Embed Size (px)
Citation preview

Clin Liver Dis 11 (2007) 893–916
Hepatitis B and End-StageLiver Disease
Ilan S. Weisberg, MD, MSa,Robert S. Brown Jr, MD, MPHb,
Samuel H. Sigal, MDa,b,*aDivision of Gastroenterology and Hepatology, New York Weill Cornell Medical Center,
525 E. 68th Street, New York, NY 10021, USAbCenter for Liver Disease and Transplantation, Columbia University Medical Center,
622 W. 168th Street, 14th floor, New York, NY 10032, USA
With more than 400 million people infected, hepatitis B virus (HBV) isthe most common cause of chronic hepatitis and end-stage liver diseaseworldwide [1]. Globally, chronic HBV (CHB) infection is responsible fora third of all cases of cirrhosis, more than half of all hepatocellular carcino-mas (HCC), and more than half a million deaths annually [2]. Although theburden of disease in the United States, with approximately 1.25 million in-fected people, is substantially lower than many other parts of the globe, suchas Africa, China, and Southeast Asia [3], increased immigration from en-demic areas of the world is transforming CHB into a growing public healthconcern in America. This trend was highlighted recently by the report that21% of Asian Americans living in New York City are chronically infectedand possess detectable hepatitis B surface antigen (HBsAg) [4].
Untreated, CHB acquired early in life results in cirrhosis, liver failure, orHCC in up to 40% of individuals [5]. Until recently, the options for a patientwho had end-stage hepatitis B cirrhosis were severely limited. Treatment forthe underlying hepatitis was not possible, and liver transplantation for thosewho had manifestations of end-stage liver disease was a relative contraindi-cation because of the nearly universal and rapid recurrence of end-stagedisease. Over the past 15 years, however, great strides have been made inprevention and treatment of hepatitis B cirrhosis. This article reviews recentadvances in the understanding of the natural history, prevention, andmedical management of HBV-related end-stage liver disease.
Dr. Sigal receives research support from and is on the speaker’s bureau for Gilead.
* Corresponding author.
E-mail address: [email protected] (S.H. Sigal).
1089-3261/07/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.cld.2007.08.009 liver.theclinics.com

894 WEISBERG et al
Natural history: chronic hepatitis B and end-stage liver disease
Development of cirrhosis and decompensated liver disease
Several large cohort studies conducted before the advent of effectiveantiviral therapy have enhanced the knowledge of the natural history ofCHB [6–8]. Untreated, the annual risk of progression to cirrhosis rangesfrom 2% to 6%, with a 5-year cumulative risk of approximately 20%.The majority of cases of HBV cirrhosis are diagnosed in asymptomaticindividuals in the fourth or fifth decade of life, underscoring the slow andinsidious progression from chronic hepatitis to advanced fibrosis [9].
Without treatment, the progression of compensated HBV cirrhosis isslow, and the 5-year survival rate is greater than 80% [10–14]. Clinicallyevident complications of cirrhosis or hepatic decompensation usually pres-ent 3 to 5 years after development of cirrhosis [15]. After the first episodeof clinical decompensation, the probability of survival decreases precipi-tously with a 5-year survival of only 14% to 35% [12,16]. Short-term predic-tors of increased mortality include advanced age and clinical markers ofportal hypertension and hepatic dysfunction such as increased bilirubinlevels, thrombocytopenia, hypoalbuminemia, and the presence of ascites,spider nevi, or hepatic encephalopathy [10,14,16,17]. The model for end-stage liver disease (MELD), which incorporates total bilirubin, albumin,and creatinine levels to predict 3-month and 1-year mortality, has beenvalidated in patients who have decompensated CHB [18]. Natural historystudies have identified a variety of additional viral, host, and confoundingfactors associated with accelerated progression to end-stage disease.
Viral factors in disease progression
Ongoing viral replication and detectable hepatitis B e antigen (HBeAg)are associated with increased risk for the development of end-stage liverdisease and death [7,8]. Seroconversion from HBeAg positivity to Hepatitis eantibody (HBeAb) positivity is an important event in the natural history ofCHB and is associated with a marked reduction in HBV DNA andnecroinflammatory activity in most patients [7,8]. In a Dutch cohort of un-treated HBV infection, HBeAg to HBeAb seroconversion was associatedwith a 55% reduction in the likelihood of death [12]. In patients whohad compensated cirrhosis, seroconversion was associated with 97%5-year survival rate, compared with only 72% in those in whom HBeAgpersisted [19].
Two recent large population studies from Taiwan highlight the importantrelationship between replication as reflected by the serum HBV DNA leveland the development of end-stage liver disease [20,21]. In a prospectivestudy involving more than 3000 patients who had CHB followed for upto 11 years, HBV viral load was the strongest predictor of progression tocirrhosis. The cumulative incidence of cirrhosis was intricately linked to

895HEPATITIS B AND END-STAGE LIVER DISEASE
baseline circulating viral DNA levels [20], ranging from 4.5% in those witha viral load of less than 300 copies/mL to 36.2% in those who had a viralload higher than 106 copies/mL. In a similar dose-dependent fashion, theHBV DNA level was shown to correlate with the risk for the developmentof HCC among 3653 Chinese patients who had CHB followed for more than11 years [21]. An incremental rise in HCC was observed with increased HBVDNA levels at study entry that remained significant after adjusting for age,sex, HBeAg status, presence of cirrhosis, exposure to other carcinogens (to-bacco and alcohol use), and serum alanine aminotransferase (ALT) levels,and it was especially significant in the HBeAg-negative CHB subgroup with-out cirrhosis or elevated aminotransferase levels.
Specific viral characteristics, such as genotype and genetic variants in reg-ulatory elements of the viral genome, also have been implicated in diseaseprogression. Among Asian patients, HBV genotype seems to influence dis-ease progression. As compared with genotype C, patients who have geno-type B infection have a favorable disease course. Sumi and colleagues [22]observed earlier age of seroconversion and a slower progression towards cir-rhosis and HCC in Japanese patients who had genotype B versus genotypeC infection. Similarly, infection with genotype B portended earlier serocon-version and decreased risk of HCC, cirrhosis, and viral reactivation than ge-notype C infection in a prospective study of 202 Chinese patients who hadHBeAg-positive CHB [23]. This effect of HBV genotype, however, has notbeen confirmed in a recent Western study that failed to identify an associa-tion with disease progression [24]. The spontaneous emergence of severalwell-defined variants, such as the pre-S deletion and precore and basalcore promoter mutants, also seems to influence the course of disease. Basalcore promoter mutations, which are more prevalent among genotype Cinfections, are associated with higher HBV viral load and increased rates ofHCC [25–27]. In addition, mutations in the major hydrophilic region of thesurface antigen also may influence rate of HBeAg seroconversion and sever-ity of liver disease [28].
Host factors in disease progression
The risk for progression to cirrhosis and decompensation increaseslinearly with age. In a 3-year prospective study of 684 Taiwanese patientswho had CHB, the risk of cirrhosis increased proportionately with age attime of study entry, particularly for those older than 40 years [7]. A similartrend has been observed in a variety of geographically distinct populationsin Asia [29], Europe [8,30], and the United States [10].
Male gender also seems to play a significant role in disease progression.Chu and colleagues [31] demonstrated that men are exponentially overrep-resented in advanced HBV-related liver disease. The male-to-female ratioincreases from 1.2:1 in asymptomatic carriers to 6.3:1 in those who havechronic liver disease and to 9.8:1 among those who have HBV-related

