Embed Size (px)
Citation preview

Hepatitis C in Asymptomatic Blood Donors
HARVEY J. ALTER,1 CATHY CONRY-CANTILENA,1 JACQUELINE MELPOLDER,1 DE TAN,1 MARK VAN RADEN,2 DAVID HERION,3
DARYL LAU,3 AND JAY H. HOOFNAGLE3
Among 248 asymptomatic blood donors positive for anti- widespread in the blood donor population, that hepatitisC accounted for more than 90% of transfusion-transmittedbody to hepatitis C virus (anti-HCV) enrolled in a long-term
prospective study, 86% had chronic HCV infection and 14% hepatitis, and that chronic HCV infection, although generallyasymptomatic, could in some cases lead to cirrhosis, hepato-appeared to have recovered as assessed by serial determina-
tions of serum alanine aminotransferase (ALT) levels and cellular carcinoma (HCC), and end-stage liver disease.2,3
First-generation tests for anti-HCV were introduced intoHCV RNA by polymerase chain reaction. Established paren-teral risk factors for HCV transmission were identified in blood donor screening in 1990. At that time, 0.5% to 0.6%
of donors were repeatedly reactive by enzyme immunoassay75% of donors. In addition, there was a strong independentassociation between HCV positivity and cocaine snorting, sug- (EIA), and approximately 0.3% could be confirmed as posi-
tive by supplemental strip recombinant immunoblot assay.gesting that shared snorting devices may be a covert routeof parenteral transmission. Ear piercing in males was also More sensitive second- and third-generation EIAs4 were in-
troduced in 1992 and 1996, respectively. Current data fromsignificantly associated with transmission. There was no evi-dence for sexual spread. Although the majority of HCV carri- the American Red Cross indicate that 0.23% of blood donors
now test repeatedly positive for anti-HCV, and 0.16% can beers had both biochemical and histological evidence of chronicviral hepatitis, the extent of liver injury was generally mild. confirmed by supplemental assays. These tests have been
extremely effective in the prevention of transfusion-associ-Among a larger population of 280 HCV RNA–positive donors,17% had repeatedly normal ALT levels, 45% had levels that ated hepatitis. An ongoing prospective study of transfusion
recipients at the Clinical Center of the National Institutesdid not exceed twice, and only 22% had levels that exceededfive times the upper limit of the normal range. Among 81 of Health (NIH) has shown no cases of hepatitis C among
approximately 650 recipients monitored since second-gener-patients who underwent liver biopsy, only 13% had evidenceof severe hepatitis (8%) or cirrhosis (5%), despite a duration ation EIA screening was implemented.
Screening assays for anti-HCV have uncovered a largeof infection that generally exceeded 15 years. No severe histo-logical lesions were observed in blood donors with chronic group of patients who are asymptomatic HCV carriers. Popu-
lation-based surveys suggest that there are almost four mil-HCV infection who had repeatedly normal ALT levels. Inboth donors and blood recipients, the frequency of severe lion HCV carriers in the United States. Furthermore, this
virus is globally distributed, with anti-HCV rates among do-morbidity or mortality related to HCV infection was less than10% during the first two decades of infection. Further long- nors throughout the world ranging from 0.3% to 1.5%. Thus,
hepatitis C has been found to be a common infection ofterm studies are required to see if the progression to severeoutcomes continues to accrue at this slow pace or whether it worldwide importance.
What is the significance of this infection to these asymp-accelerates during subsequent decades. (HEPATOLOGY 1997;26(Suppl 1):29S-33S.) tomatic individuals? How were they infected? What is the
risk that they will transmit the infection to others? Whatproportion of antibody-positive individuals have viremia andThe cloning of the hepatitis C virus (HCV)1 and subse-chronic infection? What proportion have significant liver dis-quent development of sensitive serologic assays for antibodyease? What insights can we derive from this asymptomaticto HCV (anti-HCV) and reliable polymerase chain reactiondonor population in assessing the natural history of HCV(PCR) tests for HCV RNA have shown that this agent isinfection? In the spectrum of HCV associated disorders, whatproportion are represented by the relatively benign diseaseseen in donors and what proportion progress to the severe
Abbreviations: HCV, hepatitis C virus; anti-HCV, antibody to hepatitis C virus; outcomes that now make HCV-related liver failure the lead-PCR, polymerase chain reaction; HCC, the hepatocellular carcinoma; EIA, enzyme ing indication for liver transplantation in adults? To addressimmunoassay; NIH, National Institutes of Health.
