporary correction of hemostatic Temporary correction of hemostatic defect.defect.
In patients with F VIII inhibitors, it releasesIn patients with F VIII inhibitors, it releases
- Factor VIIIc- Factor VIIIc
- von Willebrands factor- von Willebrands factor
- Tissue plasminogen activator- Tissue plasminogen activator
from endothelial storage.from endothelial storage.

For third molar surgeries For third molar surgeries F VIII replacementF VIII replacement Buccal approach to lower 3rd molarsBuccal approach to lower 3rd molars Minimal amount of bone should be removedMinimal amount of bone should be removed Section teeth for removal whenever possibleSection teeth for removal whenever possible Extraction socket should be packed with:Extraction socket should be packed with:
- Oxidized regenerated cellulose- Oxidized regenerated cellulose- Absorbable gelatin sponge- Absorbable gelatin sponge- Bone wax- Bone wax- Tranexamic acid- Tranexamic acid
Acrylic protective splints on palates.Acrylic protective splints on palates.

For Major SurgeriesFor Major Surgeries
For Major Surgeries:For Major Surgeries:
• Thorough assessment of the patient Thorough assessment of the patient • PT, APTT, Platelet count, Factor VIII PT, APTT, Platelet count, Factor VIII
assay, Fibrinogen estimation, assay, Fibrinogen estimation, Hepatitis B&C, Liver function test, Hepatitis B&C, Liver function test, blood grouping.blood grouping.

Von Willebrand disease/ Von Willebrand disease/ pseudo hemophiliapseudo hemophilia
Most common inherited bleeding disorderMost common inherited bleeding disorder Due to inherited deficiency of vWFDue to inherited deficiency of vWF Affects both males & femalesAffects both males & females Inherited as AUTOSOMAL DOMINANT but severe form Inherited as AUTOSOMAL DOMINANT but severe form
as sex-linked recessive trait like true hemophiliaas sex-linked recessive trait like true hemophilia vWF synthesized in endothelium and megakaryocytesvWF synthesized in endothelium and megakaryocytes Acts as carrier for factor VIII, protecting it from Acts as carrier for factor VIII, protecting it from
proteolytic degradation, thus deficiency lead to low proteolytic degradation, thus deficiency lead to low factor VIII concentrationfactor VIII concentration
Mediates platelet adhesion to damaged endotheliumMediates platelet adhesion to damaged endothelium Mediates platelet aggregation, thus deficiency lead to Mediates platelet aggregation, thus deficiency lead to
defective platelet adhesion, which causes secondary defective platelet adhesion, which causes secondary deficiency in factor VIIIdeficiency in factor VIII

Von Willebrand disease/ pseudo Von Willebrand disease/ pseudo hemophiliahemophilia
Types:Types:
Type I : Quantitative defect, Type I : Quantitative defect, 80%80%Type II : Qualitative defect 20%Type II : Qualitative defect 20%Type III : severe deficiency of Type III : severe deficiency of vWFvWF