896 WEISBERG et al
HCC. In a follow-up study of more than 10,000 Chinese asymptomaticHBsAg carriers, men were found to be twice as likely to have abnormaltransaminase levels than women as well as a decreased rate of HBeAgloss [32], and it has been shown that male gender is an independent riskfactor for abnormal ALT levels on multivariate analysis [33]. One possibleexplanation for this gender-associated effect on disease progression is therole of androgens and their receptors. Recent work has reported an in-creased risk of HCC with elevated circulating testosterone levels, variationsin the trinucleotide CAG repeat in the androgen receptor gene, and severalpolymorphisms of key enzymes in androgen metabolism [34].
Evidence for genetic predispositions to fibrosis also has been proposed,especially related to polymorphisms in many regulatory genes of the renin-angiotensin axis, iron uptake, and inflammatory pathways. Two commonlyoccurring variations in the core promoter region of the angiotensinogen(AGT) gene are more prevalent in cirrhotic CHB patients than in noncirrhoticcontrols [35]. Hetero- and homozygosity of the H63D mutation of the HFEgene in patients who have CHB is associated with the development of livercirrhosis [36]. Similarly, the 308G/G genotype and TCGG haplotype of thetumor necrosis factor-alpha promoter region are associated with decompen-sated cirrhosis and progression to end-stage liver disease, respectively [37].
Confounding factors on disease progression
Although age, gender, and genetic predisposition are nonmodifiable hostrisk factors related to disease progression, a variety of confounding factors,including life-style choices, which have the potential to be modified, alsomay alter the pace of CHB progression. A retrospective Japanese study ob-served an accelerated course of CHB with self-reported heavy alcohol intake[38]. On average, HCC and cirrhosis developed 10 years earlier in habitualalcohol drinkers than in their nondrinking counterparts. Chen and col-leagues [39] similarly observed an increased likelihood of developing HCCin Chinese patients with either heavy alcohol or tobacco consumption.
The influence of diabetes on CHB infection and cirrhosis is less clear.Although the incidence and severity of chronic hepatitis C is increased inpatients who have diabetes mellitus, data are conflicting for CHB. In a largeAmerican cohort of diabetic patients, the seroprevalence of HBsAg wassimilar to that in healthy blood donors (w 0.3%) [40]. A similar study con-ducted in Asia found comparable surface antigen seroprevalence in type 2diabetics and healthy controls (13.5% versus 12.4%) [41]. In contrast,a study of 174 HBeAg-negative CHB patients suggested that the presenceof diabetes is associated strongly with increasing severity of liver fibrosis[42], and a large prospective Chinese cohort study of 500 HBsAg carriersidentified diabetes as an independent predictor for developing cirrhosis [43].
Unlike their well-documented roles in disease progression in chronichepatitis C, obesity and hepatic steatosis do not seem to be implicated in

897HEPATITIS B AND END-STAGE LIVER DISEASE
advanced fibrosis during CHB infection [44,45]. In a retrospective review of233 Greek patients who had biopsy-proven CHB, hepatic steatosis corre-lated with body mass index and fasting glucose but not with grade of inflam-mation or stage of fibrosis [45]. Similarly, a prospective Australian studyconcluded that steatosis is associated with waist circumference, fastingglucose, and inflammatory markers such as C-peptide but not with fibrosis[46]. Interestingly, a recent publication has reported increased rates ofHBsAg clearance in obese patients with moderate (odds ratio, 3.2; 95% con-fidence interval, 1.2–8.4; P ¼ .02) and severe steatosis (odds ratio, 3.9; 95%confidence interval, 1.1–14.2; P ¼ 0.04) that was postulated to be caused byinterference with the cytoplasmic distribution of viral proteins [47].
Prevention of end-stage disease
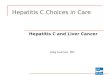
Chronic inflammation caused by hepatitis B leads to progressive fibrosisand cirrhosis, culminating in end-stage liver disease with portal hypertensionand HCC. The presence of HBeAg is associated with ongoing hepaticinflammation, and spontaneous seroconversion augurs an important timepoint in the natural history of HBV infection. In most cases, it is accompa-nied by decreased viral replication, normalization of aminotransferase levels,and improvement in histologic inflammatory activity [48,49]. Although itgenerally has been held that advanced fibrosis, once present, is static andirreversible, evidence is accumulating to suggest that fibrogenesis is a dynamicprocess, amenable to arrest or possibly even reversal with removal of theinciting agent [50]. Analogous to the improvement observed with continuedabstinence in alcoholic liver disease [51], with immunosuppression in chronicautoimmune hepatitis [52], with weight loss in steatohepatitis [53], and withclearance of HCVwith interferon and ribavirin [54], suppression of HBV rep-lication and loss of HBeAg with antiviral therapy may prevent progressivefibrosis and decompensation.
Interferon alfa
Interferon has several beneficial actions in CHB. It possesses intrinsicanti-fibrotic activity and directly inhibits hepatic stellate cell activation[50]. In animal models of cirrhosis, interferon therapy reduces collagengene transcription [55] and reverses cirrhosis [56]. In addition, it is a potentimmunomodulator and indirectly promotes HBV clearance by enhancingthe host response to chronic infection.
Both unmodified (standard) and pegylated interferon are approved forthe treatment of CHB. Treatment with pegylated interferon for 48 weeksis associated with HBeAg seroconversion and suppression of viral DNAto below 100,000 (105) copies/mL in 32% of cases [57]. In nearly half ofpatients with paired biopsies before and after interferon therapy, animprovement of at least 2 points in histologic activity was shown on the

898 WEISBERG et al
histology activity index, and this improvement was strongly associated withHBeAg seroconversion.
Long-term follow-up studies demonstrate that standard interferon pro-motes viral clearanceandprevents the development of cirrhosis and clinical de-compensation [58–60]. In a series of 103 patients who had CHB treated withinterferon alfa and followed for amean duration for 50.0� 19.8months, sero-conversion was the most important prognostic factor in predicting outcome.No patient with documented seroconversion developed severe clinical decom-pensation or required transplantation [58]. The European Concerted Actionon Viral Hepatitis (EUROHEP) study [60] compared the outcomes of 40HBeAg-positive patients who had biopsy-proven cirrhosis treated with inter-feron with the outcomes of 50 untreated controls. After a mean duration of 7years, loss of HBeAg, which occurred in 27 treated patients (67%), was asso-ciatedwith normalization ofALT, increased frequency ofHBsAg loss, and de-creased liver-relatedmortality [60]. In a recently reported 15-year (median, 6.8years) follow-up study of patientswhohadCHB, cirrhosis developed in 10.7%of the interferon-treated patientswho did not have cirrhosis at study entry ver-sus 18.3% of historical untreated controls [61]. Interferon treatment itselfseemed to mitigate progression of fibrosis. Among the non-seroconverterswho did not have cirrhosis at study entry, 13.5%of interferon-treated patientsand 22.4% of untreated controls developed cirrhosis during follow-up.Among patients who had pre-existing cirrhosis, interferon treatment alsowas associated with a substantial reduction in the risk of HCC (16% versus56%). Finally, a single case report from Iran describes complete resolutionof cirrhosis and clinical stabilization 5 years after interferon treatment [62].
Nucleos(t)ide antagonists
Both nucleoside (lamivudine, entecavir, telbivudine) and nucleotide(adefovir) antagonists of the HBV DNA polymerase are available for thetreatment of CHB infection, and the nucleotide tenofovir, which is approvedfor the treatment of HIV infection, is undergoing phase III testing. Theseagents have been shown to modulate the natural history of HBV-related liverdisease by delaying disease progression, minimizing hepatic decompensation,and promoting histologic improvement [63–65]. Analysis of paired liver biop-sies before and after lamivudine treatment reveals decreased markers ofhepatic stellate cell activity and collagen synthesis [66], suggesting thatlong-term therapy can slow or reverse hepatic fibrosis by suppressing hepato-cyte injury. Studies with all agents approved by the Food and Drug Admin-istration (FDA) have shown decreased inflammation and even decreasedfibrosis at 1 year in virologic responders [19,67–69], and continuous adefovirtreatment for up to 5 years demonstrated continued improvement in hepaticinflammation and fibrosis [70].
The histologic benefits of antiviral therapy form a pathophysiologic basisfor case reports of cirrhosis reversal after antiviral treatment [62] as well as

899HEPATITIS B AND END-STAGE LIVER DISEASE
prevention of end-stage disease. In a landmark study, Liaw and colleagues[71] randomly assigned 651 patients who had advanced fibrosis or cirrhosisto receive lamivudine (100 mg) or placebo and evaluated the time to diseaseprogression (hepatic decompensation, development of variceal bleeding,spontaneous bacterial peritonitis, HCC, or liver-related death) (Fig. 1). Af-ter a median treatment of 32 months, the study was terminated prematurelybecause of a significant difference in the number of patients reaching the pre-defined end point, 7.8% in the lamivudine arm versus 17.7% with placebo.Moreover, the development of HCC was nearly twice as likely in the placebogroup as in those treated with lamivudine (3.9% versus 7.4%). The inci-dence of HCC in the two groups diverged after 18 months, consistentwith an actual effect of treatment versus placebo.
Treatment of end-stage liver disease
Early natural history studies conducted in the era before PCR-based viraltesting was available suggested that the transition from chronic hepatitis tocirrhosis often heralded a nonreplicative phase of HBV liver disease charac-terized by HBeAg clearance, minimal to no inflammation, and the absenceof detectable viral DNA [11,15,48,72]. With improved molecular diagnostictesting, it now is understood that low-level viral replication is common. Inaddition, pathologic evaluation of explanted end-stage HBV cirrhotic liversfrequently reveals severe hepatic inflammation [73]. Thus, in a manneranalogous to the response to steroid therapy for severe alcoholic hepatitis[74] or an acute presentation of autoimmune hepatitis [75], anti-HBVtherapy may suppress viral replication and hepatic inflammation leadingto clinical stabilization and improvement.
Interferon
Low-dose interferon has been shown to effect sustained viral clearance indecompensated cirrhosis. In a study of 26 decompensated cirrhotics, a sus-tained viral response was achieved in 100%, 33%, and 0% of patients withChilds Class A, B, and C cirrhosis, respectively [76]. This study along withtwo small pilot investigations raised significant concerns about safety andefficacy, however [76–78]. In a study involving 18 patients who had decom-pensated cirrhosis treated with interferon alfa [77], 6 (33%) had sustainedloss of HBV DNA and HBeAg with normalization of serum aminotransfer-ases and resolution of symptomatic liver disease. Five patients, however, de-veloped serious bacterial infections, and 9 patients had exacerbation of theirunderlying disease. Similarly, in a French study of low-dose long-term inter-feron therapy, 10 of 15 (66%) decompensated cirrhotics treated for up to 48months had sustained viral suppression with HBV DNA and HBeAg loss[78], but life-threatening complications such as bacterial infection, hepatitisflares, and esophageal variceal bleeding were common. Because of these