these issues, we review data from an ongoing NIH study ofFrom the 1Department of Transfusion Medicine, Warren Grant Magnuson ClinicalHCV-infected blood donors and from a parallel prospectiveCenter; 2Division of Microbiology and Infectious Diseases, National Institute of Allergy
and Infectious Diseases; and 3Liver Diseases Section, Digestive Diseases Branch, Na- study of blood recipients with transfusion-associated hepati-tional Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of tis.Health, Bethesda, MD.
Received May 14, 1997.BACKGROUND: NIH PROSPECTIVE STUDY OFAddress reprint requests to: Harvey J. Alter, M.D., Department of Transfusion
HCV-INFECTED DONORSMedicine, Building 10, Room 1C-711, National Institutes of Health, Bethesda, MD20892-1184. Fax: (301) 402-1360.
In collaboration with the American Red Cross, membersCopyright q 1997 by the American Association for the Study of Liver Diseases.0270-9139/97/2603-0119$3.00/0 of the Department of Transfusion Medicine of the NIH initi-
29S
AID Hepa 0019 / 5p25$$$361 08-06-97 02:19:28 hepas WBS: Hepatology

30S ALTER ET AL. HEPATOLOGY September 1997
ated a large, prospective study of blood donors found to be parents of confirmed anti-HCV–positive donors. Nine of 85sexual partners (11%) were anti-HCV positive, but all 9 hadanti-HCV positive on routine screening. Blood donors who
tested repeatedly reactive for anti-HCV by EIA were invited independent parenteral risk factors for acquiring hepatitis C.Similarly, 5 of 47 children (11%) of HCV carriers were anti-to participate. After providing informed consent, participants
underwent careful interviews for potential risk factors and HCV positive, but 4 appeared to have anti-HCV as a result ofpassive transfer from the mother, and the fifth had a separatelaboratory testing for evidence of liver disease and serological
markers of hepatitis. A total of 481 blood donors who tested parenteral risk factor. Finally, 2 of 6 parents of HCV carrierswere anti-HCV positive, but both had known parenteral ex-repeatedly reactive for anti-HCV by EIA were enrolled; this
included 248 who had a positive reaction by supplemental posures. Thus, none of 138 sexual or household contactshad anti-HCV positivity that could not be explained by animmunoblot assay, 102 who had an indeterminate reaction,
and 131 who were immunoblot negative.5 independent parenteral risk factor or by passive transfer ofantibody. These results indicate that familial transmission of
RISK FACTORS FOR ANTI-HCV POSITIVITY hepatitis C is probably rare.Comparing anti–HCV EIA-reactive positive patients who
CHRONIC VIREMIA AMONG ANTI-HCV–POSITIVEtested positive or negative by immunoblot, several demo-BLOOD DONORSgraphic and historical factors were significantly associated
with positivity: lower age (37 vs. 44 years; P õ .001), the Evidence of chronic hepatitis and chronic viremia wassought among the various cohorts of anti-HCV–positiveabsence of college education (54% vs. 16%; P õ .001), black
race (19% vs. 7%; P Å .002), first-time donor status (24% blood donors. HCV RNA was detected by PCR in 86% ofconfirmed anti-HCV–positive donors, in 3% of donors withvs. 2%; P õ .001), a history of liver disease (31% vs. 5%; P
õ .001), and a history of sexually transmitted disease (28% an indeterminate immunoblot result, and in none of the im-munoblot-negative donors. Of the three immunoblot-inde-vs. 10%; P õ .001).