Management of Von Willebrand’s Management of Von Willebrand’s diseasedisease
Minor procedureMinor procedure Major procedureMajor procedure
PreoperativePreoperative PostoperativePostoperative PreoperativePreoperative PostoperativePostoperative
Type IType I
DDAVP-0.3µg/kg DDAVP-0.3µg/kg in 50-100cc in 50-100cc
normal saline normal saline over 20-30 mins. over 20-30 mins.
1 hour before 1 hour before surgerysurgery
OROR
Repeat every day Repeat every day for 2-3 days after for 2-3 days after
extraction extraction
OROR
DDAVP – 0.3µg/kg DDAVP – 0.3µg/kg in 50-100 cc in 50-100 cc
normal saline i.v. normal saline i.v. over 20-30 mins. over 20-30 mins. 1-2 hours before 1-2 hours before surgery (factor surgery (factor VIII level should VIII level should
be 80-100%)be 80-100%)
Repeat every day Repeat every day for 5-10 days for 5-10 days
(factor VIII level (factor VIII level 30-50%, normal 30-50%, normal
BT)BT)
DDAVP nasal DDAVP nasal spray (1.5mg/ml) spray (1.5mg/ml) 1-2 doses in each 1-2 doses in each
nostrilnostril
Repeat every day Repeat every day for 2-3 days after for 2-3 days after
extractionextraction
Type IIType II
Exogenous vWF in Exogenous vWF in cryoprecipitate cryoprecipitate
dose equal to 15-dose equal to 15-25U/kg factor VIII25U/kg factor VIII
Maintain F VIII Maintain F VIII levels at 30% i.e. levels at 30% i.e. 15U/kg, 2-3 days 15U/kg, 2-3 days postoperativelypostoperatively
Exogenous vWF in Exogenous vWF in cryoprecipitate to cryoprecipitate to obtain 80-100% obtain 80-100% levels of factor levels of factor
VIII 1-2 hrs before VIII 1-2 hrs before surgery.surgery.
Maintains F VIII Maintains F VIII levels at 30-50% levels at 30-50%
by infusing by infusing exogenous factor exogenous factor VIII every 12 hrs VIII every 12 hrs for 5-10 days.for 5-10 days.
DDAVP : 1- Desamino 8- D Arginine, Vasopressin/ 1- Desamino 8- D Arginine, Vasopressin/ DesmopressinDesmopressin

HAEMOPHILIA CHAEMOPHILIA C(FACTOR XI DEFICIENCY)(FACTOR XI DEFICIENCY)
Inherited as in complete recessive autosomal disorder.Inherited as in complete recessive autosomal disorder. Cannot activate thrombin-activable fibrinolytic Cannot activate thrombin-activable fibrinolytic
inhibitor(TAFI) –Results in rapid fibrinolysis, which is inhibitor(TAFI) –Results in rapid fibrinolysis, which is responsible for bleeding tendencyresponsible for bleeding tendency
Confers to injury related bleeding tendencyConfers to injury related bleeding tendency
TREATMENT>TREATMENT> Fresh frozen plasma or factor XI replacementFresh frozen plasma or factor XI replacement

Other Coagulation factors abnormalitiesFactor Inheritance Laboratory
defectC/F
Factor XII Autosomal recessive
aPTT,BT,CT prolonged
Nil
Factor X Autosomal recessive
aPTT,CT prolonged
Mild bleeding
Factor VII Autosomal recessive
Normal aPTT prolonged PT
Mild bleeding
Factor V Autosomal recessive
PT and aPTT prolonged
Mild bleeding
Factor II Autosomal recessive
PT and aPTT slightly prolonged
Mild bleeding
Factor XIII Autosomal recessive
PT,aPTT,Thrombin normal
Mild bleeding

Fat soluble vitaminFat soluble vitamin Present in diet and also synthesized by the gut floraPresent in diet and also synthesized by the gut flora Absorbed in small gut, in the presence of bile salts Absorbed in small gut, in the presence of bile salts Acts as a cofactor at a late stage in the synthesis by Acts as a cofactor at a late stage in the synthesis by
liver of liver of coagulation factors (II, VII ,IX, and X).coagulation factors (II, VII ,IX, and X). Gamma carboxylation of glutamate residues of these Gamma carboxylation of glutamate residues of these
zymogen proteins confers on them the capacity to zymogen proteins confers on them the capacity to bind calcium and to get bound to PL surface.bind calcium and to get bound to PL surface.
Haemorrhagic disease may result from interference Haemorrhagic disease may result from interference with Vitamin K use by >with Vitamin K use by > --AnticoagulantsAnticoagulants - -MalabsorptionMalabsorption -Obstructive jaundice -Obstructive jaundice
-Severe liver disease -Severe liver disease
Vitamin K Deficiency & Vitamin K Deficiency & malabsorptionmalabsorption

Liver Diseases
The no. of factors may contribute to the haemostatic defect in liver disease.
1. Defective synthesis of clotting factors
2. Increased fibrinolytic activities
3. Intravascular coagulation.
4. Hepatitis.
5. Malabsorption of Vitamin-K due to parenchymatous diseases.