900 WEISBERG et al
Fig. 1. Seminal report encapsulating the argument for antiviral therapy in patients advanced
HBV liver disease. (From Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with
chronic hepatitis B and advanced liver disease. N Engl J Med 2004;351:1527; with permission.
Copyright � 2004, Massachusetts Medical Society.)

901HEPATITIS B AND END-STAGE LIVER DISEASE
safety concerns, the use of interferon in patients who have decompensatedhepatitis B cirrhosis now is considered strongly contraindicated, andmany experts prefer to avoid interferon even in compensated cirrhoticsfor fear of precipitating a decompensating hepatitis flare.
Nucleos(t)ide analogues
Currently four nucleos(t)ide analogues (lamivudine, adefovir, entecavir,and telbivudine) are approved for the treatment of CHB, and several others(tenofovir, emtricitabine, clevudine, and pradefovir) are under clinical inves-tigation. Although experience with these agents in end-stage liver disease isaccumulating, efficacy data are largely restricted to small, uncontrolled trialsbecause of the clinical severity of this patient population. Because it was thefirst, and for several years was the only, agent available, lamivudine is thebest-studied agent in advanced disease. It is assumed that the lessons learnedcan be generalized to the newer agents.
LamivudineSeveral small studies of lamivudine therapy have reported improved
patient survival and decreased need for liver transplantation associatedwith effective viral suppression. Villeneuve and colleagues [79] reporteda slow but progressive improvement in liver function in the majority of35 cirrhotic patients (57% HBeAg positive) treated with daily lamivudinethat was most apparent after 9 months of therapy. Markers of hepatic func-tion (bilirubin, serum albumin levels) and Child-Turcotte-Pugh (CTP) scoreimproved significantly in 23 of the 35 patients who remained on treatmentmore than 6 months, and two patients initially listed for liver transplanta-tion were deactivated because of clinical stabilization. Kapoor and col-leagues [80] and Hann and colleagues [81] reported similar findings in 18and 75 patients, respectively. Compared with the preceding 6 months beforelamivudine was available, there was a significant reduction in the number ofhospital admissions and end-stage complications such as spontaneous bac-terial peritonitis (SBP), hepatic encephalopathy, and the need for repeatedlarge-volume paracentesis with antiviral therapy. In one of the few con-trolled trials involving decompensated cirrhosis, Yao and colleagues [82]compared daily lamivudine in 23 consecutive patients (74% HBeAg posi-tive) who had CPT scores of 10 or higher with an historical control cohortmatched for age, gender, and severity of liver disease. A significant clinicalresponse, defined as a decrease in CTP score by 3 points or more, wasachieved in 14 of the treated patients (60.9%) but in none of the controls,and the time to death or liver transplantation was substantially greater inthe treated cohort. Finally, lamivudine therapy also is effective in HBeAg-negative decompensated cirrhosis [83]. In a report comparing outcomes of30 patients treated with lamivudine and 30 noncontemporaneous matchedcontrols, there was a significant improvement in CTP in 23 (76.6%) patients

902 WEISBERG et al
and a trend towards improved survival in the treated patients [83]. Predic-tors of early death included Child’s Class C cirrhosis, impaired renal func-tion, high pretreatment HBV viral load, and an absence of biochemicalresponse within 6 months of initiating treatment [83,84].
AdefovirUntil recently, the reported literature on adefovir for end-stage liver
disease was restricted to case reports and small series of rescue therapy inpatients who developed lamivudine resistance while on therapy. Recently,however, Schiff and colleagues [85] reported the results of adefovir inlamivudine-resistant 226 patients (60% with Child Class B or C) awaitingliver transplantation. Adefovir led to marked inhibition of viral replication,HBeAg loss in 15 of 41 (48%), and HBeAg seroconversion in 7 of 31 (23%).Improvement in hepatic function was evidenced by normalization of serumalbumin level (77%), total bilirubin level (60%), and prothrombin time(84%) and improvement in MELD score. Fully 91% of patients initiallyclassified as Childs class B or C had an improvement in CTP score of at least1 point by week 48, permitting either survival to liver transplantation orremoval from the United Network of Organ Sharing waiting list becauseof clinical improvement [85].
TenofovirTenofovir is a nucleotide analogue closely related to adefovir that, at the
time of this writing, is FDA-approved for treatment of HIV but not fortreatment of HBV infection. Efficacy data, largely derived from retrospec-tive analyses of HIV/HBV-coinfected patients, suggest that tenofovir haspotent antiviral activity against HBV polymerase [86,87]. Experience withtenofovir in decompensated cirrhosis is limited to individual case reportsdescribing marked clinical improvement in patients who had lamivudineresistance and either adefovir resistance or incomplete response to adefovir[88,89].
Entecavir and telbivudineTo date there is no published experience with entecavir or telbivudine in
patients who have decompensated cirrhotic, and data from several ongoingtrials are highly anticipated (Table 1).
Treatment considerations
Patient selection for antiviral therapy
Determination of which patients are candidates for antiviral therapy hasnot been assessed in prospective, randomized studies, and published recom-mendations have been based largely on expert opinion [90,91]. There is gen-eral agreement that all compensated and decompensated cirrhotic patients,

Table 1
Ongoing/anticipat
Drug Phase Study population Start date Status
Prevention
Adefovir IV Compensated cirrhosis May 2005 Recruiting
Ishak fibrosis score O 4
Decompensated H
Telbivudine versu III Decompensated HBV December 2003 Recruiting
CTP score R 7
Entecavir versus a III Decompensated HBV August 2003 Recruiting
CTP score R 7
Tenofovir versus e
versus entecavir
II Decompensated HBV March 2006 Recruiting
CTP score 7–12 (inclusive)
Abbreviations:
Data from The icaltrials.gov. Accessed August 1, 2007.
903
HEPATIT
ISBAND
END-STAGELIV
ER
DISEASE
ed trials of anti–hepatitis B virus therapy
Trial identification Sponsor
NCT00347009 Glaxo-Smith-Kline
BV
s lamivudine NCT00076336 Idenix/Novartis
defovir NCT00065507 BMS
mtricitabine/tenofovir NCT00298363 Gilead Sciences
CTP, Child-Turcotte-Pugh; HBV, hepatitis B virus.
National Institutes of Health. Clinical trials data. Available at: Clin