In a logistic regression model analysis, significant risk fac- terminate donors who were PCR positive, two were immu-noblot positive on a more sensitive third-generation assay. Ittors for immunoblot reactivity were a history of blood trans-
fusion (27% vs. 8%; P õ .001), intranasal cocaine use (68% is important to note that 14% of confirmed antibody-positivepatients were HCV RNA negative by PCR, even when testedvs. 11%; P õ .001), injection drug use (42% vs. 2%;
P Å .001), sexual promiscuity, as defined by a history of on multiple serial specimens. These results suggest that ap-proximately 15% of patients who become infected with HCVsexually transmitted disease, sex with a prostitute or more
than five partners per year (53% vs. 24%; P õ .002), and ear recover from the infection and eradicate virus spontaneously.In agreement with this are results from our prospective studypiercing among males (30% vs. 0%; P õ .05). A history of
tattooing or imprisonment was significant in the univariate of transfusion recipients, which revealed that 15% of patientswith acute hepatitis C recover and remain HCV RNA negativeanalysis, but not in the multivariate analysis because of the
close association with injection drug use. There was no on multiple determinations over years of follow-up evalua-tion.6significant association between immunoblot positivity for
anti-HCV and acupuncture or medically related needle-stickLIVER DISEASE IN ASYMPTOMATIC HCV CARRIERSinjuries. The high frequency of injection drug use was unex-
pected because these participants had denied such use at the Biochemical evidence of liver disease was found in 56% ofconfirmed anti-HCV–positive donors on initial evaluationtime of donation. On further questioning, only one admitted
to current drug use, and 74% denied injection drug use dur- and in 69% of those who were monitored with multipledeterminations over time.5 In a current, more extensive anal-ing the previous decade. When asked why they had donated
blood despite a history of injection drug use, most stated ysis of 280 donors who are HCV RNA positive, 17% hadpersistently normal ALT levels and 45% had ALT elevationsthat they did not consider the remote drug use important to
the safety of their donation. that did not exceed twice the upper limit of the normal range.The remaining 38% of HCV RNA–positive donors had atThus, an unexpected finding was that almost half of anti-
HCV–positive blood donors had used injection drugs with least one ALT value greater than twice the upper limit ofnormal. However, even in this group, ALT elevations wereshared needles at some point in their lives. Just as unexpected
was the high proportion of donors who had used intranasal modest; only 18% had elevations between 5 and 10 times,and only 4% had levels greater than 10 times the upper limitcocaine (snorting). Indeed, 68% of confirmed ant-HCV–pos-
itive donors, as well as 11% of anti-HCV–negative donors, of normal.Liver biopsies were performed in 81 HCV RNA–positiveadmitted to a history of cocaine use. Further questioning of
cocaine users revealed that 84% shared straws, 44% had used blood donor participants in this study. All donors who hadHCV RNA in serum had histological evidence of chroniccocaine intranasally three or more times per day, 29% re-
ported a history of epistaxis during intranasal cocaine use, hepatitis, but in 53%, the histological lesions were mild, andin an additional 36%, only moderate injury was noted. Thus,and 27% observed epistaxis in others. These findings suggest
that intranasal cocaine use with shared devices and associated among volunteer blood donors identified as having chronicHCV infection after routine screening, only 13% had severeepistaxis may represent a covert mechanism of viral transmis-
sion. histological findings on liver biopsy, including 1% with se-vere chronic active hepatitis, 7% with chronic active hepatitis
FAMILIAL TRANSMISSION BY ANTI-HCV POSITIVE and bridging hepatic fibrosis, and 5% with cirrhosis. NoneBLOOD DONORS of the patients with persistently normal ALT values had cir-
rhosis. A slightly higher proportion of severe lesions wereThe possibility of HCV transmission to family contactswas evaluated among 85 sexual partners, 47 children, and 6 observed in those with ALT elevations that exceeded twice
AID Hepa 0019 / 5p25$$$362 08-06-97 02:19:28 hepas WBS: Hepatology
HEPATOLOGY Vol. 26, No. 3, Suppl. 1, 1997 ALTER ET AL. 31S
the upper limit of normal, but this was not significantlydifferent from those with lesser elevations.