DrugsDrugs
Factors influencing susceptibility of the Factors influencing susceptibility of the patient to anticoagulant drug.patient to anticoagulant drug.
PotentiatingPotentiating InhibitoryInhibitory
1.1. SalicylateSalicylate
2.2. PhenylbutazonPhenylbutazonee
3.3. SulphonamideSulphonamidess
4.4. ThyroxineThyroxine
1.1. BarbituratesBarbiturates
2.2. Chloral hydrateChloral hydrate
3.3. SpironolactoneSpironolactone
4.4. GlutethimideGlutethimide

Normal balance of hemostasis is alteredNormal balance of hemostasis is alteredResults in the uncontrolled inappropriate Results in the uncontrolled inappropriate
formation and lysis of fibrin within the formation and lysis of fibrin within the blood vesselsblood vessels
Activation of coagulation occurs Activation of coagulation occurs systemicallysystemicallyRather than locally at site of injuryRather than locally at site of injury
Fibrin is deposited diffusely within Fibrin is deposited diffusely within capillaries, arterioles and venulescapillaries, arterioles and venules
Clotting proteins, inhibitors and platelets Clotting proteins, inhibitors and platelets are consumed faster than they are are consumed faster than they are synthesizedsynthesized
Disseminated Intravascular CoagulationDisseminated Intravascular Coagulation

Clinical conditions associated with DICClinical conditions associated with DIC

Laboratory diagnosis is difficultLaboratory diagnosis is difficultAvailable tests are nonspecificAvailable tests are nonspecificNo single test can establish the definitive No single test can establish the definitive
diagnosis of DICdiagnosis of DICPT, APTT, TT prolongedPT, APTT, TT prolongedFibrin degradation products are (+)Fibrin degradation products are (+)Platelet count ↓; platelet function tests Platelet count ↓; platelet function tests
abnormalabnormalSchistocytes, thrombocytopenia on Schistocytes, thrombocytopenia on
peripheral blood smear peripheral blood smear
DIC – Laboratory DiagnosisDIC – Laboratory Diagnosis

Eliminate underlying cause, if Eliminate underlying cause, if possiblepossibleAcute DIC is often self-limited Acute DIC is often self-limited
Will disappear when fibrin is lysedWill disappear when fibrin is lysedReplacement therapy Replacement therapy
Platelets, RBC, Cryoprecipitate or fresh Platelets, RBC, Cryoprecipitate or fresh frozen plasmafrozen plasma
DIC – TherapyDIC – Therapy

Platelet Platelet countcount
Bleeding Bleeding timetime
APTAPTTT Prothrom-Prothrom-binbin
Presumptive Presumptive diagnosisdiagnosis
DecreasedDecreased ProlongedProlonged Norm.Norm. Norm.Norm. ThrombocytopeniaThrombocytopenia
Norm.Norm. ProlongedProlonged ProlongedProlonged Norm.Norm. von Willebrand’s diseasevon Willebrand’s disease
Norm./ Norm./ increasedincreased
ProlongedProlonged Norm. Norm. Norm.Norm. ThrombocytopathiaThrombocytopathia
Norm.Norm. Norm. Norm. ProlongedProlonged Norm.Norm. „„intrinsic” pathway intrinsic” pathway abnormality abnormality (FVIII. IX. XI. XII)(FVIII. IX. XI. XII)
Norm.Norm. Norm. Norm. Norm. Norm. ProlongedProlonged „„extrinsic”pathway extrinsic”pathway abnormality abnormality (FVII)(FVII)
Norm.Norm. Norm.Norm. ProlongedProlonged ProlongedProlonged „„common” pathway common” pathway abnorm. abnorm. (FI. II. V. X.)(FI. II. V. X.)
Norm.Norm. Norm.Norm. Norm.Norm. Norm.Norm. - /FXIII deficiency/ milde - /FXIII deficiency/ milde bleeding disorderbleeding disorder
Diagnosis of bleeding disorders by the screening testsDiagnosis of bleeding disorders by the screening tests