904 WEISBERG et al
irrespective of HBeAg status, should be offered antiviral therapy if there isevidence of active replication (HBV DNA O 2000 IU/mL) [90,91]. Consen-sus is lacking for the treatment of clinically evident decompensated diseasewithout evidence of active replication. The most recent guidelines of theAmerican Association for the Study of Liver Disease recommend antiviraltherapy for decompensated cirrhotics who have HBV DNA levels greaterthan 2000 IU/mL or for those who have abnormal ALT if HBV DNA is de-tectable, regardless of level [91]. Other leading experts, however, suggest thatall decompensated patients should be considered for antiviral therapy evenin the absence of detectable HBV DNA [90]. Prospective studies to clarifythis discrepancy are unlikely, and treatment decisions should be made ona case-by-case basis.
The treatment of patients who have compensated cirrhosis and low-level(! 2000 IU/mL) or undetectable viral loads is an issue of ongoing debate[90,91]. It frequently is assumed that at this stage (referred to as ‘‘burnt-out cirrhosis’’) viral replication has ceased, and inflammatory activity hasresolved. Low-level viral activity in this setting may be observed, however,leading to insidious and continual liver damage despite normal or nearlynormal transaminase levels [92,93]. Moreover, the natural history of hepati-tis B is punctuated by spontaneous bursts of viral activity that commonlyresult in flares of inflammatory activity. For patients who have advancedfibrosis or cirrhosis, flares may lead to devastating consequences, becausethese patients are at increased risk for clinical deterioration and deathwith acute exacerbations [94,95]. Prolonged use of effective antiviral therapythat fully inhibits viral replication may suppress spontaneous clinical andsubclinical flares of activity and thereby prevent clinical decompensation.
Duration of antiviral therapy
The duration of treatment for end-stage liver disease has not beenevaluated in clinical trials and is unlikely to be studied because of ethical con-cerns. Nonetheless, several well-validated arguments support the consensusthat cirrhotic patients be treated indefinitely with antiviral therapy: (1) contin-uous treatment leads to progressive histologic improvement [96–99]; (2) treat-ment withdrawal is associated with histologic regression of previous benefit[19,70]; and (3) cessation of antiviral therapy can result in life-threateningflares and hepatic decompensation [100,101]. Although HBeAg-positivepatients who seroconvert during therapy theoretically could discontinuetreatment, many experts maintain that these patients should continue ontherapy indefinitely because of the fear of hepatic decompensation in the eventof seroreversion. As a corollary, an argument can be made for treating untila finite time after HBsAg loss occurs.
Data from long-term lamivudine treatment suggest that prolonged anti-viral therapy leads to progressive improvement in liver histology [96–99].In a prospective study of continuous therapy involving 63 patients in

905HEPATITIS B AND END-STAGE LIVER DISEASE
whom liver biopsies were repeated after 1 and 3 years, there was continuedimprovement in histologic activity index scores and fibrosis [96]. After1 year, 36 of 63 patients (57%) had a 2-point or greater improvement in nec-roinflammatory activity. After an additional 2 years of therapy, 38 of 63patients (60%) maintained this benefit, and 12 of 63 (19%) continued toimprove. At the end of study, 8 of 11 (73%) of the cirrhotic patients had im-provement with a decrease in fibrosis score from 4 to less than 3. These datahave been validated by similar results in two Asian studies [99].
Similarly, long-term therapy with adefovir is associated with progressivehistologic improvement [19,70]. In comparison with placebo, 48 weeks ofadefovir in HBeAg-negative patients resulted in significant histologic(64% versus 33%), biochemical (72% versus 29%), and virologic improve-ment (median HBV DNA reduction of 3.91 versus 1.35 log copies/mL) [19].After 48 weeks, patients enrolled in the companion follow-up study were as-signed randomly to 48 additional weeks of placebo or adefovir. At 96 weeksof treatment [70], 71% of patients maintained on adefovir had undetectableviral load, whereas the majority of patients in the placebo arm had a rapidreturn to baseline levels within 4 weeks of adefovir discontinuation. Simi-larly, normalization of serum ALT was observed in 73% of patients whocontinued adefovir therapy and returned to baseline (or higher) within8 weeks of adefovir withdrawal. Most importantly, adefovir discontinuationwas associated with histologic regression.
In up to 50% of patients, abrupt withdrawal of nucleos(t)ide analoguealso results in a hepatitis flare, which may not be tolerated by a cirrhoticpatient [70,100,102]. In patients assigned randomly to discontinue or to con-tinue adefovir after 3 years of therapy, ALT increased sharply to more than10 times the upper limit of normal before returning to baseline values amongthose who discontinued treatment [70]. Because patients who have cirrhosisare at increased risk for decompensation and death in the setting of a flare[100,102], most patients, including all precore mutant (eAg-negative) pa-tients, should be maintained on life-long therapy aimed at complete viralsuppression.
Resistance
The low-fidelity HBV polymerase lacks a proofreading function, andmore than 1010 point mutations are generated daily [103]. As a result, geno-typic resistance is a major limitation of continuous antiviral therapy. Loss ofHBV suppression, similar to treatment withdrawal, can lead to hepatitisflares and clinical deterioration [83,104,105], and for patients who havecirrhosis the risk of hepatic failure and death after virologic breakthroughis increased markedly [71,105,106]. Strategies aimed at preventing resistance,combined with careful monitoring for early detection and management ofresistance once it arises, are essential components of the therapeutic ap-proach to CHB. The prevention of resistance is of paramount importance

906 WEISBERG et al
in cirrhotic patients because of the potential for hepatic decompensationshould resistance emerge.
Given that more than 30% of virologic breakthrough is attributed tomedication nonadherence [91], patients receiving antiviral therapy shouldbe counseled continually about the importance of medication compliance.In addition, the different rates of resistance among currently available nucle-os(t)ide analogues should be incorporated into treatment decisions. Forexample, because the incidence of resistance with lamivudine is greaterthan 70% at 5 years, lamivudine is unsuitable for long-term monotherapyin end-stage CHB infection, and many experts consider it unsuitable formonotherapy in any patient who has CHB [90,91]. Although the initial find-ings suggested a very low rate of adefovir resistance, resistance mutations(N236T and A181V/T) emerge in nearly 30% of patients treated withadefovir for 5 years [70]. This emergence was seen predominantly in patientswho were not suppressed by 48 weeks, highlighting the need to achievecomplete viral suppression. Entecavir has an excellent resistance profile innucleoside-naive patients. The rate of resistance in nucleoside-naive patientson entecavir therapy who remained suppressed to less than 0.7 mEq/mL at96 weeks is extremely low [107]. A resistance rate of 40%, however, has beenreported in patients who have lamivudine-refractory disease [107]. Onlya single report of HBV resistance to tenofovir has been reported thus far,and the data remain preliminary [108].
Many experts believe that resistance to nucleos(t)ide monotherapy isinevitable, raising concerns about the use of sequential monotherapy[109]. By extrapolation, some experts speculate that combination therapyshould be employed routinely in the treatment of CHB. There are no pub-lished data conclusively demonstrating superior efficacy or safety for suchregimens, however. Moreover, given the profiles of some of the currentlyavailable drugs with high potency and high genetic barriers to resistance,the design of trials to prove superiority for combination therapy would re-quire trials involving large numbers of patients over a very long duration.Because of the barriers to demonstrating the superiority of combinationtherapy conclusively, some clinicians limit the routine use of combinationtherapy to cirrhotic patients, in whom the ‘‘stakes would be highest’’ wereresistance to emerge during monotherapy [90].
The ability to achieve viral suppression is believed to influence viraloutcome, possibly by inhibiting the emergence of resistant variants. A recentpreliminary report of telbivudine therapy suggested that HBV DNA unde-tectability at 24 weeks of therapy predicted improved 2-year efficacy [69].As a further measure to prevent resistance, combination therapy to intensifyantiviral pressure and deter or treat breakthrough in a manner similar tothat used to treat HIV infection also has been advocated. In a study of114 treatment-naive patients, Sung and colleagues [110] reported a decreasedincidence of lamivudine resistance at 1 year in patients treated with adefovir/lamivudine combination therapy versus lamivudine alone (20% versus 2%).

907HEPATITIS B AND END-STAGE LIVER DISEASE
Although a study evaluating telbivudine, lamivudine, and a combination ofthe two failed to demonstrate a benefit to dual-nucleoside therapy, this re-sult may be attributed to the use of two nucleoside agents that may competefor phosphorylation and/or share resistant mutations, emphasizing the needto use both nucleoside and nucleotide agents whose differing profiles resultin a lack of cross resistance [111].
Because virologic breakthrough precedes biochemical breakthrough andthen clinical decompensation, HBV DNA levels should be monitored regu-larly, and resistance mutations should be treated promptly. Until recently,the approach to lamivudine resistance was to transition patients to adefovirmonotherapy and minimize the risk of hepatitis flare by overlapping treat-ments for 2 to 3 months [112]. Although subsequently it was demonstratedin compensated and decompensated patients that a direct switch fromlamivudine to adefovir was well tolerated and not associated with an ALTflare [113,114], combination therapy now is being recommended increas-ingly. A retrospective study of lamivudine-resistant patients in Italy demon-strated decreased adefovir resistance (0.8% versus 5%) after 2 years ofadd-on therapy (adefovir and lamivudine) versus a switch to adefovir mono-therapy [115]. In a prospective study in which 42 HBeAg-negative patientswith genotypic lamivudine resistance were assigned randomly to adefovirmonotherapy (n ¼ 14) or to combination therapy (n ¼ 28), the rates ofserum HBV DNA and ALT normalization were similar in the two groupsafter 12 months of therapy. By 40 months, however, resistance leading tovirologic breakthrough developed in 21% of those receiving monotherapybut in none of those receiving combination therapy [116].
Toxicity
The nucleos(t)ide analogues are well tolerated with excellent records ofsafety [19,65,69,117]. Because all nucleos(t)ide analogues are not metabo-lized and are renally excreted, appropriate dose adjustments should bemade in patients who have impaired creatinine clearance. Early dose-findingstudies reported an unacceptable risk of nephrotoxicity with high-dose ade-fovir (30 mg daily) [67]. Long-term treatment at the conventional dose (10mg daily) is well tolerated, with mild elevations in creatinine levels seen inonly 3% of patients who have CHB [70]. Although decompensated patientsawaiting liver transplantation are at increased risk for renal dysfunctioncaused by hepatorenal syndrome, diuretic use, and exposure to nephrotoxicagents and contrast dyes, adefovir has been used safely in this patientpopulation without increased need to discontinue therapy [118]. Tenofovir,which is structurally similar to adefovir and is less nephrotoxic, can be usedsafely at higher therapeutic dosages and is a reasonable alternative. Enteca-vir and telbivudine do not have a safety database in decompensated patientsthat is substantial enough to allow any conclusions to be drawn, but theseagents are likely to be safe as well.