DURATION OF HCV INFECTION ANDCLINICAL OUTCOME
Although it is clear that HCV infection can have seriouslong-term consequences, its clinical course is generally indo-lent. In studies from Japan,2 the mean time from a transfusionexposure to the clinical presentation of chronic hepatitis Cwas 13.6 years. Clinical cirrhosis was not apparent until anaverage of 17.8 years, and HCC until 23.4 years after expo-sure. Similar prolonged intervals were observed in a studyfrom the United States3 wherein the average period betweenexposure by blood transfusion and the clinical expression of
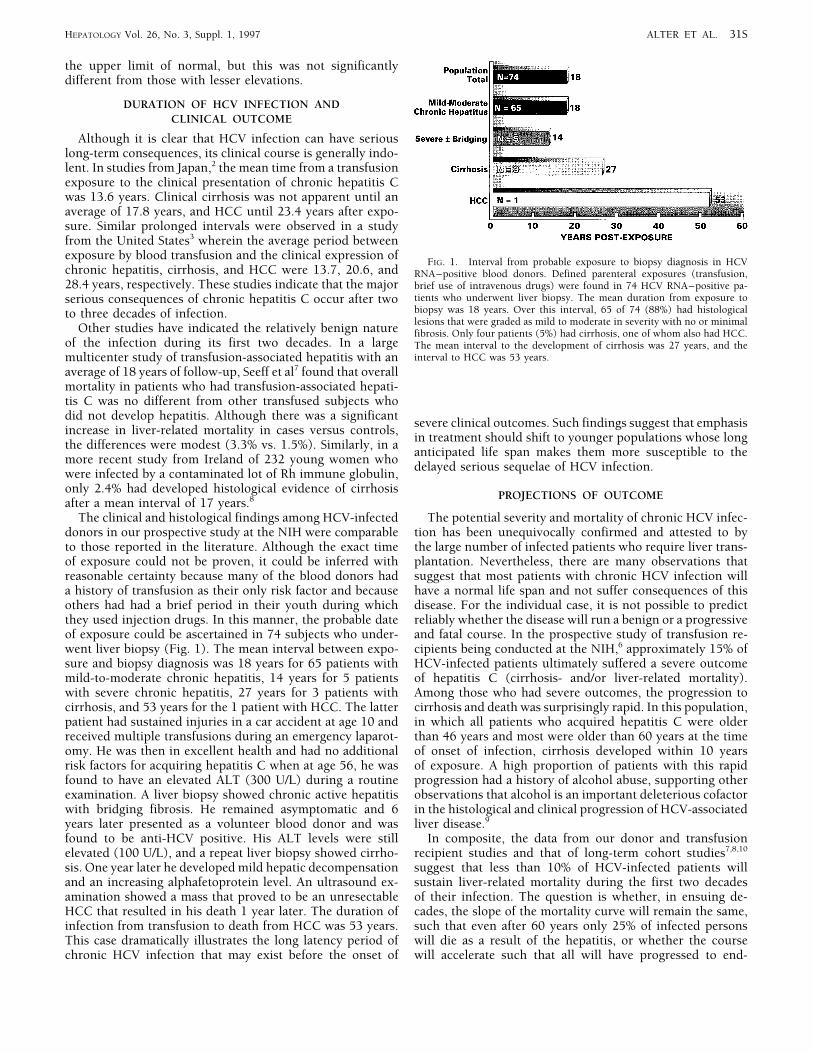
FIG. 1. Interval from probable exposure to biopsy diagnosis in HCVchronic hepatitis, cirrhosis, and HCC were 13.7, 20.6, and RNA–positive blood donors. Defined parenteral exposures (transfusion,28.4 years, respectively. These studies indicate that the major brief use of intravenous drugs) were found in 74 HCV RNA–positive pa-
tients who underwent liver biopsy. The mean duration from exposure toserious consequences of chronic hepatitis C occur after twobiopsy was 18 years. Over this interval, 65 of 74 (88%) had histologicalto three decades of infection.lesions that were graded as mild to moderate in severity with no or minimal
Other studies have indicated the relatively benign nature fibrosis. Only four patients (5%) had cirrhosis, one of whom also had HCC.of the infection during its first two decades. In a large The mean interval to the development of cirrhosis was 27 years, and the
interval to HCC was 53 years.multicenter study of transfusion-associated hepatitis with anaverage of 18 years of follow-up, Seeff et al7 found that overallmortality in patients who had transfusion-associated hepati-tis C was no different from other transfused subjects whodid not develop hepatitis. Although there was a significant
severe clinical outcomes. Such findings suggest that emphasisincrease in liver-related mortality in cases versus controls,
in treatment should shift to younger populations whose longthe differences were modest (3.3% vs. 1.5%). Similarly, in a
anticipated life span makes them more susceptible to themore recent study from Ireland of 232 young women who
delayed serious sequelae of HCV infection.were infected by a contaminated lot of Rh immune globulin,only 2.4% had developed histological evidence of cirrhosis
PROJECTIONS OF OUTCOMEafter a mean interval of 17 years.8
The clinical and histological findings among HCV-infected The potential severity and mortality of chronic HCV infec-tion has been unequivocally confirmed and attested to bydonors in our prospective study at the NIH were comparable
to those reported in the literature. Although the exact time the large number of infected patients who require liver trans-plantation. Nevertheless, there are many observations thatof exposure could not be proven, it could be inferred with
reasonable certainty because many of the blood donors had suggest that most patients with chronic HCV infection willhave a normal life span and not suffer consequences of thisa history of transfusion as their only risk factor and because