ANTICOAGULANTSANTICOAGULANTS
Heparin and Low Molecular Weight Heparin and Low Molecular Weight Heparins (e.g. enoxaparin, Heparins (e.g. enoxaparin, dalteparin)dalteparin)
Coumarin Derivatves e.g. Warfarin, Coumarin Derivatves e.g. Warfarin, AcenocoumarolAcenocoumarol
Indandione Derivatves e.g. Indandione Derivatves e.g. PhenindionePhenindione
Three classes

PARENTRAL ANTICOAGULANTSPARENTRAL ANTICOAGULANTS I-Indirect thrombin inhibitorsI-Indirect thrombin inhibitors - So called because they interact with antithrombin to - So called because they interact with antithrombin to
exert their antithrombotic effect.exert their antithrombotic effect. - Include unfractionated heparin (UFH- Include unfractionated heparin (UFH = heparin) & = heparin) & low low
molecular weight heparin (molecular weight heparin (LMWH).LMWH).HEPARINHEPARIN - Sulphated mucopolysaccadide with high molecular - Sulphated mucopolysaccadide with high molecular
weight. It is highly acidic carrying an weight. It is highly acidic carrying an electronegative electronegative charge.charge.
Mechanism of action and actions:Mechanism of action and actions: 1- Anticoagulant activity:1- Anticoagulant activity: both both i in vitro and in vivo.n vitro and in vivo. -Antithrombin III inhibits clotting factors proteases -Antithrombin III inhibits clotting factors proteases
(activated clotting factors; IIa, IXa, Xa, XIa & XIIa); most (activated clotting factors; IIa, IXa, Xa, XIa & XIIa); most importantly thrombinimportantly thrombin ( (factor IIa) factor IIa) and factor Xaand factor Xa. . In In absence of heparin, these reactions are slow; in the absence of heparin, these reactions are slow; in the presence of heparinpresence of heparin, they are , they are accelerated 1000 fold.accelerated 1000 fold.
- Binding causes conformational changes in this inhibitor - Binding causes conformational changes in this inhibitor exposing its active site for more rapid interaction with the exposing its active site for more rapid interaction with the protease. protease.

5/985/98 MedSlides.comMedSlides.com6666
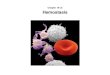
Heparin binds to antithrombin and increases the rate of thrombin inactivation
AT
Heparin
Inactivation of Thrombin byHeparin-AT ComplexesInactivation of Thrombin byHeparin-AT Complexes
ThrombinHF
S C

II- DIRECT THROMBIN INHIBITORSII- DIRECT THROMBIN INHIBITORS Directly bind to the active site of thrombinDirectly bind to the active site of thrombin
inhibiting thrombin's downstream effects thus exerting inhibiting thrombin's downstream effects thus exerting their antithrombotic activity. These their antithrombotic activity. These (in comparison (in comparison with UFHwith UFH) have ) have equal efficacy, increased equal efficacy, increased bioavailabilitybioavailability from the subcutaneous site of injection from the subcutaneous site of injection and and less frequent dosing requirements (long half life),less frequent dosing requirements (long half life),
Lepirudin:Lepirudin: -Is effective in treatment of -Is effective in treatment of heparin – induced heparin – induced
thrombocytopeniathrombocytopenia and other thromboembolic effects. and other thromboembolic effects.
DanaparoidDanaparoid:: its its anti factor anti factor XaXa is more than its is more than its antithrombin activity.antithrombin activity.
Advantages over heparin:Advantages over heparin: - Useful in - Useful in heparin – induced thrombocytopeniaheparin – induced thrombocytopenia (no (no
effect on platelet, also in heparin resistance (deficient effect on platelet, also in heparin resistance (deficient antithrombin III).antithrombin III).

The dose and frequency is controlled by The dose and frequency is controlled by aPTT measurement which is kept at 50 to aPTT measurement which is kept at 50 to 80 sec or 1.5-2.5 times the patients 80 sec or 1.5-2.5 times the patients pretreatment value.pretreatment value.
Does not cross Blood brain barrier or Does not cross Blood brain barrier or placenta (It is anticoagulant of choice in placenta (It is anticoagulant of choice in pregnancy).pregnancy).
Half life 1 – 4 hrs.Half life 1 – 4 hrs.