908 WEISBERG et al
Peritransplantation management
Early results with liver transplantation for CHB were poor, with recur-rence rates in excess of 80% and a 1-year survival of only 40% to 60%[119]. As a result, many centers initially considered HBV infection a contra-indication to liver transplantation. In 1993, Samuel and colleagues [120]demonstrated that long-term passive immunoprophylaxis with hepatitis Bimmune globulin (HBIG) could prevent graft reinfection, reduce the rateof recurrence to about 30%, and improve patient survival. With the subse-quent availability of antiviral nucleos(t)ide analogues, outcomes of livertransplantation for end-stage HBV are now similar to, if not better than,outcomes of liver transplantation for other indications [119,121,122].
Viral replication before surgery is associated with increased failure ofprophylaxis and decreased graft and patient survival [119–124]. Therefore,complete and sustained viral suppression with potent and effective nucleos(t)ide analogues before surgery is paramount. Because it was the only agentavailable for several years, more information is available about the use oflamivudine in the transplantation setting. Newer agents with greaterpotency and less risk of resistance have largely supplanted lamivudine, how-ever. Adefovir effectively suppresses viral replication in decompensated pa-tients awaiting liver transplantation and carries less risk of resistance [118].Although no published data exist for entecavir in transplantation patients, itprobably will play a prominent role in pre- and posttransplantation manage-ment in the future given its superior efficacy, resistance, and safety profile.
To prevent graft reinfection, posttransplantation prophylaxis is essential.Current practice at many transplant programs involves the administrationof HBIG and one or more nucleos(t)ide analogues [119]. HBIG is initiatedintraoperatively during the anhepatic phase and is continued indefinitelywith scheduled intravenous infusions to sustain protective anti-HBs titersof at least 100 to 150 IU/L. Antiviral therapy is begun before transplanta-tion and is maintained lifelong. The use of these two complementary strat-egies has reduced the rate of HBV recurrence to less than 10% 2 years aftertransplantation [121,125–127].
A major limitation of HBIG prophylaxis, however, is its cost at approxi-mately 100,000US dollars annually. In addition, the optimal dose, frequency,duration, and route of administration (intravenous or intramuscular) remaincontroversial, and alternative, more cost-effective strategies are being ex-plored. In a recent report of 147 patients who were treated with lamivudineand long-term monthly intramuscular HBIG [128], survival was comparableto that with standard intravenous HBIG over a mean 5-year follow-up period(92% at 1 year; 88% at 5 years), even though many patients were at high riskbecause of presence of detectable HBVDNA at time of transplantation. Onlyfive patients developed recurrent HBV, with actuarial risks of recurrence of1% and 4% at 1 and 5 years, respectively. All five responded to add-on ade-fovir therapywith complete normalization of graft function [128]. Because the

909HEPATITIS B AND END-STAGE LIVER DISEASE
risk of recurrent hepatitis B is related to the viral load before transplantation,this approach is particularly attractive for low-risk patients without viralreplication at the time of transplantation.
To reduce expense further, the possibility of completeHBIGwithdrawal innonreplicating patients also has been investigated. Buti and colleagues [129]treated 29 patients with high-dose intravenous HBIG and lamivudine for1 month after transplantation and then assigned these patients randomly tocontinued combination prophylaxis or to lamivudine monotherapy. After18 months of follow-up, all patients were alive and were without recurrenthepatitis. More recently, the long-term follow-up (median, 40 months) of 21patients maintained on nucleos(t)ide monotherapy after HBIG withdrawalhas been reported [130]. Of the 21 patients studied, only one individual devel-oped recurrentHBV 34months after stoppingHBIG; this instance was attrib-uted to noncompliancewith antiviral therapy.A secondpatient haddetectableHBV DNA (3.3 log copies/mL) without detectable HBsAg after approxi-mately 4 years. To limit viral breakthroughs that are inevitably associatedwith resistance, HBIGwithdrawal followed by combination antiviral therapyhas been evaluated. In a report of 10 patients treatedwith lamivudine/adefovirafter an initial 6 months of lamivudine/HBIG prophylaxis, none developedHBV recurrence after a mean follow-up period of 21 months [131].
Summary and treatment recommendations
Hepatic decompensation is associated with an extremely poor prognosisfor survival. Early initiation of effective antiviral therapy should be offeredto all patients, both to prevent and to treat end-stage liver disease. Althoughtreatment with interferon is contraindicated in decompensated liver disease,oral inhibitors of the HBV DNA polymerase are well tolerated and shouldbe continued indefinitely. Ideal treatment regimens will employ nucleos(t)ideanalogues, probably in combination, that possess potent antiviral activityand nonoverlapping resistance profiles. Ongoing clinical trials will help iden-tify the optimal regimen for preventing and treating end-stage liver diseaseresulting from CHB. Despite early and effective viral suppression, more than15% of decompensated patients either will not respond or will not survivelong enough to achieve a response [132]. Therefore, all decompensatedpatients should be referred promptly to a liver transplantation center forevaluation. Research is required to identify patients at risk for destabiliza-tion despite treatment to permit appropriate prioritization and optimalutilization of this scarce resource.
References
[1] McMahon BJ. Epidemiology and natural history of hepatitis B. Semin Liver Dis 2005;
25(Suppl 1):3–8.

910 WEISBERG et al
[2] Perz JF, Armstrong GL, Farrington, et al. The contributions of hepatitis B and
hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol
2006;45:529–38.
[3] Lee WM. Medical progress: hepatitis B. N Engl J Med 1997;337:1733–45.
[4] Sherman A, Tsang T, Villanueva G, et al. Mass screening in New York city reveal extraor-
dinarily high prevalence of hepatitis B in an urbanAsian population [Abstract]. Hepatology
2005;42:214A.
[5] Lok ASF. Chronic hepatitis B. N Engl J Med 2002;346:1682–3.
[6] LoKJ, TongMJ, ChienMC, et al. The natural course of hepatitis B surface antigen positive
chronic active hepatitis in Taiwan. J Infect Dis 1982;146:205–10.
[7] LiawYF, Tai DI, ChuCM, et al. The development of cirrhosis in patients with chronic type
B hepatitis: a prospective study. Hepatology 1988;8:493–6.
[8] FattovichG, Brollo L, GiustinaG, et al. Natural history and prognostic factors for chronic
hepatitis type B. Gut 1991;32:294–8.
[9] Fattovich G. Natural history and prognosis of hepatitis B. Semin Liver Dis 2003;23:47–58.
[10] Weissberg JI, Andres LL, Smith CI, et al. Survival in hepatitis B. Ann InternMed 1984;101:
613–6.
[11] Liaw YF, Lin DY, Chen TJ, et al. Natural course after the development of cirrhosis in
patients with chronic type B hepatitis: a prospective study. Liver 1989;9:235–41.
[12] De Jongh FE, Janssen HLA, De Man RA, et al. Survival and prognostic indicators in
hepatitis B surface antigen-positive cirrhosis of the liver. Gastroenterology 1992;103:
1630–5.
[13] Realdi G, FattovichG,Hadziyannis S, et al. Survival and prognostic factors in 366 patients
with compensated cirrhosis type B: a multicenter study. J Hepatol 1994;21:656–66.
[14] Kobayashi M, Ikeda K, Hosaka T, et al. Natural history of compensated cirrhosis in the
Child-Pugh class A compared between 490 patients with hepatitis C and 167 with B virus
infections. J Med Virol 2006;78:459–65.
[15] Chu CM, Liaw YF. Hepatitis B virus-related cirrhosis: natural history and treatment.
Semin Liver Dis 2006;26:142–52.
[16] Fattovich G, Giustina G, Schalm SW, et al. Occurrence of hepatocellular carcinoma and
decompensation in western European patients with cirrhosis type B. Hepatology 1995;
21:77–82.
[17] HuiAY,ChanLYC, LeungNWY, et al. Survival and prognostic indicators in patients with
hepatitis B virus-related cirrhosis after onset of hepatic decompensation. J Clin Gastroen-
terol 2002;34:569–72.
[18] ChanHLY, ChimAML, Lau JTF, et al. Evaluation of model for end-stage liver disease for
prediction of mortality in decompensated chronic hepatitis B. Am J Gastrotenterol 2006;
101:1516–23.
[19] Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Adefovir dipivoxil for the treatment
of hepatitis e antigen-negative chronic hepatitis B. N Engl J Med 2003;348:800–7.
[20] Iloeje UH, Yang HI, Su J, et al. Predicting cirrhosis risk based on the level of circulating
hepatitis B viral load. Gastroenterol 2006;130:678–86.
[21] Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biologic gradient
of serum hepatitis B virus DNA level. JAMA 2006;295:65–73.
[22] Sumi H, Yokosuka O, Seki N, et al. Influence of hepatitis B virus genotypes on the progres-
sion of chronic type B liver disease. Hepatology 2003;37:19–26.
[23] ChuCM,LiawYF.GenotypeC hepatitis B virus infection is associatedwith a higher risk of
reactivation of hepatitis B and progression to cirrhosis than genotype B: a longitudinal
study of hepatitis B e antigen-positive patients with normal aminotransferase levels at base-
line. J Hepatol 2005;43:411–7.
[24] Halfon P, Bourliere M, Pol S, et al. Multicentre study of hepatitis B virus genotypes in
France: correlation with liver fibrosis and hepatitis B e antigen status. J Viral Hepat
2006;13:329–35.