others had had a brief period in their youth during which disease. For the individual case, it is not possible to predictreliably whether the disease will run a benign or a progressivethey used injection drugs. In this manner, the probable date
of exposure could be ascertained in 74 subjects who under- and fatal course. In the prospective study of transfusion re-cipients being conducted at the NIH,6 approximately 15% ofwent liver biopsy (Fig. 1). The mean interval between expo-
sure and biopsy diagnosis was 18 years for 65 patients with HCV-infected patients ultimately suffered a severe outcomeof hepatitis C (cirrhosis- and/or liver-related mortality).mild-to-moderate chronic hepatitis, 14 years for 5 patients
with severe chronic hepatitis, 27 years for 3 patients with Among those who had severe outcomes, the progression tocirrhosis and death was surprisingly rapid. In this population,cirrhosis, and 53 years for the 1 patient with HCC. The latter
patient had sustained injuries in a car accident at age 10 and in which all patients who acquired hepatitis C were olderthan 46 years and most were older than 60 years at the timereceived multiple transfusions during an emergency laparot-
omy. He was then in excellent health and had no additional of onset of infection, cirrhosis developed within 10 yearsof exposure. A high proportion of patients with this rapidrisk factors for acquiring hepatitis C when at age 56, he was
found to have an elevated ALT (300 U/L) during a routine progression had a history of alcohol abuse, supporting otherobservations that alcohol is an important deleterious cofactorexamination. A liver biopsy showed chronic active hepatitis
with bridging fibrosis. He remained asymptomatic and 6 in the histological and clinical progression of HCV-associatedliver disease.9years later presented as a volunteer blood donor and was
found to be anti-HCV positive. His ALT levels were still In composite, the data from our donor and transfusionrecipient studies and that of long-term cohort studies7,8,10elevated (100 U/L), and a repeat liver biopsy showed cirrho-
sis. One year later he developed mild hepatic decompensation suggest that less than 10% of HCV-infected patients willsustain liver-related mortality during the first two decadesand an increasing alphafetoprotein level. An ultrasound ex-
amination showed a mass that proved to be an unresectable of their infection. The question is whether, in ensuing de-cades, the slope of the mortality curve will remain the same,HCC that resulted in his death 1 year later. The duration of
infection from transfusion to death from HCC was 53 years. such that even after 60 years only 25% of infected personswill die as a result of the hepatitis, or whether the courseThis case dramatically illustrates the long latency period of
chronic HCV infection that may exist before the onset of will accelerate such that all will have progressed to end-
AID Hepa 0019 / 5p25$$$362 08-06-97 02:19:28 hepas WBS: Hepatology

32S ALTER ET AL. HEPATOLOGY September 1997
stage liver disease, if they have not died from an intercurrent on liver biopsy are rare among patients with normal andnear-normal ALT levels. Given the low level of efficacy ofillness.