ORAL ANTICOAGULANTS ( VIT. K antagonists): -Coumarin anticoagulants include warfarin and dicumarol. Mechanism of anticoagulant activity (effective only in vivo): Inhibits vit. K epoxide reductase enzyme → prevention of reactivation of vitamin K (regeneration of the reduced form from the epoxide form) → interfere with synthesis of vitamin K – Dependent clotting factors (II, VII, IX, X) in liver by blocking γ – carboxylation of several glutamate residues in the above mentioned factors → inactive clotting factors Rapidly and completely absorbed from intestine and is 99 % plasma protein bound.It crosses placenta, and is secreted in milk

WARFARIN: MECHANISM OF ACTIONWARFARIN: MECHANISM OF ACTION
Inactive factors II, VII, IX, and X
Proteins S and C
Active factors II, VII, IX, and X
Proteins S and C
Vitamin K epoxide
Vitamin K reduced
WA
RFA
RIN
Warfarin blocks the reduction of oxidized vitamin K and thereby prevents the posttranscriptional carboxylation of the above four factors.This carboxylation reaction is essential for the ability of clotting factors to bind to calcium and to get bound to PL ,necessary for coagulation process to succeed.
Has no effect on previously formed thrombusHas no effect on previously formed thrombus

PLASMA HALF-LIVES OF VITAMIN K-PLASMA HALF-LIVES OF VITAMIN K-DEPENDENT PROTEINSDEPENDENT PROTEINS
Factor IIFactor II 72h72h
Factor VIIFactor VII 6h6h
Factor IXFactor IX 24h24h
Factor XFactor X 36h36h
Though the synthesis of clotting factors Though the synthesis of clotting factors diminishes within 2-4 hrs of warfarin diminishes within 2-4 hrs of warfarin administration, anticoagulant effect administration, anticoagulant effect develops gradually over the next 1-3 days develops gradually over the next 1-3 days as the level of clotting factors already as the level of clotting factors already present in plasma decline progressively. present in plasma decline progressively. Thus there is always a delay between Thus there is always a delay between administration of drug and anticoagulant administration of drug and anticoagulant effect .effect .

INDICATIONSINDICATIONS
Prophylaxis and treatment of venous Prophylaxis and treatment of venous thromboembolism (deep vein thromboembolism (deep vein thrombosis and pulmonary embolism)thrombosis and pulmonary embolism)
Prophylaxis and treatment of Atrial Prophylaxis and treatment of Atrial fibrillationfibrillation
Valvular stenosisValvular stenosis Heart valve replacementHeart valve replacement Myocardial infarctionMyocardial infarction

MONITORING OF WARFARIN THERAPYMONITORING OF WARFARIN THERAPY
Prothrombin timeProthrombin time PT ratioPT ratio INR (International Normalized Ratio)INR (International Normalized Ratio)

PROTHROMBIN TIME (PT)PROTHROMBIN TIME (PT)
Time required for blood to coagulate is Time required for blood to coagulate is called PTcalled PT
Performed by adding a mixture of calcium Performed by adding a mixture of calcium and thromboplastin to citrated plasmaand thromboplastin to citrated plasma
As a control, a normal blood sample is As a control, a normal blood sample is tested continuouslytested continuously
PT ratio (PTR) = PT ratio (PTR) = Patient’s PTPatient’s PT
Control PTControl PT

INTERNATIONAL NORMALISED RATIO (INR)INTERNATIONAL NORMALISED RATIO (INR)
INR = [PTINR = [PTptpt] ] ISIISI
[PT[PTRefRef]]
PTPTpt pt – prothrombin time of patient– prothrombin time of patient
PTPTRef Ref – prothrombin time of normal pooled sample– prothrombin time of normal pooled sample
ISI – International Sensitivity IndexISI – International Sensitivity Index
The International Normalized ratio is a recommended method for reporting prothrombin time results for control of oral anticoagulation (British Community for Standards in Hematology 1990).