911HEPATITIS B AND END-STAGE LIVER DISEASE
[25] Kao JH, Chen PJ, Lai MY, et al. Basal core promoter mutations of hepatitis B virus
increase the risk of hepatocellular carcinoma in hepatitis B carriers. Gastroenterol 2003;
124:327–34.
[26] Lin CL, Liao LY,WangCS, et al. Basal core-promoter mutant of hepatitis B virus and pro-
gression of liver disease in hepatitis B e antigen-negative chronic hepatitis B. Liver Int 2005;
25:564–70.
[27] Tong MJ, Blatt LM, Kao JH, et al. Precore/basal core promoter mutants and hepatitis B
viral DNA levels as predictors for liver deaths and hepatocellular carcinoma.World J Gas-
troenterol 2006;12:6620–6.
[28] Song BC, Kim SH, KimH, et al. Prevalence of naturally occurring surface antigen variants
of hepatitis B virus in Korean patients infected chronically. J Med Virol 2005;76:194–202.
[29] Huo T,Wu JC,Hwang SJ, et al. Factors predictive of liver cirrhosis in patients with chronic
hepatitis B: a multivariate analysis in a longitudinal study. Eur J Gastroenterol Hepatol
2000;12:687–93.
[30] Moreno-Otero R, Garcia-Monzon C, Garcia-Sanchez A, et al. Development of cirrhosis
after chronic type B hepatitis: a clinicopathologic and follow-up study of 46 HbeAg-
positive asymptomatic patientws. Am J Gastroenterol 1991;86:560–4.
[31] Chu CM, Liaw YF, Sheen IS, et al. Sex difference in chronic hepatitis B virus infection: an
appraisal based on the status of hepatitis B e antigen and antibody. Hepatology 1983;3:
947–50.
[32] Chu CM, Sheen IS, Lin SM, et al. Sex difference in chronic hepatitis B virus infection: stud-
ies of serum HBeAg and alanine aminotransferase levels in 10,431 asymptomatic Chinese
HBsAg carriers. Clin Infect Dis 1993;16:709–13.
[33] Tsai JF, ChuangLY, Jeng JE, et al. Sex differences in relation to serum hepatitis B e antigen
and alanine aminotransferase levels among asymptomatic hepatitis B surface antigen car-
riers. J Gastroenterol 2000;35:690–5.
[34] YuMW, Cheng SW, LinMW, et al. Androgen-receptor gene CAG repeats, plasma testos-
terone levels, and risk of hepatitis B-related hepatocellular carcinoma. J Natl Cancer Inst
2000;92:2023–8.
[35] Xiao F,WeiH, Song S, et al. Polymorphisms in the promoter region of the angiotensinogen
gene are associated with liver cirrhosis in patients with chronic hepatitis B. J Gastroenterol
Hepatol 2006;21:1488–91.
[36] Mah YH, Kao JH, Liu CJ, et al. Prevalence and clinical implications of HFE gene muta-
tions (C282Y and H63D) in patients with chronic hepatitis B and C in Taiwan. Liver Int
2005;25:214–9.
[37] Niro GA, Fontana R, Gioffreda D, et al. Tumor necrosis factor gene polymorphisms and
clearance or progression of hepatitis B virus infection. Liver Int 2005;25:1175–81.
[38] Ohnishi K, Iida S, Iwama S, et al. The effect of chronic habitual alcohol intake on the de-
velopment of liver cirrhosis and hepatocellular carcinoma: relation to hepatitis B surface
antigen carriage. Cancer 1984;49:672–7.
[39] ChenCJ, LiangKY,ChangAS, et al. Effects of hepatitis B virus, alcohol drinking, cigarette
smoking and familial tendency on hepatocellular carcinoma. Hepatology 1991;13:398–406.
[40] Mason AL, Lau JY, Hoang N, et al. Association of diabetes mellitus and chronic hepatitis
C virus infection. Hepatology 1999;29:328–33.
[41] Chen HF, Li CY, Chen P, et al. Seroprevalence of hepatitis B and C in type 2 diabetic
patients. J Chin Med Assoc 2006;69:146–52.
[42] PaptheodoridisGV,ChrysanthosN, Savvas S, et al.Diabetesmellitus in chronic hepatitis B
and C: prevalence and potential association with the extent of liver fibrosis. J Viral Hepat
2006;313:303–10.
[43] Huo TI,Wu JC, Lee PC, et al. Diabetes mellitus as a risk factor of liver cirrhosis in patients
with chronic hepatitis B virus infection. J Clin Gastroenterol 2000;30:250–4.
[44] Altlparmak E, Koklu S, Yalinkilic M, et al. Viral and host causes of fatty liver in chronic
hepatitis B. World J Gastroenterol 2005;11:3056–9.