It is difficult to ascertain the likelihood of long-term severe current antiviral therapy and the frequency of side effects,treatment in this group should be deferred until more effec-consequences of chronic hepatitis C from standard prospec-
tive studies because of the generally indolent nature of this tive therapies are developed or until ALT elevations are ob-served during the course of long-term follow-up.disease. An alternative approach to classic prospective studies
is to test samples from archived repositories and then trace In our study of HCV RNA–positive blood donors, histo-logical evidence of severe hepatitis and cirrhosis was ob-the outcomes of HCV-infected patients and controls. Such a
study of Air Force recruits who were sampled 50 years ago served in only 13% after a mean interval of 18 years fromsuspected time of exposure. Similarly, in a prospective studyis being conducted by Seeff et al., but data have not been
fully analyzed. If these patients, who have been infected for of HCV-infected transfusion recipients, approximately 15%developed cirrhosis or sustained liver-related mortality withhalf a century, show no or minimally increased mortality
compared with controls and if patients in the multicenter a follow-up duration of 10 to 20 years. In some blood transfu-sion recipients, cirrhosis and end-stage liver disease devel-transfusion study7 and those who have received contami-
nated Rh immune globulin8,10 continue to show low rates of oped within 10 years of transfusion. The more-rapid-than-anticipated progression may relate to the older age at theliver-related mortality into the third and fourth decades of
follow-up, then it is probable that the mortality curve ob- time of exposure or to past alcohol abuse. These studiessupport the recommendation that HCV-infected individualsserved in the first 20 years of infection will continue its
current slope. If such were the case, then 75% of HCV-in- minimize their alcohol intake.Age appears to have an important influence on the severityfected patients would live out their ‘‘natural’’ life span, even
without antiviral therapy. The conundrum is that for antiviral and progression of hepatitis C. Although most persons olderthan 60 years who become infected with HCV will die oftherapy to be effective in altering the natural history of this
indolent disease, it probably should be applied at an early natural causes or intercurrent illnesses before they have clini-cal manifestations of HCV infection, a proportion will havestage, before the onset of significant fibrosis or hepatic injury,
at a time when the likelihood of eventual serious complica- rapidly progressive disease. These opposing outcomes maketreatment decisions for the elderly difficult. On the other endtions appears low.of the spectrum, it is essential to establish whether neonates,
SUMMARY AND CONCLUSIONS infants, and older children have the same rate of persistentinfection and progression to chronic liver disease as doApproximately 15% of immunoblot-confirmed anti-HCV–
positive blood donors and recipients have recovered from a adults. If so, treatment emphasis should shift to youngerpopulations whose anticipated longevity provides the timeprior HCV infection as judged by normal ALT levels and
absence of HCV RNA by PCR on repeated determinations. frame for the slow evolution of the serious sequelae of HCVinfection. Prospective studies of HCV infection in childrenTesting for HCV RNA by qualitative PCR is important to the
proper counseling of anti-HCV reactive individuals. are needed.There are substantial data from prospective transfusionIn approximately 75% of subjects with chronic hepatitis
C, the mode of transmission can be identified by direct ques- studies and from retrospective-prospective cohort studies toindicate that liver-related mortality or severe morbidity istioning that establishes a history of parenteral exposures,
most frequently transfusion and injection drug use. Expo- less than 10% in the first two decades of infection. At issueis whether the mortality curve will maintain its course orsures such as drug use are often remote and elicited only