How is Warfarin (Coumadin®) Monitor How is Warfarin (Coumadin®) Monitor and What Dose Doand What Dose Do
I Take?I Take?
Warfarin (Coumadin®) is monitored by a Warfarin (Coumadin®) is monitored by a blood test called an INR (International blood test called an INR (International Normalized Ratio). Warfarin belongs to a Normalized Ratio). Warfarin belongs to a category of drugs known as category of drugs known as “narrow “narrow range of effectiveness” range of effectiveness” drugs. This means drugs. This means that there is a very narrow range where that there is a very narrow range where the drug is considered therapeutic. the drug is considered therapeutic. For For most indications, the INR range is 2.0 to most indications, the INR range is 2.0 to 3.03.0. For people with mechanical heart . For people with mechanical heart valve replacements and certain other valve replacements and certain other conditions, the range is 2.5 to 3.5. conditions, the range is 2.5 to 3.5.

When your INR falls within your range (for example, between 2.0 and 3.0), this means that your level is “therapeutic”. When your INR level goes below the range (for example, 1.5) this means your blood is “too thick”, and places you at risk for blood clots. In this situation, your healthcare provider will prescribe a higher dose of warfarin for you to take. If your INR goes above your range (for example, 4.5) this means your blood is “too thin”, and places you at risk for bleeding. In this situation, your healthcare provider will prescribe a lower dose of warfarin for you to take.Because warfarin (Coumadin®) affects each person differently, some people will be on small doses of warfarin and some will be on very large doses. Some people will achieve their appropriate INR quickly and others more slowly. The dose of warfarin you need is the one that keeps the INR in the therapeutic range for your condition. Many factors can affect your INR level including a change in diet, a change in medications, the onset of a new illness,or having to stop your warfarin for a procedure.

When a person first starts taking warfarin (Coumadin®) the INR level tends to fluctuate up and down until the correct dose of warfarin is found that keeps your INR level stable. It is therefore very important to get your INR level checked frequently. In general, when you first start warfarin you will need to get your INR level checked 2 to 3 times a week for the first two weeks, then one to two times a week for two weeks, then every other week, then once a month. This may vary, depending on how your INR levels are. If the INR level becomes stable quickly, you will go for INR blood tests less often, if the INR level does not become stable, you will need to go for INR blood tests more often.When your INR level is too high or too low, you often will not feel any symptoms. This is why it is so important to get your INR blood tests done regularly!

PERIODONTAL CONSIDERATIONPERIODONTAL CONSIDERATION1) Consult the patient physician to determine 1) Consult the patient physician to determine
the nature of the underlying medical problem the nature of the underlying medical problem and the degree of required anticoagulation.and the degree of required anticoagulation.
2) 2) A)INFILTRATION ANAESHESIA,SCALING AND A)INFILTRATION ANAESHESIA,SCALING AND ROOT PLANNING ROOT PLANNING may be done-if INR less may be done-if INR less than 3.than 3.
B)BLOCK ANAESTHESIA,MINOR B)BLOCK ANAESTHESIA,MINOR PERIODONTAL SURGERY AND SIMPLE PERIODONTAL SURGERY AND SIMPLE EXTRACTION-EXTRACTION-if INR less than 2 to 2.5if INR less than 2 to 2.5
C)COMPLEX SURGERY OR MULTIPLE C)COMPLEX SURGERY OR MULTIPLE EXTRACTIONS EXTRACTIONS may require INR less than 1.5 may require INR less than 1.5 to 2.to 2.

3) Often, the anticoagulant is discontinued for 2 to 3 days before periodontal treatment(clearance half life of warfarin is 36-42 hours), and INR is checked on the day of therapy.If INR is within acceptable target range,the procedure is done and anticoagulant resumed immediately after treatment.
4)Careful technique and complete wound closure are paramount. For all procedures, application of pressure can minimize hemorrhage.
5)Use of oxidized cellulose, micrifibrillar collagen, topical thrombin,and tranexamic acid should be considered for persistent bleeding.