912 WEISBERG et al
[45] ThomopoulosKC,Arvaniti V, TsamantasAC, et al. Prevalence of liver steatosis in patients
with chronic hepatitis B: a study of associated factors and of relationship with fibrosis. Eur
J Gastroenterol Hepatol 2006;18:233–7.
[46] Gordon A, McLean CA, Pedersen JS, et al. Hepatic steatosis in chronic hepatitis B and C:
predictors, distribution and effect on fibrosis. J Hepatol 2005;43:38–44.
[47] Chu CM, Lin DY, Liaw YF. Does increased body mass index with hepatic steatosis con-
tribute to seroclearance of hepatitis B virus (HBV) surface antigen in chronic HBV infec-
tion? Int J Obes 2007;31:871–5.
[48] Hoofnagle JH, Dusheiko GM, Seef LB, et al. Seroconversion from hepatitis B e antigen to
antibody in chronic hepatitis type B hepatitis. Ann Intern Med 1981;94:744–8.
[49] FattovichG, RuggeM, Brollo L, et al. Clinical, virologic and histologic outcome following
seroconversion fromHbeAg to anti-Hbe in chronic hepatitis B. Hepatology 1986;6:167–72.
[50] Bataller R, Brenner DA. Liver fibrosis. Clin Investig 2005;115:209–18.
[51] Pares A, Caballeria J, Bruguera M, et al. Histological course of alcoholic hepatitis.
Influence of abstinence, sex, and extent of hepatic damage. J Hepatol 1986;2:33–42.
[52] Mohamadnejad M, Malekzadeh R, Nasseri-Moghaddam S, et al. Impact of immunosup-
pressive treatment on liver fibrosis in autoimmune hepatitis. Dig Dis Sci 2005;50:547–51.
[53] Dixon JB, Bhathal PS, Hughes NR, et al. Nonalcoholic fatty liver disease: improvement in
liver histologic analysis with weight loss. Hepatology 2004;39:1647–54.
[54] Arif A, Levine RA, Sanderson SO, et al. Regression of fibrosis in chronic hepatitis C after
therapy with interferon and ribavirin. Dig Dis Sci 2003;48:1425–30.
[55] Inagaki Y, Nemoto T, Kushida M, et al. Interferon alfa down-regulates collagen gene
transcription and suppresses experimental hepatic fibrosis in mice. Hepatology 2003;38:
890–9.
[56] Mathew TC, Abdeen S, Dashti H, et al. Effect of alpha-interferon and alpha-tocopherol in
reversing hepatic cirrhosis in rats. Anat Histol Embryol 2007;36:88–93.
[57] Lau GKK, Piratvisuth T, Luo KX, et al. Peginterferon alfa-2a, lamivudine, and the
combination for HbeAg positive chronic hepatitis B. N Engl J Med 2005;352:2682–95.
[58] Niederau C, Heintges T, Lange S, et al. Long-term follow-up of HbeAg-positive patients
treated with interferon alfa for chronic hepatitis B. N Engl J Med 1996;334:1422–7.
[59] LauDTY, Everhart J, Kleiner DE, et al. Long-term follow-up of patients with chronic hep-
atitis B treated with interferon alfa. Gastrotenterology 1997;113:1660–7.
[60] Fattovich G, Giustina G, Realdi G, et al. Long-term outcome of hepatitis B e antigen pos-
itive patients with compensated cirrhosis treated with interferon alfa. Hepatology 1997;26:
1338–42.
[61] Lin SM, YuML, Lee CM, et al. Interferon therapy in HbeAg positive chronic hepatitis re-
duces progression to cirrhosis and hepatocellular carcinoma. J Hepatol 2007;46:45–52.
[62] MalekzadehR,MohamadnejadM,RakhshaniN, et al. Reversibility of cirrhosis in chronic
hepatitis B. Clin Gastroenterol Hepatol 2004;2:344–7.
[63] Lai CL, Chien RN, Leung NWY, et al. A one year trial of lamivudine for chronic hepatitis
B. N Engl J Med 1998;339:61–8.
[64] Suzuki Y, KumadaH, IkedaK, et al. Histological changes in liver biopsies after one year of
lamivudine treatment in patients with chronic hepatitis B infection. J Hepatol 1999;30:
743–8.
[65] Dienstag JL, Schiff ER,Wright TL. Lamivudine as initial treatment for chronic hepatitis B
in the United States. N Engl J Med 1999;341:1256–63.
[66] Kweon YO, Goodman ZD, Dienstag JL, et al. Decreasing fibrogenesis: an immunohisto-
chemical study of paired liver biopsies following lamivudine therapy for chronic hepatitis
B. J Hepatol 2001;35:749–55.
[67] Marcellin P, Chang TT, Lim SG, et al. Adefovir dipivoxil for the treatment of hepatitis B e
antigen-positive chronic hepatitis B. N Engl J Med 2003;348:808–16.
[68] Lai CL, Shouval D, Lok AS, et al. Entecavir versus lamivudine for patients with
HbeAg –negative chronic hepatitis B. N Engl J Med 2006;354:1011–26.

913HEPATITIS B AND END-STAGE LIVER DISEASE
[69] Lai CL, Gane E, Hsu C, et al. Two-year results from the GLOBE trial in patients with
hepatitis B: greater clinical and antiviral efficacy for telbivudine (LdT) vs. lamivudine [ab-
stract]. Presented at the American Association for the Study of Liver Disease (AASLD),
October 30, 2006.
[70] Hadziyannis SJ, Tassopoulos NC,Heathcote EJ, et al. Long-term therapy with adefovir di-
pivoxil for HbeAg negative chronic hepatitis B for up to 5 years. Gastroetenrology 2006;
131:1743–51.
[71] Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and
advanced liver disease. N Engl J Med 2004;351:1521–31.
[72] Kiki I, Yilmaz O, Erdem F, et al. Tumour necrosis factor-alpha levels in hepatitis B virus-
related chronic active hepatitis and liver cirrhosis and its relationship toKnodell andChild-
Pugh Scores. Int J Clin Pract 2006;9:1075–9.
[73] Sigal SH, Ala A, Ivanov K, et al. Histopathology and clinical correlates of end-stage
hepatitis B cirrhosis: a possible mechanism to explain the response to antiviral therapy.
Liver Transpl 2005;11:82–8.
[74] Akriviadis E, Botla R, BriggsW, et al. Pentoxifylline improves short-term survival in severe
acute alcoholic hepatitis: a double-blind, placebo-controlled trial. Gastroenterology 2000;
119:1637–48.
[75] Montano-Loza AJ, Czaja AJ. Current therapy for autoimmune hepatitis. Nat Clin Pract
Gastroenterol Hepatol 2007;4:202–14.
[76] Perrillo R, Tamburro C, Regenstein F, et al. Low dose, titrateable interferon alpha in de-
compensated liver disease caused by chronic infection with hepatitis B virus. Gastroenterol
1995;109:908–16.
[77] Hoofnagle JH, Di Bisceglie AM, Waggoner JG, et al. Interferon alfa for patients with
clinically apparent cirrhosis due to chronic hepatitis B. Gastroenterology 1993;104:
1116–21.
[78] Marcellin P, Giuily N, Loriot MA, et al. Prolonged interferon-alpha therapy of hepatitis
B virus-related decompensated cirrhosis. J Viral Hepat 1997;4S:21–6.
[79] Villeneuve JP, Condreay LD, Willems B, et al. Lamivudine treatment for decompensated
cirrhosis resulting from chronic hepatitis B. Hepatology 2000;31:207–10.
[80] Kapoor D, Guptan RC, Wakil SM, et al. Beneficial effects of lamivudine in hepatitis
B virus-related decompensated cirrhosis. J Hepatol 2000;33:308–12.
[81] Hann HW, Fontana RJ, Wright T, et al. A United States compassionate use study of
lamivudine treatment in nontransplantation candidates with decompensated hepatitis
B virus-related cirrhosis. Liver Transpl 2003;9:49–56.
[82] Yao FY, Terrault NA, Freise C, et al. Lamivudine is beneficial in patients with severely
decompensated cirrhosis and actively replicating hepatitis b infection awaiting liver trans-
plantation: a comparative study using a matched, untreated cohort. Hepatology 2001;34:
411–6.
[83] Manolakopoulos S,Karatapanis S, Elefsiniotis J, et al. Clinical course of lamivudinemono-
therapy in patients decompensated cirrhosis due toHbeAg negative chronicHBV infection.
Am J Gastroenterol 2004;99:57–63.
[84] Fontana RJ, Hann HW, Perillo RP, et al. Determinants of early mortality in patients with
decompensated chronic hepatitis B treated with antiviral therapy. Gastroenterology 2002;
123:719–27.
[85] Schiff E, Lai CL, Hadziyannis S, et al. Adefovir dipivoxil for wait-listed and post-liver
transplantation patients with lamivudine resistant hepatitis B: final long-term results. Liver
Transpl 2007;13:349–60.
[86] Lacombe K, Gozlan J, Boelle PY, et al. Long-term hepatitis B virus dynamics in HIV-
hepatitis B virus-co-infected patients treated with tenofovir disoproxil fumarate. AIDS
2005;19:907–15.
[87] Benhamou Y, Fleury H, Trimoulet, et al. Anti-hepatitis B virus efficacy of tenofovir
disoproxil fumarate in HIV-infected patients. Hepatology 2006;43:548–55.