after careful interview. Intranasal cocaine use with shared sharply escalate in the ensuing decades. If the curve is main-tained, then only 25% will have a fatal outcome even afterstraws may be an important covert form of parenteral expo-
sure. Further studies are needed to establish the role of co- 60 years, but if the slope accelerates, then every patient mightultimately have a severe outcome if they do not succumb tocaine use and other potential covert exposures in the trans-
mission of hepatitis C. an intercurrent disease. This question has major implicationsfor treatment decisions, and high priority should be given toAlthough sexual transmission of hepatitis C has been sug-
gested by the frequency of a history of sexual promiscuity the continued follow-up of patients who are already in long-term follow-up studies and for the initiation of new studiesamong HCV-infected individuals, studies of family members
and sexual contacts of HCV carriers have rarely identified that can identify cohorts that were infected 30 or more yearsago.evidence for sexual transmission of this disease. Therefore,
safe sex practices are recommended for all promiscuous indi-REFERENCESviduals, but individuals involved in long-term monogamous
relationships need not change their sexual practices. It is 1. Choo Q-L, Kuo G, Weiner AJ, Overby LR, Bradley DW, Houghton M.Isolation of a cDNA clone derived from a blood-borne non-A, non-Buseful to test the sexual partner of patients with hepatitis Cviral hepatitis genome. Science 1989;244:359-362.in that a negative result provides useful information on which
2. Kiyosawa K, Akahane Y, Nagata A, Koike Y, Furuta S. Significance ofthe couple can base decisions regarding condom use in theirblood transfusion in non-A, non-B chronic liver disease in Japan. Vox
specific situation, and a positive result will lead to additional Sanguinis 1982;43:45-52.risk history and proper medical management of the partner. 3. Tong MJ, El-Farra S, Reikes R, Co RL. Clinical outcomes after transfu-
sion-associated hepatitis C. New Engl J Med 1995;332:1463-1466.Among HCV RNA–positive blood donors, the majority4. Huang YY, Yang SS, Wu CH, Shih WS, Huang CS, Chen PH, Lin YM,have normal or near-normal ALT levels, even when tested
et al. Impact of screening blood donors for hepatitis C antibody onon multiple occasions; only a small proportion of blood do- posttransfusion hepatitis: a prospective study with second-generationnors with HCV infection have ALT values that exceeded five anti-hepatitis C virus assay. Transfusion 1994;34:661-669.
5. Conry-Cantilena C, VanRaden M, Gibble J, Melpolder J, Shakil AO,times the upper limit of normal. Severe histological lesions
AID Hepa 0019 / 5p25$$$363 08-06-97 02:19:28 hepas WBS: Hepatology

HEPATOLOGY Vol. 26, No. 3, Suppl. 1, 1997 ALTER ET AL. 33S
Viladomiu L, Cheung L, et al. Routes of infection, viremia and liver Kelley P, et al. Presentation of hepatitis C in a unique uniformcohort 17 years from inoculation [Abstract]. Gastroenterologydisease in blood donors found to have hepatitis C virus. New Engl J
Med 1996;334:1691-1696. 1995;108:A1054.9. Bellintani S, Tribelli C, Saccoccio G, Soddle M, Fratti N, DeMartin C,6. Alter HJ. To C or not to C: these are the questions. Blood 1995;85:
1681-1695. Christianni G, et al. Prevalence of chronic liver diseases in the generalpopulation of northern Italy: the Dionysos Study. HEPATOLOGY 1994;7. Seeff LB, Buskell-Bales Z, Wright EC, Durako SJ, Alter HJ, Iber FL,
Hollinger FB, et al. Long-term mortality after transfusion-associated 20:1442-1450.10. Muller R. The natural history of hepatitis C: clinical experiences. Jnon-A, non-B hepatitis. New Engl J Med 1992;327:1906-1911.
8. Crowe J, Doyle C, Fielding JF, Holloway H, Keegan M, Kelleher D, Hepatol 1996;24(Suppl):52-54.
AID Hepa 0019 / 5p25$$$363 08-06-97 02:19:28 hepas WBS: Hepatology







![Long-Term Persistence of Antibody Response with Two Doses ... · 114.2 million cases worldwide [2]. Hepatitis A virus infection is typically asymptomatic and self-limiting in children,](https://img.pdfslide.net/doc/110x75/5fb7c4ed6e0626190f30737c/long-term-persistence-of-antibody-response-with-two-doses-1142-million-cases.jpg)