SIDE EFFECTSSIDE EFFECTS
Hemorrhage Hemorrhage Skin necrosisSkin necrosis Purple toe syndromePurple toe syndrome Microembolization Microembolization TeratogenecityTeratogenecity
Agranulocytosis, leukopenia, diarrhoea,Agranulocytosis, leukopenia, diarrhoea,
nausea, anorexia.nausea, anorexia.

Periodontal ProceduresPeriodontal Procedures
Periodontal health is critically important because of two principal reasons: 1) Hyperemic gingiva contributes to
spontaneous and induced gingival bleeding2) Periodontitis is a leading cause of tooth
morbidity, necessitating extraction Oral hygiene neglect due to fear of toothbrush-
induced bleeding Oral physiotherapy can be accomplished Periodontal probing and supragingival scaling
and polishing can be done routinely. Careful subgingival scaling with fine scalers

Severely inflamed and swollen tissues are best treated initially
with chlorhexidine oral rinses or by gross debridement with a cavitron or hand instruments to allow gingival shrinkage prior to deep scaling
Periodontal surgical procedures warrant elevating circulating factor levels to 50% and use of post-treatment antifibrinolytics
8383

Dabigatran and rivaroxaban, new oral Dabigatran and rivaroxaban, new oral anticoagulants. new approaches inanticoagulants. new approaches in
dentistrydentistry J Clin Exp Dent. 2010;2(1):e1-5J Clin Exp Dent. 2010;2(1):e1-5..
New generation of antithrombotic agents not New generation of antithrombotic agents not related to coumarin are dabigatran etexilate related to coumarin are dabigatran etexilate (Pradaxa ®) and rivaroxaban (Xarelto ®).(Pradaxa ®) and rivaroxaban (Xarelto ®).
Anticoagulant Anticoagulant DABIGATRANDABIGATRAN is the first is the first directdirect thrombin inhibitor, orally availablethrombin inhibitor, orally available. Specifically . Specifically and reversibly inhibits thrombin, so the duration and reversibly inhibits thrombin, so the duration of action is predictable. The anticoagulant effect of action is predictable. The anticoagulant effect correlates well with plasma drug concentrations, correlates well with plasma drug concentrations, which implies an effective anticoagulation with which implies an effective anticoagulation with low bleeding risk without major problems of low bleeding risk without major problems of interactions with other drugs.interactions with other drugs.

Rivaroxaban is first oral anticoagulant inhibitor of factor Xa (F Xa). It produces a predictable and reversible inhibition of F Xa activity with ability to inhibit clot-bound F Xa. The emergence of new oral anticoagulants, such as dabigatran and rivaroxaban, has in recent years appear as a substitute of coumarin anticoagulants and have the potential to changethe standards of clinical practice in the prevention ofdeep vein thrombosis and pulmonary embolism. The useof dabigatran and rivaroxaban does not require continuous monitoring of INR. Furthermore, dabigatran and rivaroxaban, unlike warfarin or acenocoumarol, have no drug interactions with NSAIDs or with most first-choice antimicrobials used in the dental office, so it is a dental management safer and easier for the professional in the oral cavity.

ReferencesReferences
PRINCIPLES OF INTERNAL MEDICINE, PRINCIPLES OF INTERNAL MEDICINE, HARRISON’S, 15HARRISON’S, 15THTH EDITION. EDITION.
BURKET’S ORAL MEDICINE 10BURKET’S ORAL MEDICINE 10THTH EDITION EDITION CONCISE MEDICAL PHYSIOLOGY, CHOUDHARI, CONCISE MEDICAL PHYSIOLOGY, CHOUDHARI,
9th EDITION.9th EDITION. CLINICAL PERIODONTOLOGY,CARANZZA,10CLINICAL PERIODONTOLOGY,CARANZZA,10THTH
EDITION.EDITION. ESSENTIAL OF MEDICAL PHARMACOLOGY, ESSENTIAL OF MEDICAL PHARMACOLOGY,
K.D.TRIPATHI,6K.D.TRIPATHI,6THTH EDITION. EDITION. JOURNAL OF CLINICAL AND EXPERIMENTAL JOURNAL OF CLINICAL AND EXPERIMENTAL
DENTISTRY 2010;2(1)DENTISTRY 2010;2(1)