914 WEISBERG et al
[88] Taltuvull TC, Chahri N, Verdura B, et al. Successful treatment with tenofovir in a child C
cirrhotic patient with lamivudine-resistant hepatitis B virus awaiting liver transplantation.
Post-transplant results. Transpl Int 2005;18:879–83.
[89] Ratziu V, Thibault V, Benhamou Y, et al. Successful rescue therapy with tenofovir in a pa-
tient with hepatic decompensation and adefovir resistant HBV mutant. Comp Hepatol
2006;5:1.
[90] Keeffe EB, Dieterich DT, Han SHB, et al. A treatment algorithm for the management of
chronic hepatitis B virus infection in the United States: an update. Clin Gastroenterol
Hepatol 2006;4:936–62.
[91] Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2007;45:507–39.
[92] YuenMF, ChowDH, Tsui K, et al. Liver histology of Asian patients with chronic hepatitis
B on prolonged therapy. Aliment Pharmicol Ther 2005;21:841–9.
[93] YimHJ, ByunKS, ChangYJ, et al. Levels of hepatitis B virus (HBV) replication during the
nonreplicative phase: HBV quantification by real-time PCR in Korea. Dig Dis Sci 2007;52:
2403–9.
[94] Chien RN, Lin CH, Liaw YF. The effect of lamivudine therapy in hepatic decompensation
during acute exacerbation of chronic hepatitis B. J Hepatol 2003;38:322–7.
[95] Tsubota A, Arase Y, Suzuki Y, et al. Lamivudine monotherapy for spontaneous severe
acute exacerbation of chronic hepatitis B. J Gastrotenterol Hepatol 2005;20:426–32.
[96] Dienstag JL, Goldin RD, Heathcote EJ, et al. Histological outcome during long-term
lamivudine therapy. Gastroenterology 2003;124:105–17.
[97] Suzuki Y, Arase Y, IkedaK, et al. Histological improvements after a three-year lamivudine
therapy in patients with chronic hepatitis B in whom YMDD mutants did or did not
develop. Intervirology 2003;46:164–70.
[98] RizzettoM, Tassopoulos NC,GoldinRD, et al. Extended lamivudine treatment in patients
with HbeAg-negative chronic hepatitis B. J Hepatol 2005;42:173–9.
[99] Yuen MF, Yuan HJ, Wong DK, et al. Prognostic determinants of chronic hepatitis B in
Asians: therapeutic implications. Gut 2005;54:1610–4.
[100] Lim SG, Wai CT, Rajnakova A, et al. Fata hepatitis B reactivation following discontinu-
ation of nucleoside analogues for chronic hepatitis B. Gut 2002;51:597–9.
[101] Zhang JM,WangXY,HuangYX, et al. Fatal liver failure with the emergence of hepatitis B
surface antigen variants with multiple stop mutations after discontinuation of lamivudine
therapy. J Med Virol 2006;78:324–8.
[102] HonkoopP, deManRA,NiestersHG, et al. Acute exacerbationof chronic hepatitis B virus
infection after withdrawal of lamivudine therapy. Hepatology 2000;32:635–9.
[103] GhanyM, Liang TJ. Drug targets and molecular mechanisms of drug resistance in chronic
hepatitis B. Gastroetnerology 2007;132:1574–85.
[104] Fung SK, Andreone P, Han SH, et al. Adefovir resistant hepatitis B can be associated with
viral rebound and hepatic decompensation. J Hepatol 2005;43:937–43.
[105] DiMarco V, DiStefano R, Ferraro D, et al. HBV-DNA suppression and disease course in
HBV cirrhosis patients on long-term lamivudine therapy. Antivir Ther 2005;10:431–9.
[106] Wiegand J, Tischendorf JJ, Nashan B, et al. Severe exacerbation of chronic hepatitis B after
emergence of lamivudine resistance in a cirrhotic patient: immediate switch to adefovir di-
pivoxil appears to be indicated. Z Gastroenterol 2004;42:15–8.
[107] Colonno RJ, Rose RE, Pokornowski K, et al. Four year assessment of ETV resistance in
nucleoside-naı̈ve and lamivudine refractory patients. Presented at the 42ndAnnualMeeting
of theEuropeanAssociation for the Studyof theLiver. Barcelona, Spain,April 11–15, 2007.
[108] Sheldon J, CaminoN, Rodes B, et al. Selection of hepatitis B virus polymerasemutations in
HIV-coinfected patients treated with tenofovir. Antivir Ther 2005;10:727–34.
[109] Locarnini S. Molecular virology and the development of resistance mutants: implications
for therapy. Semin Liver Dis 2006;25S:9–19.
[110] Sung JJY, Lai JY, Zeuzem S, et al. A randomized double-blind phase II study of lamivu-
dine (LAM) compared to lamivudine plus adefovir dipivoxil (ADV) for treatment naı̈ve

915HEPATITIS B AND END-STAGE LIVER DISEASE
patients with chronic hepatitis B (CHB): Week 52 analysis. J Hepatol 2003;38(Suppl 2):
25–6.
[111] Lai CL, Leung N, Teo EK, et al. A 1-year trial of telbivudine, lamivudine, and the combi-
nation in patients with hepatitis B e antigen-positive chronic hepatitis B. Gastroenterology
2005;129:528–36.
[112] Liaw YF. Rescue therapy for lamivudine-resistant chronic hepatitis B: When and how?
Hepatology 2007;45:266–8.
[113] Kim KM, Choi WB, Lim YS, et al. Adefovir dipivoxil alone or in combination with
ongoing lamivudine in patients with decompensated liver disease and lamivudine resistant
hepatitis B virus. J Korean Med Sci 2005;20:821–8.
[114] Liaw YF, Lee CM, Chien RN, et al. Switching to adefovir monotherapy after the emer-
gence of lamivudine resistant mutations in patients with liver cirrhosis. J Viral Hepat
2006;13:250–5.
[115] LamperticoP,MarzanoA, LevreroM, et al. Adefovir and lamivudine combination therapy
is superior to adefovir monotherapy for lamivudine-resistant patients with HBeAg-nega-
tive chronic hepatitis B. Presented at the 42ndAnnualMeeting of theEuropeanAssociation
for the Study of the Liver. Barcelona, Spain, April 11–15, 2007.
[116] Rapti I, Dimou E, Mitsoula P, et al. Adding-on versus switching-to adefovir therapy in
lamivudine-resistant HBeAg-negative chronic hepatitis. Hepatology 2007;45:307–13.
[117] Chang T, Gish R, De Man R, et al. A comparison of entecavir and lamivudine in HbeAg-
positive chronic hepatitis B. N Engl J Med 2006;354:1001–10.
[118] Schiff ER, Lai CL, Hadziyannis S, et al. Adefovir dipivoxil therapy for lamivudine-
resistant hepatitis B in pre- and post-liver transplantation patients. Hepatology 2003;
38:1419–27.
[119] Terrault N, Roche B, Samuel D.Management of the hepatitis B virus in the liver transplan-
tation setting: a European and an American perspective. Liver Transpl 2005;11:716–32.
[120] Samuel D, Muller R, Alexander G, et al. Liver transplantation in European patients with
the hepatitis B surface antigen. N Engl J Med 1993;329:1842–7.
[121] Han SH, Ofman J, Holt C, et al. An efficacy and cost-effectiveness strategy of combination
hepatitis B immune globulin and lamivudine to prevent recurrent hepatitis B after ortho-
topic liver transplantation comparedwith hepatitis B immune globulinmonotherapy. Liver
Transpl 2001;6:741–8.
[122] KimWR, Poterucha JJ, Kremers WK, et al. Outcome of liver transplantation for hepatitis
B in the United States. Liver Transpl 2004;10:968–74.
[123] Rosenau J, Bahr M, Tillman HL, et al. Lamivudine and low-dose hepatitis B immune
globulin for prophylaxis of hepatitis B reinfection after liver transplantation. Possible
role of mutations in the YMDD motif prior to transplantation as a risk factor for reinfec-
tion. J Hepatol 2001;34:895–902.
[124] Seehofer D, Rayes N, Naumann U, et al. Preoperative antiviral treatment and post-
operative prophylaxis in HBV-DNA positive patients undergoing liver transplantation.
Transplantation 2001;72:1381–5.
[125] Markowitz JS, Martin P, Conrad AJ, et al. Prophylaxis against hepatitis B recurrence
following liver transplant using combination lamivudine and hepatitis B immune globulin.
Hepatology 1998;28:585–9.
[126] Angus PW, McCaughan GW, Gane EJ, et al. Combination low-dose hepatitis B immune
globulin and lamivudine therapy provides effective prophylaxis against post-transplanta-
tion hepatitis B. Liver Transpl 2000;6:429–33.
[127] Marzano A, Salizzoni M, Debernardi-Vernon W, et al. Prevention of hepatitis B virus
recurrence after liver transplantation in cirrhotic patients treated with lamivudine and
passive immunoprophylaxis. J Hepatol 2001;34:903–10.
[128] Gane EJ, Angus PW, Strasser S, et al. Lamivudine plus low-dose hepatitis B immunoglob-
ulin to prevent recurrent hepatitis B following liver transplantation. Gastroenterology
2007;132:931–7.

916 WEISBERG et al
[129] Buti M, Mas A, Prieto M, et al. A randomized study comparing lamivudine monotherapy
after a short course of hepatitis B immune globulin (HBIG) and lamivudine with long-term
lamivudine plusHBIG in the prevention of hepatitis B virus recurrence after liver transplan-
tation. J Hepatol 2003;38:811–7.
[130] Wong SN, Chi-Jen C, Chun-Tao W, et al. Low risk of hepatitis B virus recurrence after
treatment withdrawal of long-term hepatitis B immunoglobulin in patients receiving main-
tenance nucleos(t)ide analogue therapy. Liver Transpl 2007;13:374–81.
[131] Neff GW, Kemmer N, Kaiser TE, et al. Combination therapy in liver transplant recipients
with hepatitis B virus without hepatitis B immune globulin. Dig Dise Sci 2007;52:2497–500.
[132] Fontana RJ, Keeffe EB, Carey W, et al. Effect of lamivudine treatment on survival of 309
North American patients awaiting liver transplantation for chronic hepatitis B. Liver
Trasnpl 2002;8:433–9.